Differences and Similarities in Diabetes Research between China and the USA


Abstract
:1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
- Primary research studies or secondary analyses of routinely collected data or existing research datasets.
- Studies on diabetes research (e.g., risk factors, prognosis, prevention, diagnosis, treatment, and epidemiology).
- Studies conducted in mainland China or the USA.
- Studies published either in 2010 or 2015, in scientific journals, and with abstracts.
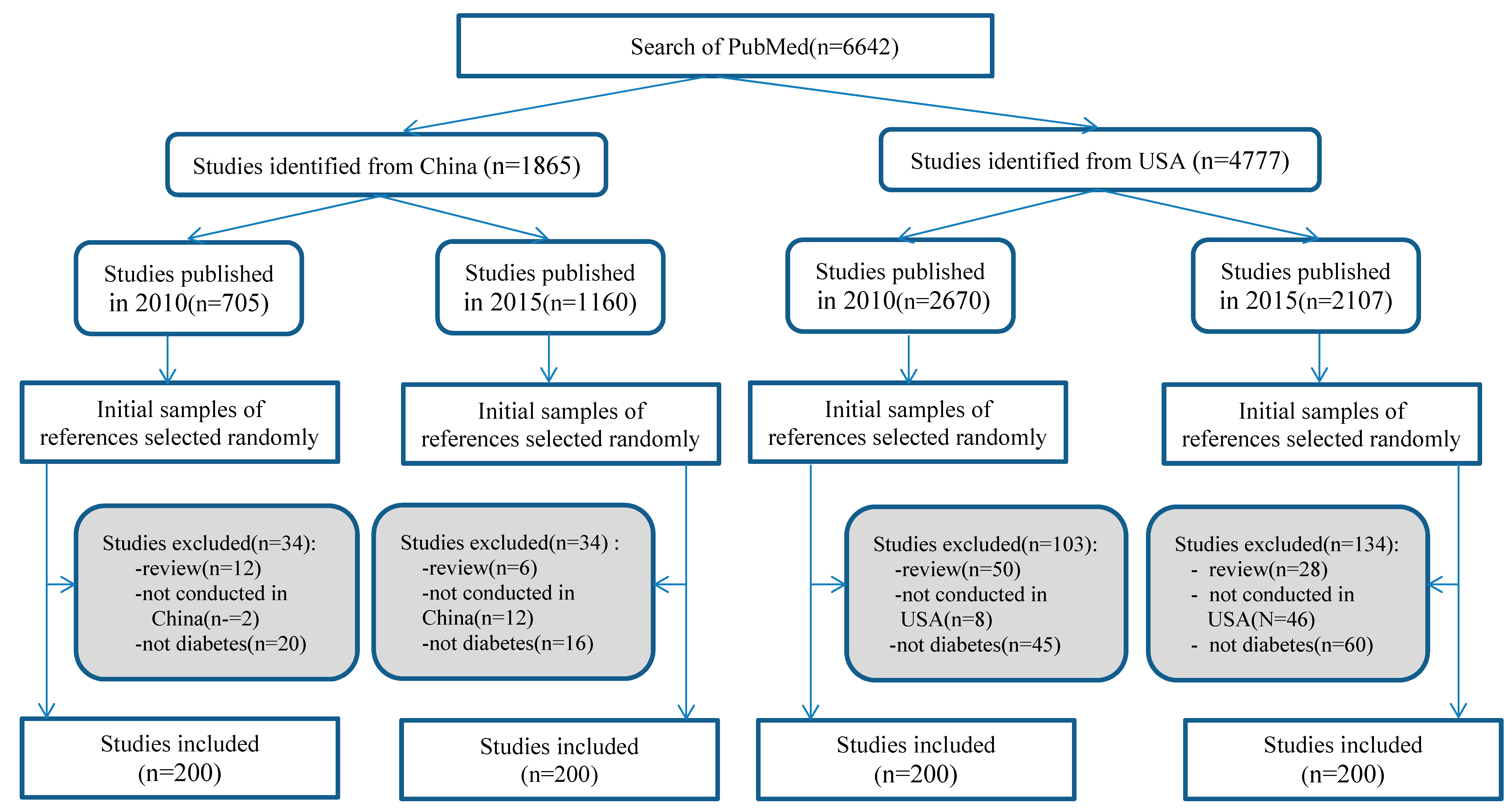
2.2. Study Search and Selection Strategy
2.3. Data Extraction and Analysis
3. Results
3.1. Main Characteristics of Included Studies
3.2. Relevance of the Included Studies
3.3. Type of Interventions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| NCDs | Non-communicable diseases |
| LMICs | Low and Middle Income Countries |
| USA | United States of America |
| RCTs | Randomized Controlled Trials |
References
- WHO. Non-communicable diseases country profiles. 2014. Available online: http://www.who.int/nmh/publications/ncd-profiles-2014/en/ (accessed on 28 July 2017).
