Analysis of the Relation between Periodontitis and Chronic Gastritis/Peptic Ulcer: A Cross-Sectional Study Using KoGES HEXA Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
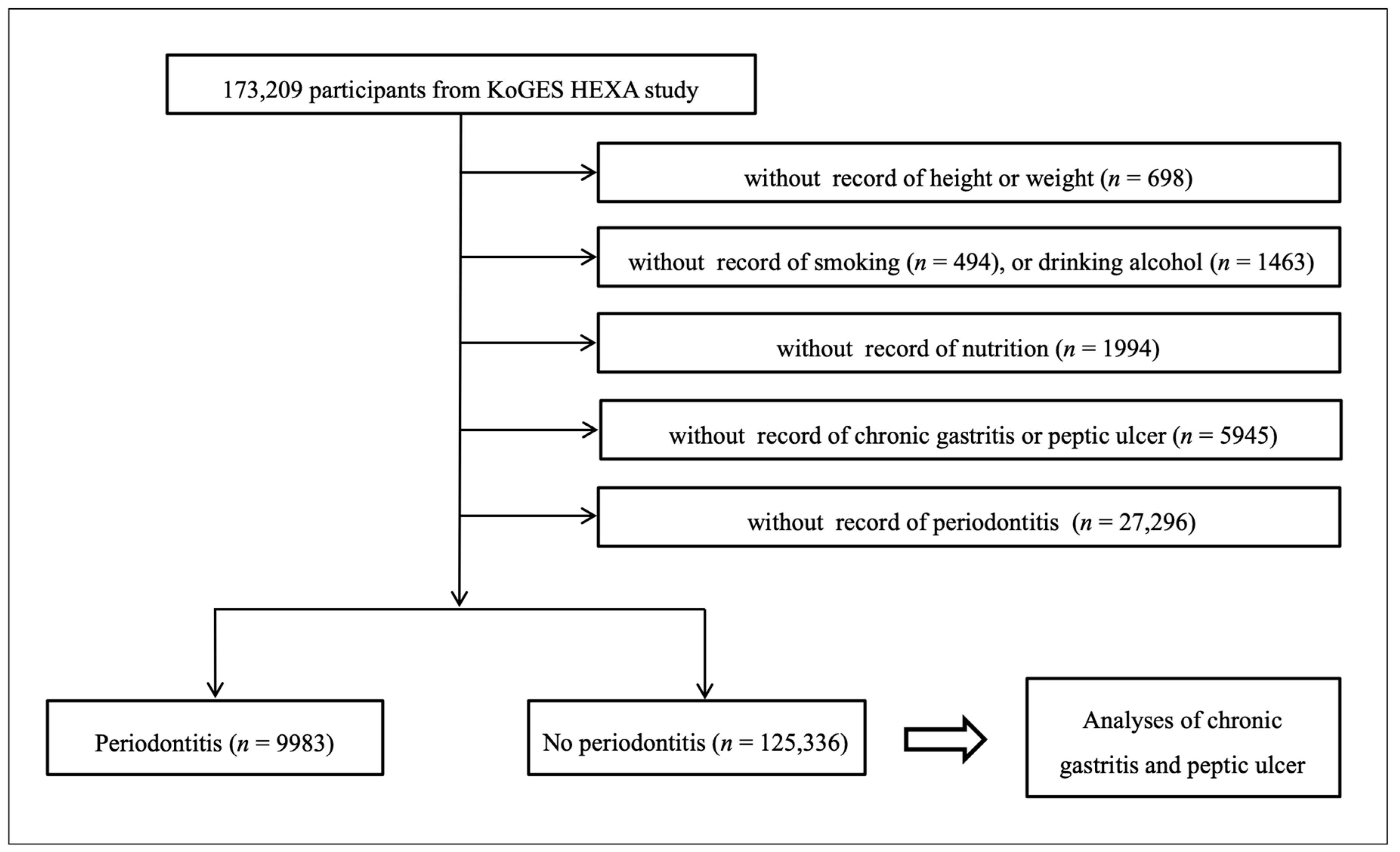
2.2. Participant Selection
2.3. Survey
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Narayanan, M.; Reddy, K.M.; Marsicano, E. Peptic Ulcer Disease and Helicobacter pylori infection. Mo. Med. 2018, 115, 219–224. [Google Scholar] [PubMed]
- Lanas, A.; Chan, F.K.L. Peptic ulcer disease. Lancet 2017, 390, 613–624. [Google Scholar] [CrossRef]
- Lanas, A.; Garcia-Rodriguez, L.A.; Polo-Tomas, M.; Ponce, M.; Quintero, E.; Perez-Aisa, M.A.; Gisbert, J.P.; Bujanda, L.; Castro, M.; Munoz, M.; et al. The changing face of hospitalisation due to gastrointestinal bleeding and perforation. Aliment. Pharmacol. Ther. 2011, 33, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnenberg, A. Review article: Historic changes of Helicobacter pylori-associated diseases. Aliment. Pharmacol. Ther. 2013, 38, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Malmi, H.; Kautiainen, H.; Virta, L.J.; Farkkila, N.; Koskenpato, J.; Farkkila, M.A. Incidence and complications of peptic ulcer disease requiring hospitalisation have markedly decreased in Finland. Aliment. Pharmacol. Ther. 2014, 39, 496–506. [Google Scholar] [CrossRef] [Green Version]
- Lanas, A. We Are Using Too Many PPIs, and We Need to Stop: A European Perspective. Am. J. Gastroenterol. 2016, 111, 1085–1086. [Google Scholar] [CrossRef]
- Siddique, O.; Ovalle, A.; Siddique, A.S.; Moss, S.F. Helicobacter pylori Infection: An Update for the Internist in the Age of Increasing Global Antibiotic Resistance. Am. J. Med. 2018, 131, 473–479. [Google Scholar] [CrossRef]
- Meyer-Rosberg, K.; Scott, D.R.; Rex, D.; Melchers, K.; Sachs, G. The effect of environmental pH on the proton motive force of Helicobacter pylori. Gastroenterology 1996, 111, 886–900. [Google Scholar] [CrossRef]
- Zaki, M.; Coudron, P.E.; McCuen, R.W.; Harrington, L.; Chu, S.; Schubert, M.L. H. pylori acutely inhibits gastric secretion by activating CGRP sensory neurons coupled to stimulation of somatostatin and inhibition of histamine secretion. Am. J. Physiol. Gastrointest. Liver Physiol. 2013, 304, G715–G722. [Google Scholar] [CrossRef]
- El-Omar, E.M.; Oien, K.; El-Nujumi, A.; Gillen, D.; Wirz, A.; Dahill, S.; Williams, C.; Ardill, J.E.; McColl, K.E. Helicobacter pylori infection and chronic gastric acid hyposecretion. Gastroenterology 1997, 113, 15–24. [Google Scholar] [CrossRef]
