Sleep Regularity Index in Patients with Alcohol Dependence: Daytime Napping and Mood Disorders as Correlates of Interest

Abstract
:1. Introduction
Purpose of Study
2. Materials and Methods
2.1. Sleep Measures
2.1.1. Pittsburgh Sleep Quality Index (PSQI)
2.1.2. Sleep and Symptom Diary
2.1.3. Epworth Sleepiness Scale (ESS)
2.1.4. Actigraphy
2.1.5. Calculation of the Sleep Regularity Index
2.1.6. Filtering of Actigraphy Data
2.1.7. Clinical Institute Withdrawal Assessment—Alcohol Revised (CIWA-Ar)
2.1.8. Structured Clinical Interview for DSM-IV Axis I Disorders (SCID)
2.1.9. Timeline Followback (TLFB)
2.1.10. Comprehensive Pathological Rating Scale (CPRS)
2.1.11. Penn Alcohol Craving Scale (PACS)
2.1.12. Data Analysis
3. Sample and Demographics
Participant Exclusion Filtering Results
4. Results
4.1. SRI and Assessment of Other Sleep Variables (Aims #1 and #2)
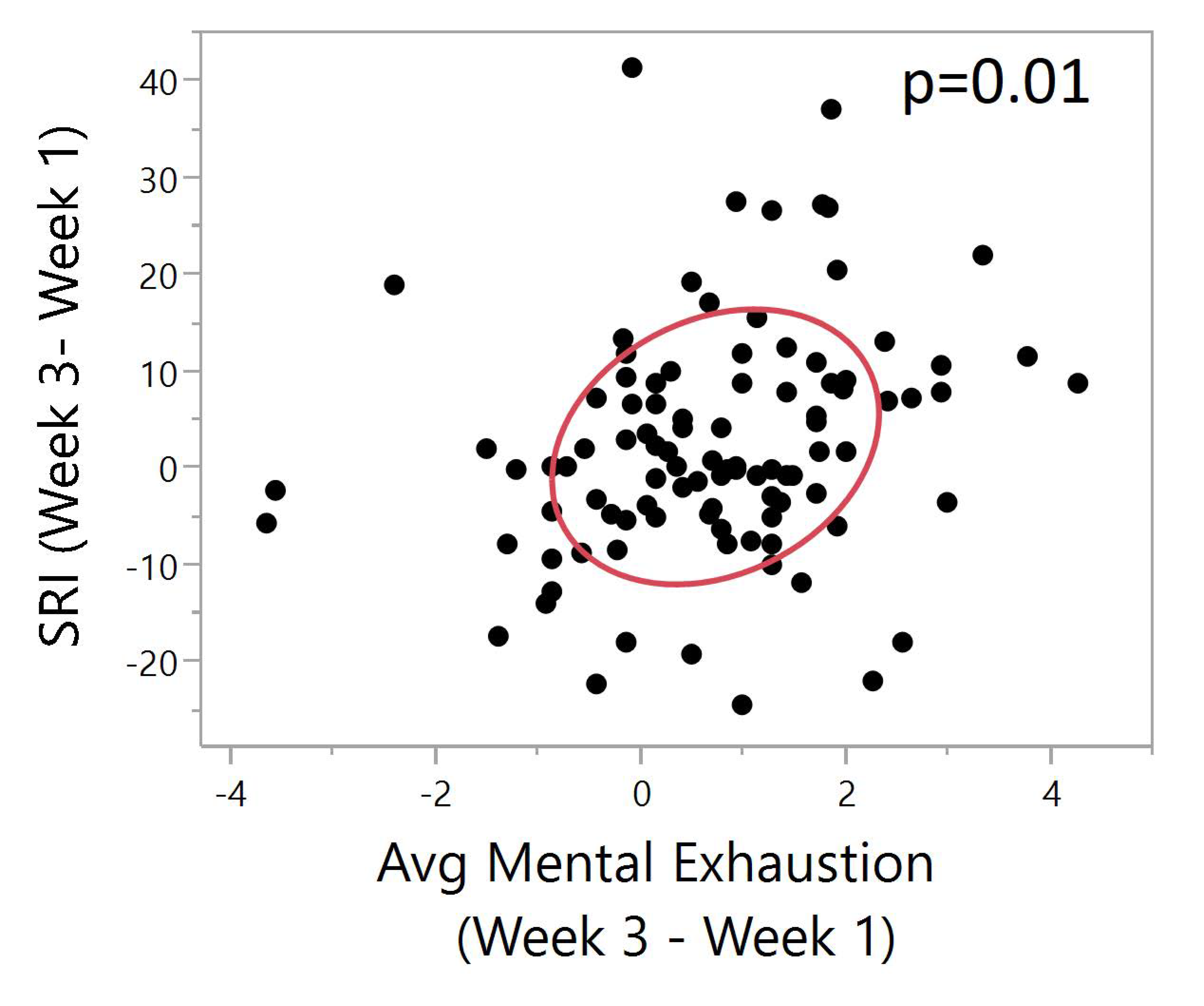
4.2. Correlating SRI with Clinical Variables (Aim #3)
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Global Status Report on Alcohol and Health. Available online: https://apps.who.int/iris/bitstream/handle/10665/312318/WHO-MSD-MSB-18.2-eng.pdf?sequence=1&isAllowed=y (accessed on 30 September 2019).
