Time to Onset of Paresthesia Among Community Members Exposed to the World Trade Center Disaster


Abstract
:1. Introduction
2. Materials and Methods
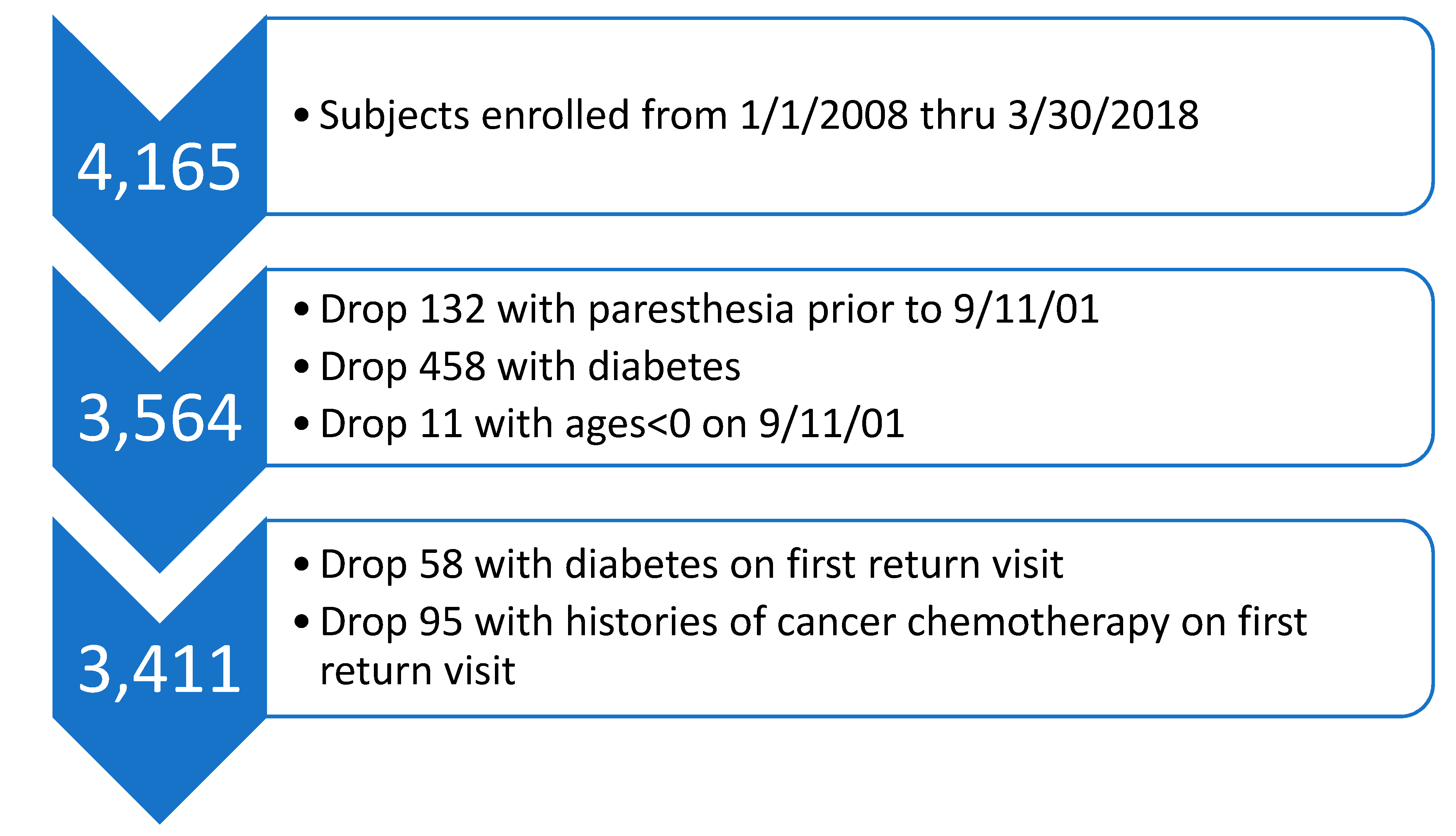
2.1. Study Population
2.2. Paresthesia
2.3. Time to Onset of Paresthesia
2.4. Statistical Analyses
3. Results
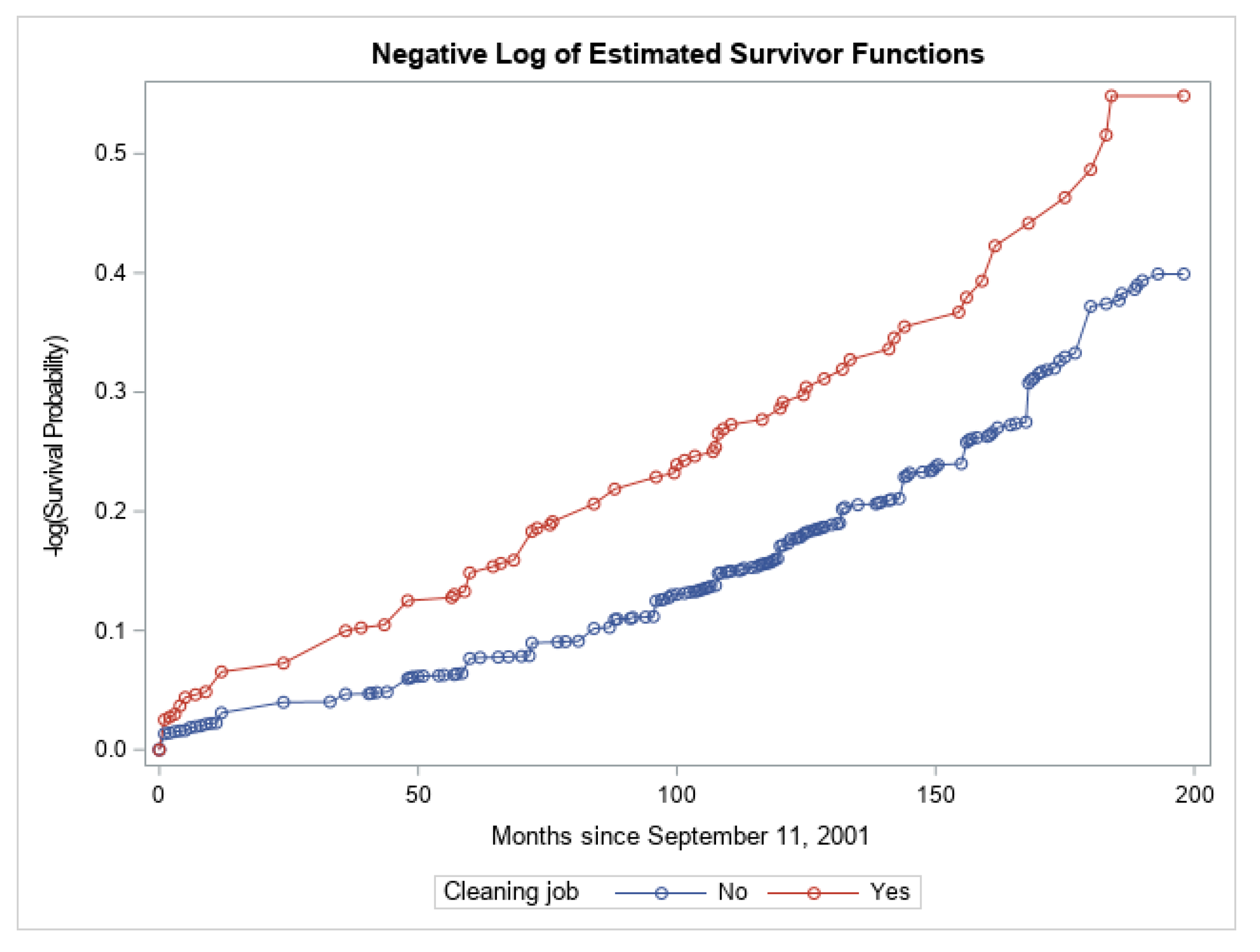
3.1. Time to Onset of Paresthesia: Nonparametric Analysis
3.2. Time to Onset of Paresthesia: Multivariate Cox Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Reibman, J.; Levy-Carrick, N.; Miles, T.; Flynn, K.; Hughes, C.; Crane, M.; Lucchini, R.G. Destruction of the World Trade Center Towers. Lessons Learned from an Environmental Health Disaster. Ann. Am. Thoracic Soc. 2016, 13, 577–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reibman, J.; Liu, M.; Cheng, Q.; Liautaud, S.; Rogers, L.; Lau, S.; Berger, K.I.; Goldring, R.M.; Marmor, M.; Fernandez-Beros, M.E.; et al. Characteristics of a residential and working community with diverse exposure to World Trade Center dust, gas, and fumes. J. Occup. Environ. Med. 2009, 51, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, N.; Morita, H.; Nakajima, T. Sarin experiences in Japan: Acute toxicity and long-term effects. J. Neurol. Sci. 2006, 249, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, B.C.; Price, R.S.; Feldman, E.L. Distal Symmetric Polyneuropathy: A Review. JAMA 2015, 314, 2172–2181. [Google Scholar] [CrossRef] [PubMed]
- Stecker, M.; Segelnick, J.; Wilkenfeld, M. Analysis of short-term effects of World Trade Center dust on rat sciatic nerve. J. Occup. Environ. Med. 2014, 56, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Lippmann, M.; Cohen, M.D.; Chen, L.C. Health effects of World Trade Center (WTC) Dust: An unprecedented disaster’s inadequate risk management. Crit. Rev. Toxicol. 2015, 45, 492–530. [Google Scholar] [CrossRef]
