Sleep Disturbance in Older Patients in the Emergency Department: Prevalence, Predictors and Associated Outcomes


Abstract
:1. Introduction
2. Materials and Methods
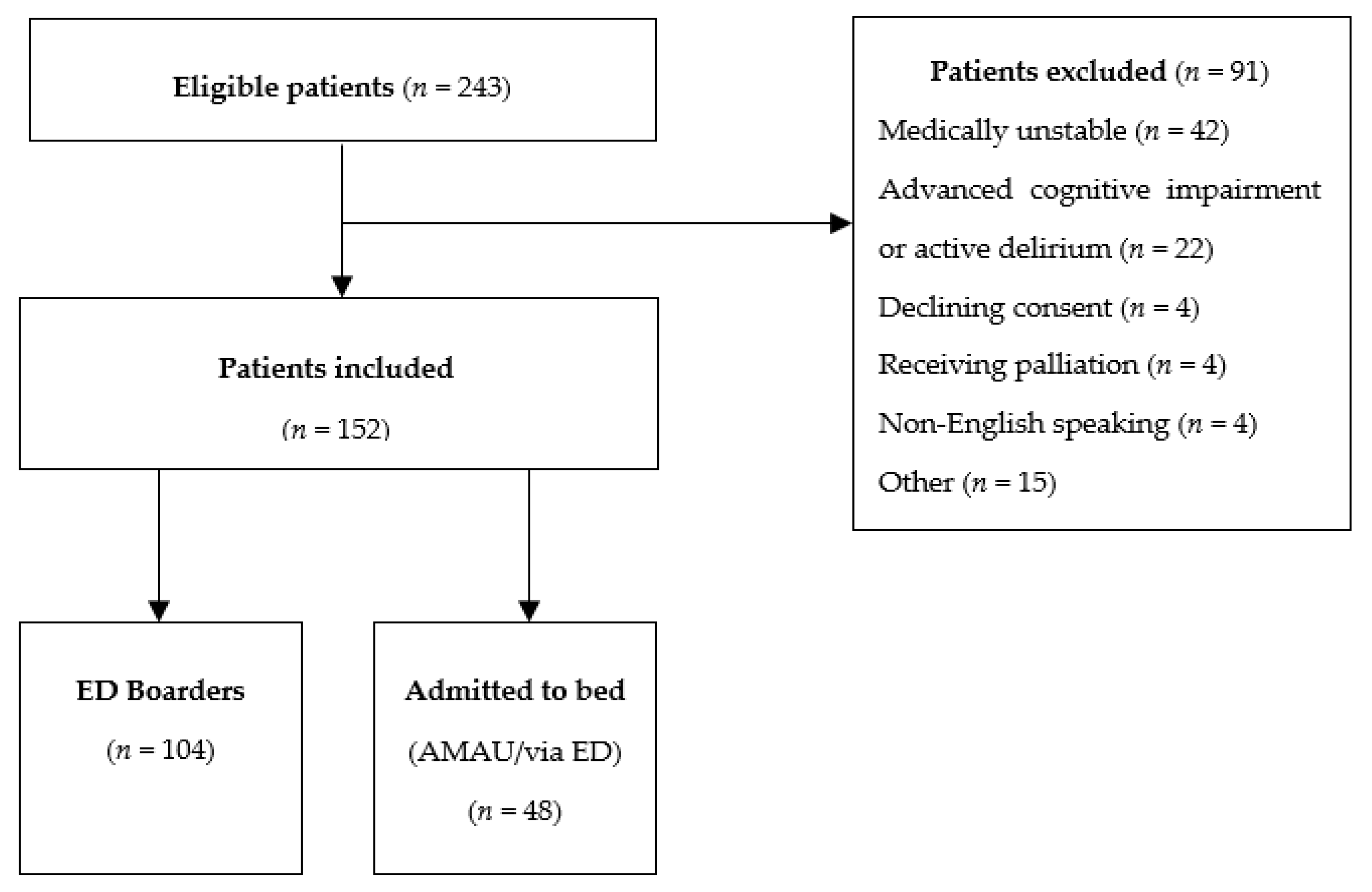
2.1. Patients
2.2. Data Collection
2.3. Sleep Measures
2.4. Other Measures
2.5. Statistical Analysis and Sample Size Calculation
3. Results
3.1. Baseline Characteristics
3.2. ED Boarders
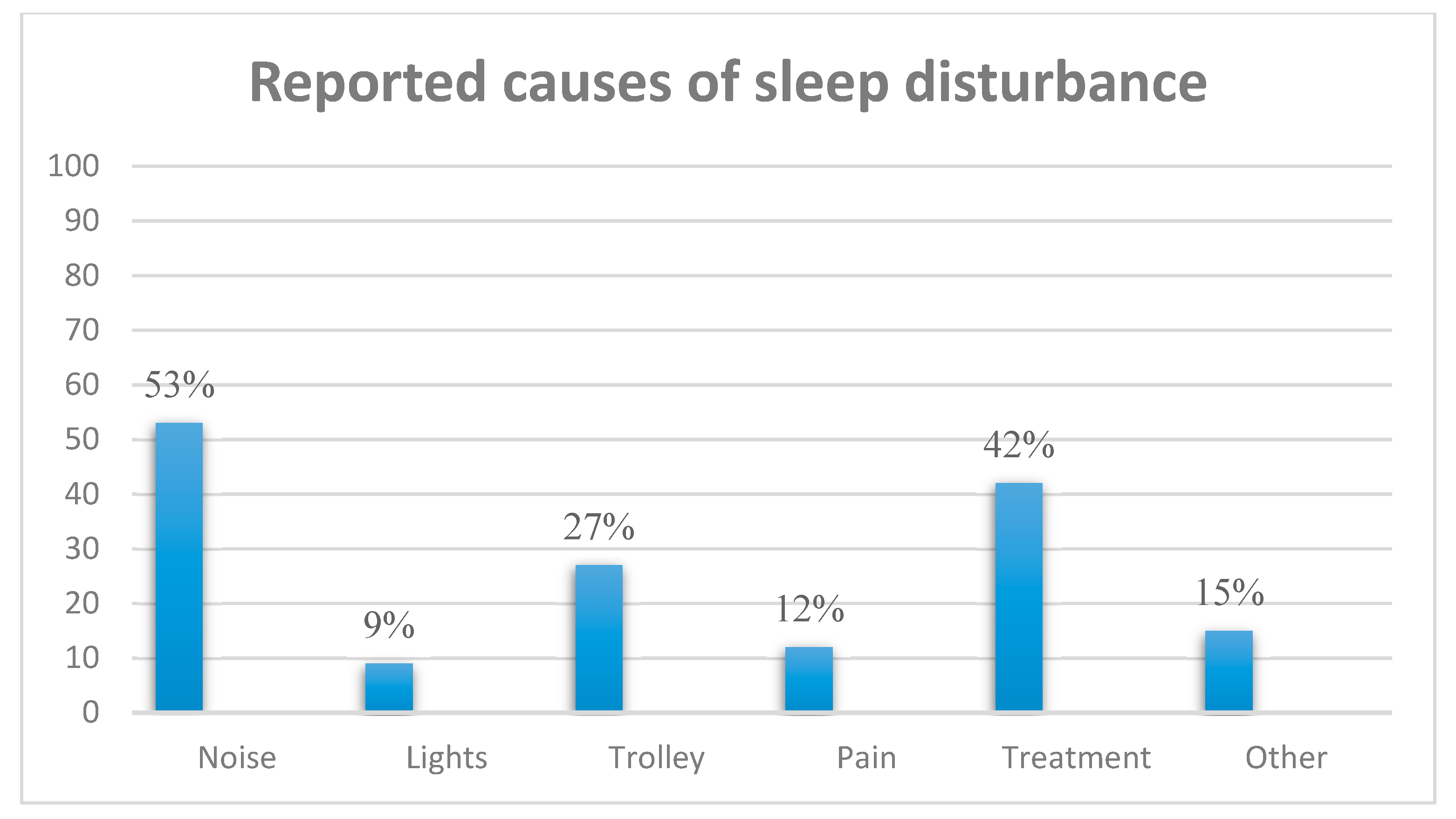
3.3. Prevalence of Sleep Disturbance
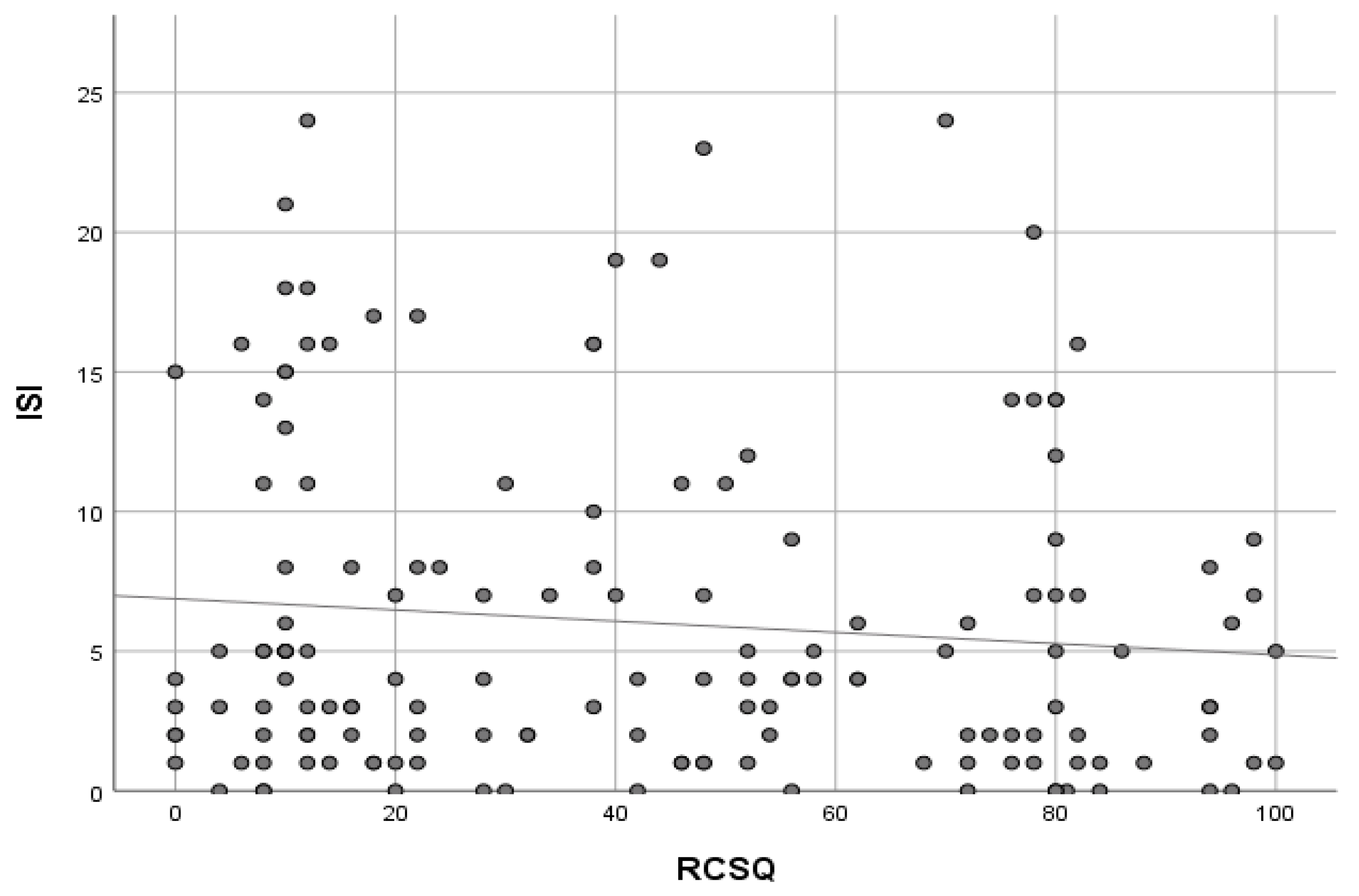
3.4. Sleep and Adverse Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Krueger, P.M.; Friedman, E.M. Sleep duration in the United States: A cross-sectional population-based study. Am. J. Epidemiol. 2009, 169, 1052–1063. [Google Scholar] [CrossRef] [PubMed]
- Neikrug, A.B.; Ancoli-Israel, S. Sleep disorders in the older adult—A mini-review. Gerontology 2010, 56, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Wesselius, H.M.; van den Ende, E.S.; Alsma, J.; Ter Maaten, J.C.; Schuit, S.C.E.; Stassen, P.M.; de Vries, O.J.; Kaasjager, K.H.A.H.; Haak, H.R.; van