- Moss, S.F.; Legon, S.; Bishop, A.E.; Polak, J.M.; Calam, J. Effect of Helicobacter pylori on gastric somatostatin in duodenal ulcer disease. Lancet 1992, 340, 930–932. [Google Scholar] [CrossRef]
- McColl, K.E. Helicobacter pylori-negative nonsteroidal anti-inflammatory drug-negative ulcer. Gastroenterol. Clin. North. Am. 2009, 38, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabe, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; Collaborators, G.B.D.O.H. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990-2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Demmer, R.T.; Papapanou, P.N. Epidemiologic patterns of chronic and aggressive periodontitis. Periodontol. 2000 2010, 53, 28–44. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.H.; Hwang, H.J.; Kim, S.H.; Kim, T.H. Associations Between Periodontitis and Chronic Obstructive Pulmonary Disease: The 2010 to 2012 Korean National Health and Nutrition Examination Survey. J. Periodontol. 2016, 87, 864–871. [Google Scholar] [CrossRef]
- Konig, J.; Holtfreter, B.; Kocher, T. Periodontal health in Europe: Future trends based on treatment needs and the provision of periodontal services--position paper 1. Eur J. Dent. Educ. 2010, 14 Suppl. 1, 4–24. [Google Scholar] [CrossRef]
- Dye, B.A.; Tan, S.; Smith, V.; Lewis, B.G.; Barker, L.K.; Thornton-Evans, G.; Eke, P.I.; Beltran-Aguilar, E.D.; Horowitz, A.M.; Li, C.H. Trends in oral health status: United States, 1988–1994 and 1999–2004. Vital Health Stat. 11 2007, 1–92. [Google Scholar]
- Joshipura, K.J.; Wand, H.C.; Merchant, A.T.; Rimm, E.B. Periodontal disease and biomarkers related to cardiovascular disease. J. Dent. Res. 2004, 83, 151–155. [Google Scholar] [CrossRef]
- Singh, M.; Bains, V.K.; Jhingran, R.; Srivastava, R.; Madan, R.; Maurya, S.C.; Rizvi, I. Prevalence of Periodontal Disease in Type 2 Diabetes Mellitus Patients: A Cross-sectional Study. Contemp. Clin. Dent. 2019, 10, 349–357. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Hodges, J.S.; Michalowicz, B.; Wohlfahrt, J.C.; Garcia, R.I. Promoting oral health care because of its possible effect on systemic disease is premature and may be misleading. J. Am. Dent. Assoc. 2018, 149, 401–403. [Google Scholar] [CrossRef]
