Associations between Urban Green Spaces and Health are Dependent on the Analytical Scale and How Urban Green Spaces are Measured


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Background and Household Survey
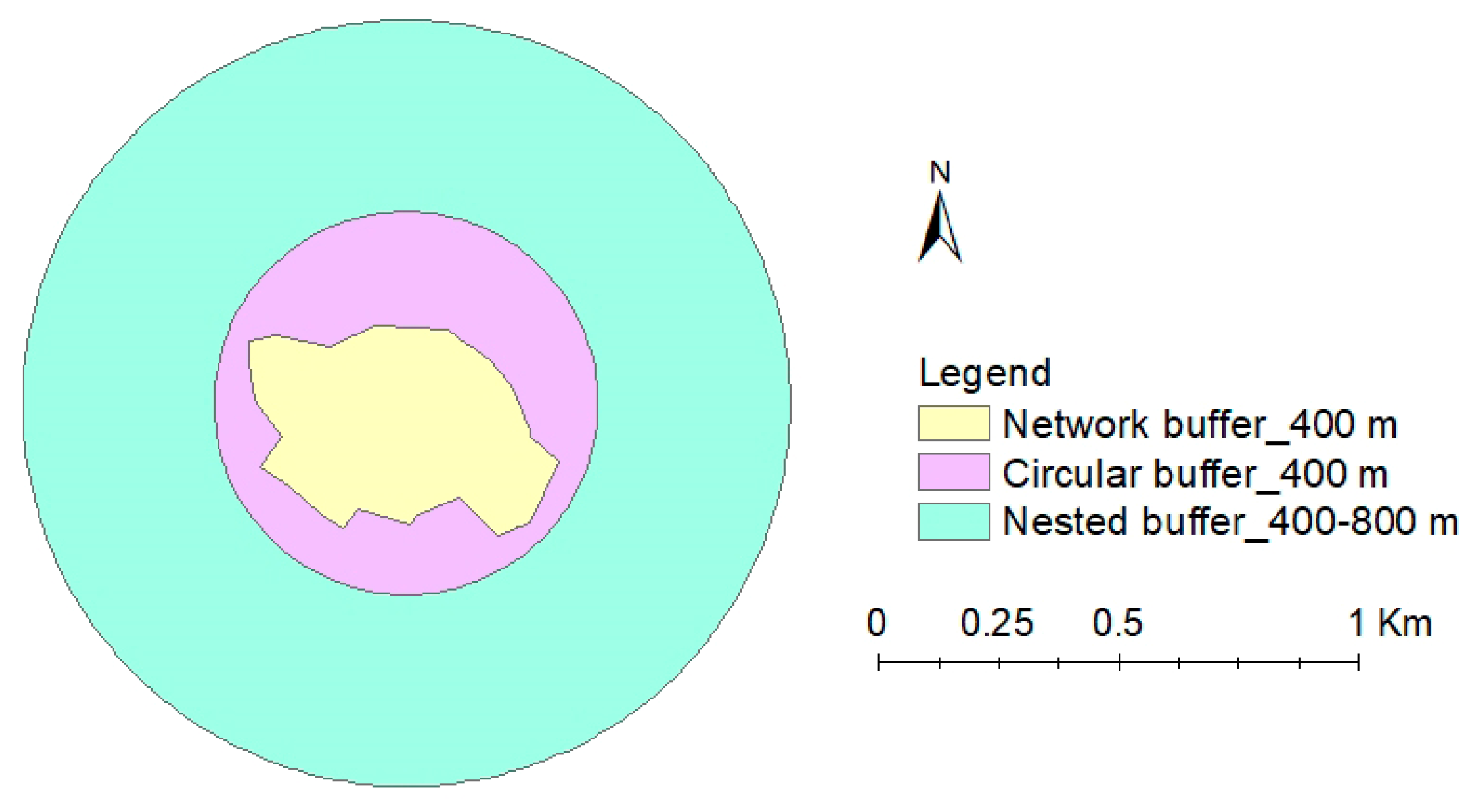
2.2. Assessment of UGS Quantity at Different Scales
2.3. Statistical Analyses
3. Results
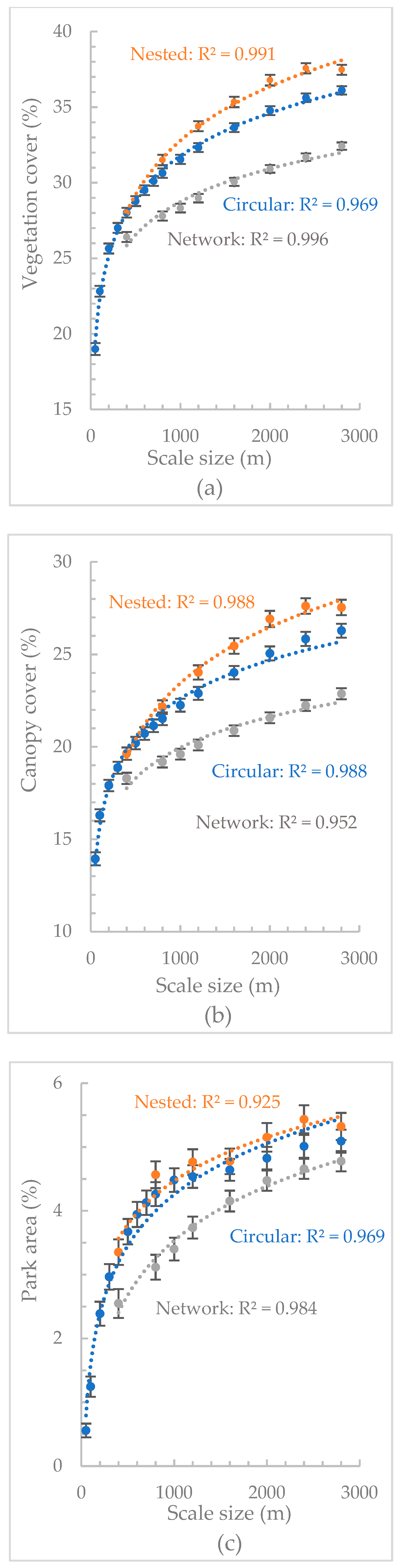
3.1. Quantity of Different UGS Metrics at Different Scales
3.2. Study Population
3.3. Comparison of Different UGS Metrics
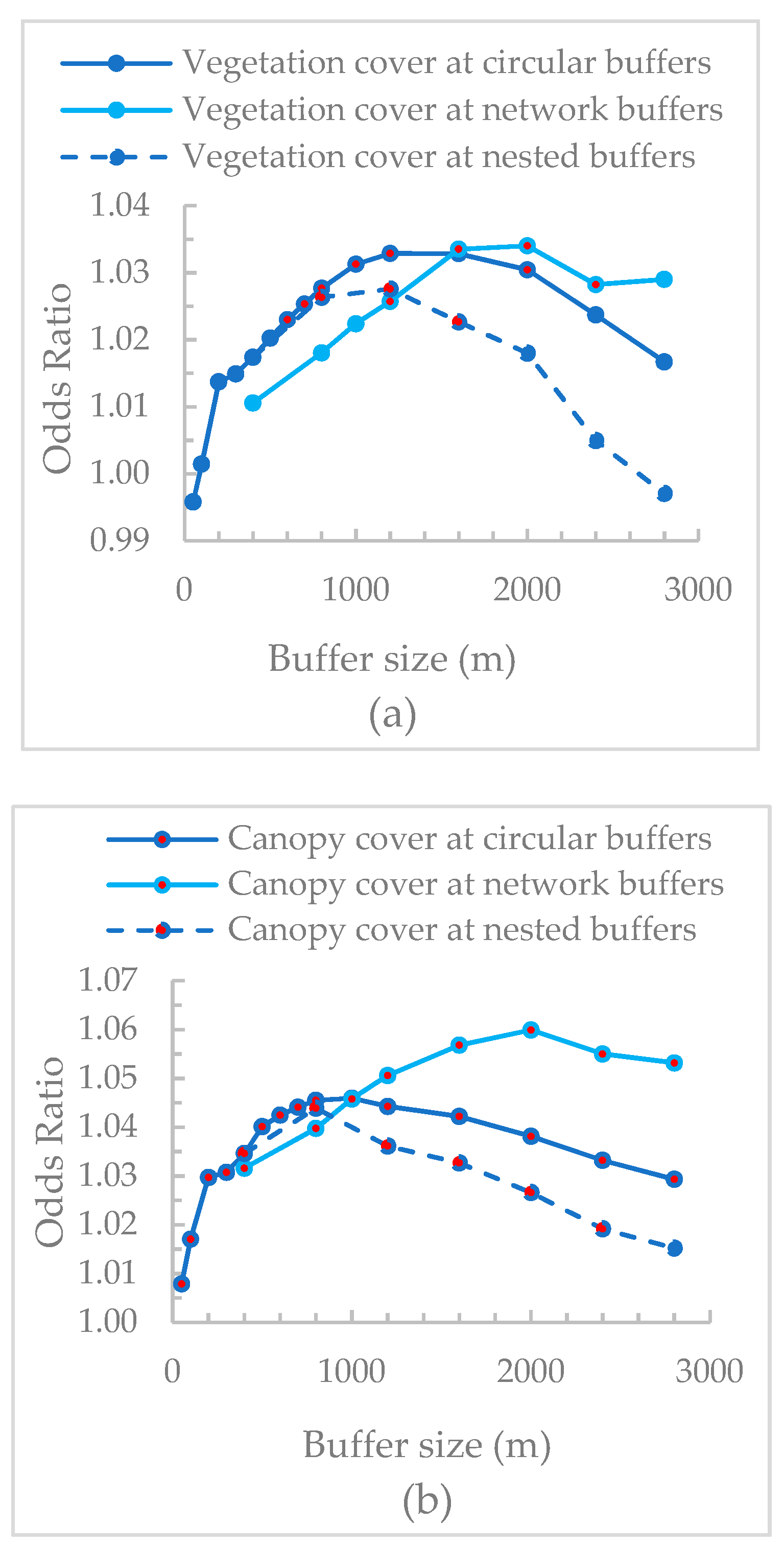
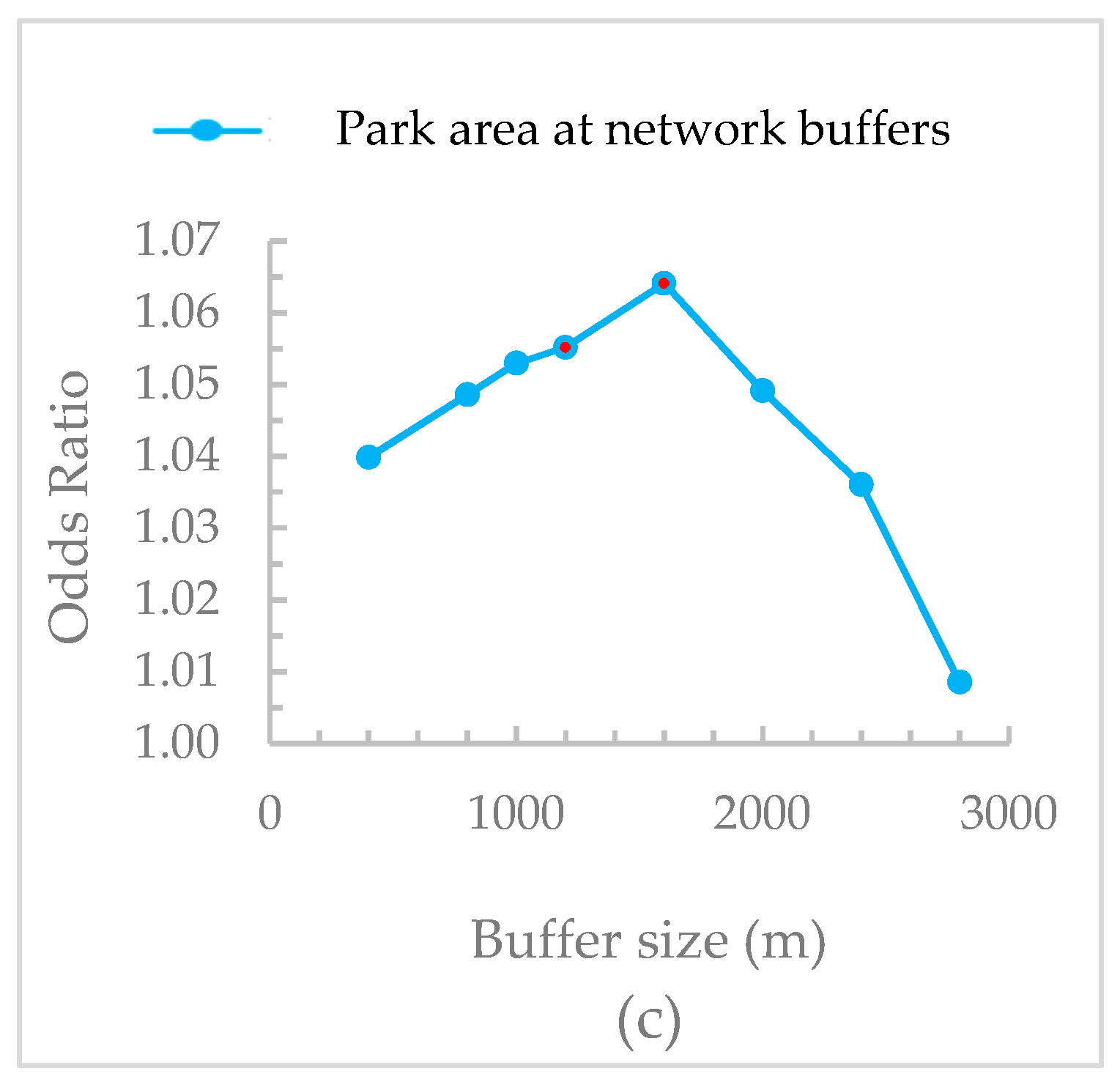
3.4. Comparison of Different Spatial Scales
4. Discussion
4.1. The Associations of Different UGS Metrics with Mental Health
4.2. The Influence of Analytical Scale on UGS-Health Associations
4.3. Study Limitations
4.4. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, L.; Tan, P.Y.; Diehl, J.A. A conceptual framework for studying urban green spaces effects on health. J. Urban Ecol. 2017, 3, 1–13. [Google Scholar] [CrossRef]
- Taylor, L.; Hochuli, D.F. Defining greenspace: Multiple uses across multiple disciplines. Landsc. Urban Plan. 2017, 158, 25–38. [Google Scholar] [CrossRef] [Green Version]
- Dadvand, P.; Sunyer, J.; Basagaña, X.; Ballester, F.; Lertxundi, A.; Fernández-Somoano, A.; Estarlich, M.; García-Esteban, R.; Mendez, M.A.; Nieuwenhuijsen, M.J. Surrounding greenness and pregnancy outcomes in four Spanish birth cohorts. Environ. Health Perspect. 2012, 120, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Jonker, M.F.; van Lenthe, F.; Donkers, B.; Mackenbach, J.P.; Burdorf, A. The effect of urban green on small-area (healthy) life expectancy. J. Epidemiol. Community Health 2014, 68, 999–1002. [Google Scholar] [CrossRef] [PubMed]