- NIAAA. Available online: https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/alcohol-use-disorders (accessed on 2 January 2020).
- Stein, M.D.; Friedmann, P.D. Disturbed sleep and its relationship to alcohol use. Subst. Abus. 2005, 26, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koob, G.F.; Colrain, I.M. Alcohol use disorder and sleep disturbances: A feed-forward allostatic framework. Neuropsychopharmacology 2020, 45, 141–165. [Google Scholar] [CrossRef] [PubMed]
- Farhud, D.; Aryan, Z. Circadian Rhythm, Lifestyle and Health: A Narrative Review. Iran. J. Public Health 2018, 47, 1068–1076. [Google Scholar] [PubMed]
- Zhu, L.; Zee, P.C. Circadian rhythm sleep disorders. Neurol. Clin. 2012, 30, 1167–1191. [Google Scholar] [CrossRef] [Green Version]
- Thakkar, M.M.; Sharma, R.; Sahota, P. Alcohol disrupts sleep homeostasis. Alcohol 2015, 49, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Hasler, B.P.; Kirisci, L.; Clark, D.B. Restless Sleep and Variable Sleep Timing During Late Childhood Accelerate the Onset of Alcohol and Other Drug Involvement. J. Stud. Alcohol Drugs 2016, 77, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Hasler, B.P.; Pedersen, S.L. Sleep and circadian risk factors for alcohol problems: A brief overview and proposed mechanisms. Curr. Opin. Psychol. 2020, 34, 57–62. [Google Scholar] [CrossRef]
- Phillips, A.J.K.; Clerx, W.M.; O’Brien, C.S.; Sano, A.; Barger, L.K.; Picard, R.W.; Lockley, S.W.; Klerman, E.B.; Czeisler, C.A. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci. Rep. 2017, 7, 3216. [Google Scholar] [CrossRef]
- Ford, D.E.; Kamerow, D.B. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA 1989, 262, 1479–1484. [Google Scholar] [CrossRef]
- Brower, K.J.; Aldrich, M.S.; Robinson, E.A.; Zucker, R.A.; Greden, J.F. Insomnia, self-medication, and relapse to alcoholism. Am. J. Psychiatry 2001, 158, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Brower, K.J.; Perron, B.E. Sleep disturbance as a universal risk factor for relapse in addictions to psychoactive substances. Med. Hypotheses 2010, 74, 928–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.B.; Donahue, M.L.; Carey, K.B.; Scott-Sheldon, L.A.J. Insomnia treatment in the context of alcohol use disorder: A systematic review and meta-analysis. Drug Alcohol Depend. 2017, 181, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.T.; Krumlauf, M.; Fryer, C.S.; Beck, K.H.; Yang, L.; Ramchandani, V.A.; Wallen, G.R. Critical Transitions: A Mixed Methods Examination of Sleep from Inpatient Alcohol Rehabilitation Treatment to the Community. PLoS ONE 2016, 11, e0161725. [Google Scholar] [CrossRef] [PubMed]
- Lunsford-Avery, J.R.; Engelhard, M.M.; Navar, A.M.; Kollins, S.H. Validation of the Sleep Regularity Index in Older Adults and Associations with Cardiometabolic Risk. Sci. Rep. 2018, 8, 14158. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.M.; Phillips, A.J.K.; Magee, M.; Sletten, T.L.; Gordon, C.; Lovato, N.; Bei, B.; Bartlett, D.J.; Kennaway, D.J.; Lack, L.C.; et al. Sleep regularity is associated with sleep-wake and circadian timing, and mediates daytime function in Delayed Sleep-Wake Phase Disorder. Sleep Med. 2019, 58, 93–101. [Google Scholar] [CrossRef]
- Bei, B.; Wiley, J.F.; Trinder, J.; Manber, R. Beyond the mean: A systematic review on the correlates of daily intraindividual variability of sleep/wake patterns. Sleep Med. Rev. 2016, 28, 108–124. [Google Scholar] [CrossRef] [Green Version]
