Are Respiratory Responses to Cold Air Exercise Different in Females Compared to Males? Implications for Exercise in Cold Air Environments


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Experimental Design
2.2. Cold Air Trials
2.3. Respiratory Function Testing and Questionnaires
2.4. Calculation of Variables and Statistical Analysis
3. Results
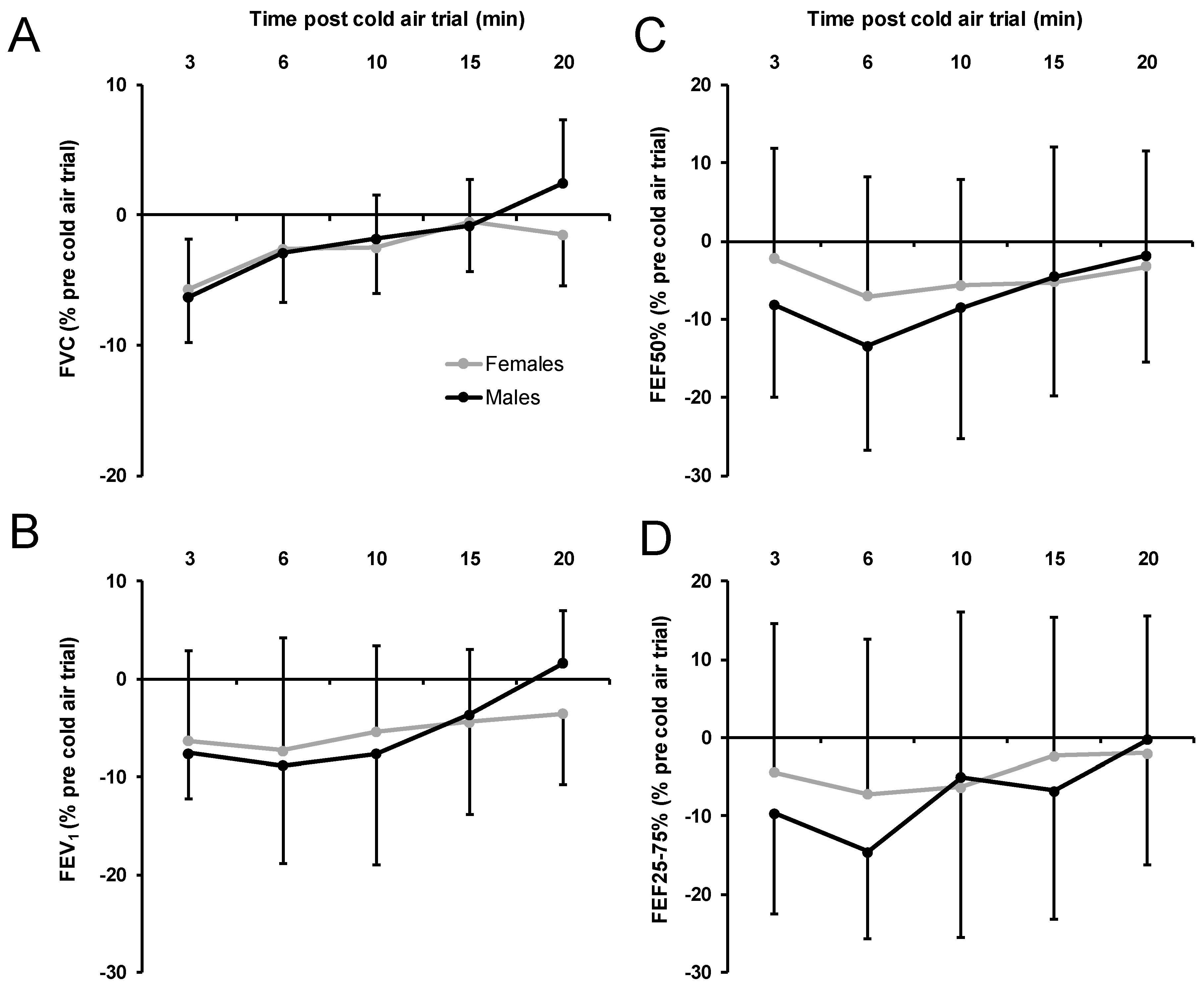
3.1. Spirometry Measures
3.2. Respiratory Symptoms Post-trial
3.3. Exercise Intensity Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rebuck, A.S.; Read, J. Exercise-induced asthma. Lancet 1968, 292, 429–431. [Google Scholar] [CrossRef]
- Crompton, G.K. An unusual example of exercise-induced asthma. Thorax 1968, 23, 165–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiler, J.M.; Anderson, S.D.; Randolph, C.; Bonini, S.; Craig, T.J.; Pearlman, D.S.; Rundell, K.W.; Silvers, W.S.; Storms, W.W.; Bernstein, D.I. Pathogenesis, prevalence, diagnosis, and management of exercise-induced bronchoconstriction: A practice parameter. Ann. Allergy Asthma Immunol. 2010, 105, S1–S47. [Google Scholar] [CrossRef] [PubMed]
- Weiler, J.M.; Brannan, J.D.; Randolph, C.C.; Hallstrand, T.S.; Parsons, J.; Silvers, W.; Storms, W.; Zeiger, J.; Bernstein, D.I.; Blessing-Moore, J.; et al. Exercise-induced bronchoconstriction update—2016. J. Allergy Clin. Immunol. 2016, 138, 1292.e36–1295.e36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitch, K.D.; Sue-Chu, M.; Anderson, S.D.; Boulet, L.-P.; Hancox, R.J.; McKenzie, D.C.; Backer, V.; Rundell, K.W.; Alonso, J.M.; Kippelen, P. Asthma and the elite athlete: Summary of the International Olympic Committee’s consensus conference, Lausanne, Switzerland, January 22–24, 2008. J. Allergy Clin. Immunol. 2008, 122, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Hanks, C.D.; Parsons, J.; Benninger, C.; Kaeding, C.; Best, T.M.; Phillips, G.; Mastronarde, J.G. Etiology of dyspnea in elite and recreational athletes. Phys. Sportsmed. 2012, 40, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Helenius, I.J.; Tikkanen, H.O.; Haahtela, T. Occurrence of exercise induced bronchospasm in elite runners: Dependence on atopy and exposure to cold air and pollen. Br. J. Sports Med. 1998, 32, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Mannix, E.T.; Manfredi, F.; Farber, M.O. A comparison of two challenge tests for identifying exercise-induced bronchospasm in figure skaters. Chest 1999, 115, 649–653. [Google Scholar] [CrossRef] [Green Version]
- Wilber, R.L.; Rundell, K.W.; Szmedra, L.; Jenkinson, D.M.; Im, J.; Drake, S.D. Incidence of exercise-induced bronchospasm in Olympic winter sport athletes. Med. Sci. Sports Exerc. 2000, 32, 732–737. [Google Scholar] [CrossRef]
- Price, O.J.; Hull, J.H.; Ansley, L. Advances in the diagnosis of exercise-induced bronchoconstriction. Expert Rev. Respir. Med. 2014, 8, 209–220. [Google Scholar] [CrossRef]
