The SED-GIH: A Single-Item Question for Assessment of Stationary Behavior—A Study of Concurrent and Convergent Validity

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Design
2.2. Self-Reported Stationary Behavior
2.3. Accelerometer
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
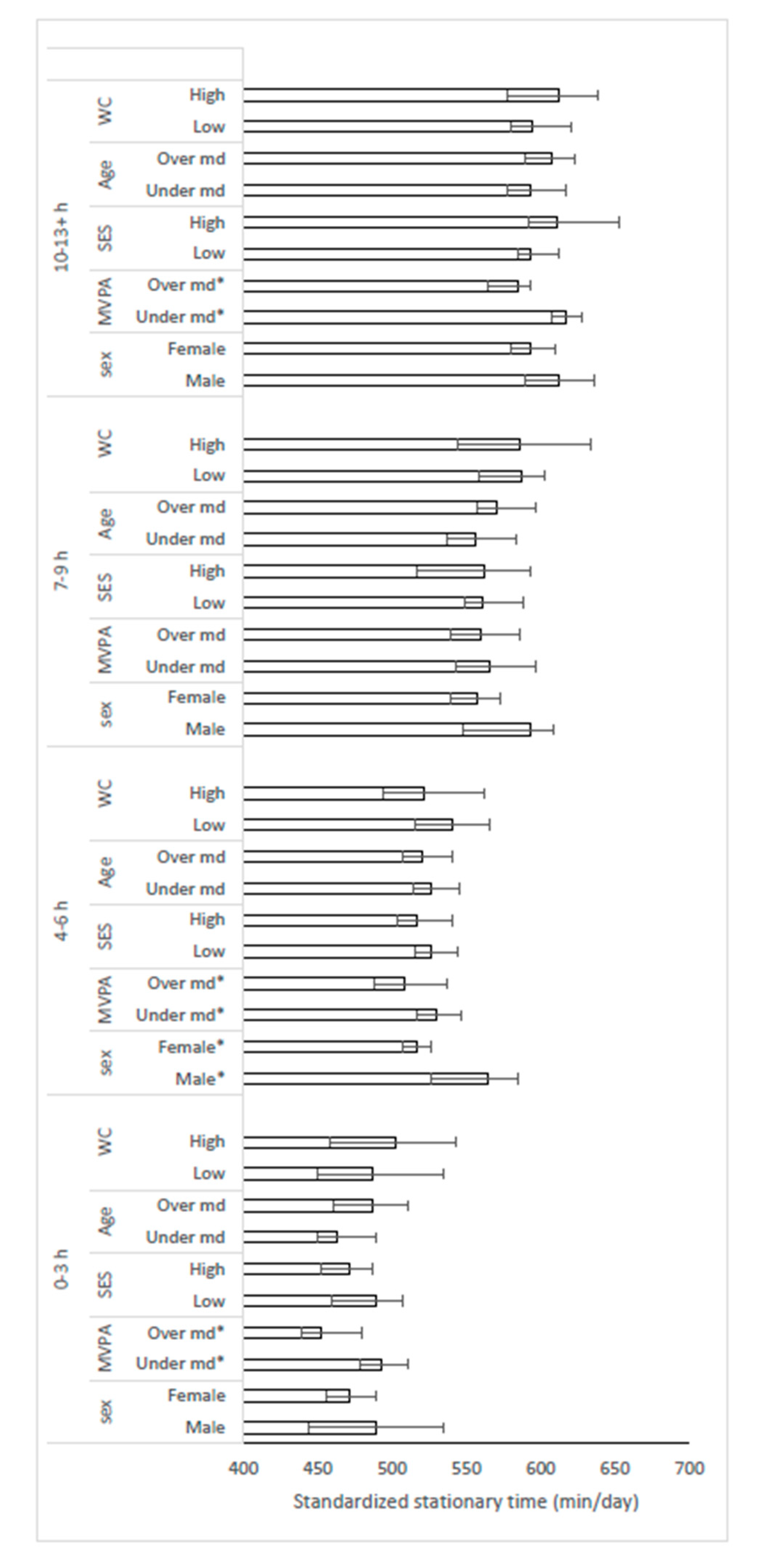
3.2. Concurrent Validity of SED-GIH Using Accelerometer as Reference
3.3. Convergent Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pandey, A.; Salahuddin, U.; Garg, S.; Ayers, C.; Kulinski, J.; Anand, V.; Mayo, H.; Kumbhani, D.J.; De Lemos, J.; Berry, J.D. Continuous Dose-Response Association between Sedentary Time and Risk for Cardiovascular Disease. JAMA Cardiol. 2016, 1, 575–583. [Google Scholar] [CrossRef]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary Time and Its Association with Risk for Disease Incidence, Mortality, and Hospitalization in Adults. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting Time and Mortality from All Causes, Cardiovascular Disease, and Cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef]
- Young, D.R.; Hivert, M.F.; Alhassan, S.; Camhi, S.M.; Ferguson, J.F.; Katzmarzyk, P.T.; Lewis, C.E.; Owen, N.; Perry, C.K.; Siddique, J.; et al. Sedentary Behavior and Cardiovascular Morbidity and Mortality: A Science Advisory from the American Heart Association. Circulation 2016, 134, e262–e279. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in sedentary time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Egerton, T.; Leask, C.; Stamatakis, E. Meta-analysis of the relationship between breaks in sedentary behavior and cardiometabolic health. Obesity 2015, 23, 1800–1810. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Wong, S.L.; Winkler, E.; Healy, G.N.; Colley, R.C.; Tremblay, M.S. Patterns of sedentary time and cardiometabolic risk among Canadian adults. Prev. Med. 2014, 65, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Benatti, F.B.; Ried-Larsen, M. The Effects of Breaking up Prolonged Sitting Time: A Review of Experimental Studies. Med. Sci. Sports Exerc. 2015, 47, 2053–2061. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef]
- Bailey, D.P.; Locke, C.D. Breaking up prolonged sitting with light-intensity walking improves postprandial glycemia, but breaking up sitting with standing does not. J. Sci. Med. Sport 2015, 18, 294–298. [Google Scholar] [CrossRef]
- Brocklebank, L.A.; Andrews, R.C.; Page, A.; Falconer, C.L.; Leary, S.; Cooper, A. The Acute Effects of Breaking Up Seated Office Work With Standing or Light-Intensity Walking on Interstitial Glucose Concentration: A Randomized Crossover Trial. J. Phys. Act. Health 2017, 14, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Popkin, B.M. Time use and physical activity: A shift away from movement across the globe. Obes. Rev. 2012, 13, 659–680. [Google Scholar] [CrossRef] [PubMed]
- Olsson, S.J.G.; Ekblom, Ö.; Andersson, E.; Börjesson, M.; Kallings, L.V. Categorical answer modes provide superior validity to open answers when asking for level of physical activity: A cross-sectional study. Scand. J. Public Health 2016, 44, 70–76. [Google Scholar] [CrossRef] [PubMed]