- Hajishengallis, G. Immunomicrobial pathogenesis of periodontitis: Keystones, pathobionts, and host response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, S.; Schlitt, A.; Hofmann, B.; Schaller, H.G.; Reichert, S. Periodontal pathogens and their role in cardiovascular outcome. J. Clin. Periodontol. 2020, 47, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umeda, M.; Kobayashi, H.; Takeuchi, Y.; Hayashi, J.; Morotome-Hayashi, Y.; Yano, K.; Aoki, A.; Ohkusa, T.; Ishikawa, I. High prevalence of Helicobacter pylori detected by PCR in the oral cavities of periodontitis patients. J. Periodontol. 2003, 74, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Boylan, M.R.; Khalili, H.; Huang, E.S.; Michaud, D.S.; Izard, J.; Joshipura, K.J.; Chan, A.T. A prospective study of periodontal disease and risk of gastric and duodenal ulcer in male health professionals. Clin. Transl. Gastroenterol. 2014, 5, e49. [Google Scholar] [CrossRef]
- Yu, H.C.; Chen, T.P.; Wei, C.Y.; Chang, Y.C. Association between Peptic Ulcer Disease and Periodontitis: A Nationwide Population-Based Case-Control Study in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 912. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Han, B.G.; Ko, G.E.S.g. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Bouziane, A.; Ahid, S.; Abouqal, R.; Ennibi, O. Effect of periodontal therapy on prevention of gastric Helicobacter pylori recurrence: A systematic review and meta-analysis. J. Clin. Periodontol. 2012, 39, 1166–1173. [Google Scholar] [CrossRef]
- Al Asqah, M.; Al Hamoudi, N.; Anil, S.; Al Jebreen, A.; Al-Hamoudi, W.K. Is the presence of Helicobacter pylori in dental plaque of patients with chronic periodontitis a risk factor for gastric infection? Can. J. Gastroenterol. 2009, 23, 177–179. [Google Scholar] [CrossRef] [Green Version]
- Namiot, D.B.; Leszczynska, K.; Namiot, Z.; Chilewicz, M.; Bucki, R.; Kemona, A. The occurrence of Helicobacter pylori antigens in dental plaque; an association with oral health status and oral hygiene practices. Adv. Med. Sci. 2010, 55, 167–171. [Google Scholar] [CrossRef]
- Gao, J.; Li, Y.; Wang, Q.; Qi, C.; Zhu, S. Correlation between distribution of Helicobacter pylori in oral cavity and chronic stomach conditions. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2011, 31, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.K.; Khan, A.A.; Khan, A.A.; Izhar, M.; Alam, A.; Shah, S.W.; Shafqat, F. Correlation of Helicobacter pylori in dental plaque and gastric mucosa of dyspeptic patients. J. Pak. Med. Assoc. 2002, 52, 196–200. [Google Scholar] [PubMed]
- Zaric, S.; Bojic, B.; Jankovic, L.; Dapcevic, B.; Popovic, B.; Cakic, S.; Milasin, J. Periodontal therapy improves gastric Helicobacter pylori eradication. J. Dent. Res. 2009, 88, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Schenkein, H.A.; Loos, B.G. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J. Periodontol. 2013, 84, S51–S69. [Google Scholar] [CrossRef]