- Roe, J.J.; Ward Thompson, C.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Abelt, K.; Mclafferty, S. Green Streets: Urban Green and Birth Outcomes. Int. J. Environ. Res. Public Health 2017, 14, 771. [Google Scholar] [CrossRef]
- Donovan, G.H.; Michael, Y.L.; Butry, D.T.; Sullivan, A.D.; Chase, J.M. Urban trees and the risk of poor birth outcomes. Health Place 2011, 17, 390–393. [Google Scholar] [CrossRef]
- Donovan, G.H.; Gatziolis, D.; Longley, I.; Douwes, J. Vegetation diversity protects against childhood asthma: Results from a large New Zealand birth cohort. Nat. Plants 2018, 4. [Google Scholar] [CrossRef]
- Sivarajah, S.; Smith, S.M.; Thomas, S.C. Tree cover and species composition effects on academic performance of primary school students. PLoS ONE 2018, 13, e0193254. [Google Scholar] [CrossRef]
- Dzhambov, A.; Hartig, T.; Markevych, I.; Tilov, B.; Dimitrova, D. Urban residential greenspace and mental health in youth: Different approaches to testing multiple pathways yield different conclusions. Environ. Res. 2018, 160, 47–59. [Google Scholar] [CrossRef]
- Beyer, K.M.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Javier Nieto, F.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef]
- Huynh, Q.; Craig, W.; Janssen, I.; Pickett, W. Exposure to public natural space as a protective factor for emotional well-being among young people in Canada. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paquet, C.; Orschulok, T.P.; Coffee, N.T.; Howard, N.J.; Hugo, G.; Taylor, A.W.; Adams, R.J.; Daniel, M. Are accessibility and characteristics of public open spaces associated with a better cardiometabolic health? Landsc. Urban Plan. 2013, 118, 70–78. [Google Scholar] [CrossRef]