- The National Board of Health and Welfare. Disease Prevention in the Swedish Healthcare System: Health Situation, National Guidelines and Implementation; The National Board of Health and Welfare: Västerås, Sweden, 2013.
- Olsson, S.J.G. Studies of Physical Activity in the Swedish Population. Ph.D. Thesis, The Swedish School of Sport and Health Sciences, Stockholm, Sweden, 2016. [Google Scholar]
- Olsson, S.J.G.; Ekblom-Bak, E.; Ekblom, B.; Kallings, L.V.; Ekblom, Ö.; Börjesson, M. Association of perceived physical health and physical fitness in two Swedish national samples from 1990 and 2015. Scand. J. Med. Sci. Sports 2018, 28, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.E.; Bull, F.C.; Marshall, A.L.; Sallis, J.F.; Bauman, A.E. Assessment of sedentary behavior with the International Physical Activity Questionnaire. J. Phys. Act. Health 2008, 5, S30–S44. [Google Scholar] [CrossRef]
- Marshall, A.L.; Miller, Y.D.; Burton, N.W.; Brown, W.J. Measuring total and domain-specific sitting: A study of reliability and validity. Med. Sci. Sports Exerc. 2010, 42, 1094–1102. [Google Scholar] [CrossRef]
- Clemes, S.A.; David, B.M.; Zhao, Y.; Han, X.; Brown, W. Validity of Two Self-Report Measures of Sitting Time. J. Phys. Act. Health 2012, 9, 533–539. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Rowlands, A.V.; Bunnewell, S.; Sanders, J.; Esliger, D.W.; Gorely, T.; O’Connell, S.; Davies, M.J.; Khunti, K.; Yates, T. Accuracy of Posture Allocation Algorithms for Thigh- and Waist-Worn Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 1085–1090. [Google Scholar] [CrossRef]
- Santos-Lozano, A.; Torres-Luque, G.; Marin, P.J.; Ruiz, J.R.; Lucia, A.; Garatachea, N. Intermonitor variability of GT3X accelerometer. Int. J. Sports Med. 2012, 33, 994–999. [Google Scholar] [CrossRef]
- Santos-Lozano, A.; Santin-Medeiros, F.; Cardon, G.; Torres-Luque, G.; Bailon, R.; Bergmeir, C.; Ruiz, J.R.; Lucia, A.; Garatachea, N. Actigraph GT3X: Validation and determination of physical activity intensity cut points. Int. J. Sports Med. 2013, 34, 975–982. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of Time Spent in Sedentary Behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking Up Prolonged Sitting Reduces Postprandial Glucose and Insulin Responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Latouche, C.; Jowett, J.B.M.; Carey, A.L.; Bertovic, D.A.; Owen, N.; Dunstan, D.W.; Kingwell, B.A. Effects of breaking up prolonged sitting on skeletal muscle gene expression. J. Appl. Physiol. 2013, 114, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Johnson, W.D.; Katzmarzyk, P.T. U.S. Population Profile of Time-Stamped Accelerometer Outputs: Impact of Wear Time. J. Phys. Act. Health 2011, 8, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Katapally, T.R.; Muhajarine, N. Towards Uniform Accelerometry Analysis: A Standardization Methodology to Minimize Measurement Bias Due to Systematic Accelerometer Wear-Time Variation. J. Sports Sci. Med. 2014, 13, 379–386. [Google Scholar]
- Chuhe, C.; Jerome, G.J.; LaFerriere, D.; Young, D.R.; Vollmer, W.M. Procedures Used to Standardize Data Collected by RT3 Triaxial Accelerometers in a Large-Scale Weight-Loss Trial. J. Phys. Act. Health 2009, 6, 354–359. [Google Scholar] [CrossRef]
