1. Introduction
Research has shown that adolescent alcohol consumption varies across neighborhoods [
1,
2]. Adolescents also vary in their motivations for drinking [
3]. The Scottish Government’s Alcohol Framework identifies that it is crucial to understand motives for drinking to limit the negative impact of alcohol on individuals and society [
4]. Additionally, gaining such information is vital for the design of effective public health strategies [
3,
5,
6,
7].
Drinking motives are often regarded as the final pathway to alcohol use, which link to various drinking patterns and may mediate more distal influences [
7,
8]. Currently there are no studies that examine the extent to which adolescent drinking motives vary across neighborhoods; existing studies have examined perceptions of neighborhoods but ignore neighborhood membership. Understanding if drinking motives are associated with where adolescents reside allows for a better comprehension of the pathways by which neighborhood impacts adolescent alcohol use. Therefore, exploring the associations of neighborhood conditions with drinking motives has been identified as an important area for research [
9].
Drinking motives are defined as the reasons why people drink, with the assumption that people drink to obtain a desired outcome [
10]. These motives can be conceptualized as representing dimensions of a motivational construct [
8]. Using this model, the motives to drink are categorized by two underlying dimensions which were proposed by Cox and Klinger [
11]: valence (positive or negative forces that attract or detract i.e., pleasantness or utility [
12]) and source (internal or external) of the outcomes individuals expect to achieve from alcohol use. In terms of valence, it is theorized that people drink to gain positive outcomes or to avoid negative consequences. In terms of source, internal motives of “enhancement of a desired internal emotional state or by external rewards such as social approval or acceptance” ([
6] p. 11) also underlie drinking behavior. Four drinking motives are generally recognized. These are drinking for: (1) coping, (2) enhancement, (3) social and (4) conformity motives [
7]. These four motives are commonly measured using a four factor Drinking Motives Questionnaire, known as the DMQR (Drinking Motives Questionnaire Revised) which was developed by Cooper [
10] and has been validated for use in several samples (adults, university students and adolescents) [
13,
14,
15].
The dimensions and source map onto the four motives as follows:
Internally generated, positive reinforcement = enhancement, i.e., drinking to have fun and get drunk
Externally generated, positive reinforcement = social, i.e., to better enjoy social gatherings
Internally generated, negative reinforcement = coping, i.e., to alleviate problems and worries
Externally generated, negative reinforcement = conformity, i.e., not to feel left out
Motives are often theorized as a potential pathway between neighborhood characteristics and alcohol use. The most common hypothesis is that in stress-inducing neighborhoods (i.e., neighborhoods experiencing material deprivation and disorder) alcohol is used to cope with the increased pressure that comes from living in such an environment [
16,
17,
18]. Previous research has shown that a greater frequency of stressful events occurs in low-income neighborhoods [
19]. Additionally, adverse neighborhood conditions may reduce adolescents’ psychological coping resources; this may lead to increased substance use to deal with life’s challenges [
20]. In contrast, in areas where norms are in favor of alcohol, it would be expected that extrinsic motivations (i.e., social and conformity motives) would be higher. Despite these theorized relationships and suggestive evidence, there are few studies that have examined the motivational pathways through which neighborhoods may impact alcohol use among the adolescent population.
A review undertaken by Kuntsche et al. [
13] examined factors related to adolescents’ alcohol use motives and found that sex, age, mental state (i.e., depression), and situation (i.e., drinking at a party) were all related to motives to drink. The review only found macro-level factors, as measured by cross-national differences in sociocultural factors, in the literature; studies examining within-country neighborhood differences were not identified [
13]. However, as posited above, the neighborhood characteristics that adolescents are exposed to may impact on their drinking motives. A study of Portuguese adolescents examined whether adolescents’ self-reported perceptions of their neighborhoods were associated with their motives for drinking. This study found that drinking for enhancement, to be social, to conform, and to cope, were higher when adolescents perceived high levels of night-time entertainment, violence and robberies, and when they reported that they live in an isolated area. However, perceived social cohesion in their local area was not associated with any drinking motives [
5]. Research that examined associations of drinking to cope with family and individual characteristics found that adolescents from higher socio-economic family backgrounds drank more to increase confidence; while those from families from lower socio-economic backgrounds drank more to cope with low mood [
3]. Although these studies suggest there may be an association between neighborhood characteristics and adolescent drinking motives, they deal only with individual perceptions of the neighborhood or family background, and so little is known about whether the external observable conditions of where adolescents live are associated with their drinking motives. A study of US adults found that objectively measured neighborhood disadvantage was negatively correlated with social motives for drinking and positively correlated with drinking to cope (to forget worries and problems) [
9]. However, whether these relationships exist among adolescents is unknown.
Research is needed to identify sub-groups of young people who have varying drinking motives [
8]. Additionally, calls have been made for further research to investigate drinking motives as a potential mediator in the relationships between neighborhood characteristics and alcohol outcomes [
9]. Accordingly, this study will examine associations between social and physical dimensions of the neighborhood; and adolescent drinking motives. The potential for drinking motives to mediate the relationship between neighborhoods and alcohol use is also explored.