- Parra, D.C.; Gomez, L.F.; Sarmiento, O.L.; Buchner, D.; Brownson, R.; Schimd, T.; Gomez, V.; Lobelo, F. Perceived and objective neighborhood environment attributes and health related quality of life among the elderly in Bogotá, Colombia. Soc. Sci. Med. 2010, 70, 1070–1076. [Google Scholar] [CrossRef]
- Villeneuve, P.J.; Jerrett, M.; Su, J.; Burnett, R.T.; Chen, H.; Wheeler, A.J.; Goldberg, M.S. A cohort study relating urban green space with mortality in Ontario, Canada. Environ. Res. 2012, 115, 51–58. [Google Scholar] [CrossRef]
- Annerstedt, M.; Östergren, P.-O.; Björk, J.; Grahn, P.; Skärbäck, E.; Währborg, P. Green qualities in the neighbourhood and mental health—Results from a longitudinal cohort study in Southern Sweden. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Potestio, M.L.; Patel, A.B.; Powell, C.D.; McNeil, D.A.; Jacobson, R.D.; McLaren, L. Is there an association between spatial access to parks/green space and childhood overweight/obesity in Calgary, Canada? Int. J. Behav. Nutr. Phys. Act. 2009, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- de Vries, S.; van Dillen, S.M.E.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef]
- Bixby, H.; Hodgson, S.; Fortunato, L.; Hansell, A.; Fecht, D. Associations between green space and health in english cities: An ecological, cross-sectional study. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.A.; Mitchell, R.; Hartig, T.; de Vries, S.; Astell-Burt, T.; Frumkin, H. Green cities and health: A question of scale? J. Epidemiol. Community Health 2012, 66, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Astell-Burt, T.; Richardson, E.A. A comparison of green space indicators for epidemiological research. J. Epidemiol. Community Health 2011, 65, 853–858. [Google Scholar] [CrossRef] [Green Version]