- Cao, X. A call for global research on non-communicable diseases. Lancet 2015, 385, e5–e6. [Google Scholar] [CrossRef]
- Ebrahim, S.; Pearce, N.; Smeeth, L.; Casas, J.P.; Jaffar, S.; Piot, P. Tackling non-communicable diseases in low- and middle-income countries: is the evidence from high-income countries all we need? PLoS Med. 2013, 10, e1001377. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, C.; Blacklock, C.; Perera, R.; Davis, R.; Banerjee, A.; Gill, P.; Liew, S.; Chamas, L.; Hernandez, J.; Mahtani, K.; et al. Evidence for non-communicable diseases: analysis of Cochrane reviews and randomised trials by World Bank classification. BMJ Open 2013, 3, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rottingen, J.A.; Regmi, S.; Eide, M.; Young, A.J.; Viergever, R.F.; Ardal, C.; Guzman, J.; Edwards, D.; Matlin, S.A.; Terry, R.F.; et al. Mapping of available health research and development data: what's there, what's missing, and what role is there for a global observatory? Lancet 2013, 382, 1286–1307. [Google Scholar] [CrossRef]
- Mendis, S.; Yach, D.; Bengoa, R.; Narvaez, D.; Zhang, X. Research gap in cardiovascular disease in developing countries. Lancet 2003, 361, 2246–2247. [Google Scholar] [CrossRef]
- Fan, H.; Song, F. An assessment of randomized controlled trials (RCTs) for non-communicable diseases (NCDs): more and higher quality research is required in less developed countries. Sci. Rep. 2015, 5, 13221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mony, P.K.; Srinivasan, K. A bibliometric analysis of published non-communicable disease research in India. Indian J. Med. Res. 2011, 134, 232–234. [Google Scholar] [PubMed]
- Lei, J.; Sockolow, P.; Guan, P.; Meng, Q.; Zhang, J. A comparison of electronic health records at two major Peking University Hospitals in China to United States meaningful use objectives. BMC med. Infor. Decis. 2013, 13, 96. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in Chinese adults. Jama 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. 2016. Available online: http://www.nhfpc.gov.cn/zwgk/tjxx1/ejflist.shtml (accessed on 28 July 2017).
- Reversing the rising tide of diabetes in China. Available online: https://www.thelancet.com/action/showPdf?pii=S0140-6736%2816%2932384-4 (accessed on 5 July 2019).
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017: Estimates of diabetes and its burden in the United States. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 5 August 2019).
- Centers for Disease Control and Prevention. National Diabetes Statistical Report: Estimates of Diabetes and Its Burden in the United States. 2014. Available online: http://www.cdc.gov/diabetes/pubs/statsreport14.htm (accessed on 28 July 2017).
- Menke, A.C.S.; Geiss, L.; Cowie, C.C. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. Jama 2015, 314, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.C.; Geneau, R. Assessing research activity on priority interventions for non-communicable disease prevention in low- and middle-income countries: a bibliometric analysis. Global health action 2012, 5, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Søreide, K.; Alderson, D.; Bergenfelz, A.; Beynon, J.; Connor, S.; Deckelbaum, D.L.; Dejong, C.H.; Earnshaw, J.J.; Kyamanywa, P.; Perez, R.O.; et al. Strategies to improve clinical research in surgery through international collaboration. The Lancet 2013, 382, 1140–1151. [Google Scholar] [CrossRef]