- Lioy, P.J.; Weisel, C.P.; Millette, J.R.; Eisenreich, S.; Vallero, D.; Offenberg, J.; Buckley, B.; Turpin, B.; Zhong, M.; Cohen, M.D.; et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ. Health Perspect. 2002, 110, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Soffritti, M.; Falcioni, L.; Bua, L.; Tibaldi, E.; Manservigi, M.; Belpoggi, F. Potential carcinogenic effects of World Trade Center dust after intratracheal instillation to Sprague-Dawley rats: First observation. Am. J. Ind. Med. 2013, 56, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Yiin, L.M.; Millette, J.R.; Vette, A.; Ilacqua, V.; Quan, C.; Gorczynski, J.; Kendall, M.; Chen, L.C.; Weisel, C.P.; Buckley, B.; et al. Comparisons of the dust/smoke particulate that settled inside the surrounding buildings and outside on the streets of southern New York City after the collapse of the World Trade Center, September 11, 2001. J. Air Waste Manag. Assoc. 2004, 54, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Thomson, R.M.; Parry, G.J. Neuropathies associated with excessive exposure to lead. Muscle Nerve 2006, 33, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Herskowitz, A.; Ishii, N.; Schaumburg, H. N-hexane neuropathy. A syndrome occurring as a result of industrial exposure. N. Engl. J. Med. 1971, 285, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Tenenbein, M.; deGroot, W.; Rajani, K.R. Peripheral neuropathy following intentional inhalation of naphtha fumes. Can. Med. Assoc. J. 1984, 131, 1077–1079. [Google Scholar]
- Marmor, M.; Shao, Y.; Bhatt, D.H.; Stecker, M.M.; Berger, K.I.; Goldring, R.M.; Rosen, R.L.; Caplan-Shaw, C.; Kazeros, A.; Pradhan, D.; et al. Paresthesias Among Community Members Exposed to the World Trade Center Disaster. J. Occup. Environ. Med. 2017, 59, 389–396. [Google Scholar] [CrossRef] [Green Version]
- Macefield, G.; Burke, D. Paraesthesiae and tetany induced by voluntary hyperventilation. Increased excitability of human cutaneous and motor axons. Brain 1991, 114 Pt 1B, 527–540. [Google Scholar] [CrossRef]
- Stecker, M.M.; Yu, H.; Barlev, R.; Marmor, M.; Wilkenfeld, M. Neurologic Evaluations of Patients Exposed to the World Trade Center Disaster. J. Occup. Environ. Med. 2016, 58, 1150–1154. [Google Scholar] [CrossRef]
- Rosen, R.L.; Levy-Carrick, N.; Reibman, J.; Xu, N.; Shao, Y.; Liu, M.; Ferri, L.; Kazeros, A.; Caplan-Shaw, C.E.; Pradhan, D.R.; et al. Elevated C-reactive protein and posttraumatic stress pathology among survivors of the 9/11 World Trade Center attacks. J. Psychiatr. Res. 2017, 89, 14–21. [Google Scholar] [CrossRef]