- Takano, T.; Fu, J.; Nakamura, K.; Uji, K.; Fukuda, Y.; Watanabe, M.; Nakajima, H. Age-adjusted mortality and its association to variations in urban conditions in Shanghai. Health Policy 2002, 61, 239–253. [Google Scholar] [CrossRef]
- Kwan, M.P. How GIS can help address the uncertain geographic context problem in social science research. Ann. GIS 2012, 18, 245–255. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Markevych, I.; Lercher, P. Greenspace seems protective of both high and low blood pressure among residents of an Alpine valley. Environ. Int. 2019, 121, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Fuertes, E.; Tiesler, C.M.T.; Birk, M.; Bauer, C.; Koletzko, S.; Berg, A.; Berdel, D.; Heinrich, J. Health & Place Surrounding greenness and birth weight: Results from the GINIplus and LISAplus birth cohorts in Munich. Health Place 2014, 26, 39–46. [Google Scholar] [CrossRef]
- Dadvand, P.; Villanueva, C.M.; Font-ribera, L.; Martinez, D.; Vrijheid, M.; Kogevinas, M. Children’ s Health Risks and Benefits of Green Spaces for Children: A Cross-Sectional Study. Environ. Health Perspect. 2014, 122, 1329–1336. [Google Scholar] [CrossRef]
- Kondo, M.C.; Low, S.C.; Henning, J.; Branas, C.C. The Impact of Green Stormwater Infrastructure Installation on Surrounding Health and Safety. Am. J. Public Health 2015, 105, 114–121. [Google Scholar] [CrossRef]
- Fan, Y.; Das, K.V.; Chen, Q. Neighborhood green, social support, physical activity, and stress: Assessing the cumulative impact. Health Place 2011, 17, 1202–1211. [Google Scholar] [CrossRef]
