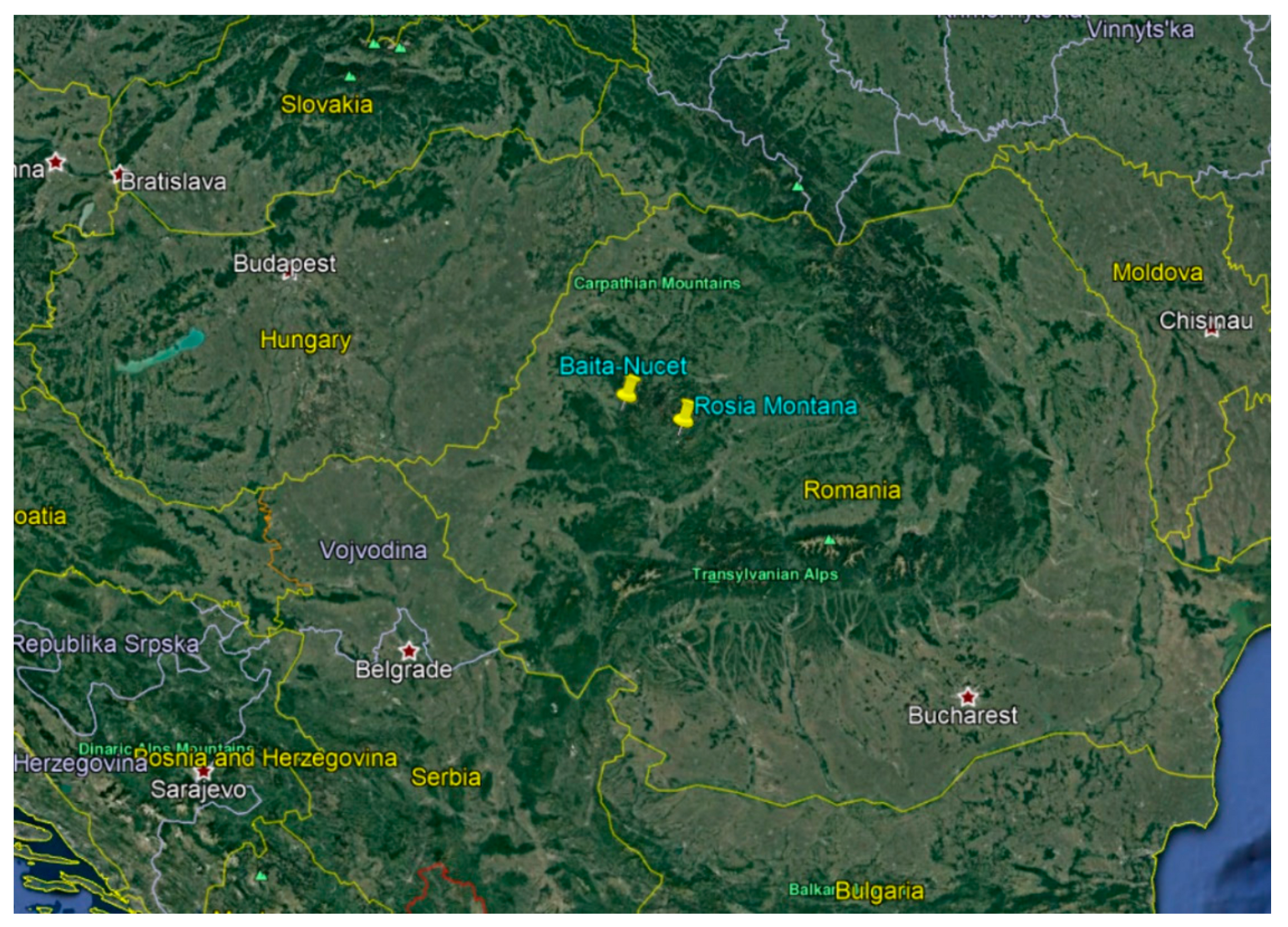
Environmental Factors Associated with Malocclusion in Children Population from Mining Areas, Western Romania

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Occlusal Clinical Signs (Between the Two Jaws)
- Sagittal plan:
- ○
- The presence of neutral report at 6-year molars revealing Angle Class I; neutral (normal) report was recorded when the mesiobuccal cusp of the maxillary first permanent molar occluded with the mesiobuccal groove of the mandibular first permanent molar;
- ○
- The presence of mesial molar occlusion in 6-year molars, for determining Angle Class III; the mesial molar occlusion was recorded when there was deviation of at least one-half cusp width mesially to Class I;
- ○
- The presence of distal molar occlusion in 6-year molars, for determining Angle Class II, was recorded when there was deviation of at least one-half cusp width distally to Class I.
