Differences in Insomnia Symptoms between Immigrants and Non-Immigrants in Switzerland attributed to Emotional Distress: Analysis of the Swiss Health Survey

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Co-Variates
2.4. Data Analysis
3. Results
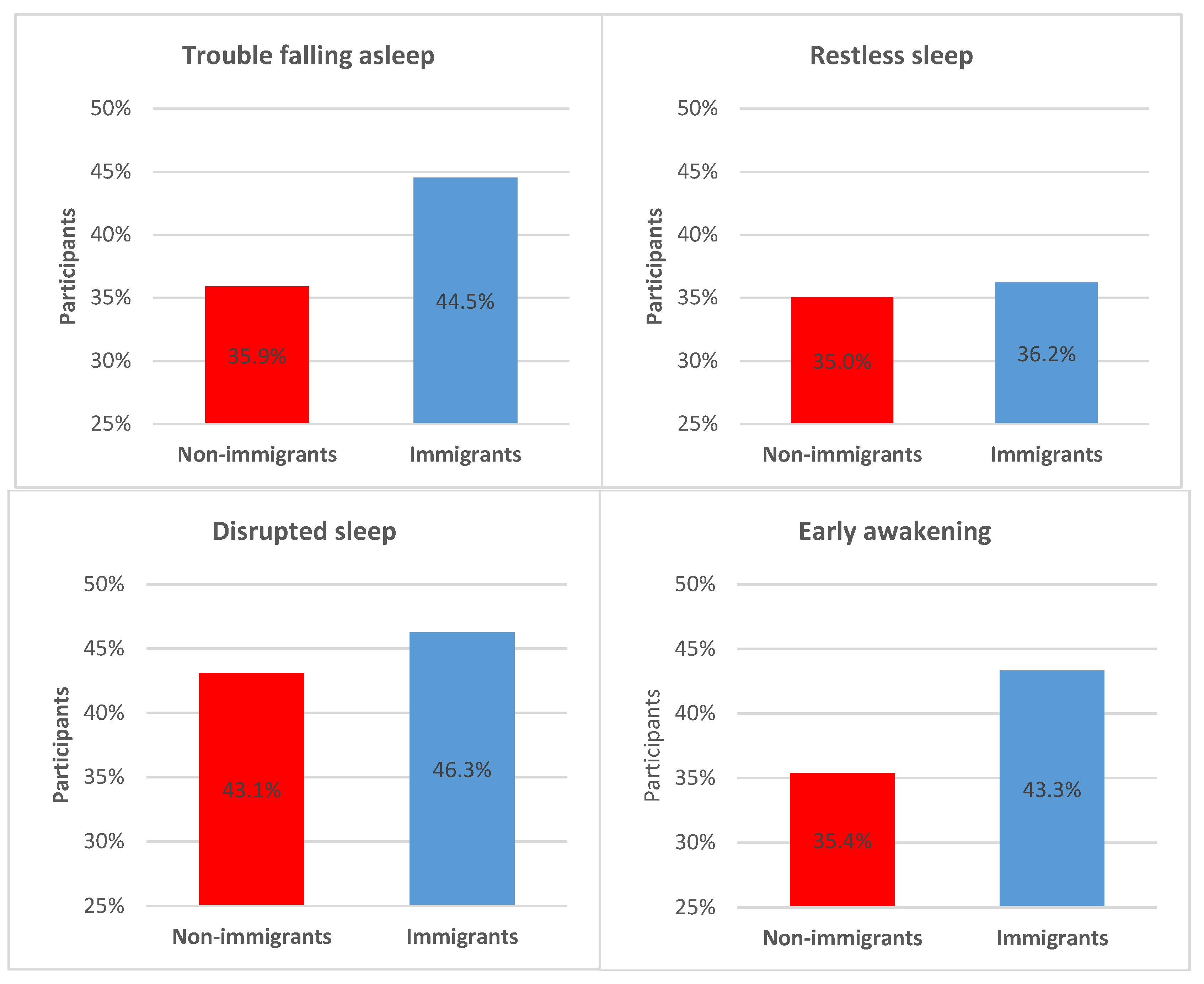
3.1. Descriptive Statistics
3.2. Inferential Statistics
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Migration Report 2015; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2016.
- UNHCR. Worldwide Displacement Hits All-Time High as War and Persecution Increase. Available online: http://www.unhcr.org/558193896.html (accessed on 4 March 2016).
- Migration and Migrant Population Statistics. Available online: http://ec.europa.eu/eurostat/statistics-explained/pdfscache/1275.pdf (accessed on 17 October 2017).