- De Cauwer, H.; Somville, F. Neurological disease in the aftermath of terrorism: A review. Acta. Neurol. Belg. 2018, 118, 193–199. [Google Scholar] [CrossRef]
- Barth, S.K.; Kang, H.K.; Bullman, T.A.; Wallin, M.T. Neurological mortality among U.S. veterans of the Persian Gulf War: 13-year follow-up. Am. J. Ind. Med. 2009, 52, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Herskovitz, S.S.H. Neuropathy caused by drugs. In Peripheral Neuropathy, 4th ed.; Dyck, P.J., Thomas, P.K., Eds.; Elsevier Inc.: Philadelphia, PA, USA, 2005. [Google Scholar]
- Cianchetti, C.; Abbritti, G.; Perticoni, G.; Siracusa, A.; Curradi, F. Toxic polyneuropathy of shoe-industry workers. A study of 122 cases. J. Neurol. Neurosurg. Psychiatry 1976, 39, 1151–1161. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chen, S.; Wang, Z. Electrophysiological follow-up of patients with chronic peripheral neuropathy induced by occupational intoxication with n-hexane. Cell Biochem. Biophys. 2014, 70, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.R.; Schaumburg, H.H. Human toxic neuropathy caused by industrial agents. In Peripheral Neuropathy, 4th ed.; Dyck, P.J., Thomas, P.K., Eds.; Elsevier Inc.: Philadelphia, PA, USA, 2005. [Google Scholar]
- Weiss, D.; Tomasallo, C.D.; Meiman, J.G.; Alarcon, W.; Graber, N.M.; Bisgard, K.M.; Anderson, H.A. Elevated Blood Lead Levels Associated with Retained Bullet Fragments—United States, 2003–2012. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 130–133. [Google Scholar] [CrossRef]
- Johannsen, L.; Smith, T.; Havsager, A.M.; Madsen, C.; Kjeldsen, M.J.; Dalsgaard, N.J.; Gaist, D.; Schroder, H.D.; Sindrup, S.H. Evaluation of patients with symptoms suggestive of chronic polyneuropathy. J. Clin. Neuromuscul. Dis. 2001, 3, 47–52. [Google Scholar] [CrossRef]
- Lubec, D.; Mullbacher, W.; Finsterer, J.; Mamoli, B. Diagnostic work-up in peripheral neuropathy: An analysis of 171 cases. Postgrad. Med. J. 1999, 75, 723–727. [Google Scholar] [CrossRef]