- Transversal plan:
- ○
- The narrowing of the maxillary arch, an indicator for posterior crossbite; posterior crossbite was registered when the buccal cusps of the maxillary premolars and/or molars occluded with the lingual cusps of the opposing mandibular teeth;
- ○
- The narrowing of the mandibular arch, an indicator for scissors bite; scissors bite was registered when any of the maxillary premolars and/or molars totally occluded to the buccal surface of the mandibular antagonists.
- Vertical plan:
- ○
- Vertical inocclusion space, an indicator for posterior open bite.
- Sagittal plan:
- ○
- Positive overjet was recorded if the upper incisors were ahead/in front of the lower incisors;
- ○
- Negative overjet was recorded when the upper incisors were behind the lower incisors.
- Transversal plan:
- ○
- Midline shift was defined as non-coincident upper and lower midlines when the posterior teeth were in contact.
- Vertical plan:
- ○
- Overbite was considered as the vertical overlap of the incisors when the posterior teeth were in contact. An overbite exceeding 1/3 was an indicator for deep bite;
- ○
- Vertical inocclusion space between the incisal edge of the maxillary central incisors and the incisal edge of the corresponding mandibular incisors when the posterior teeth were in contact was an indicator for anterior open bite.
2.2. Space Discrepancies (Inside One Jaw)
- ○
- Crowding was recorded when the total sum of slipped contacts, for the incisor segment, was at least 2 mm;
- ○
- Spacing was recorded when the total spacing was at least 2 mm for the incisor segment.
- Sagittal malocclusions:
- ○
- Angle Class I malocclusion, the occlusion with the following clinical signs: neutral molar report, the anomaly being present at the incisal level;
- ○
- Angle Class II/1 malocclusion, the occlusion with the following clinical signs: distal molar occlusion and positive overjet at the incisal level;
- ○
- Angle Class II/2 malocclusion, the occlusion with the following clinical signs: distal molar occlusion, without overjet at the incisal level;
- ○
- Angle Class III malocclusion, the occlusion with following clinical signs: mesial molar occlusion with or without negative overjet at incisal level.