Research questions:
Are characteristics of the neighborhood associated with adolescent drinking motives?
If so, is there evidence that motives mediate the relationship between neighborhood conditions and adolescent alcohol use?
4. Discussion
In line with past research, we found Scottish adolescents reported alcohol use most frequently for social motives, followed by enhancement, coping, and conformity [
5,
8,
27]. Sex differences were only found for negative valence motives. Differences in coping motives are consistent with previous research from Cooper [
10] who found that girls scored higher than boys in coping motives in early adolescence (13–15 years) but among older adolescents the reverse was found. We also found that boys had higher conformity motives, which is consistent with previous studies [
27]. Sex differences in drinking motives are largely thought to be due to differences in personality traits with adolescent females typically being more anxiety sensitive than males and males being more extroverted and impulsive [
27].
This study aimed to determine whether neighborhood conditions were associated with drinking motives and whether drinking motives mediate the link between neighborhood conditions and drinking outcomes among adolescents. There was little variation evident in social enhancement and conformity motives by neighborhood. Previous work with adults found that neighborhood affluence was associated with social motives [
9]; however, such associations were not present for neighborhood deprivation in this sample of Scottish adolescents. Social motives for drinking are frequently reported among adolescents, across different cross-cultural contexts, and appear to be equally important across various neighborhood conditions. This finding supports the need for universal intervention strategies which provide social activities for young people that may be an alternative to alcohol use.
Considering the lack of variation across neighborhoods in social, enhancement and conformity motives, it is not surprising that few neighborhood characteristics were associated with these motives. One exception is that those in the second most deprived neighborhood category had lower conformity motives than those in the most deprived areas. This may be because those residing in the most deprived neighborhoods may be more susceptible to peer group pressures [
48] and that pressure to conform to drinking practices is related in a non-linear fashion to neighborhood deprivation. Based on these findings there is little evidence that neighborhood conditions impact on adolescents’ positive valence, and the impact is also limited for conformity motives.
Coping motives were higher among those living in more deprived areas. This is in line with Karriker-Jaffe et al.’s [
9] findings that adults in disadvantaged neighborhoods report more coping motives for alcohol use. The higher levels of coping motives are of particular concern in deprived neighborhoods, where stress levels may be high and coping resources limited [
9]. Moreover, those who drink to avoid negative outcomes typically experience more negative use-related consequences [
7]. Coping motives in adolescence have also been associated with problem drinking later in life [
49]. Therefore, based on our findings, Scottish adolescents residing in more deprived areas or accessible small towns may be at greater risk of alcohol related harms which has implications for their immediate and longer-term health.
The link between deprivation and drinking to cope may be explained by two, not mutually exclusive, hypotheses: (1) deprived neighborhoods create stress due to the physical and social conditions of the neighborhood, and alcohol is used to cope with the stress created by the environment, and (2) those residing in such neighborhoods have different strategies for coping with life’s general stresses and are more likely to use alcohol to deal with problems [
9]. Because coping-motivated drinking may represent a form of self-medication [
3], our findings suggest the need to develop and evaluate strategies that can help individuals cope with negative affect without alcohol. Additionally, removing neighborhood stress through programs to improve neighborhood conditions may reduce drinking to cope, as well as having wider benefits.
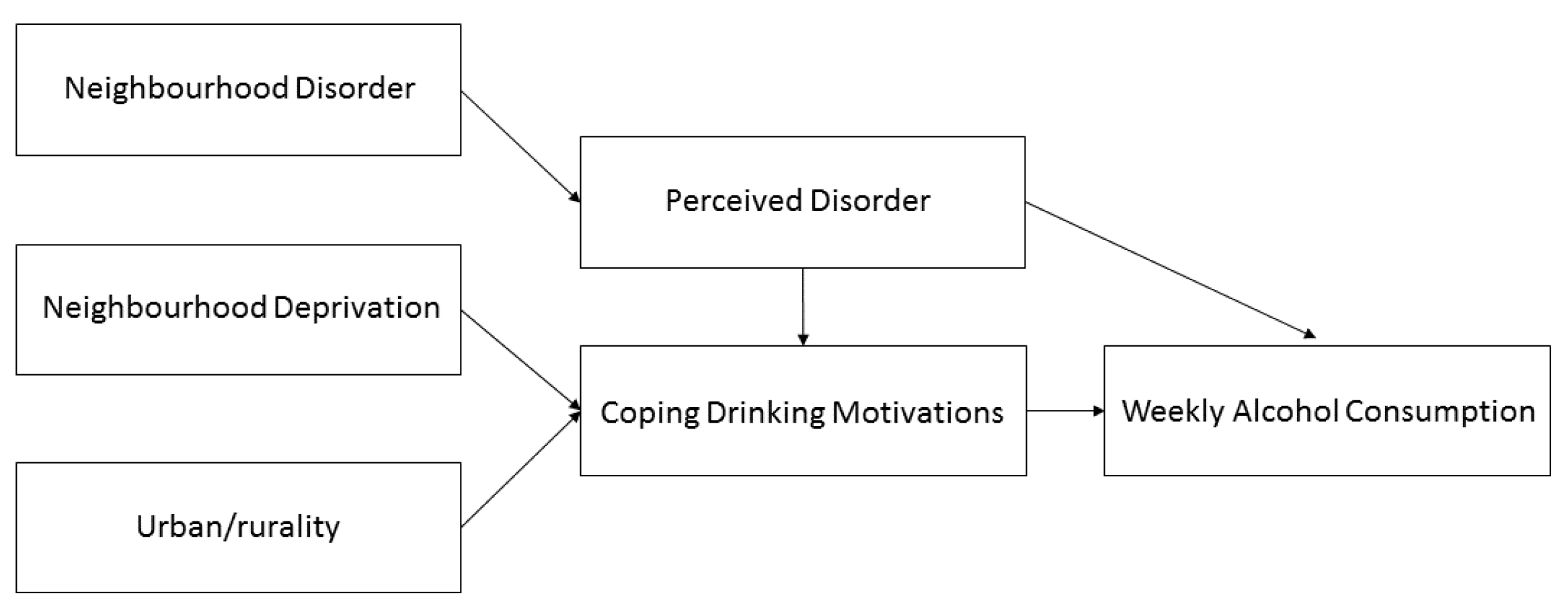
Neighborhood-level disorder was associated with coping motives indirectly through perceived disorder. Moreover, perceived disorder was associated with social and enhancement motives. This is similar to findings that perceptions of violence and robberies, as an indicator of disorder, are associated with drinking to cope [