- Mengel, D.; Fraune, L.; Sommer, N.; Stettner, M.; Reese, J.P.; Dams, J.; Glynn, R.J.; Balzer-Geldsetzer, M.; Dodel, R.; Tackenberg, B. Costs of illness in chronic inflammatory demyelinating polyneuropathy in Germany. Muscle Nerve 2018, 58, 681–687. [Google Scholar] [CrossRef]
- Rajabally, Y.A.; Seri, S.; Cavanna, A.E. Neuropsychiatric manifestations in inflammatory neuropathies: A systematic review. Muscle Nerve 2016, 54, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kerckhove, N.; Collin, A.; Conde, S.; Chaleteix, C.; Pezet, D.; Balayssac, D. Long-Term Effects, Pathophysiological Mechanisms, and Risk Factors of Chemotherapy-Induced Peripheral Neuropathies: A Comprehensive Literature Review. Front Pharmacol. 2017, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Salinero-Fort, M.A.; Gomez-Campelo, P.; San Andres-Rebollo, F.J.; Cardenas-Valladolid, J.; Abanades-Herranz, J.C.; Carrillo de Santa Pau, E.; Chico-Moraleja, R.M.; Beamud-Victoria, D.; de Miguel-Yanes, J.M.; Jimenez-Garcia, R.; et al. Prevalence of depression in patients with type 2 diabetes mellitus in Spain (the DIADEMA Study): Results from the MADIABETES cohort. BMJ Open 2018, 8, e020768. [Google Scholar] [CrossRef]
- Zafeiri, M.; Tsioutis, C.; Kleinaki, Z.; Manolopoulos, P.; Ioannidis, I.; Dimitriadis, G. Clinical Characteristics of Patients with co-Existent Diabetic Peripheral Neuropathy and Depression: A Systematic Review. Exp. Clin. Endocrinol. Diabetes 2018. [Google Scholar] [CrossRef]
- Bharucha, N.E.; Bharucha, A.E.; Bharucha, E.P. Prevalence of peripheral neuropathy in the Parsi community of Bombay. Neurology 1991, 41, 1315–1317. [Google Scholar] [CrossRef]
- Savettieri, G.; Rocca, W.A.; Salemi, G.; Meneghini, F.; Grigoletto, F.; Morgante, L.; Reggio, A.; Costa, V.; Coraci, M.A.; Di Perri, R. Prevalence of diabetic neuropathy with somatic symptoms: A door-to-door survey in two Sicilian municipalities. Sicilian Neuro-Epidemiologic Study (SNES) Group. Neurology 1993, 43, 1115–1120. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value | N at Baseline | N (%) with Return | N (%) without Return | p-Value |
|---|---|---|---|---|---|
| Gender | 0.4 | ||||
| Female | 1811 | 711 (39.3) | 1100 (60.7) | ||
| Male | 1753 | 662 (37.8) | 1091 (62.2) | ||
| Age on 911 | <0.0001 | ||||
| <35 | 967 | 302 (31.2) | 665 (68.8) | ||