- Chan, A.W.; Song, F.; Vickers, A.; Jefferson, T.; Dickersin, K.; Gøtzsche, PC.; Krumholz, H.M.; Ghersi, D.; van, H.B.; et al. Increasing value and reducing waste: addressing inaccessible research. Lancet 2014, 383, 257–266. [Google Scholar] [CrossRef] [Green Version]
- Woodward, M. Use of national data sources in diabetes epidemiology. Lancet Diabetes Endo. 2015, 3, 92–93. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.D.; Langenberg, C.; Rapsomaniki, E.; Denaxas, S.; Pujades-Rodriguez, M.; Gale, C.P.; Deanfield, J.; Smeeth, L.; Timmis, A.; Hemingway, H.; et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet Diabetes Endo. 2015, 3, 105–113. [Google Scholar] [CrossRef]
- Contopoulos-Ioannidis, D.G.; Ntzani, E.; Ioannidis, J.P. Translation of highly promising basic science research into clinical applications. AM. J. Med. 2003, 114, 477–484. [Google Scholar] [CrossRef]
- The Lancet. The best science for achieving Healthy China 2030. Lancet 2016, 388, 1851. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Countries of Authors | Published in 2010 | Published in 2015 | All | ||||
|---|---|---|---|---|---|---|---|
| China | USA | China | USA | China | USA | p | |
| China | 200 (100%) | 0 (0%) | 187 (93.5%) | 0 (0%) | 387 (96.7%) | 0 (0%) | 0.000 * |
| USA | 0 (0%) | 200 (100%) | 0 (0%) | 151 (75.5%) | 0 (0%) | 351 (87.7%) | |
| Multiple | 0 (0%) | 0 (0%) | 13 (6.5%) | 49 (24.5%) | 13 (3.3%) | 49 (12.3%) | |
| Publication language | |||||||
| Chinese | 49 (24.5%) | 0 (0%) | 20 (10%) | 0 (0%) | 69 (17.3%) | 0 (0%) | 0.000 * |
| English | 151 (75.5%) | 200 (100%) | 180 (90%) | 200 (100%) | 331 (82.7%) | 400 (100%) | |
| Data source | |||||||
| Primary | 190 (95%) | 139 (69.5%) | 194 (97%) | 164 (82%) | 384 (96%) | 303 (75.7%) | 0.000 * |
| Secondary | 10 (5%) | 61 (30.5%) | 6 (3%) | 36 (18%) | 16 (4%) | 97 (24.3%) | |
| Design | |||||||
| Case series | 13 (6.5%) | 5 (2.5%) | 1 (0.5%) | 3 (1.5%) | 14 (3.5%) | 8 (2.0%) | 0.000 ** |
| Case-control | 39 (19.5%) | 19 (9.5%) | 32 (16%) | 21 (10.5%) | 71 (17.7%) | 40 (10%) | |
| Clinical trial | 14 (7%) | 25 (12.5%) | 11 (5.5%) | 33 (16.5%) | 25 (6.2%) | 58 (14.5%) | |
| Cohort | 12 (6%) | 53 (26.5%) | 23 (11.5%) | 51 (25.5%) | 35 (8.8%) | 104 (26%) | |
| Cross sectional | 24 (12%) | 37 (18.5%) | 29 (14.5%) | 30 (15%) | 53 (13.3%) | 67 (16.7%) | |
| Laboratory-based | 98 (49%) | 61 (30.5%) | 104 (52%) | 62 (31%) | 202 (50.5%) | 123 (30.8%) | |
| Study subjects | |||||||
| Animal | 92 (46%) | 55 (27.5%) | 96 (48%) | 55 (27.5%) | 188 (47%) | 110 (27.5%) | 0.000 ** |
| Bio-sample | 6 (3%) | 5 (2.5%) | 8 (4%) | 6 (3%) | 14 (3.5%) | 11 (2.7%) | |
| Care providers | 0 (0%) | 4 (2%) | 0 (0%) | 1 (0.5%) | 0 (0%) | 5 (1.3%) | |
| Patients | 86 (43%) | 120 (60%) | 85 (42.5%) | 123 (61.5%) | 171 (42.7%) | 243 (60.7%) | |
| Population | 16 (8%) | 12 (6%) | 10 (5%) | 14 (7%) | 26 (6.5%) | 26 (6.5%) | |
| Multiple | 0 (0%) | 3 (1.5%) | 1 (0.5%) | 1 (0.5%) | 1 (0.3%) | 4 (1%) | |
| Other | 0 (0%) | 1 (0.5%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0.3%) | |
| Type of diabetes | |||||||
| Type 1 and 2 | 191 (95.5%) | 172 (86%) | 162 (81%) | 171 (85.5%) | 353 (88.3%) | 343 (85.7%) | 0.221 * |