5], highlighting that perceiving the local area as a more problematic neighborhood gives rise to stronger drinking motives generally. It is difficult to explain these relationships as they may result from an unmeasured confounding variable such as a personality trait; or it may be that observing disordered neighborhood conditions leads to a higher motivated state to drink alcohol. Future work is needed to disentangle these associations.
Those living in accessible small towns had higher coping motives than their peers living in large cities. Few studies have examined the health of adolescents residing in small towns on the periphery of larger urban areas. Research in the US examined affluent suburban adolescents compared to disadvantaged urban adolescents and found that suburban youth reported significantly higher levels of substance use than urban adolescents and that anxiety levels were also higher [
50]. However, Scottish small towns that are located near urban areas may differ substantially from affluent US suburban areas; these small-town regions are seldom examined in research and more studies are needed to understand the health behaviors of adolescents in these areas. Adolescents in such areas are often overlooked in research compared to their urban and rural peers.
Mediation analysis found that neighborhood deprivation and living in an accessible small-town were indirectly associated with weekly drinking through coping motives. This supports previous research that found the effects of neighborhood socio-economic status on substance use outcomes were likely to be indirect [
51,
52]. Additionally, as discussed above, neighborhood-level disorder had an indirect relationship with weekly drinking through perceived disorder and coping motives, further highlighting that distal exposures are often transmitted through several links in a chain [
53].
Drinking motives are a concept that may aid in better targeting and designing prevention and intervention programs for at-risk adolescents [
54,
55]. The current coping measures are based on drinking to deal with negative emotions, depression, anxiety, and low mood. Simply reducing access to alcohol for adolescents in neighborhoods at greater risk may impact on consumption but does not get to the root of why adolescents are drinking more frequently in these contexts. Therefore, public health strategies that also address the fundamental factors that lead to drinking to cope may be more effective at reducing geographic inequalities in adolescent health than those which focus solely on consumption.
This research has several strengths. First, it examines multiple conditions of the neighborhood to determine which specific conditions may be associated with adolescent drinking motives. Second, to the best of our knowledge, this is the first study which tests for a potential mediation effect of drinking motives on the relationship between neighborhood characteristics and alcohol consumption among adolescents. However, there are several limitations to consider. This work did not account for personality traits and so further work is needed to understand how personality might impact the relationship between neighborhood conditions and alcohol use. However, altering individual intrinsic factors such as personality may be more difficult than modifying or targeting the neighborhoods where young people reside. Furthermore, this study is cross-sectional, so causation cannot be inferred. Time-series analyses and evaluation studies are needed to understand the impact of changes in the neighborhood on drinking motives and alcohol use [
56]. The data on alcohol outlet density and SIMD were from two years after the HBSC data collection. Moreover, the neighborhood definitions used in this study were based on administrative boundaries, which may not align with adolescents’ perceptions of their local area.
In conclusion, of the four motives examined, only coping motives varied significantly across neighborhoods. Based on these findings, public health policies that develop adaptive strategies to improve alcohol-free methods for young people to cope better with life’s stresses may be particularly effective at reducing inequalities, if targeted at young people living in accessible small towns or areas of high neighborhood deprivation. Additionally, reduction of coping motives and regular alcohol use may be a potential side effect of improving neighborhood conditions.





{kind=link}
{kind=link}
{kind=link}
{kind=link}