Doormaal, F.F.; et al. Quality and Quantity of Sleep and Factors Associated with Sleep Disturbance in Hospitalized Patients. JAMA Intern. Med. 2018, 178, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Spira, A.P.; Chen-Edinboro, L.P.; Wu, M.N.; Yaffe, K. Impact of sleep on the risk of cognitive decline and dementia. Curr. Opin. Psychiatry 2014, 27, 478. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Blackwell, T.L.; Redline, S.; Ancoli-Israel, S.; Paudel, M.L.; Cawthon, P.M.; Dam, T.T.; Barrett-Connor, E.; Leung, P.C.; Stone, K.L.; et al. Sleep Disturbances and Frailty Status in Older Community Dwelling Men. J. Am. Geriatr. Soc. 2009, 57, 2085–2093. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Blackwell, T.L.; Redline, S.; Ancoli-Israel, S.; Paudel, M.L.; Cawthon, P.M.; Dam, T.T.; Barrett-Connor, E.; Leung, P.C.; Stone, K.L.; et al. Sleep Disturbances and Risk of Frailty and Mortality in Older Men. Sleep Med. 2012, 13, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Bock, J.O.; König, H.H.; Brenner, H.; Haefeli, W.E.; Quinzler, R.; Matschinger, H.; Saum, K.U.; Schöttker, B.; Heider, D. Associations