| 35–44 | 1155 | 452 (39.1) | 703 (60.9) | ||
| 45–54 | 1022 | 435 (42.6) | 587 (57.4) | ||
| 55–64 | 356 | 156 (43.8) | 200 (56.2) | ||
| ≥65 | 64 | 28 (43.8) | 36 (56.2) | ||
| Year of enrollment | <0.0001 | ||||
| 2008–2010 | 1432 | 746 (52.1) | 686 (47.9) | ||
| 2011–2013 | 817 | 381 (46.6) | 436 (53.4) | ||
| 2014–2015 | 538 | 197 (36.6) | 341 (63.4) | ||
| 2016–2018 | 777 | 49 (6.3) | 728 (93.7) | ||
| Race/Ethnicity | <0.0001 | ||||
| Hispanic | 799 | 382 (47.8) | 417 (52.2) | ||
| Non-Hispanic Caucasian | 1713 | 566 (33.0) | 1147 (67.0) | ||
| Non-Hispanic African-American | 705 | 294 (41.7) | 411 (58.3) | ||
| Asian | 263 | 93 (35.4) | 170 (64.6) | ||
| Other or Native American | 47 | 16 (34.0) | 31 (66.0) | ||
| Missing race/ethnicity | 37 |
| Variable | Value | N (Column %) |
|---|---|---|
| Gender | ||
| Male | 1681 (49.3) | |
| Female | 1730 (50.7) | |
| Age at enrollment (years) | ||
| <25 | 138 (4.0) | |
| 25–34 | 231 (6.8) | |
| 35–44 | 552 (16.2) | |
| 45–54 | 1006 (29.5) | |
| 55–64 | 1001 (29.3) | |
| ≥65 | 483 (14.2) | |
| Median age at enrollment (IQR) 53(44–61) | ||
| Year of enrollment | 2008–2010 | 1372 (40.2) |
| 2011–2013 | 776 (22.8) | |
| 2014–2015 | 499 (14.6) | |
| 2016–2018 | 764 (22.4) | |
| Race and ethnicity | ||
| Hispanic | 765 (22.4) | |
| Non-Hispanic Caucasian | 1635 (47.9) | |
| Non-Hispanic African- American | 675 (19.8) | |
| Asian | 258 (7.6) | |
| Other or Native American | 44 (1.3) | |
| Missing | 34 (1.0) | |
| Subjects reported paresthesia | Yes | 605 (17.7) |
| No | 2806 (82.3) | |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|
| Gender | F vs. M | 1.14 | 0.99 | 1.33 | 0.08 |
| Age on 911 (years) | Per unit increase | 1.01 | 1.01 | 1.02 | <0.0001 |
| Race-Ethnicity (vs. Non-Hispanic Caucasian) | Hispanic | 1.24 | 1.03 | 1.50 | 0.03 |
| Non-Hispanic African-American | 1.12 | 0.92 | 1.37 | 0.2 | |
| Asian | 0.85 | 0.61 | 1.18 | 0.3 | |
| Other or Native-American | 1.83 | 1.07 | 3.13 | 0.03 | |
| Cleaning Job | Yes vs. No | 1.37 | 1.11 | 1.69 | 0.003 |
| Covered in Dust | Much vs. Little | 1.09 | 0.94 | 1.27 | 0.2 |
| Body mass index (kg/m2) | Per unit increase | 1.02 | 1.01 | 1.03 | 0.001 |