- Transversal malocclusions: posterior crossbite, scissors bite, midline shift;
- Vertical malocclusions: posterior open bite, anterior open bite, deep bite;
- Space discrepancies: crowding, spacing;
2.3. Ethics Approval and Consent to Participate
3. Results
3.1. Batch Distribution
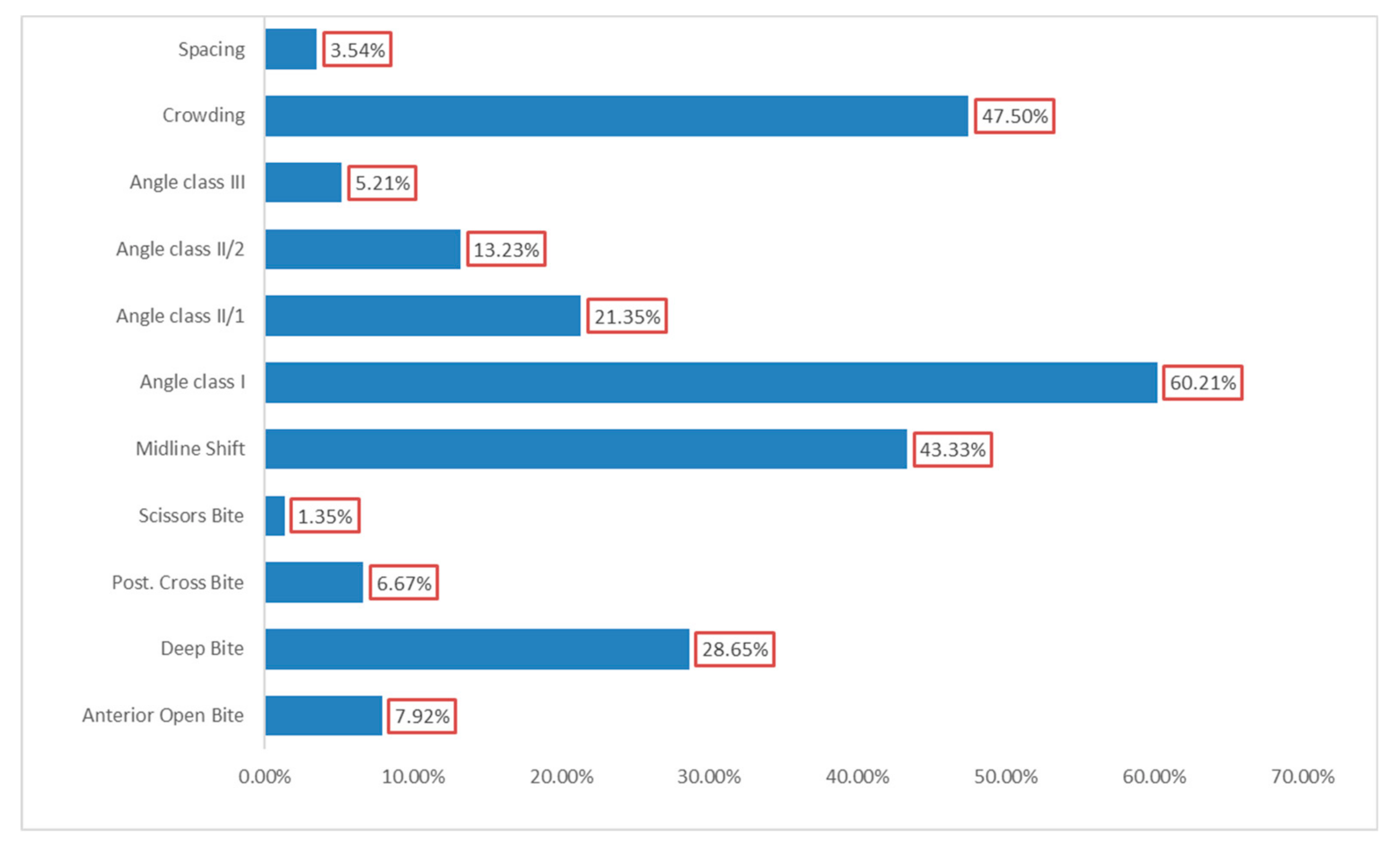
3.2. Prevalence of Malocclusions—Overall Findings
3.3. Distribution of Malocclusion Types by Environmental Factors
4. Discussions
4.1. Overall Findings
4.2. The Distribution of Different Types of Malocclusion According to the Geographical Region
4.3. The Distribution of Different Types of Malocclusion According to Gender
4.4. The Distribution of Different Types of Malocclusion According to Ethnicity
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Walther, D.; Houston, W.; Jones, M.; Oliver, R. Walther and Houston’s Orthodontic Notes, 5th ed.; Butterworth-Heinemann: Oxford, UK, 1994. [Google Scholar]
- Mtaya, M.; Brudvik, P.; Åstrøm, A.N. Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12-to 14-year-old Tanzanian schoolchildren. Eur. J. Orthod. 2009, 31, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Borzabadi-Farahani, A.; Eslamipour, F. Malocclusion and occlusal traits in an urban Iranian population. An epidemiological study of 11 to 14 year-old children. Eur. J. Orthod. 2009, 31, 477–484. [Google Scholar]
- WHO. Oral Health Survey: Basic Method, 3rd ed.; WHO, Oral Health Unit: Geneva, Switzerland, 1987. [Google Scholar]
- Vaida, L.; Todor, B.; Bertossi, D.; Corega, C. Correlations between Stress, Anxiety and Coping Mechanisms in Orthodontic Patients. Iran. J. Public Health 2015, 44, 147–149. [Google Scholar]
- Ţenţ, A.; Todor, L.; Ciavoi, G.; Popovici-Mut, A.; Domocos, D.; Pogan, M.; Vaida, L.; Porumb, A. Non-syndromic hypodontia of permanent dentition associated with other dental 35 anomalies in children and adolescents. Rom. J. Morphol. Embryol. 2018, 59, 879–883. [Google Scholar]
- Zhou, X.; Zhang, Y.; Wang, Y.; Zhang, H.; Chen, L.; Liu, Y. Prevalence of Malocclusion in 3—to 5-Year-Old Children in Shanghai, China. Int. J. Environ. Res. Public Health 2017, 14, 328. [Google Scholar] [CrossRef]