- BFS Migration and Integration—Data, Indicators: Population by Migration Status. Available online: https://www.bfs.admin.ch/bfs/en/home/statistics/population/migration-integration/by-migration-status.html (accessed on 15 January 2019).
- BFS Migration and Integration—Data, Indicators: Population by Place of Birth. Available online: https://www.bfs.admin.ch/bfs/en/home/statistics/population/migration-integration/by-place-birth.html (accessed on 15 January 2019).
- WHO. Health of Migrants Report by the Secretariat. Available online: http://www.who.int/iris/handle/10665/23467 (accessed on 15 January 2019).
- Lara, M.; Gamboa, C.; Kahramanian, M.I.; Morales, L.S.; Hayes Bautista, D.E. Acculturation and Latino health in the United States: A review of the literature and its sociopolitical context. Annu. Rev. Public Health 2005, 26, 367–397. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, A.; Wanner, P. The self-reported health of immigrant groups in Switzerland. J. Immigr. Minor. Health 2008, 10, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Knipscheer, J.W.; Kleber, R.J. Help-seeking attitudes and utilization patterns for mental health problems of Surinamese migrants in the Netherlands. J. Couns. Psychol. 2001, 48, 28. [Google Scholar] [CrossRef]
- Voss, U.; Tuin, I. Integration of immigrants into a new culture is related to poor sleep quality. Health Qual. Life Outcomes 2008, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Maneze, D.; DiGiacomo, M.; Salamonson, Y.; Descallar, J.; Davidson, P.M. Facilitators and barriers to health-seeking behaviours among Filipino migrants: Inductive analysis to inform health promotion. Biomed. Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Seixas, A.A.; Nunes, J.V.; Airhihenbuwa, C.O.; Williams, N.J.; Pandi-Perumal, S.R.; James, C.C.; Jean-Louis, G. Linking emotional distress to unhealthy sleep duration: Analysis of the 2009 National Health Interview Survey. Neuropsychiatr. Dis. Treat. 2015, 11, 24–25. [Google Scholar] [CrossRef] [PubMed]
- Moussa, J.S.; Pecoraro, M.; Ruedin, D.; Houmard, S. The Gender Gap in Mental Health: Immigrants in Switzerland. In Women’s Mental Health; Springer: Cham, Switzerland, 2015; pp. 217–231. [Google Scholar]
- Rumpf, H.-J.; Meyer, C.; Hapke, U.; John, U. Screening for mental health: Validity of the MHI-5 using DSM-IV Axis I psychiatric disorders as gold standard. Psychiatry Res. 2001, 105, 243–253. [Google Scholar] [CrossRef]
- Drapeau, A.; Marchand, A.; Beaulieu-Prévost, D. Epidemiology of psychological distress. Ment. Illn. Underst. Predict. Control 2011, 134–155. [Google Scholar]
- BFS. Die Schweizerische Gesundheitsbefragung 2007 in Kürze-Konzept, Methode, Durchführung; Bundesamt für Statistik: Neuchâtel, Switzerland, 2013. [Google Scholar]
- Kelly, M.J.; Dunstan, F.D.; Lloyd, K.; Fone, D.L. Evaluating cutpoints for the MHI-5 and MCS using the GHQ-12: A comparison of five different methods. BMC psychiatry 2008, 8, 10. [Google Scholar] [CrossRef]
- SPSS. SPSS for Windows (version 24.0). SPSS. Inc.: Chicago, IL, USA, 2016. [Google Scholar]
- Seixas, A.A.; Auguste, E.; Butler, M.; James, C.; Newsome, V.; Auguste, E.; da Silva Fonseca, V.A.; Schneeberger, A.; Zizi, F.; Jean-Louis, G. Differences in short and long sleep durations between blacks and whites attributed to emotional distress: Analysis of the National Health Interview Survey in the United States. Sleep Health 2016. [Google Scholar] [CrossRef]
- Aichberger, M.; Bromand, Z.; Montesinos, A.H.; Temur-Erman, S.; Mundt, A.; Heinz, A.; Rapp, M.; Schouler-Ocak, M. Socio-economic status and emotional distress of female Turkish immigrants and native German women living in Berlin. Eur. Psychiatry 2012, 27, S10–S16. [Google Scholar] [CrossRef]