- Loos, B.G.; Craandijk, J.; Hoek, F.J.; Wertheim-van Dillen, P.M.; van der Velden, U. Elevation of systemic markers related to cardiovascular diseases in the peripheral blood of periodontitis patients. J. Periodontol. 2000, 71, 1528–1534. [Google Scholar] [CrossRef]
- Kanaparthy, R.; Kanaparthy, A.; Mahendra, M. C-reactive protein as a marker of periodontal disease. Gen. Dent. 2012, 60, e1–e5. [Google Scholar]
- Ebersole, J.L.; Machen, R.L.; Steffen, M.J.; Willmann, D.E. Systemic acute-phase reactants, C-reactive protein and haptoglobin, in adult periodontitis. Clin. Exp. Immunol. 1997, 107, 347–352. [Google Scholar] [CrossRef]
- Michaud, D.S.; Joshipura, K.; Giovannucci, E.; Fuchs, C.S. A prospective study of periodontal disease and pancreatic cancer in US male health professionals. J. Natl. Cancer. Inst. 2007, 99, 171–175. [Google Scholar] [CrossRef]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Giovannucci, E.; Joshipura, K. Periodontal disease, tooth loss, and cancer risk in male health professionals: A prospective cohort study. Lancet. Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Total Participants | p-Value | |
|---|---|---|---|
| Periodontitis | No Periodontitis | ||
| Age (mean, SD, y) | 54.8 (7.9) | 53.0 (8.3) | <0.001 * |
| Sex (n, %) | <0.001 * | ||
| Men | 3852 (38.6) | 43,410 (34.6) | |
| Women | 6131 (61.4) | 81,926 (65.4) | |
| BMI (mean, SD, kg/m2) | 24.0 (2.9) | 23.9 (2.9) | <0.001 * |
| Income (n, %) | <0.001 * | ||
| Missing, no response | 766 (7.7) | 10,856 (8.7) | |
| Lowest | 3441 (34.5) | 35,593 (28.4) | |
| Middle | 3679 (36.9) | 49,428 (39.4) | |
| Highest | 2097 (21.0) | 29,459 (23.5) | |
| Smoking status (n, %) | <0.001 * | ||
| Nonsmoker | 6697 (67.1) | 91,133 (72.7) | |
| Past smoker | 1796 (18.0) | 18,593 (14.8) | |
| Current smoker | 1490 (14.9) | 15,610 (12.5) | |
| Alcohol consumption (n, %) | <0.001 * | ||
| Non drinker | 4792 (48.0) | 64,045 (51.1) | |
| Past drinker | 479 (4.8) | 4536 (3.6) | |
| Current drinker | 4712 (47.2) | 56,755 (45.3) | |
| Nutritional intake (mean, SD) | |||
| Total calories (kcal/d) | 1760.1 (580.0) | 1749.4 (569.3) | 0.071 |
| Protein (g/d) | 58.9 (26.6) | 59.8 (26.4) | 0.002 * |
| Fat (g/d) | 27.5 (18.5) | 28.3 (18.2) | <0.001 * |
| Carbohydrate (g/d) | 315.0 (95.2) | 309.8 (92.8) | <0.001 * |
| Chronic gastritis | 2062 (20.7) | 12,393 (9.9) | <0.001 * |
| Peptic ulcer | 1262 (12.6) | 7724 (6.2) | <0.001 * |
| Characteristics | Odds Ratios for Periodontitis | ||||||
|---|---|---|---|---|---|---|---|