- Alhamadi, M.; Halboub, E.; Salah-Fayed, M.; Labib, A.; El-Saaidi, C. Global distribution of malocclusion traits: A systematic review. Dent. Press J. Orthod. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Hassan, R.; Akb, R. Occlusion, Malocclusion and method of measurements—An overview. Arch. Orofac Sci. 2007, 2, 3–9. [Google Scholar]
- Gudipaneni, R.; Aldameshi, R.; Patil, S.; Alam, M. The prevalence of malocclusion and the need for orthodontic treatment among adolescents in the northern border region of Saudi Arabia: An epidemiological study. BMC Oral Health 2018, 18, 16. [Google Scholar] [CrossRef] [PubMed]
- Hanna, A.; Chaaya, M.; Moukarzel, C.; el Asmar, K.; Jaffa, M.; Ghafari, J. Malocclusion in 55 elementary school children in Beirut: Severity and related social/behavioral factors. Int. J. Dent. 2015, 2015, 351231. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, V.; Ierardo, G.; Corridore, D.; di Carlo, G.; di Giorgio, G.; Leonardi, E.; Campus, G.; Vozza, I.; Polimeni, A.; Bossù, M. Evaluation of the orthodontic treatment need in a paediatric sample from Southern Italy and its importance among paediatricians for improving oral health in pediatric dentistry. J. Clin. Exp. Dent. 2017, 9, 995–1001. [Google Scholar] [CrossRef]
- Thilander, B.; Pena, L.; Infante, C.; Parada, S.; de Mayorga, C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur. J. Orthod. 2001, 23, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Lagana, G.; Masucci, C.; Fabi, F.; Bollero, P.; Cozza, P. Prevalence of malocclusions, oral habits and orthodontic 300 treatment need in a 7-to 15-year-old schoolchildren population in Tirana. Prog. Orthod. 2013, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, R.; Arnautska, H.; Belcheva, A.; Georgieva, M.; Dimitrov, E. Epidemiological study of malocclusions of 5 and 6 years old children from northeastern region of Bulgaria. J. IMAB 2016, 22, 1172–1174. [Google Scholar] [CrossRef]
- Gábris, K.; Márton, S.; Madléna, M. Prevalence of malocclusions in Hungarian adolescents. Eur. J. Orthod. 2006, 28, 467–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorobăţ, V.; Stanciu, D. Ortodonţie şi Ortopedie Dento-Facială; Editura Medicală: Bucharest, Romania, 2011. [Google Scholar]
- Environmental Impact Assessment for Roșia Montană Project. Rosia Montana Gold Corporation. 2006. Available online: http://en.rmgc.ro/rosia-montana-project/environment/environmental-impact-assessment.html (accessed on 15 April 2019).
