Development and Validation of a Homemade, Low-Cost Laparoscopic Simulator for Resident Surgeons (LABOT)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. How to Build LABOT
- plywood
- medium density fibreboard (MDF)
- rubber (to place the trocar)
- neon lamp (30 cm long)
- bullet mini camera
- low-cost lamp (such as an Ikea lamp, JANSJO®)
- screws
- angle Bracket (1 cm large)
- bolt (to fix the camera)
- insulating tape.
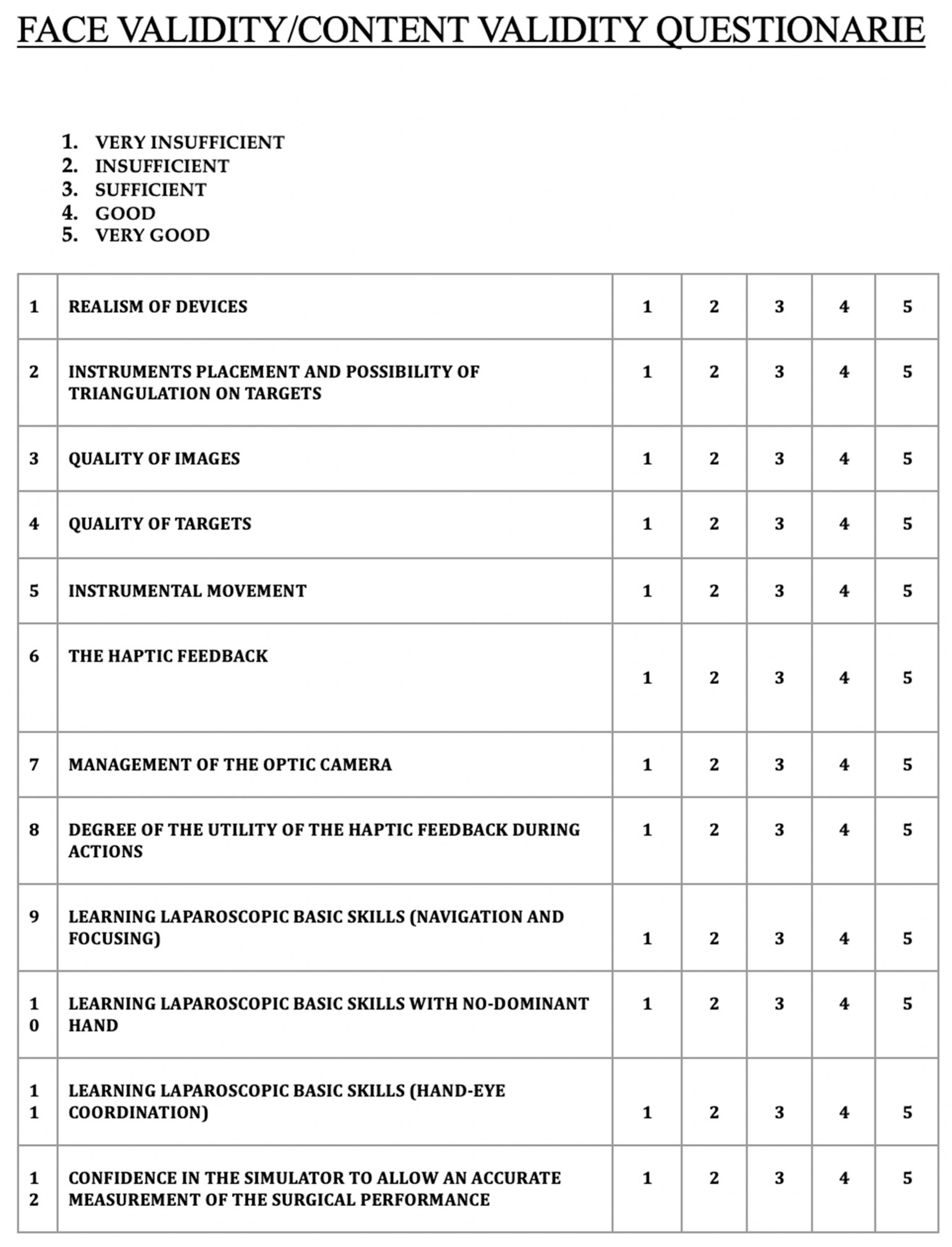
2.2. Validation Process
- simulating the surgical reality;
- having a positive impact on the operator’s learning (learning curve);
- obtaining satisfactory ergonomic results.