| Gestational | 4 (2%) | 4 (2%) | 8 (4%) | 4 (2%) | 12 (3%) | 8 (2%) | |
| With other diseases | 5 (2.5%) | 24 (12%) | 30 (15%) | 25 (12.5%) | 35 (8.7%) | 49 (12.3%) | |
| Relevance of the Included Studies | Published in 2010 | Published in 2015 | All | ||||
|---|---|---|---|---|---|---|---|
| China | USA | China | USA | China | USA | p Value | |
| Consequence | 0 (0%) | 2 (1%) | 0 (0%) | 5 (2.5%) | 0 (0%) | 7 (1.7%) | 0.015 ** |
| Diagnosis | 19 (9.5%) | 15 (7.5%) | 12 (6%) | 16 (8%) | 31 (7.7%) | 31 (7.7%) | 1.000 * |
| Disease risk factors | 47 (23.5%) | 29 (14.5%) | 44 (22%) | 30 (15%) | 91 (22.7%) | 59 (14.7%) | 0.005 * |
| Epidemiology | 6 (3%) | 9 (4.5%) | 3 (1.5%) | 7 (3.5%) | 9 (2.3%) | 16 (4%) | 0.222 * |
| Prevention | 1 (0.5%) | 7 (3.5%) | 2 (1%) | 6 (3%) | 3 (0.7%) | 13 (3.3%) | 0.020 * |
| Prognosis | 10 (5%) | 14 (7%) | 14 (7%) | 16 (8%) | 24 (6%) | 30 (7.5%) | 0.481 * |
| Treatment | 84 (42%) | 79 (39.5%) | 85 (42.5%) | 70 (35%) | 169 (42.3%) | 149 (37.3%) | 0.170 * |
| Multiple | 2 (1%) | 0 (0%) | 3 (1.5%) | 3 (1.5%) | 5 (1.3%) | 3 (0.7%) | 0.725 ** |
| Other | 31 (15.5%) | 45 (22.5%) | 37 (18.5%) | 47 (23.5%) | 68 (17%) | 92 (23%) | 0.042 * |
| Type of Interventions | Published in 2010 | Published in 2015 | all | ||||
|---|---|---|---|---|---|---|---|
| China | USA | China | USA | China | USA | p | |
| Behavioral or Educational | 0 (0%) | 12 (6.0%) | 1 (0.5%) | 11 (5.5%) | 1 (0.2%) | 23 (5.8%) | 0.000 * |
| Biological | 8 (4%) | 5 (2.5%) | 6 (3%) | 7 (3.5%) | 14 (3.5%) | 12 (3%) | 0.842 * |
| Diagnostic tests | 10 (5%) | 11 (5.5%) | 12 (6%) | 11 (5.5%) | 22 (5.5%) | 22 (5.5%) | 1.000 * |
| Disease management | 8 (4%) | 34 (17%) | 5 (2.5%) | 19 (9.5%) | 13 (3.3%) | 53 (13.3%) | 0.000 * |
| Pharmacological | 71 (35.5%) | 41 (20.5%) | 75 (37.5%) | 42 (21%) | 146 (36.5%) | 83 (20.7%) | 0.000 * |
| Radiological | 1 (0.5%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0.3%) | 0 (0%) | 1.000 ** |
| Surgical | 4 (2%) | 10 (5%) | 5 (2.5%) | 3 (1.5%) | 9 (2.3%) | 13 (3.3%) | 0.518 * |
| Multiple | 3 (1.5%) | 1 (0.5%) | 0 (0%) | 2 (1%) | 3 (0.7%) | 3 (0.7%) | 1.000 ** |
| NA | 95 (47.5%) | 83 (41.5%) | 93 (46.5%) | 101 (50.5%) | 188 (47%) | 184 (46%) | 0.557 * |
| Other | 0 (0%) | 3 (1.5%) | 3 (1.5%) | 4 (2%) | 3 (0.7%) | 7 (1.7%) | 0.341 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, H.; Bhurke, S.; Jia, G.; Song, F. Differences and Similarities in Diabetes Research between China and the USA. Int. J. Environ. Res. Public Health 2019, 16, 2989. https://doi.org/10.3390/ijerph16162989
Fan H, Bhurke S, Jia G, Song F. Differences and Similarities in Diabetes Research between China and the USA. International Journal of Environmental Research and Public Health. 2019; 16(16):2989. https://doi.org/10.3390/ijerph16162989
Chicago/Turabian StyleFan, Hong, Sheetal Bhurke, Guizhen Jia, and Fujian Song. 2019. "Differences and Similarities in Diabetes Research between China and the USA" International Journal of Environmental Research and Public Health 16, no. 16: 2989. https://doi.org/10.3390/ijerph16162989
APA StyleFan, H., Bhurke, S., Jia, G., & Song, F. (2019). Differences and Similarities in Diabetes Research between China and the USA. International Journal of Environmental Research and Public Health, 16(16), 2989. https://doi.org/10.3390/ijerph16162989