- Institutul National de Statistica a Romaniei. Recensamantul populatiei din 2011 (Romania). 2011. Available online: http://www.recensamantromania.ro/rezultate-2/ (accessed on 15 April 2019).
- Parekh, N.; Rose, T. Health Inequalities of the Roma in Europe: A Literature Review. Cent. Eur. J. Public Health 2011, 19, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Hajioff, S.; Mckee, M. The health of the Roma people: A review of the published literature. J. Epidemiol. Community Health 2000, 54, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Olau, P.; Filimon, L.; Nemes, V. Integrating strategic approaches into local urban policies. An insight into the urban planning process in Beiuş land, Romania. Rev. Rom. Geogr. Politica 2012, 14, 78–87. [Google Scholar]
- Cosma, C.; Dinu, A.C.; Papp, B.; Moldovan, M.; Begy, R.; Dicu, T.; Nita, D.; Burghele, B.; Fulea, D.; Cindea, C.; et al. Radon Measurements 92 and Radon Remediationa in Baita-Stei Prone Area. Carpath. J. Earth Environ. Sci. 2013, 8, 191–199. [Google Scholar]
- Bai, H.; Hu, B.; Wang, C.; Bao, S.; Sai, G.; Xu, X.; Zhang, S.; Li, Y. Assessment of Radioactive Materials and Heavy Metals in the Surface Soil around the Bayanwula Prospective Uranium Mining Area in China. Int. J. Environ. Res. Public Health 2017, 14, 300. [Google Scholar] [CrossRef]
- Israel, G. Determining the Sample Size (PEOD6); University of Florida: Gainesville, FL, USA, 1992. [Google Scholar]
- Bjoerk, B.; Krebs, R.; Solow, B. A method for epidemiological registration of malocclusion. Acta Odontal. Scand. 1964, 22, 27–41. [Google Scholar] [CrossRef]
- WHO. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Šidlauskas, A.; Lopatienė, K. The prevalence of malocclusion among 7-15-year-old Lithuanian schoolchildren. Medicina 2009, 45, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Abu-Alhaija, E.; Qudeimat, M. Occlusion and tooth/arch dimension in primary dentition of preschool Jordanian children. Int. J. Paediatr. Dent. 2003, 13, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Aikins, E.A.; Onyeaso, C.O. Prevalence of malocclusion and occlusal traits among adolescents and young adults in Rivers State, Nigeria. Odontostomatol Trop. 2014, 37, 5–12. [Google Scholar] [PubMed]
- Bourzgui, F.; Sebbar, M.; Hamza, M.; Lazrak, L.; Abidine, Z.; el Quars, F. Prevalence of malocclusions and orthodontic treatment need in 8 to 12-year-old schoolchildren in Casablanca, Morocco. Prog. Orthod. 2012, 13, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Bugaighis, I.; Karanth, D. The prevalence of malocclusion in urban Libyan schoolchildren. J. Orthod. Sci. 2013, 2, 1–6. [Google Scholar] [CrossRef]
- Kaur, H.; Pavithra, U.; Abraham, R. Prevalence of malocclusion among adolescents in South Indian population. J. Int. Soc. Prev. Community Dent. 2013, 3, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Silva, R.; Kang, D. Prevalence of malocclusion among Latino adolescents. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Chibelean, M.; Jurca, A.; Halitchi, L.G.; Pacurar, M. Statistical study of malocclusion in a population of central Romania region. Int. J. Med. Dent. 2014, 18, 216–221. [Google Scholar]