- Bromand, Z.; Temur-Erman, S.; Yesil, R.; Montesinos, A.H.; Aichberger, M.; Kleiber, D.; Schouler-Ocak, M.; Heinz, A.; Kastrup, M.; Rapp, M. Mental health of Turkish women in Germany: Resilience and risk factors. Eur. Psychiatry 2012, 27, S17–S21. [Google Scholar] [CrossRef]
- Llácer, A.; Zunzunegui, M.V.; del Amo, J.; Mazarrasa, L.; Bolůmar, F. The contribution of a gender perspective to the understanding of migrants’ health. J. Epidemiol. Community Health 2007, 61, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Mewes, R.; Skoluda, N.; Strahler, J.; Nater, U. Psychobiological impact of ethnic discrimination in Turkish immigrants living in Germany. Psychoneuroendocrinology 2015, 61, 71–72. [Google Scholar] [CrossRef]
- Buckley, T.M.; Schatzberg, A.F. On the interactions of the hypothalamic-pituitary-adrenal (HPA) axis and sleep: Normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J. Clin. Endocrinol. Metab. 2005, 90, 3106–3114. [Google Scholar] [CrossRef]
- McDonald, J.T.; Kennedy, S. Insights into the ‘healthy immigrant effect’: Health status and health service use of immigrants to Canada. Soc. Sci. Med. 2004, 59, 1613–1627. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.R.; Seixas, A.; Dib, S.I. Obstructive sleep apnea and stroke: Links to health disparities. Sleep Health 2015, 1, 244–248. [Google Scholar] [CrossRef]
- Grandner, M.A.; Jackson, N.J.; Izci-Balserak, B.; Gallagher, R.A.; Murray-Bachmann, R.; Williams, N.J.; Patel, N.P.; Jean-Louis, G. social and behavioral determinants of perceived insufficient sleep. Front. Neurol. 2015, 6. [Google Scholar] [CrossRef]
- SEM Migration Report; State Secretariat for Migration: Bern, Switzerland, 2014.



{kind=link}
{kind=link}
| Variables | Immigrants | Non-Immigrants | |||
|---|---|---|---|---|---|
| Sociodemographic variables | n | n | p-value | ||
| Gender (%) | 0.540 | ||||
| Females | 1815 | (53.3%) | 7675 | (52.7%) | |
| Males | 1591 | (46.7%) | 6887 | (47.3%) | |
| Age (SD) | 47.6 | (15.8) | 48.6 | (18.8) | 0.001 |
| Marital status (%) | <0.001 | ||||
| Single | 914 | (22.1%) | 5257 | (32.4%) | |
| Married | 2583 | (62.4%) | 8465 | (52.1%) | |
| Registered partners | 12 | (0.3%) | 37 | (0.2%) | |
| Separated | 77 | (1.9%) | 165 | (1.0%) | |
| Divorced | 386 | (9.3%) | 1313 | (8.1%) | |
| Widowed | 167 | (5.7%) | 999 | (6.1%) | |
| Others | 0 | (0.0%) | 3 | (0.0%) | |
| Monthly household income Swiss francs (SD) | 4752 | (6400) | 4981 | (6425) | <0.001 |
| Clinical variables | Immigrants | Non-immigrants | |||
| Health variables | |||||
| Emotional distress rating (SD) | 19.4 | (16.7) | 15.5 | (13.9) | <0.001 |
| BMI kg/m2 (SD) | 24.8 | (4.8) | 24.3 | (5.0) | <0.001 |
| n | n | p-value | |||
| Arterial hypertension (%) | 466 | (13.3) | 2391 | (16.4) | <0.001 |
| Heart disease (%) | 48 | (1.4) | 260 | (1.8) | 0.128 |
| Cancer (%) | 93 | (2.9) | 424 | (2.9) | 0.569 |
| Diabetes mellitus (%) | 150 | (4.4) | 653 | (4.5) | 0.838 |
| Continent of Origin | Females | Males | ||
|---|---|---|---|---|
| n | % | n | % | |
| Continent | ||||
| Europe | 1531 | 84.35% | 1396 | 87.74% |
| North and South America | 156 | 8.60% | 75 | 4.71% |
| Africa | 84 | 4.63% | 83 | 5.22% |
| Asia | 40 | 2.20% | 35 | 2.20% |
| Australia and Oceania | 4 | 0.22% | 2 | 0.13% |
| Years since immigration | ||||
| 20 years or more | 950 | 52.34% | 831 | 52.23% |
| 10–19 years | 399 | 21.98% | 294 | 18.48% |
| 5–9 years | 240 | 13.22% | 247 | 15.52% |
| 0–4 years | 226 | 12.45% | 219 | 13.76% |
| Variables | OR | 95% CI | |
|---|---|---|---|
| Model 1 | Immigrant status | 1.209 | [1.109, 1.319] * |
| Emotional distress | 3.718 | [3.431, 4.028] * | |
| Model 1a | Immigrant status | 1.208 | [1.103, 1.323] * |