| Anxiety (vs. <1.75) | ≥1.75 | 1.37 | 1.10 | 1.71 | 0.006 |
| Missing | 1.45 | 0.28 | 7.58 | 0.7 | |
| Post-Traumatic Stress Disorder (vs. PCL*- < 44) | PCL ≥ 44 | 1.29 | 1.04 | 1.59 | 0.02 |
| Missing | 0.98 | 0.19 | 5.14 | 0.9 | |
| Depression (vs. <1.75) | ≥1.75 | 1.41 | 1.13 | 1.76 | 0.002 |
| Missing | 1.45 | 0.28 | 7.58 | 0.7 | |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|
| Gender | F vs. M | 1.22 | 1.05 | 1.41 | 0.01 |
| Age on 911 (years) | Per unit increase | 1.01 | 1.01 | 1.02 | <0.0001 |
| Race-Ethnicity (vs. Non-Hispanic Caucasian) | Hispanic | 0.85 | 0.61 | 1.18 | 0.3 |
| Non-Hispanic African-American | 1.32 | 1.09 | 1.59 | 0.004 | |
| Asian | 1.29 | 1.06 | 1.57 | 0.0106 | |
| Other or Native-American | 1.75 | 1.02 | 2.99 | 0.04 | |
| Cleaning Job | Yes vs. No | 1.52 | 1.24 | 1.87 | <0.0001 |
| Covered in Dust | Much vs. Little | 1.19 | 1.03 | 1.38 | 0.02 |
| Body mass index (kg/m2) | Per unit increase | 1.02 | 1.01 | 1.03 | 0.0007 |
| Anxiety (vs. <1.75) | ≥1.75 | 1.51 | 1.21 | 1.89 | 0.0002 |
| Missing | 1.10 | 0.25 | 4.82 | 0.9 | |
| Post-Traumatic Stress Disorder (vs. PCL < 44) | PCL ≥ 44 | 1.35 | 1.09 | 1.67 | 0.006 |
| Missing | 1.42 | 0.32 | 6.27 | 0.6 | |
| Depression (vs. <1.75) | ≥1.75 | 1.49 | 1.19 | 1.85 | 0.0004 |
| Missing | 1.10 | 0.25 | 4.82 | 0.9 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thawani, S.; Wang, B.; Shao, Y.; Reibman, J.; Marmor, M. Time to Onset of Paresthesia Among Community Members Exposed to the World Trade Center Disaster. Int. J. Environ. Res. Public Health 2019, 16, 1429. https://doi.org/10.3390/ijerph16081429
Thawani S, Wang B, Shao Y, Reibman J, Marmor M. Time to Onset of Paresthesia Among Community Members Exposed to the World Trade Center Disaster. International Journal of Environmental Research and Public Health. 2019; 16(8):1429. https://doi.org/10.3390/ijerph16081429
Chicago/Turabian StyleThawani, Sujata, Bin Wang, Yongzhao Shao, Joan Reibman, and Michael Marmor. 2019. "Time to Onset of Paresthesia Among Community Members Exposed to the World Trade Center Disaster" International Journal of Environmental Research and Public Health 16, no. 8: 1429. https://doi.org/10.3390/ijerph16081429