- Stefanescu, I.; Zetu, I.; Rusu, M. Effect of adverse oral habits on the development of the 323 dentomaxillary system. Rev. Med. Chir. Soc. Med. Nat. Iasi 2011, 115, 567–571. [Google Scholar]
- Al-Emran, S.; Wisth, P.; Boe, O. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent. Oral Epidemiol. 1990, 18, 253–255. [Google Scholar] [CrossRef]
- Christopherson, E.; Briskie, D.; Inglehart, M. Objective, subjective, and self-assessment of 352 preadolescent orthodontic treatment need-a function of age, gender, and ethnic/racial background. J. Public Health Dent. 2009, 69, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Rauten, A.; Olteanu, M.; Maglaviceanu, C.; Popescu, M.; Teodorescu, E.; Surlin, P. Malocclusions assesment in a group of romanian school 361 children with different socio-economic status. Int. J. Med. Dent. 2014, 18, 181–188. [Google Scholar]
- Zegan, G.; Anistoroaiei, D. The statistical study of malocclusion. Rom. J. Oral Rehabil. 2009, 1, 43–49. [Google Scholar]
- Celikoglu, M.; Akpınar, S.; Yavu, I. The pattern of malocclusion in a sample of orthodontic patients from Turkey. Med. Oral Patol. Oral Cir. Bucal 2010, 15, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Tausche, E.; Luck, O.; Harzer, W. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need. Eur. J. Orthod. 2004, 26, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Hollander, C.; Full, C. Midline correction by extraction of the remaining mandibular canine: Myth or reality. ASDC J. Dent. Child. 1992, 59, 207–211. [Google Scholar] [PubMed]
- Todor, B.; Vaida, L.; Scrobota, I. Influence of socio-economic status on caries experience to schoolchildren from mining areas. Human Vet. Med. Int. J. Bioflux Soc. 2014, 6, 140–147. [Google Scholar]
- Dascălu, I.; Diaconu, O.; Gheorghiţă, L.; Amărăscu, M.; Coleş, E.; Tîrcă, T.; Scieciu, M. Contribuţii la studiul comparativ al prevalenţei malocluziei clasa II/1 şi II/2 Angle în arealul Craiovei. Rom. J. Stomatol. 2015, 61, 227–230. [Google Scholar]
- Sayin, M.; Turkkahraman, H. Malocclusion and crowding in an orthodontically referred Turkish population. Angle Orthod. 2003, 74, 635–639. [Google Scholar]
- Tomislav, L. Orofacial analysis on the Adriatic islands: An epidemiological study of malocclusions on Hvar Island. Eur. J. Orthod. 2003, 25, 273–278. [Google Scholar]
- Zlotogora, J. Genetic disorders among Palestinian Arabs: 1. Effects of consanguinity. Am. J. Med. Genet. 1997, 68, 472–475. [Google Scholar] [CrossRef]
- Akbari, M.; Lankarani, K.; Honarvar, B.; Tabrizi, R.; Mirhadi, H.; Moosazadeh, M. Prevalence of malocclusion among Iranian children: A systematic review and meta-analysis. Dent. Res. J. (Isfahan) 2016, 13, 387–395. [Google Scholar]
- Cabrera, L.D.C.; Retamoso, L.B.; Mei, R.M.S.; Tanaka, O. Sagittal and verticalaspects of Class II division 1 subjects according to the respiratorypattern. Dent. Press J. Orthod. 2013, 18, 30–35. [Google Scholar] [CrossRef]
- Graber, W.; Vanarsdall, W. Current Principles and Technique; Mosby: Maryland Heights, MO, USA, 2011. [Google Scholar]