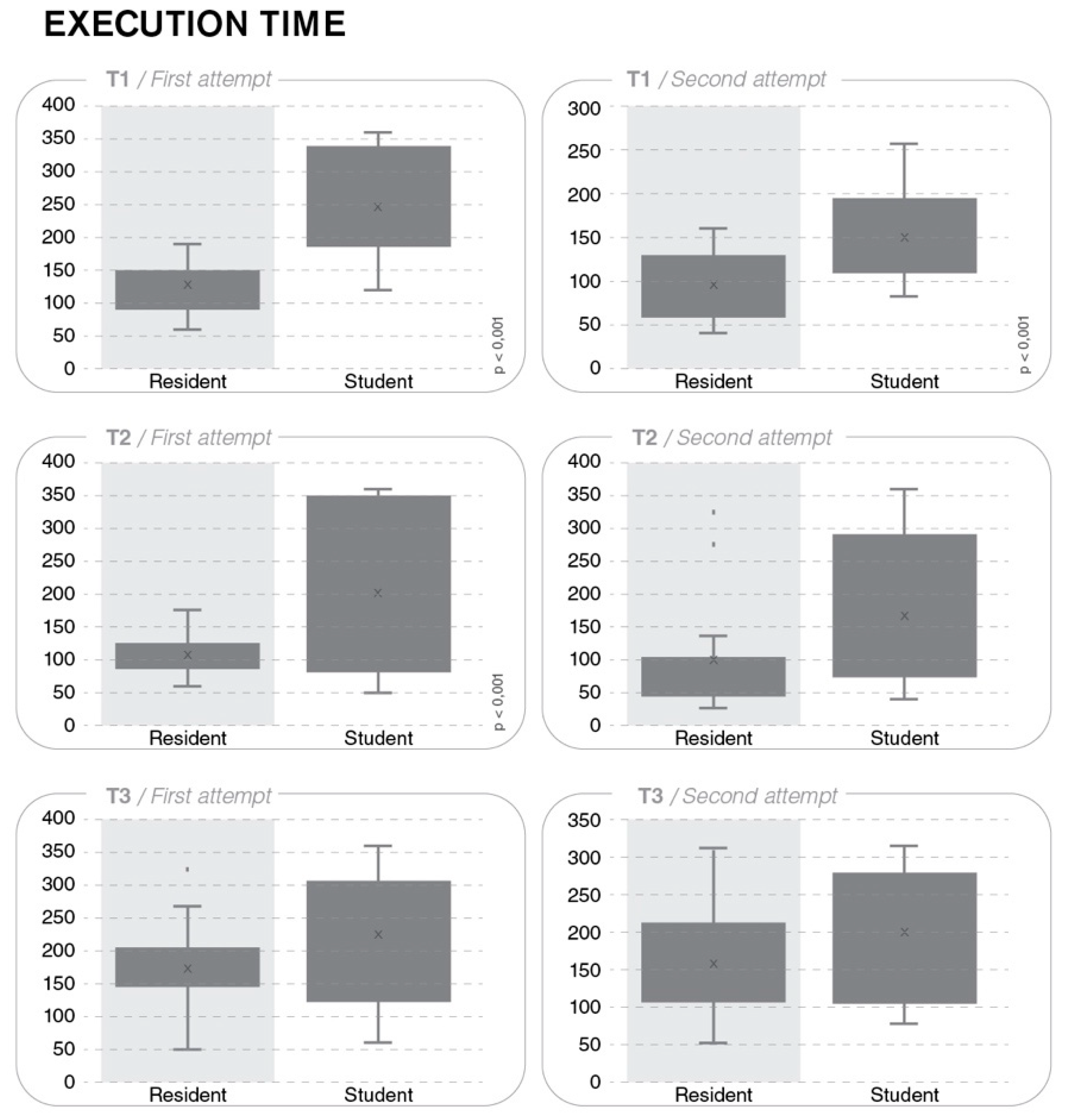
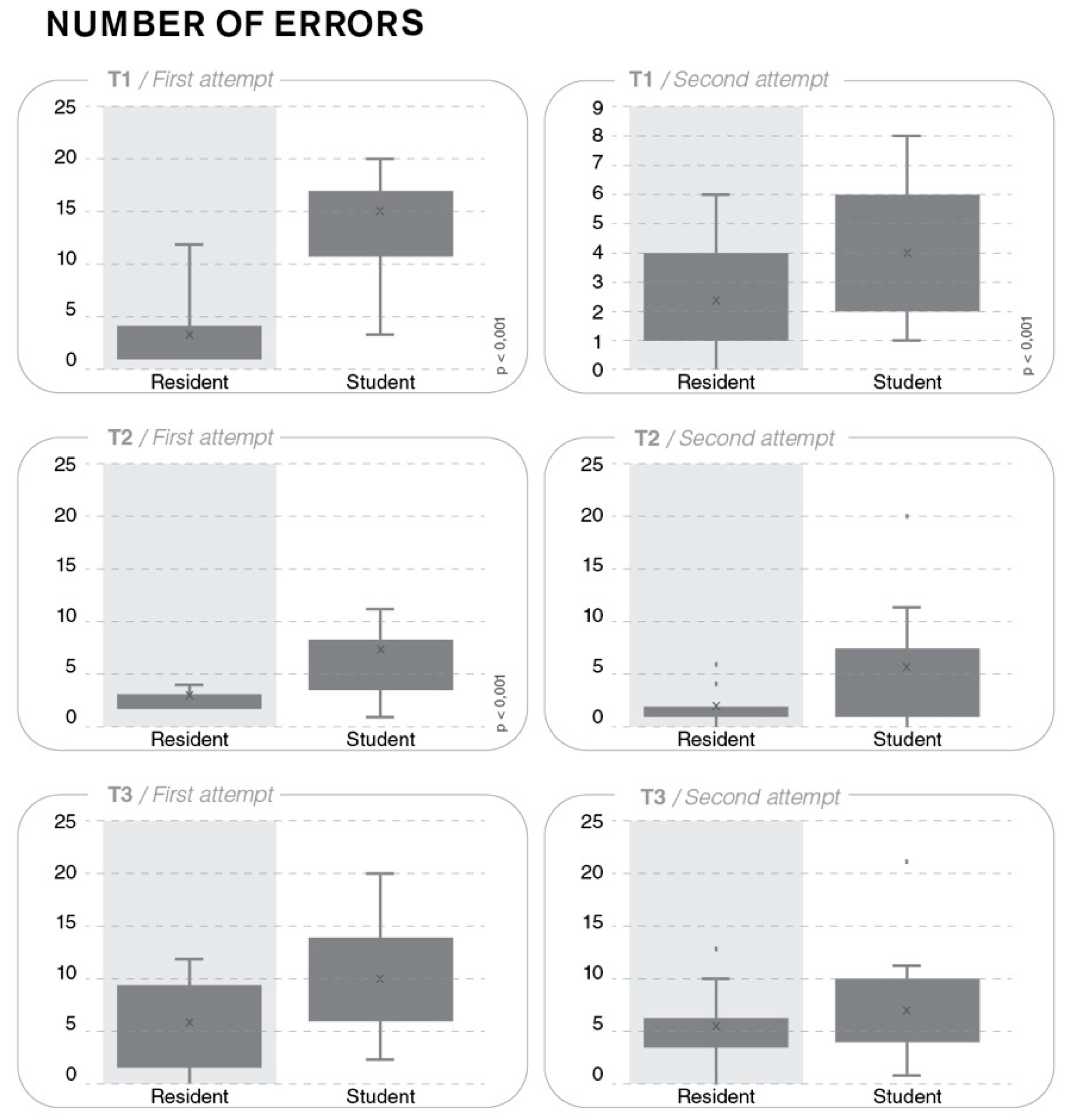
- T1 consisted of passing a thread through a ring path; not entering the wire into the ring and an accidental fall of the wire were judged as procedural errors.