of frailty with health care costs–results of the ESTHER cohort study. BMC Health Serv. Res. 2016, 16, 128. [Google Scholar] [CrossRef]
- Alhola, P.; Polo-Kantola, P. Sleep deprivation: Impact on cognitive performance. Neuropsychiatr. Dis. Treat. 2007, 3, 553–567. [Google Scholar]
- Lim, J.; Dinges, D.F. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol. Bull. 2010, 136, 375. [Google Scholar] [CrossRef]
- Watson, P.L.; Ceriana, P.; Fanfulla, F. Delirium: Is sleep important? Best Pract. Res. Clin. Anaesthesiol. 2012, 26, 355–366. [Google Scholar] [CrossRef] [Green Version]
- Depner, C.M.; Stothard, E.R.; Wright, K.P., Jr. Metabolic consequences of sleep and circadian disorders. Curr. Diab. Rep. 2014, 14, 507. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflügers Arch. 2012, 463, 121–137. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Cornally, N.; McGlade, C.; Gao, Y.; O’Herlihy, E.; Svendrowski, A.; Clarnette, R.; Lavan, A.H.; Gallagher, P.; Molloy, D.W. Reducing inappropriate prescribing for older adults with advanced frailty: A review based on a survey of practice in four countries. Maturitas 2019, 126, 1–10. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, S.; Musich, S.; Kraemer, S.; Wicker, E. Practical non-pharmacological intervention approaches for sleep problems among older adults. Geriatr. Nurs. 2018, 39, 506–512. [Google Scholar] [CrossRef]
- Medrzycka-Dabrowska, W.; Lewandowska, K.; Kwiecień-Jaguś, K.; Czyż-Szypenbajl, K. Sleep deprivation in Intensive Care Unit–systematic review. Open Med. 2018, 13, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Chauny, J.M.; Paquet, J.; Carrier, J.; Lavigne, G.; Marquis, M.; Cournoyer, A.; Manzini, C.; Daoust, R. Subjective sleep quality and its etiology in the emergency department. Can. J. Emerg. Med. 2019, 21, 249–252. [Google Scholar] [CrossRef]
- ACEM. Statement on Emergency Department Overcrowding, 2006. Available online: https://www. acem.org.au/getattachment/0789ef2f-d814-4e86-af81-aad8b9e57c6d/Statement-on-Emergency-Department-Overcrowding.aspx (accessed on 28 May 2019).