- Twohig-bennett, C.; Jones, A. The health bene fi ts of the great outdoors: A systematic review and meta- analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Donovan, G.H.; Butry, D.T.; Michael, Y.L.; Prestemon, J.P.; Liebhold, A.M.; Gatziolis, D.; Mao, M.Y. The relationship between trees and human health: Evidence from the spread of the emerald ash borer. Am. J. Prev. Med. 2013, 44, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.J.; Hirabayashi, S.; Bodine, A.; Greenfield, E. Tree and forest effects on air quality and human health in the United States. Environ. Pollut. 2014, 193, 119–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller-Riemenschneider, F.; Petrunoff, N.; Sia, A.; Ramiah, A.; Ng, A.; Han, J.; Wong, M.; Choo, T.B.; Uijtdewilligen, L. Prescribing physical activity in parks to improve health and wellbeing: Protocol of the park prescription randomized controlled trial. Int. J. Environ. Res. Public Health 2018, 15, 1154. [Google Scholar] [CrossRef] [PubMed]
- Sia, A.; Ng, K.S.; Ng, M.K.; Chan, H.Y.; Tan, C.H.; Rawtaer, I.; Feng, L.; Mahendran, R.; Kua, E.H.; Ho, R. The Effect of Therapeutic Horticulture on the Psychological Wellbeing of Elderly in Singapore: A Randomised Controlled Trial. J. Ther. Hortic. 2018, 28, 1–10. [Google Scholar]
- Tan, P.Y.; Wang, J.; Sia, A. Perspectives on five decades of the urban greening of Singapore. Cities 2013, 32, 24–32. [Google Scholar] [CrossRef]
- Ling, S.K. The Value of Parks Nearby and Ways to Enhance Them. Research Technical Note Urban Studies Series; 2012. Available online: https://www.nparks.gov.sg/-/media/cuge/pdf/rtn-09-2012---the-value-of-parks-nearby-and-ways-to-enhance-them.pdf (accessed on 14 February 2019).