- T2 consisted of putting five bolts on top of each other; dropping the bolt was judged a procedural error.
- T3 consisted of passing a bolt from one hand to the other and putting it in a box by using two atraumatic forceps (Joannes type) with the repetition of this procedure five times; dropping the bolt, non-centering, and displacing the box were judged as procedural errors.
2.3. Statistical Analysis
3. Results
3.1. T1 Task
3.2. T2 Task
3.3. T3 Task
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
Instructions for Building LABOT
References
- Kavanagh, D.; Gibson, D.; Moran, D.C.; Smith, M.; Donnell, K.O.; Eguare, E.; Keane, F.B.V.; Riordain, D.S.O.; Neary, P.C. Short-term outcomes following laparoscopic resection for colon cancer. Int. J. Colorectal Dis. 2011, 26, 361–368. [Google Scholar] [CrossRef]
- Yiasemidou, M.; de Siqueira, J.; Tomlinson, J.; Glassman, D.; Stock, S.; Gough, M. Take-home box trainers are an effective alternative to virtual reality simulators. J. Surg. Res. 2017, 213, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Salkini, M.W.; Hamilton, A.J. The effect of age on acquiring laparoscopic skills. J. Endourol. 2010, 24, 377–379. [Google Scholar] [CrossRef]
- Aggarwal, R.; Moorthy, K. Laparoscopic skills training and assessment. Br. J. Surg. 2004, 91, 1549–1558. [Google Scholar] [CrossRef]
- Gaba, D.M. The future vision of simulation in health care. Qual. Saf. Health Care 2004, 13, i2–i10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickel, F.; Brzoska, J.A.; Gondan, M.; Rangnick, H.M.; Chu, J.; Kenngott, H.G.; Linke, G.R.; Kadmon, M.; Fischer, L.; Müller-Stich, B.P. Virtual reality training versus blended learning of laparoscopic cholecystectomy. A randomized controlled trial with laparoscopic novices. Medicine 2005, 94, e764. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.R.; Soerensen, J.L.; Grantcharov, T.P.; Dalsgaard, T.; Schouenborg, L.; Ottosen, C.; Schroeder, T.V.; Ottesen, B.S. Effect of virtual reality training on laparoscopic surgery: Randomised controlled trial. BMJ 2009, 338, b1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, N.E.; Gallagher, A.G.; Roman, S.A.; O’Brien, M.K.; Bansal, V.K.; Andersen, D.K.; Satava, R.M. Virtual reality training improves operating room performance: Results of a randomized, double-blinded study. Ann. Surg. 2002, 236, 458–463. [Google Scholar] [CrossRef]
- Montanari, E.; Schwameis, R.; Louridas, M.; Göbl, C.; Kuessel, L.; Polterauer, S.; Husslein, H. Training on an inexpensive tablet-based device is equally effective as on a standard laparoscopic box trainer. A randomized controlled trial. Medicine 2016, 95, e4826. [Google Scholar] [CrossRef] [PubMed]
- Sackier, J.M.; Berci, G.; Paz-Partlow, M. A new training device for laparoscopic cholecystectomy. Surg. Endosc. 1991, 5, 158–159. [Google Scholar] [CrossRef] [PubMed]
- Li, M.M.; George, J. A systematic review of low-cost laparoscopic simulators. Surg. Endosc. 2016, 31, 38–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oti, A.T.; Galvão, L.N.; Pessoa, T.C.P.; Rocha, C.R.O.; Monteiro, A.M.; Fonteles, M.J.P.; Brito, M.V.H.; Yasojima, E.Y. Development of a laparoscopic training model using a smartphone. Revista do Colégio Brasileiro de Cirurgiões 2017, 44, 471–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Couto, R.S.; Veloso, A.D.C.; Antunes, F.G.; Ferrari, R.; Carneiro, R.G.F. Device model for training of laparoscopic surgical skills. Revista do Colégio Brasileiro de Cirurgiões 2015, 42, 418–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslam, A.; Nason, G.J.; Giri, S.K. Homemade laparoscopic surgical simulator: A cost-effective solution to the challenge of acquiring laparoscopic skills? Ir. J. Med. Sci. 2016, 185, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Thinggaard, E.; Bjerrum, F.; Strandbygaard, J.; Gögenur, I.; Konge, L. Validity of a cross-specialty test in basic laparoscopic techniques. Br. J. Surg. 2015, 102, 1106–1113. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekera, S.K.; Donohue, J.F.; Orley, D.; Barber, N.J.; Shah, N.; Bishai, P.M.; Muir, G.H. Basic laparoscopic surgical training: Examination of a low-cost alternative. Eur. Urol. 2006, 50, 1285–1291. [Google Scholar] [CrossRef]
- Kenney, P.A.; Wszolek, M.F.; Gould, J.J.; Libertino, J.A.; Moinzadeh, A. Face, Content, and Construct Validity of dV-Trainer, a Novel Virtual Reality Simulator for Robotic Surgery. Urology 2009, 73, 1288–1292. [Google Scholar] [CrossRef]
- Xiao, D.; Jakimowic, J.J.; Albayrak, A.; Buzink, S.N.; Botden, S.M.B.I.; Goossens, R.H.M. Face, Content, and Construct Validity of a Novel Portable Ergonomic Simulator for Basic Laparoscopic Skills. J. Surg. Educ. 2014, 71, 65–72. [Google Scholar] [CrossRef]
- Brewin, J.; Nedas, T.; Challacombe, B.; Elhage, O.; Keisu, J.; Dasgupta, P. Face, content and construct validation of the first virtual reality laparoscopic nephrectomy simulator. BJU Int. 2010, 106, 850–854. [Google Scholar] [CrossRef]
- Escamirosa, F.P.; Flores, R.M.O.; García, I.O.; Vidal, C.R.Z.; Martínez, A.M. Face, content, and construct validity of the EndoViS training system for objective assessment of psychomotor skills of laparoscopic surgeons. Surg. Endosc. 2015, 29, 3392–3403. [Google Scholar] [CrossRef] [Green Version]
- Leijte, E.; Arts, E.; Witteman, B.; Jakimowicz, J.; Blaauw, I.V.; Botden, S. Construct, content and face validity of the eoSim laparoscopic simulator on advanced suturing tasks. Surg. Endosc. 2019, 33, 3635–3643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons, C.; Goldfarb, D.; Jones, S.L.; Badhiwala, N.; Miles, B.; Link, R.; Dunkin, B.J. Which skills really matter? proving face, content, and construct validity for a commercial robotic simulator. Surg. Endosc. 2013, 27, 2020–2030. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Perez, M.; Perrenot, C.; Hubert, N.; Hubert, J. Face, content, construct, and concurrent validity of a novel robotic surgery patient-side simulator: The Xperience TM Team Trainer. Surg. Endosc. 2016, 30, 3334–3344. [Google Scholar] [CrossRef] [PubMed]
- Pokorny, M.R.; McLaren, S.L. Inexpensive home-made laparoscopic trainer and camera. ANZ J. Surg. 2004, 74, 691–693. [Google Scholar] [CrossRef] [PubMed]
- Beatty, J.D. How to build an inexpensive laparoscopic webcam-based trainer. BJU Int. 2005, 96, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Rivas, A.M.; Vilanova, A.C.; Pereferrer, F.S.; González, M.H.; Déjardin, D.C. Low cost simulator for acquiring basic laparoscopic skills. Cirugía Española 2010, 87, 26–32. [Google Scholar] [CrossRef]
- Kiely, D.J.; Stephanson, K.; Ross, S. Assessing image quality of low-cost laparoscopic box trainers: Options for residents training at home. Simul. Healthc. 2011, 6, 292–298. [Google Scholar] [CrossRef]
- Kobayashi, S.A.; Jamshidi, R.; O’Sullivan, P.; Palmer, B.; Hirose, S.; Stewart, L.; Kim, H.K. Bringing the skills laboratory home: An affordable webcam-based personal trainer for developing laparoscopic skills. J. Surg. Educ. 2011, 68, 105–109. [Google Scholar] [CrossRef]