- Wallen, G.R.; Brooks, A.T.; Whiting, B.; Clark, R.; Krumlauf, M.C.; Yang, L.; Schwandt, M.L.; George, D.T.; Ramchandani, V.A. The prevalence of sleep disturbance in alcoholics admitted for treatment: A target for chronic disease management. Fam. Community Health 2014, 37, 288–297. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, M. Daytime sleepiness, snoring, and obstructive sleep apnea. Chest 1993, 103, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Kushida, C.A.; Chang, A.; Gadkary, C.; Guilleminault, C.; Carrillo, O.; Dement, W.C. Comparison of actigraphic, polysomnographic, and subjective assessment of sleep parameters in sleep-disordered patients. Sleep Med. 2001, 2, 389–396. [Google Scholar] [CrossRef]
- Yavuz-Kodat, E.; Reynaud, E.; Geoffray, M.M.; Limousin, N.; Franco, P.; Bourgin, P.; Schroder, C.M. Validity of Actigraphy Compared to Polysomnography for Sleep Assessment in Children With Autism Spectrum Disorder. Front. Psychiatry 2019, 10, 551. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, J.T.; Sykora, K.; Schneiderman, J.; Naranjo, C.A.; Sellers, E.M. Assessment of alcohol withdrawal: The revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br. J. Addict. 1989, 84, 1353–1357. [Google Scholar] [CrossRef]
- Kraemer, K.L.; Mayo-Smith, M.F.; Calkins, D.R. Independent clinical correlates of severe alcohol withdrawal. Subst. Abuse 2003, 24, 197–209. [Google Scholar] [CrossRef]
- Mayo-Smith, M.F. Pharmacological management of alcohol withdrawal: A meta-analysis and evidence-based practice guideline. JAMA 1997, 278, 144–151. [Google Scholar] [CrossRef]
- Saitz, R.; Mayo-Smith, M.F.; Roberts, M.S.; Redmond, H.A.; Bernard, D.R.; Calkins, D.R. Individualized treatment for alcohol withdrawal: A randomized double-blind controlled trial. JAMA 1994, 272, 519–523. [Google Scholar] [CrossRef]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition; SCID-I/P: New York, NY, USA, 2002. [Google Scholar]
- Sobell, L.; Sobell, M. Timeline follow-back: A technique for assessing self-reported alcohol consumption. In Measuring Acohol Consumption: Psychosocial and Biochemical Methods; Humana Press: Totowa, NJ, USA, 1992; pp. 41–72. [Google Scholar]
- Sobell, L.C.; Sobell, M.B. Timeline Followback: User’s Guide; Addiction Research Foundation= Fondation de la recherche sur la toxicomanie: Toronto, ON, Canada, 1996. [Google Scholar]
- Åsberg, M.; Montgomery, S.A.; Perris, C.; Schalling, D.; Sedvall, G. A COMPREHENSIVE PSYCHOPATHOLOGICAL RATING SCALE. Acta Psychiatr. Scand. 1978, 57, 5–27. [Google Scholar] [CrossRef]
- Tyrer, P.; Owen, R.T.; Cicchetti, D.V. The brief scale for anxiety: A subdivision of the comprehensive psychopathological rating scale. J. Neurol. Neurosurg. Psychiatry 1984, 47, 970–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, S.A.; Åsberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Flannery, B.A.; Volpicelli, J.R.; Pettinati, H.M. Psychometric properties of the Penn Alcohol Craving Scale. Alcohol Clin. Exp. Res. 1999, 23, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Peter, L.; Reindl, R.; Zauter, S.; Hillemacher, T.; Richter, K. Effectiveness of an Online CBT-I Intervention and a Face-to-Face Treatment for Shift Work Sleep Disorder: A Comparison of Sleep Diary Data. Int. J. Environ. Res. Public Health 2019, 16, 3081. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean (SD) |