- Bond, D.S.; Raynor, H.A.; Phelan, S.; Steeves, J.; Daniello, R.; Wing, R.R. The Relationship between Physical Activity Variety and Objectively Measured Moderate-to-Vigorous Physical Activity Levels in Weight Loss Maintainers and Normal-Weight Individuals. J. Obes. 2012, 2012, 812414. [Google Scholar] [CrossRef]
- Muijs, D. Doing Quantitative Research in Education; Sage Publications: London, UK, 2004. [Google Scholar] [CrossRef]
- Matthews, C.E.; Keadle, S.K.; Troiano, R.P.; Kahle, L.; Koster, A.; Brychta, R.; Van Domelen, D.; Caserotti, P.; Chen, K.Y.; Harris, T.B.; et al. Accelerometer-measured dose-response for physical activity, sedentary time, and mortality in US adults. Am. J. Clin. Nutr. 2016, 104, 1424–1432. [Google Scholar] [CrossRef]
- Lee, P.H. Examining Non-Linear Associations between Accelerometer-Measured Physical Activity, Sedentary Behavior, and All-Cause Mortality Using Segmented Cox Regression. Front. Physiol. 2016, 7, 272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekblom, Ö.; Ekblom-Bak, E.; Rosengren, A.; Hallsten, M.; Bergström, G.; Börjesson, M. Cardiorespiratory Fitness, Sedentary Behaviour and Physical Activity Are Independently Associated with the Metabolic Syndrome, Results from the SCAPIS Pilot Study. PLoS ONE 2015, 10, e0131586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekblom, O.; Ekblom-Bak, E.; Bolam, K.; Ekblom, B.; Schmidt, C.; Soderberg, S.; Bergstrom, G.; Borjesson, M. Concurrent and predictive validity of physical activity measurement items commonly used in clinical settings- data from SCAPIS pilot study. BMC Public Health 2015, 15, 978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkin, A.J.; Gorely, T.; Clemes, S.A.; Yates, T.; Edwardson, C.; Brage, S.; Salmon, J.; Marshall, S.J.; Biddle, S.J. Methods of Measurement in epidemiology: Sedentary Behaviour. Int. J. Epidemiol. 2012, 41, 1460–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuval, K.; Kohl, H.W.; Bernstein, I.; Cheng, D.; Pettee Gabriel, K.; Barlow, C.E.; Yinghui, L.; DiPietro, L. Sedentary behaviour and physical inactivity assessment in primary care: The Rapid Assessment Disuse Index (RADI) study. Br. J. Sports Med. 2014, 48, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Gardner, B.; Flint, S.; Rebar, A.L.; Dewitt, S.; Quail, S.K.; Whall, H.; Smith, L. Is sitting invisible? Exploring how people mentally represent sitting. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 85. [Google Scholar] [CrossRef]
- Pulsford, R.M.; Blackwell, J.; Hillsdon, M.; Kos, K. Intermittent walking, but not standing, improves postprandial insulin and glucose relative to sustained sitting: A randomised cross-over study in inactive middle-aged men. J. Sci. Med. Sport 2017, 20, 278–283. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Concurrent Validity Analysis | All (n = 711) | Women (n = 489) | Men (n = 222) | p-Value * |
| SED-GIH c (n = 711) | 2 (2–3) | 2 (2–3) | 3 (2–4) | <0.001 |
| Accelerometer data | ||||
| Stationary time (min/day) | 492 (433–546) | 480 (427–532) | 525 (459–578) | <0.001 |
| Standardized a stationary time (min/day) | 540 (481–601) | 529 (470–582) | 577 (497–625) | <0.001 |