- Gilligan, P.; Winder, S.; Singh, I.; Gupta, V.; Kelly, P.O.; Hegarty, D. The boarders in the emergency department (BED) study. Emerg. Med. J. 2008, 25, 265–269. [Google Scholar] [CrossRef]
- Mackway-Jones, K.; Marsden, J.; Windle, J.; Manchester Triage Group. Emergency Triage, 3rd ed.; BMJ Publishing Group: London, UK, 2014; ISBN 978-1-118-29906-7. [Google Scholar]
- Richards, K.C.; O’Sullivan, P.S.; Phillips, R.L. Measurement of sleep in critically ill patients. J. Nurs. Meas. 2000, 8, 131–144. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar]
- Smyth, C.A. Evaluating Sleep Quality in Older Adults: The Pittsburgh Sleep Quality Index can be used to detect sleep disturbances or deficits. Am. J. Nurs. 2008, 108, 42–50. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [PubMed]
- Kamdar, B.B.; Shah, P.A.; King, L.M.; Kho, M.E.; Zhou, X.; Colantuoni, E.; Collop, N.A.; Needham, D.M. Patient-nurse interrater reliability and agreement of the Richards-Campbell sleep questionnaire. AJCC 2012, 21, 261–269. [Google Scholar] [CrossRef]
- McKinley, S.; Fien, M.; Elliott, R.; Elliott, D. Sleep and psychological health during early recovery from critical illness: An observational study. J. Psychosom. Res. 2013, 75, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Raîche, M.; Hébert, R.; Dubois, M. PRISMA-7: A case-finding tool to identify older adults with moderate to severe disabilities. Arch. Geront. Geriatr. 2008, 47, 9–18. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallis, S.J.; Wall, J.; Biram, R.W.; Romero-Ortuno, R. Association of the clinical frailty scale with hospital outcomes. QJM 2015, 108, 943–949. [Google Scholar] [CrossRef] [Green Version]
- Brazier, J.E.; Walters, S.J.; Nicholl, J.P.; Kohler, B. Using the SF-36 and Euroqol on an elderly population. Qual. Life Res. 1996, 5, 195–204. [Google Scholar] [CrossRef]
- Bellelli, G.; Morandi, A.; Davis, D.H.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, T.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a new instrument for rapid delirium screening: A study in 234 hospitalised older people. Age Ageing 2014, 43, 496–502. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index: A simple index of independence useful in scoring improvement in the rehabilitation of the chronically ill. MD. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Molloy, D.W.; Standish, T.I.; Dubois, S.; Cunje, A. A short screen for depression: The AB Clinician Depression Screen (ABCDS). Int. Psychogeriatr. 2006, 18, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Roffman, C.E.; Buchanan, J.; Allison, G.T. Charlson comorbidities index. J. Physiol. 2016, 62, 171. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Gao, Y.; Svendovski, A.; Gallagher, P.; Eustace, J.; Molloy, D.W. Comparing approaches to optimize cut-off scores for short cognitive screening instruments in mild cognitive impairment and dementia. J. Alzheimer’s Dis. 2017, 57, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Jaussent, I.; Dauvilliers, Y.; Ancelin, M.L.; Dartigues, J.F.; Tavernier, B.; Touchon, J.; Ritchie, K.; Besset, A. Insomnia symptoms in older adults: Associated factors and gender differences. Am. J. Geriatr. Psychiatry. 