- Browning, M.; Lee, K. Within what distance does “greenness” best predict physical health? A systematic review of articles with gis buffer analyses across the lifespan. Int. J. Environ. Res. Public Health 2017, 14, 675. [Google Scholar] [CrossRef]
- Egorov, A.I.; Gri, S.M.; Converse, R.R.; Styles, J.N.; Sams, E.A.; Wilson, A.; Jackson, L.E.; Wade, T.J. Vegetated land cover near residence is associated with reduced allostatic load and improved biomarkers of neuroendocrine, metabolic and immune functions. Environ. Res. 2017, 158, 508–521. [Google Scholar] [CrossRef]
- Alcock, I.; White, M.P.; Wheeler, B.W.; Fleming, L.E.; Depledge, M.H. Longitudinal effects on mental health of moving to greener and less green urban areas TL-48. Environ. Sci. Technol. 2014, 48, 1247–1255. [Google Scholar] [CrossRef]
- Alcock, I.; White, M.P.; Lovell, R.; Higgins, S.L.; Osborne, N.J.; Husk, K.; Wheeler, B.W. Landscape and Urban Planning What accounts for ‘England’ s green and pleasant land? A panel data analysis of mental health and land cover types in rural England. Landsc. Urban Plan. 2015, 142, 38–46. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The association between green space and mental health varies across the lifecourse. A longitudinal study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Bartoll, X.; Basagaña, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C.; et al. Green spaces and General Health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural environments—Healthy environments? An exploratory analysis of the relationship between greenspace and health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef]
- Tsurumi, T.; Imauji, A.; Managi, S. Greenery and Subjective Well-being: Assessing the Monetary Value of Greenery by Type. Ecol. Econ. 2018, 148, 152–169. [Google Scholar] [CrossRef]
- van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- Lim, L.; Ng, T.P.; Chua, H.C.; Chiam, P.C.; Won, V.; Lee, T.; Fones, C.S.L.; Kua, E.H. Generalised anxiety disorder in Singapore: Prevalence, co-morbidity and risk factors in a multi-ethnic population. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 972–979. [Google Scholar] [CrossRef]
- Satghare, P.; Abdin, E.; Vaingankar, J.A.; Chua, B.Y.; Pang, S.; Picco, L.; Poon, L.Y.; Chong, S.A.; Subramaniam, M. Prevalence of Sleep Problems Among Those With Internet Gaming Disorder in Singapore. Asean J. Psychiatry 2016, 17, 188–198. [Google Scholar]
- Rai, D.; Kosidou, K.; Lundberg, M.; Araya, R.; Lewis, G.; Magnusson, C. Psychological distress and risk of long-term disability: Population-based longitudinal study. J. Epidemiol. Community Health 2012, 66, 586–592. [Google Scholar] [CrossRef]
- Nichani, V.; Dirks, K.; Burns, B.; Bird, A.; Grant, C. Green space and depression during pregnancy: Results from the growing up in New Zealand study. Int. J. Environ. Res. Public Health 2017, 14, 1083. [Google Scholar] [CrossRef]
- Triguero-Mas, M.; Dadvand, P.; Cirach, M.; Martínez, D.; Medina, A.; Mompart, A.; Basagaña, X.; Gražulevičienė, R.; Nieuwenhuijsen, M.J. Natural outdoor environments and mental and physical health: Relationships and mechanisms. Environ. Int. 2015, 77, 35–41. [Google Scholar] [CrossRef]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. The use of the Godin-Shephard Leisure-Time Physical Activity Questionnaire in oncology research: A systematic review. BMC Med. Res. Methodol. 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Grootaert, C.; Narayan, D.; Jones, V.N.; Woolcock, M. Measuring Social Capital: An Integrated Questionnaire; The World Bank: Washington, DC, USA, 2004; ISBN 9780821356616. [Google Scholar]
- Hamid, A.R.; Tan, P.Y. Urban Ecological Networks for Biodiversity Conservation in Cities. In Greening Cities: Forms and Functions; Tan, P.Y., Jim, C.Y., Eds.; Springer Singapore: Singapore, 2017; pp. 251–277. [Google Scholar]
- Chong, S.A.; Abdin, E.; Vaingankar, J.A.; Heng, D.; Sherbourne, C.D.; Yap, M.; Lim, Y.W.; Wong, H.B.; Ghosh-Dastidar, B.; Kwok, K.W.; et al. A population-based survey of mental disorders in Singapore. Ann. Acad. Med. 2012, 41, 49–66. [Google Scholar]