| Prolonged b stationary time (min/day) | 160 (109–224) | 147 (99–201) | 201 (142–262) | <0.001 |
| Standardized a prolonged stationary time (min/day) | 177 (118–244) | 161 (107–219) | 217 (158–281) | <0.001 |
| MVPA (min/day) | 36 (23–54) | 34 (23–51) | 41 (25–60) | 0.001 |
| Convergent Validity Analysis | All (n = 560) | Women (n = 367) | Men (n = 193) | p-Value * |
| SED-GIH c | 2 (2–3) | 2 (2–3) | 3 (2–4) | <0.001 |
| Katzmarzyk c | 2 (2–3) | 2 (2–3) | 3 (2–3) | <0.001 |
| IPAQ (min) | 360 (240–480) | 330 (210–480) | 360 (270–555) | 0.001 |
| Marshall (min) | 415 (270–560) | 365 (240–539) | 480 (330–603) | <0.001 |
| Accelerometer data | <0.001 | |||
| Stationary time (min/day) | 502 (440–553) | 486 (433–538) | 528 (467–584) | <0.001 |
| Standardized a stationary time (min/day) | 548 (486–606) | 533 (471–588) | 582 (510–627) | <0.001 |
| Prolonged b stationary time (min/day) | 168 (115–233) | 153 (100–208) | 201 (145–258) | <0.001 |
| Standardized a prolonged stationary time (min/day) | 184 (125–251) | 169 (111–231) | 218 (163–279) | <0.001 |
| Over-Reporting | Correct Reporting | Under-Reporting | ||
|---|---|---|---|---|
| SED-GIH | 0–3 h | - | 0 | 143 (100%) |
| 4–6 h | 0 | 13 (5%) | 266 (95%) | |
| 7–9 h | 2 (1%) | 88 (52%) | 79 (47%) | |
| 10+ h a | 37 (31%) | 83 (69%) | - | |
| SES | Low | 30(7%) | 114 (26%) | 294 (67%) |
| High | 39 (3%) | 69 (26%) | 186 (71%) | |
| Gender | Male * | 17 (8%) | 71 (32%) | 134 (60%) |
| Female * | 22 (5%) | 113 (23%) | 354 (72%) | |
| MVPA | Under median * | 13 (3%) | 97 (24%) | 293 (73%) |
| Over median * | 26 (8%) | 87 (28%) | 195 (63%) | |
| Age | Under median * | 25 (7%) | 104 (29%) | 235 (65%) |
| Over median * | 14 (4%) | 80 (23%) | 253 (73%) | |
| WC | Low | 20 (7%) | 77 (27%) | 191 (66%) |
| High | 6 (6%) | 33 (34%) | 57 (59%) |
| Varieties | Stationary (min/day) | Prolonged Stationary b (min/day) | SED-GIH | Katzmarzyk | IPAQ (min) | Marshall (min) |
|---|---|---|---|---|---|---|
| SED-GIH | 0.48 c | 0.44 c | - | 0.89 e | 0.83 e | 0.72 d |
| Katzmarzyk | 0.53 d | 0.46 c | 0.89 e | - | 0.72 d | 0.72 d |
| IPAQ (min) | 0.44 c | 0.41 c | 0.83 e | 0.72 d | - | 0.70 d |
| Marshall (min) | 0.48 c | 0.46 c | 0.72 d | 0.72 d | 0.70 d | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kallings, L.V.; Olsson, S.J.G.; Ekblom, Ö.; Ekblom-Bak, E.; Börjesson, M. The SED-GIH: A Single-Item Question for Assessment of Stationary Behavior—A Study of Concurrent and Convergent Validity. Int. J. Environ. Res. Public Health 2019, 16, 4766. https://doi.org/10.3390/ijerph16234766
Kallings LV, Olsson SJG, Ekblom Ö, Ekblom-Bak E, Börjesson M. The SED-GIH: A Single-Item Question for Assessment of Stationary Behavior—A Study of Concurrent and Convergent Validity. International Journal of Environmental Research and Public Health. 2019; 16(23):4766. https://doi.org/10.3390/ijerph16234766
Chicago/Turabian StyleKallings, Lena V., Sven J. G. Olsson, Örjan Ekblom, Elin Ekblom-Bak, and Mats Börjesson. 2019. "The SED-GIH: A Single-Item Question for Assessment of Stationary Behavior—A Study of Concurrent and Convergent Validity" International Journal of Environmental Research and Public Health 16, no. 23: 4766. https://doi.org/10.3390/ijerph16234766