| Emotional distress | 3.577 | [3.267, 3.918] * | |
| Immigrant status × emotional distress | 1.096 | [1.040, 1.154] ** | |
| Model 2 | Immigrant status | 1.196 | [1.091, 1.312] * |
| Emotional distress | 3.608 | [3.294, 3.952] * | |
| Immigrant status × emotional distress | 1.097 | [1.041, 1.155] * | |
| Model 3 | Immigrant status | 1.255 | [1.143, 1.377] * |
| Emotional distress | 3.522 | [3.214, 3.859] * | |
| Immigrant status × emotional distress | 1.093 | [1.039, 1.151] ** | |
| Model 4 | Immigrant status | 1.277 | [1.163, 1.402] * |
| Emotional distress | 3.478 | [3.173, 3.812] * | |
| Immigrant status × emotional distress | 1.096 | [1.041, 1.153] * |
| Variables | OR | 95% CI | |
|---|---|---|---|
| Model 1 | Immigrant status | 1.181 | [1.052, 1.325] * |
| Emotional distress | 3.606 | [3.251, 4.001] ** | |
| Model 1a | Immigrant status | 1.181 | [1.049, 1.328] * |
| Emotional distress | 3.557 | [3.186, 3.972] ** | |
| Immigrant status × emotional distress | 1.045 | [0.978, 1.116] | |
| Model 2 | Immigrant status | 1.144 | [1.016, 1.289] * |
| Emotional distress | 3.576 | [3.202, 3.993] ** | |
| Immigrant status × emotional distress | 1.046 | [0.979, 1.117] | |
| Model 3 | Immigrant status | 1.210 | [1.073, 1.366] * |
| Emotional distress | 3.524 | [3.155, 3.936] ** | |
| Immigrant status × emotional distress | 1.040 | [0.974, 1.111] | |
| Model 4 | Immigrant status | 1.229 | [1.089, 1.387] * |
| Emotional distress | 3.524 | [3.155, 3.937] ** | |
| Immigrant status × emotional distress | 1.041 | [0.974, 1.111] |
| Variables | OR | 95% CI | |
|---|---|---|---|
| Model 1 | Immigrant status | 1.252 | [1.098, 1.429] * |
| Emotional distress | 3.660 | [3.222, 4.157] ** | |
| Model 1a | Immigrant status | 1.246 | [1.082, 1.434] ** |
| Emotional distress | 3.325 | [2.832, 3.903] ** | |
| Immigrant status × emotional distress | 1.169 | [1.075, 1.271] * | |
| Model 2 | Immigrant status | 1.229 | [1.065, 1.418] * |
| Emotional distress | 3.320 | [2.826, 3.899] ** | |
| Immigrant status × emotional distress | 1.172 | [1.078, 1.274] ** | |
| Model 3 | Immigrant status | 1.319 | [1.141, 1.525] ** |
| Emotional distress | 3.326 | [2.828, 3.911] ** | |
| Immigrant status × emotional distress | 1.175 | [1.081, 1.276] ** | |
| Model 4 | Immigrant status | 1.346 | [1.164, 1.556] ** |
| Emotional distress | 3.285 | [2.794, 3.861] ** | |
| Immigrant status × emotional distress | 1.169 | [1.077, 1.269] ** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schneeberger, A.R.; Seixas, A.; Schweinfurth, N.; Lang, U.E.; Cajochen, C.; Bux, D.A.; Richards, S.; Jean-Louis, G.; Huber, C.G. Differences in Insomnia Symptoms between Immigrants and Non-Immigrants in Switzerland attributed to Emotional Distress: Analysis of the Swiss Health Survey. Int. J. Environ. Res. Public Health 2019, 16, 289. https://doi.org/10.3390/ijerph16020289
Schneeberger AR, Seixas A, Schweinfurth N, Lang UE, Cajochen C, Bux DA, Richards S, Jean-Louis G, Huber CG. Differences in Insomnia Symptoms between Immigrants and Non-Immigrants in Switzerland attributed to Emotional Distress: Analysis of the Swiss Health Survey. International Journal of Environmental Research and Public Health. 2019; 16(2):289. https://doi.org/10.3390/ijerph16020289
Chicago/Turabian StyleSchneeberger, Andres R., Azizi Seixas, Nina Schweinfurth, Undine E. Lang, Christian Cajochen, Donald A. Bux, Shannique Richards, Girardin Jean-Louis, and Christian G. Huber. 2019. "Differences in Insomnia Symptoms between Immigrants and Non-Immigrants in Switzerland attributed to Emotional Distress: Analysis of the Swiss Health Survey" International Journal of Environmental Research and Public Health 16, no. 2: 289. https://doi.org/10.3390/ijerph16020289