2011, 19, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Naing, L.; Winn, T.; Rusli, B.N. Practical Issues in Calculating the Sample Size for Prevalence Studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Gnjidic, D.; Hilmer, S.N.; Blyth, F.M.; Naganathan, V.; Waite, L.; Seibel, M.J.; McLachlan, A.J.; Cumming, R.G.; Handelsman, D.J.; Le Couteur, D.G. Polypharmacy cutoff and outcomes: Five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. J. Clin. Epidemiol. 2012, 65, 989–995. [Google Scholar] [CrossRef]
- Filus, W.; de Lacerda, A.B.M.; Albizu, E. Ambient noise in emergency rooms and its health hazards. Int. Arch. Otorhinolaryngol. 2015, 19, 205–209. [Google Scholar] [CrossRef]
- Orellana, D.; Busch-Vishniac, I.J.; West, J.E. Noise in the adult emergency department of Johns Hopkins Hospital. J. Acoust. Soc. Am. 2007, 121, 1996–1999. [Google Scholar] [CrossRef]
- Lei, Z.; Qiongjing, Y.; Qiuli, W.; Sabrina, K.; Xiaojing, L.; Changli, W. Sleep quality and sleep disturbing factors of inpatients in a Chinese general hospital. J. Clin. Nurs. 2009, 18, 2521–2529. [Google Scholar] [CrossRef]
- Ho, A.; Raja, B.; Waldhorn, R.; Baez, V.; Mohammed, I. New onset of insomnia in hospitalized patients in general medical wards: Incidence, causes, and resolution rate. J. Community Hosp. Intern. Med. Perspect. 2017, 7, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, L.; Dobrinas, M.; Tagan, D.; Sautebin, A.; Blanc, A.L.; Widmer, N. Prescription of sedative drugs during hospital stay: A Swiss prospective study. Drugs-Real World Outcomes 2017, 4, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Spira, A.P.; Beaudreau, S.A.; Stone, K.L.; Kezirian, E.J.; Lui, L.Y.; Redline, S.; Ancoli-Israel, S.; Ensrud, K.; Stewart, A. Reliability and validity of the Pittsburgh Sleep Quality Index and the Epworth Sleepiness Scale in older men. J. Geront. Ser. A Biomed. Sci. Med. Sci. 2011, 67, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Beaudreau, S.A.; Spira, A.P.; Stewart, A.; Kezirian, E.J.; Lui, L.Y.; Ensrud, K.; Redline, S.; Ancoli-Israel, S.; Stone, K.L.; Study of Osteoporotic Fractures. Validation of the Pittsburgh Sleep Quality Index and the Epworth Sleepiness Scale in older black and white women. Sleep Med. 2012, 13, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, N. Self-reports: How the questions shape the answers. Am. Psychol. 1999, 54, 93–105. [Google Scholar] [CrossRef]
- Krumholz, H.M. Post-hospital syndrome—An acquired, transient condition of generalized risk. NEJM 2013, 368, 100–102. [Google Scholar] [CrossRef]
- Gilligan, P.; Joseph, D.; Bartlett, M.; Morris, A.; Mahajan, A.; McHugh, K.; Hillary, F.; O’Kelly, P. The ‘who are all these people?’ study. Emerg. Med. J. 2015, 32, 109–111. [Google Scholar] [CrossRef]
- Norton, C.; Flood, D.; Brittin, A.; Miles, J. Improving sleep for patients in acute hospitals. Nurs. Stand. 2015, 29, 35–42. [Google Scholar] [CrossRef]
- DuBose, J.R.; Hadi, K. Improving inpatient environments to support patient sleep. Int. J. Qual. Health Care 2016, 28, 540–553. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 152) | ‘Direct’ to Bed (Including AMAU) (n = 48) | ED Boarder (n = 104) | p = X |