- Grippaudo, C.; Oliva, B.; Greco, A.; Sferra, S.; Deli, R. Relationshipbetween vertical facial patterns and dental arch form in class II malocclusion. Prog. Orthod. 2013, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Cook, B.; Wayne, G.; Valentine, A. Revisiting the evidence on health and health care disparities among the Roma: A systematic review 2003–2012. Int. J. Public Health 2013, 58, 885–911. [Google Scholar] [CrossRef] [PubMed]
- Romero, C.; Scavone-Junior, H.; Garib, D.; Cotrim-Ferreira, F.; Ferreira, R. Breastfeeding and non-nutritive sucking patterns related to the prevalence of anterior open bite in primary dentition. J. Appl. Oral Sci. 2011, 19, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Hermont, A.; Martins, C.; Zina, L.; Auad, S.; Paiva, S.; Pordeus, I. Breastfeeding, Bottle Feeding Practices and Malocclusion in the Primary Dentition: A Systematic Review of Cohort Studies. Int. J. Environ. Res. Public Health 2015, 12, 3133–3151. [Google Scholar] [CrossRef] [Green Version]
- Soh, J.; Sandhman, A.; Chan, Y. Occlusal Status in Asian Male Adults. Angle Orthod. 2005, 75, 814–820. [Google Scholar] [PubMed]
- Erum, G.-E.; Fida, M. Pattern of malocclusion in orthodontic patients: A hospital based study. J. Ayub Med. Coll. Abbottabad 2008, 20, 43–47. [Google Scholar]
- De Stefani, A.; Bruno, G.; Conte, E.; Frezza, A.; Balasso, P.; Gracco, A. Prevalence and patterns of tooth agenesis in Angle class II division 2 malocclusion in Italy: A case-control study. Int. Orthod. 2019, 17, 538–543. [Google Scholar] [CrossRef]
- Van der Linden, F.P. Genetic and environmental factors in dentofacial morphology. Am. J. Orthod. 1966, 52, 576–583. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Results | |||
|---|---|---|---|---|
| Age (years) | Roşia Montană mining area | Băița-Nucet mining area | 10.1 ± 1.9 | |
| Gender | Boys | 391 (46.2%) | 51 (45.1%) | 442 (46%) |
| Girls | 456 (53.8%) | 62 (54.9%) | 518 (54%) | |
| Ethnicity | Romanian | 726 (85.7%) | 110 (97.3%) | 836 (87.1%) |
| Romani | 121 (14.3%) | 3 (2.7%) | 124 (12.9%) | |
| Geographical area | RM mining area | 847 (88.2%) | n/a | 847 (88.2%) |
| B-N mining area | n/a | 113 (11.8%) | 113 (11.8%) | |
| Variables | Values | p-Value |
|---|---|---|
| Total malocclusion | 898 (93.5%) | <0.0001 |
| Without malocclusion | 62 (6.5%) | |
| Roşia Montană mining area | 798 (94.2%) | 0.03 |
| Băița-Nucet mining area | 100 (88.5%) | |
| Girls | 421 (95.2%) | 0.04 |
| Boys | 477 (92.1%) | |
| Romani | 107 (86.3%) | 0.001 |
| Romanians | 791 (94.6%) |
| Variables | Roşia Montană Mining Area | Băița-Nucet Mining Area | p | Girls | Boys | p | Romani/Minority | Romanians/Majority | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Space Anomalies | ||||||||||
| Crowding | 434 (51.2%) | 22 (19.5%) | <0.001 | 220 (49.8%) | 236 (45.6%) | 0.2 | 44 (35.5%) | 412 (49.3%) | 0.006 | |
| Spacing | 25 (3.0%) | 9 (8.0%) | 0.1 | 14 (3.2%) | 20 (3.9%) | 0.6 | - | 34 (4.1) | 0.01 | |
| Vertical Plan | ||||||||||
| Open Bite * | 70 (8.3%) | 6 (5.3%) | 0.4 | 40 (9%) | 36 (6.9%) | 0.007 | 25 (20.2%) | 51 (6.1%) | <0.001 | |
| Deep Bite | 244 (28.8%) | 31 (27.4%) | 145 (32.8%) | 130 (25.1%) | 31 (25%) | 244 (29.2%) | ||||
| Transversal Plan | ||||||||||