- Larsson, K.; Tornling, G.; Gavhed, D.; Muller-Suur, C.; Palmberg, L. Inhalation of cold air increases the number of inflammatory cells in the lungs in healthy subjects. Eur. Respir. J. 1998, 12, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Stensrud, T.; Berntsen, S.; Carlsen, K.-H. Exercise capacity and exercise-induced bronchoconstriction (EIB) in a cold environment. Respir. Med. 2007, 101, 1529–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, M.D.; Faulhaber, M. Respiratory function and symptoms post cold air exercise in female high and low ventilation sport athletes. Allergy Asthma Immunol. Res. 2018, 10, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sue-Chu, M. Winter sports athletes: Long-term effects of cold air exposure. Br. J. Sports Med. 2012, 46, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.D.; Steele, A.R.; Parent, E.C.; Steinback, C.D. Cold air exercise screening for exercise induced bronchoconstriction in cold weather athletes. Respir. Physiol. Neurobiol. 2019, 269. [Google Scholar] [CrossRef] [PubMed]
- Sue-Chu, M.; Brannan, J.D.; Anderson, S.D.; Chew, N.; Bjermer, L. Airway hyperresponsiveness to methacholine, adenosine 5-monophosphate, mannitol, eucapnic voluntary hyperpnoea and field exercise challenge in elite cross-country skiers. Br. J. Sports Med. 2010, 44, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Eichner, E.R. Asthma in athletes: Scope, risks, mimics, trends. Curr. Sports Med. Rep. 2008, 7, 118–119. [Google Scholar] [CrossRef] [Green Version]
- Rundell, K.W.; Im, J.; Mayers, L.B.; Wilber, R.L.; Szmedra, L.; Schmitz, H.R. Self-reported symptoms and exercise-induced asthma in the elite athlete. Med. Sci. Sports Exerc. 2001, 33, 208–213. [Google Scholar] [CrossRef]
- Larsson, K.; Ohlsen, P.; Larsson, L.; Malmberg, P.; Rydstrom, P.O.; Ulriksen, H. High prevalence of asthma in cross country skiers. Br. Med. J. 1993, 307, 1326–1329. [Google Scholar] [CrossRef] [Green Version]
- McClaran, S.R.; Harms, C.A.; Pegelow, D.F.; Dempsey, J.A. Smaller lungs in women affect exercise hyperpnea. J. Appl. Physiol. (1985) 1998, 84, 1872–1881. [Google Scholar] [CrossRef]
- Langdeau, J.-B.; Day, A.; Turcotte, H.; Boulet, L.-P. Gender differences in the prevalence of airway hyperresponsiveness and asthma in athletes. Respir. Med. 2009, 103, 401–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rundell, K.W.; Wilber, R.L.; Szmedra, L.; Jenkinson, D.M.; Mayers, L.B.; Im, J. Exercise-induced asthma screening of elite athletes: Field versus laboratory exercise challenge. Med. Sci. Sports Exerc. 2000, 32, 309–316. [Google Scholar] [CrossRef]
- Lennelöv, E.; Irewall, T.; Naumburg, E.; Lindberg, A.; Stenfors, N. The prevalence of asthma and respiratory symptoms among cross-country skiers in early adolescence. Can. Respir. J. 2019, 2019, 1514353. [Google Scholar] [CrossRef] [Green Version]
- Dominelli, P.B.; Molgat-Seon, Y.; Sheel, A.W. Sex differences in the pulmonary system influence the integrative response to exercise. Exerc. Sport Sci. Rev. 2019, 47, 142–150. [Google Scholar] [CrossRef] [PubMed]
- William, S.A.; Dominelli, P.B.; Yannick, M. Revisiting dysanapsis: Sex-based differences in airways and the mechanics of breathing during exercise. Exp. Physiol. 2016, 101, 213–218. [Google Scholar] [CrossRef]
- Nimphius, S. Exercise and sport science failing by design in understanding female athletes. Int. J. Sports Physiol. Perform. 2019, 14, 1157–1158. [Google Scholar] [CrossRef]