| Crude † | p-Value | Model 1 † | p-Value | Model 2 ‡ | p-Value | ||
| Total participants (n = 134,855) | |||||||
| Chronic gastritis | 2.37 (2.25–2.50) | <0.001 * | 2.35 (2.23–2.48) | <0.001 * | 2.22 a (2.10–2.34) | <0.001 * | |
| Peptic ulcer | 2.20 (2.07–2.35) | <0.001 * | 2.08 (1.95–2.22) | <0.001 * | 1.86 b (1.74–1.98) | <0.001 * | |
| Characteristics | Odds Ratios for Periodontitis | ||||||
|---|---|---|---|---|---|---|---|
| Crude † | p-Value | Model 1 † | p-Value | Model 2 ‡ | p-Value | ||
| Age < 53 years old, men (n = 21,513) | |||||||
| Chronic gastritis | 2.16 (1.83–2.56) | <0.001 * | 2.10 (1.77–2.48) | <0.001 * | 1.97 a (1.66–2.33) | <0.001 * | |
| Peptic ulcer | 1.92 (1.62–2.28) | <0.001 * | 1.82 (1.54–2.16) | <0.001 * | 1.67 b (1.41–1.99) | <0.001 * | |
| Age < 53 years old, women (n = 45,469) | |||||||
| Chronic gastritis | 2.44 (2.21–2.70) | <0.001 * | 2.35 (2.13–2.61) | <0.001 * | 2.24 a (2.02–2.48) | <0.001 * | |
| Peptic ulcer | 2.34 (1.95–2.56) | <0.001 * | 2.13 (1.85–2.44) | <0.001 * | 1.88 b (1.64–2.16) | <0.001 * | |
| Age ≥ 53 years old, men (n = 25,749) | |||||||
| Chronic gastritis | 2.28 (2.03–2.55) | <0.001 * | 2.29 (2.05–2.57) | <0.001 * | 2.12 a (1.89–2.38) | <0.001 * | |
| Peptic ulcer | 2.17 (1.94–2.44) | <0.001 * | 2.12 (1.89–2.38) | <0.001 * | 1.93 b (1.71–2.17) | <0.001 * | |
| Age ≥ 53 years old, women (n = 42,588) | |||||||
| Chronic gastritis | 2.38 (2.20–2.59) | <0.001 * | 2.40 (2.21–2.60) | <0.001 * | 2.28 a (2.10–2.48) | <0.001 * | |
| Peptic ulcer | 2.09 (1.88–2.33) | <0.001 * | 2.07 (1.86–2.31) | <0.001 * | 1.84 b (1.64–2.05) | <0.001 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, S.H.; Min, C.; Hong, S.J.; Choi, H.G.; Koh, D.H. Analysis of the Relation between Periodontitis and Chronic Gastritis/Peptic Ulcer: A Cross-Sectional Study Using KoGES HEXA Data. Int. J. Environ. Res. Public Health 2020, 17, 4387. https://doi.org/10.3390/ijerph17124387
Byun SH, Min C, Hong SJ, Choi HG, Koh DH. Analysis of the Relation between Periodontitis and Chronic Gastritis/Peptic Ulcer: A Cross-Sectional Study Using KoGES HEXA Data. International Journal of Environmental Research and Public Health. 2020; 17(12):4387. https://doi.org/10.3390/ijerph17124387
Chicago/Turabian StyleByun, Soo Hwan, Chanyang Min, Seok Jin Hong, Hyo Geun Choi, and Dong Hee Koh. 2020. "Analysis of the Relation between Periodontitis and Chronic Gastritis/Peptic Ulcer: A Cross-Sectional Study Using KoGES HEXA Data" International Journal of Environmental Research and Public Health 17, no. 12: 4387. https://doi.org/10.3390/ijerph17124387