- Moreira-Pinto, J.; Silva, J.G.; Castro, J.L.R.; Correia-Pinto, J. Five really easy steps to build a homemade low-cost simulator. Surg. Innov. 2013, 20, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Beard, J.H.; Akoko, L.; Mwanga, A.; Mkony, C.; O’Sullivan, P. Manual laparoscopic skills development using a low-cost trainer box in Tanzania. J. Surg. Educ. 2014, 71, 85–90. [Google Scholar] [CrossRef]
- Walczak, D.A.; Piotrowski, P.; Jędrzejczyk, A.; Pawełczak, D.; Pasiek, Z. A laparoscopic simulator—Maybe it is worth making it yourself. Wideochir. Inne Tech. Maloinwazyjne 2014, 9, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khine, M.; Leung, E.; Morran, C.; Muthukumarasamy, G. Homemade laparoscopic simulators for surgical trainees. Clin. Teach. 2011, 8, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.K.; Kushner, D.M. Development and validation of a home-based, mirrored, gynecologic laparoscopy trainer. J. Minim. Invasive Gynecol. 2006, 13, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Mughal, M. A cheap laparoscopic surgery trainer. Ann. R. Coll. Surg. Engl. 1992, 74, 256–257. [Google Scholar]
- Sharpe, B.A.; MacHaidze, Z.; Ogan, K. Randomized comparison of standard laparoscopic trainer to novel, at-home, low cost, camera-less laparoscopic trainer. Urology 2005, 66, 50–54. [Google Scholar] [CrossRef]
- Ghesquiere, L.; Garabedian, C.; Boukerrou, M.; Dennis, T.; Garbin, O.; Hery, R.; Rubod, C.; Cosson, M. Implementation of a laparoscopy surgery training via simulation in a low-income country. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 187–190. [Google Scholar] [CrossRef]
- Kristin, L.; Spears, C.; Kenady, D.E.; Roth, J.S. Implementation of a low-cost laparoscopic skills curriculum in a third-world setting. Journal of surgical education. J. Surg. Educ. 2014, 71, 860–864. [Google Scholar]
- Damas, E.; Norcéide, C.; Zephyr, Y.; Williams, K.; Renouf, T.; Dubrowski, A. Development of a sustainable simulator and simulation program for laparoscopic skills training in Haiti. Cureus 2016, 8, e623. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Undergone Validation | Yes (43%) | No (57%) | |||
| Figure for cost | Yes (46%) | No (54%) | |||
| Abdominal Wall | Plastic (52%) | Cardboard (16%) | Plywood (5%) | Others (27%) | |
| Light Source | External light (36%) | Laparoscope (16%) | Desk lapm (12.5%) | LED (7%) | Others (28.5%) |
| Visualization | TV o PC screen Phone and digital Camera (61%) | Laparoscope (23%) | Direct vision (3.5%) | Mirror (3.5%) | Others (9%) |
| Monitor | PC, tablet, laptop (34%) | TV screen (25%) | Video monitor (16%) | Other (25%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soriero, D.; Atzori, G.; Barra, F.; Pertile, D.; Massobrio, A.; Conti, L.; Gusmini, D.; Epis, L.; Gallo, M.; Banchini, F.; et al. Development and Validation of a Homemade, Low-Cost Laparoscopic Simulator for Resident Surgeons (LABOT). Int. J. Environ. Res. Public Health 2020, 17, 323. https://doi.org/10.3390/ijerph17010323
Soriero D, Atzori G, Barra F, Pertile D, Massobrio A, Conti L, Gusmini D, Epis L, Gallo M, Banchini F, et al. Development and Validation of a Homemade, Low-Cost Laparoscopic Simulator for Resident Surgeons (LABOT). International Journal of Environmental Research and Public Health. 2020; 17(1):323. https://doi.org/10.3390/ijerph17010323
Chicago/Turabian StyleSoriero, Domenico, Giulia Atzori, Fabio Barra, Davide Pertile, Andrea Massobrio, Luigi Conti, Dario Gusmini, Lorenzo Epis, Maurizio Gallo, Filippo Banchini, and et al. 2020. "Development and Validation of a Homemade, Low-Cost Laparoscopic Simulator for Resident Surgeons (LABOT)" International Journal of Environmental Research and Public Health 17, no. 1: 323. https://doi.org/10.3390/ijerph17010323