- Emmonds, S.; Heyward, O.; Jones, B. The challenge of applying and undertaking research in female sport. Sport. Med. Open 2019, 5, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Society for Exercise Physiology. Physical Activity Training for Health (CSEP-PATH); Canadian Society for Exercise Physiology: Ottawa, ON, Canada, 2013; ISBN 1896900321/9781896900308/1896900305. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Heindl, S.; Struck, J.; Wellhöner, P.; Sayk, F.; Dodt, C. Effect of facial cooling and cold air inhalation on sympathetic nerve activity in men. Respir. Physiol. Neurobiol. 2004, 142, 69–80. [Google Scholar] [CrossRef]
- Carlsen, K.-H.; Engh, G.; Mørk, M. Exercise-induced bronchoconstriction depends on exercise load. Respir. Med. 2000, 94, 750–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van der Grinten, C.P.; Gustafsson, P. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karjalainen, E.-M.; Laitinen, A.; Sue-Chu, M.; Altraja, A.; Bjermer, L.; Laitinen, L.A. Evidence of airway inflammation and remodeling in ski athletes with and without bronchial hyperresponsiveness to methacholine. Am. J. Respir. Crit. Care Med. 2000, 161, 2086–2091. [Google Scholar] [CrossRef] [PubMed]
- Brannan, J.D.; Koskela, H.O.; Anderson, S.D.; Chew, N. Responsiveness to mannitol in asthmatic subjects with exercise- and hyperventilation-induced asthma. Am. J. Respir. Crit. Care Med. 1998, 158, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.D.; Brannan, J.D. Methods for “indirect” challenge tests including exercise, eucapnic voluntary hyperpnea, and hypertonic aerosols. Clin. Rev. Allergy Immunol. 2003, 24, 27–54. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Psychology Press: New York, NY, USA, 1988; ISBN 0805802835/9780805802832. [Google Scholar]
- Stanojevic, S.; Wade, A.; Stocks, J. Reference values for lung function: Past, present and future. Eur. Respir. J. 2010, 36, 12–19. [Google Scholar] [CrossRef]
- Carey, D.G.; Aase, K.A.; Pliego, G.J. The acute effect of cold air exercise in determination of exercise-induced bronchospasm in apparently healthy athletes. J. Strength Cond. Res. 2010, 24, 2172–2178. [Google Scholar] [CrossRef]
- Leuppi, J.D. Bronchoprovocation tests in asthma: Direct versus indirect challenges. Curr. Opin. Pulm. Med. 2014, 20, 31–36. [Google Scholar] [CrossRef]
- Rundell, K.W.; Anderson, S.D.; Spiering, B.A.; Judelson, D.A. Field exercise vs. laboratory eucapnic voluntary hyperventilation to identify airway hyperresponsiveness in elite cold weather athletes. Chest 2004, 125, 909–915. [Google Scholar] [CrossRef]
- McKenzie, D.C.; McLuckie, S.L.; Stirling, D.R. The protective effects of continuous and interval exercise in athletes with exercise-induced asthma. Med. Sci. Sports Exerc. 1994, 26, 951–956. [Google Scholar] [CrossRef]
- Mickleborough, T.D.; Lindley, M.R.; Turner, L.A. Comparative effects of a high-intensity interval warm-up and salbutamol on the bronchoconstrictor response to exercise in asthmatic athletes. Int. J. Sports Med. 2007, 28, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Rundell, K.W.; Spiering, B.A.; Judelson, D.A.; Wilson, M.H. Bronchoconstriction during cross-country skiing: Is there really a refractory period? Med. Sci. Sports Exerc. 2003, 35, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Strauss, R.H.; McFadden, E.R., Jr.; Ingram, R.H., Jr.; Jaeger, J.J.; Stearns, D.R. Enhancement of exercise-induced asthma by cold air. N. Engl. J. Med. 1977, 297, 743–747. [Google Scholar] [CrossRef] [PubMed]