| Post. Crossbite | 55 (6.5%) | 9 (8%) | 0.3 | 24 (37.5%) | 40 (62.5%) | 0.004 | 4 (3.2%) | 60 (7.2%) | 0.1 | |
| Scissors Bite | 13 (1.5%) | - | 0.1 | 9 (0.2%) | 7 (0.1%) | 0.6 | 2 (0.1%) | 14 (0.1%) | 1 | |
| Midline Shift | 394 (46.5%) | 22 (19.5%) | <0.001 | 192 (43.4%) | 224 (43.2%) | 1.000 | 44 (35.5%) | 372 (44.5%) | 0.07 | |
| Sagital Plan | ||||||||||
| Angle Class | I | 531 (62.7%) | 47 (41.6%) | <0.001 | 243 (55%) | 335 (64.7%) | <0.001 | 78 (62.9%) | 500 (59.8%) | 0.2 |
| II/1 | 145 (17.1%) | 60 (53.1%) | 120 (27.1%) | 85 (16.4%) | 31 (25%) | 174 (20.8%) | ||||
| II/2 | 123 (14.5%) | 4 (3.5%) | 65 (14.7%) | 62 (12%) | 11 (8.9%) | 116 (13.9%) | ||||
| III | 48 (5.7%) | 2 (1.8%) | 14 (3.2%) | 36 (6.9%) | 4 (3.2%) | 46 (5.5%) | ||||
| Angle Class ** | I | 531 (62.7%) | 47 (41.6%) | <0.001 | 243 (55%) | 335 (64.7%) | <0.001 | 78 (62.9%) | 500 (59.8%) | 0.5 |
| II–III | 316 (37.3%) | 66 (58.4%) | 199 (45%) | 183 (35.3%) | 46 (37.1%) | 336 (40.2%) | ||||
| Variables | B | p | OR | 95% CI | |
|---|---|---|---|---|---|
| Malocclusion | |||||
| Băița-Nucet mining area | −0.95 | 0.005 | 0.38 | 0.19 | 0.74 |
| Romanians/majority | 1.19 | <0.001 | 3.31 | 1.80 | 6.11 |
| Male gender | −0.64 | 0.02 | 0.52 | 0.30 | 0.90 |
| Variables | B | P | OR | 95% CI | |
|---|---|---|---|---|---|
| Crowding | |||||
| N-B mining area | −1.55 | <0.001 | 0.21 | 0.13 | 0.34 |
| Romanians/majority | 0.71 | <0.001 | 2.03 | 1.36 | 3.03 |
| Male gender | −0.24 | 0.07 | 0.78 | 0.60 | 1.02 |
| Midline Shift | |||||
| N-B mining area | −1.32 | <0.001 | 0.26 | 0.16 | 0.43 |
| Romanians/majority | 0.47 | 0.01 | 1.60 | 1.08 | 2.38 |
| Deep Bite | |||||
| Romanians/majority | 1.34 | <0.001 | 3.85 | 2.08 | 7.13 |
| Male gender | −0.09 | 0.7 | 0.90 | 0.53 | 1.54 |
| Angle Class II | |||||
| N-B mining area | 0.84 | <0.001 | 2.32 | 1.55 | 3.47 |
| Male gender | −0.39 | 0.004 | 0.67 | 0.52 | 0.88 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Todor, B.I.; Scrobota, I.; Todor, L.; Lucan, A.I.; Vaida, L.L. Environmental Factors Associated with Malocclusion in Children Population from Mining Areas, Western Romania. Int. J. Environ. Res. Public Health 2019, 16, 3383. https://doi.org/10.3390/ijerph16183383
Todor BI, Scrobota I, Todor L, Lucan AI, Vaida LL. Environmental Factors Associated with Malocclusion in Children Population from Mining Areas, Western Romania. International Journal of Environmental Research and Public Health. 2019; 16(18):3383. https://doi.org/10.3390/ijerph16183383
Chicago/Turabian StyleTodor, Bianca Ioana, Ioana Scrobota, Liana Todor, Alexandra Ioana Lucan, and Luminita Ligia Vaida. 2019. "Environmental Factors Associated with Malocclusion in Children Population from Mining Areas, Western Romania" International Journal of Environmental Research and Public Health 16, no. 18: 3383. https://doi.org/10.3390/ijerph16183383
APA StyleTodor, B. I., Scrobota, I., Todor, L., Lucan, A. I., & Vaida, L. L. (2019). Environmental Factors Associated with Malocclusion in Children Population from Mining Areas, Western Romania. International Journal of Environmental Research and Public Health, 16(18), 3383. https://doi.org/10.3390/ijerph16183383