|---|---|---|---|---|
| Age (years) Median ± IQR | 80 (84 − 74= ± 10) | 81.5 (86 − 76 = ± 10) | 79 (83 − 74 = ± 9) | p = 0.11 |
| Gender (% M) | 61% | 73% | 57% | p = 0.49 |
| Polypharmacy (% ≥ Five medications) | 86% | 87.5% | 85% | p = 0.64 |
| Manchester Triage Score Median ± IQR | 3 (3 − 3 = ± 0) | 3 (3 − 3 = ± 0) | 3 (3 − 3 = ± 0) | p = 0.82 |
| RCSQ Median ± IQR (Poor sleep overnight < 70) | 40 (75 − 12 = ± 63) | 71 (80 − 46 = ± 34) | 23 (55 − 10 = ± 45) | p ≤ 0.001 |
| PSQI score Median ± IQR (Poor sleep quality at baseline ≥5 ) | 7 (11 − 4 = ± 7) | 7.5 (11 − 4 = ± 9) | 7 (11 − 4 = ± 7) | p = 0.73 |
| ISI score Median ± IQR (Insomnia at baseline ≥15) | 4 (8 − 2 = ± 6) | 4 (9 − 2 = ± 7)s | 4 (8 − 2=±6) | p = 0.79 |
| Euroqol EQ-5D VAS (QoL) Median ± IQR | 70 (80 − 58 = ± 22) | 72.5 (80 − 60 = ± 20) | 70 (80 − 50 = ± 30) | p = 0.06 |
| Barthel Index Median ± IQR | 19 (20 − 15 = ± 5) | 18 (20 − 1 5= ± 5) | 19 (20 − 15 = ± 5) | p = 0.61 |
| 4AT Median ± IQR | 0 (1 − 0 = ± 1) | 0 (0 − 0 = ± 0) | 0 (0 − 0 = ± 0) | p = 0.84 |
| ABC Depression Score Median ± IQR | 0 (0 − 0 = ± 0) | 0 (0 − 0 = ± 0) | 0 (0 − 0 = ± 0) | p = 0.89 |
| PRISMA-7 Median ± IQR | 4 (6 − 2 = ± 4) | 4 (6 − 3 = ± 3) | 4 (5 − 2 = ± 3) | p = 0.17 |
| Charlson Co-morbidity Index Median ± IQR | 6 (7 − 5 = ± 2) | 6 (8 − 5 = ± 3) | 6 (7 − 5 = ± 2) | p = 0.29 |
| Clinical Frailty Scale Median ± IQR (% Frail: CFS ≥ 5 - at assessment) | 4 (5 − 3 = ± 2) (43%) | 5 (5 − 3 = ± 2) (49%) | 4 (5 − 3 = ± 2) (42%) | p = 0.29 |
| Variable | OR | 95% Confidence Interval | p = x |
|---|---|---|---|
| Age | 1.05 | 0.98–1.13 | 0.14 |
| Barthel Index | 0.99 | 0.85–1.15 | 0.88 |
| Boarder in ED | 4.36 | 1.67–11.4 | 0.003 |
| Clinical Frailty Scale | 0.69 | 0.40-1.19 | 0.18 |
| Charlson Co-Morbidity Index | 0.90 | 0.63–1.30 | 0.59 |
| Use of hypnotic medications | 0.40 | 0.10–1.67 | 0.21 |
| Gender (male) | 0.90 | 0.36–2.26 | 0.83 |
| Insomnia Severity Index | 1.00 | 0.92–1.09 | 0.96 |
| Manchester Triage System score | 1.79 | 0.53–6.05 | 0.35 |
| Pittsburgh Sleep Quality Index | 2.41 | 0.78–7.87 | 0.15 |
| 4 AT score | 0.93 | 0.69–1.26 | 0.64 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannion, H.; Molloy, D.W.; O’Caoimh, R. Sleep Disturbance in Older Patients in the Emergency Department: Prevalence, Predictors and Associated Outcomes. Int. J. Environ. Res. Public Health 2019, 16, 3577. https://doi.org/10.3390/ijerph16193577
Mannion H, Molloy DW, O’Caoimh R. Sleep Disturbance in Older Patients in the Emergency Department: Prevalence, Predictors and Associated Outcomes. International Journal of Environmental Research and Public Health. 2019; 16(19):3577. https://doi.org/10.3390/ijerph16193577
Chicago/Turabian StyleMannion, Helen, D. William Molloy, and Rónán O’Caoimh. 2019. "Sleep Disturbance in Older Patients in the Emergency Department: Prevalence, Predictors and Associated Outcomes" International Journal of Environmental Research and Public Health 16, no. 19: 3577. https://doi.org/10.3390/ijerph16193577