- Midi, H.; Sarkar, S.K.; Rana, S. Collinearity diagnostics of binary logistic regression model. J. Interdiscip. Math. 2010, 13, 253–267. [Google Scholar] [CrossRef] [Green Version]
- Klompmaker, J.O.; Hoek, G.; Bloemsma, L.D.; Gehring, U.; Strak, M.; Wijga, A.H.; van den Brink, C.; Brunekreef, B.; Lebret, E.; Janssen, N.A.H. Green space definition affects associations of green space with overweight and physical activity. Environ. Res. 2018, 160, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Tyrväinen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Beil, K.; Hanes, D. The influence of urban natural and built environments on physiological and psychological measures of stress- A pilot study. Int. J. Environ. Res. Public Health 2013, 10, 1250–1267. [Google Scholar] [CrossRef] [PubMed]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health: A conceptual model. Am. J. Prev. Med. 2005, 28, 159. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.; Clougherty, J.; Shmool, J.; Kubzansky, L. Is All Urban Green Space the Same? A Comparison of the Health Benefits of Trees and Grass in New York City. Int. J. Environ. Res. Public Health 2017, 14, 1411. [Google Scholar] [CrossRef]
- Jeanjean, A.P.R.; Monks, P.S.; Leigh, R.J. Modelling the effectiveness of urban trees and grass on PM2.5 reduction via dispersion and deposition at a city scale. Atmos. Environ. 2016, 147, 1–10. [Google Scholar] [CrossRef]
- Zupancic, T.; Westmacott, C.; Bulthuis, M. The Impact of Green Space on Heat and Air Pollution in Urban Communities: A Meta-Narrative Systematic Review; David Suzuki Foundation: Vancouver, BC, Canada, 2015. [Google Scholar]
- Armson, D.; Stringer, P.; Ennos, A.R. The effect of tree shade and grass on surface and globe temperatures in an urban area. Urban For. Urban Green. 2012, 11, 245–255. [Google Scholar] [CrossRef]
- Lindal, P.J.; Hartig, T. Effects of urban street vegetation on judgments of restoration likelihood. Urban For. Urban Green. 2015, 14, 200–209. [Google Scholar] [CrossRef]
- Picavet, H.S.J.; Milder, I.; Kruize, H.; de Vries, S.; Hermans, T.; Wendel-Vos, W. Greener living environment healthier people? Exploring green space, physical activity and health in the Doetinchem Cohort Study. Prev. Med. 2016, 89, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Lachowycz, K.; Jones, A.P. Towards A Better Understanding Of The Relationship Between Greenspace And Health: Development Of A Theoretical Framework. Landsc. Urban Plan. 2013, 118, 62–69. [Google Scholar] [CrossRef]
- Kardan, O.; Gozdyra, P.; Misic, B.; Moola, F.; Palmer, L.J.; Paus, T.; Berman, M.G. Neighborhood greenspace and health in a large urban center. Sci. Rep. 2015, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Ekholm, O.; Schipperijn, J.; Toftager, M.; Kamper-Jørgensen, F.; Randrup, T.B. Health promoting outdoor environments—Associations between green space, and health, health-related quality of life and stress based on a Danish national representative survey. Scand. J. Public Health 2010, 38, 411–417. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Wheeler, B.W.; Depledge, M.H. Would You Be Happier Living in a Greener Urban Area? A Fixed-Effects Analysis of Panel Data. Psychol. Sci. 2013, 24, 920–928. [Google Scholar] [CrossRef]
- Helbich, M.; Klein, N.; Roberts, H.; Hagedoorn, P.; Groenewegen, P.P. More green space is related to less antidepressant prescription rates in the Netherlands: A Bayesian geoadditive quantile regression approach. Environ. Res. 2018, 166, 290–297. [Google Scholar] [CrossRef]
- Rosenman, R.; Tennekoon, V.; Hill, L.G. Measuring bias in self-reported data. Int. J. Behav. Healthc. Res. 2011, 2, 320–332. [Google Scholar] [CrossRef]
- Akpinar, A. Assessing the Associations among Green Space Type, Structure, General Mental Health and General Health Employing the BRFSS and the US National Land Cover Data. Ph.D. Thesis, Washington State University, Pullman, WA, USA, 2013. [Google Scholar]