|---|---|
| Age | 46.3 (9.3) |
| Number (%) | |
| Gender | |
| Male | 82 (66.1) |
| Female | 42 (33.9) |
| Race | |
| Black or African American | 57 (46.0) |
| White | 56 (45.2) |
| American Indian/Alaska Native | 1 (0.8) |
| Asian | 3 (2.4) |
| More Than One Race | 3 (2.4) |
| Unknown | 4 (3.2) |
| Ethnicity | |
| Non-Hispanic | 119 (96.0) |
| Hispanic | 3 (2.4) |
| Unknown | 2 (1.6) |
| Marital Status | |
| Divorced | 14 (11.3) |
| Unknown | 2 (1.6) |
| Married | 20 (16.1) |
| Separated | 10 (8.1) |
| Single | 76 (61.3) |
| Widowed | 2 (1.6) |
| Anxiety Disorders (SCID IV) ** | |
| Yes | 63 (50.8) |
| Mood Disorders (SCID IV) ** | |
| Yes | 70 (56.5) |
| Max CIWA (Clinical Institute Withdrawal Assessment) Score (Days 1–4) | |
| Mean (SD) | 7.73 (5.62) |
| PSQI (Pittsburgh Sleep Quality Index) (Total Score) | |
| Baseline (Day 2) | 11.01 (4.41) |
| Pre-Discharge (Day 28) | 6.46 (3.82) |
| Characteristic, Mean (SD) | Week 1 (N = 124) | Week 2 (N = 116) | Week 3 (N = 99) | Total (N = 124) |
|---|---|---|---|---|
| SRI (Sleep Regularity Index) | 75.72 (10.48) | 77.29 (10.20) | 77.76 (10.21) | 76.95 (7.87) |
| PSQI (Pittsburgh Sleep Quality Index) | ||||
| Baseline (day 2) | 11.01 (4.41) | |||
| Before discharge (day 28) | 6.46 (3.82) | |||
| CPRS (Comprehensive Psychopathological Rating Scale) | ||||
| BSA (Brief Scale for Anxiety) | 10.97 (6.85) | 6.39 (5.30) | 5.49 (4.74) | |
| MADRS (Montgomery-Asberg Depression Rating Scale) | 16.14 (9.07) | 7.68 (6.44) | 6.55 (6.10) | |
| ESS (Epworth Sleepiness Scale) | 7.65 (4.32) | 7.26 (4.26) | 6.98 (4.28) | |
| PACS (Penn Alcohol Craving Scale) | 11.53 (7.86) | 8.56 (6.70) | 7.21 (5.83) | |
| Actigraphy Measures | ||||
| Nap Duration | 215.58 (207.0) | 213.75 (207.22) | 243.77 (239.42) | 649.02 (707.61) |
| Sleep Efficiency | 75.68 (11.23) | 74.84 (12.95) | 76.56 (12.35) | 76.01 (10.48) |
| Wake after Sleep Onset | 65.58 (23.99) | 63.30 (24.60) | 62.17 (25.93) | 63.83 (21.35) |
| Sleep Duration | 386.52 (76.48) | 371.84 (74.70) | 379.02 (77.75) | 381.78 (67.82) |
| Sleep Onset Latency | 15.59 (13.35) | 16.44 (16.74) | 15.17 (17.62) | 15.18 (10.57) |
| Average Activity | 262.68 (93.93) | 179.75 (93.49) | 276.11 (92.40) | 272.96 (81.97) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brooks, A.T.; Raju, S.; Barb, J.J.; Kazmi, N.; Chakravorty, S.; Krumlauf, M.; Wallen, G.R. Sleep Regularity Index in Patients with Alcohol Dependence: Daytime Napping and Mood Disorders as Correlates of Interest. Int. J. Environ. Res. Public Health 2020, 17, 331. https://doi.org/10.3390/ijerph17010331
Brooks AT, Raju S, Barb JJ, Kazmi N, Chakravorty S, Krumlauf M, Wallen GR. Sleep Regularity Index in Patients with Alcohol Dependence: Daytime Napping and Mood Disorders as Correlates of Interest. International Journal of Environmental Research and Public Health. 2020; 17(1):331. https://doi.org/10.3390/ijerph17010331
Chicago/Turabian StyleBrooks, Alyssa T., Shravya Raju, Jennifer J. Barb, Narjis Kazmi, Subhajit Chakravorty, Michael Krumlauf, and Gwenyth R. Wallen. 2020. "Sleep Regularity Index in Patients with Alcohol Dependence: Daytime Napping and Mood Disorders as Correlates of Interest" International Journal of Environmental Research and Public Health 17, no. 1: 331. https://doi.org/10.3390/ijerph17010331