- Ordóñez-Gómez, J.D.; Arroyo-Rodríguez, V.; Nicasio-Arzeta, S.; Cristóbal-Azkarate, J. Which is the appropriate scale to assess the impact of landscape spatial configuration on the diet and behavior of spider monkeys? Am. J. Primatol. 2015, 77, 56–65. [Google Scholar] [CrossRef]
- Olszewska-Guizzo, A.A.; Paiva, T.O.; Barbosa, F. Effects of 3D Contemplative Landscape Videos on Brain Activity in a Passive Exposure EEG Experiment. Front. Psychiatry 2018, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Saw, L.E.; Lim, F.K.S.; Carrasco, L.R. The relationship between natural park usage and happiness does not hold in a tropical city-state. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Stratification | Target | Collected | Difference |
|---|---|---|---|---|
| Gender | Male | 49.1% | 45% | −4.1% |
| Female | 50.9% | 55% | +4.1% | |
| Ethnicity | Chinese | 74.3% | 72.2% | −2.1% |
| Malays | 13.4% | 15.3% | +1.9% | |
| Indians | 9.1% | 9.3% | +0.2% | |
| Others | 3.2% | 3.2% | 0 | |
| Housing type | Total HDB Dwellings 1 | 81.1% | 81.1% | 0 |
| Condominiums, Other Apartments | 12.5% | 12.6% | +0.1% | |
| Landed Properties | 6.4% | 6.3% | −0.1% |
| Sociodemographic | Total (N = 977) n (% of Total Sample) |
|---|---|
| Gender | |
| Men | 442 (45.2%) |
| Women | 535 (54.8%) |
| Age | |
| 21–24 | 49 (5.0%) |
| 25–34 | 123 (12.6%) |
| 35–44 | 190 (19.4%) |
| 45–54 | 183 (18.7%) |
| 55–64 | 194 (19.9%) |
| 65–74 | 157 (16.1%) |
| 75–84 | 72 (7.4%) |
| 85 & over | 9 (0.9%) |
| Ethnicity | |
| Chinese | 702 (71.9%) |
| Malay | 152 (15.6%) |
| Indian | 91 (9.3%) |
| Others | 32 (3.3%) |
| House ownership | |
| Owned | 896 (91.7%) |
| Rental | 81 (8.3%) |
| Housing type | |
| HDB1 1–2 room flat | 61 (6.2%) |
| HDB 3 room flat | 187 (19.1%) |
| HDB 4 room flat | 325 (33.3%) |
| HDB 5 room or executive flat | 218 (22.3%) |
| Private condominium/apartment | 123 (12.6%) |
| Private housing (landed property) | 63 (6.4%) |
| Marital status | |
| Single | 185 (18.9%) |
| Married | 701 (71.8%) |
| Widowed | 51 (5.2%) |
| Divorced/Separated | 40 (4.1%) |
| Employment status | |
| Full-time | 376 (38.5%) |
| Part-time | 106 (10.8%) |
| Self-employed | 65 (6.7%) |
| Retired | 168 (17.2%) |
| Student/NSF2 | 25 (2.6%) |
| Homemaker/Unemployed | 237 (24.3%) |
| Highest Education level | |
| Below Secondary | 224 (22.9%) |
| Secondary | 280 (28.7%) |
| Post-Secondary (Non-Tertiary) | 87 (8.9%) |
| Diploma & Professional Qualification | 170 (17.4%) |
| University & above | 216 (22.1%) |
| Sociodemographic | Percentage of Respondents with Poor Mental Health |
|---|---|
| Gender | |
| Men | 10.0% |
| Women | 14.0% |
| Age | |
| 21–24 | 8.2% |
| 25–34 | 12.2% |
| 35–44 | 7.9% |
| 45–54 | 14.2% |
| 55–64 | 13.4% |
| 65–74 | 14.7% |
| 75–84 | 13.9% |
| 85 & over | 0% |
| Ethnicity | |
| Chinese | 12.4% |
| Malay | 9.2% |
| Indian | 11.0% |
| Others | 25.00% |
| House ownership | |
| Owned | 11.3% |
| Rental | 22.2% |
| Housing type | |
| HDB 1–2 room flat | 29.5% |
| HDB 3 room flat | 11.2% |
| HDB 4 room flat | 11.7% |
| HDB 5 room or executive flat | 11.9% |
| Private condominium/apartment | 9.8% |
| Private housing (landed property) | 6.4% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Tan, P.Y. Associations between Urban Green Spaces and Health are Dependent on the Analytical Scale and How Urban Green Spaces are Measured. Int. J. Environ. Res. Public Health 2019, 16, 578. https://doi.org/10.3390/ijerph16040578
Zhang L, Tan PY. Associations between Urban Green Spaces and Health are Dependent on the Analytical Scale and How Urban Green Spaces are Measured. International Journal of Environmental Research and Public Health. 2019; 16(4):578. https://doi.org/10.3390/ijerph16040578
Chicago/Turabian StyleZhang, Liqing, and Puay Yok Tan. 2019. "Associations between Urban Green Spaces and Health are Dependent on the Analytical Scale and How Urban Green Spaces are Measured" International Journal of Environmental Research and Public Health 16, no. 4: 578. https://doi.org/10.3390/ijerph16040578