- McFadden, E.R., Jr.; Lenner, K.A.; Strohl, K.P. Postexertional airway rewarming and thermally induced asthma. New insights into pathophysiology and possible pathogenesis. J. Clin. Investig. 1986, 78, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Hartung, G.H.; Myhre, L.G.; Nunneley, S.A. Physiological effects of cold air inhalation during exercise. Aviat. Space Environ. Med. 1980, 51, 591–594. [Google Scholar]
- Quirion, A.; Laurencelle, L.; Paulin, L.; Therminarias, A.; Brisson, G.R.; Audet, A.; Dulac, S.; Vogelaere, P. Metabolic and hormonal responses during exercise at 20°, 0° and −20 °C. Int. J. Biometeorol. 1989, 33, 227–232. [Google Scholar] [CrossRef]
- Aggarwal, A.N. How appropriate is the gold standard for diagnosis of airway obstruction? Lung India 2008, 25, 139–141. [Google Scholar] [CrossRef]
- Turmel, J.; Bougault, V.; Boulet, L.P. Seasonal variations of cough reflex sensitivity in elite athletes training in cold air environment. Cough 2012, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, M.D.D.; Davidson, W.J.J.; Wong, L.E.E.; Traves, S.L.L.; Leigh, R.; Eves, N.D.D. Airway inflammation, cough and athlete quality of life in elite female cross-country skiers: A longitudinal study. Scand. J. Med. Sci. Sports 2015, 26. [Google Scholar] [CrossRef]
- Sue-Chu, M.; Larsson, L.; Bjermer, L. Prevalence of asthma in young cross-country skiers in central Scandinavia: Differences between Norway and Sweden. Respir. Med. 1996, 90, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Boulet, L.-P.; Turmel, J.; Irwin, R.S. Cough in the athlete: CHEST guideline and expert panel report. Chest 2017, 151, 441–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stensrud, T.; Carlsen, K. Can one single test protocol for provoking exercise-induced bronchoconstriction also be used for assessing aerobic capacity? Clin. Respir. J. 2008, 2, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Farley, R.D.; Albazzaz, M.K.; Patel, K.R. Role of cooling and drying in hyperventilation induced asthma. Thorax 1988, 43, 289–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rundell, K.W.; Spiering, B.A.; Baumann, J.M.; Evans, T.M. Effects of montelukast on airway narrowing from eucapnic voluntary hyperventilation and cold air exercise. Br. J. Sports Med. 2005, 39, 232–236. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Yamada, G.; Saikai, T.; Hashimoto, M.; Tanaka, S.; Suzuki, K.; Fujii, M.; Takahashi, H.; Abe, S. Increased airway vascularity in newly diagnosed asthma using a high-magnification bronchovideoscope. Am. J. Respir. Crit. Care Med. 2003, 168, 1495–1499. [Google Scholar] [CrossRef]
- Esteve-Lanao, J.; San Juan, A.F.; Earnest, C.P.; Foster, C.; Lucia, A. How do endurance runners actually train? Relationship with competition performance. Med. Sci. Sports Exerc. 2005, 37, 496–504. [Google Scholar] [CrossRef] [Green Version]
- Parsons, J.P.; Kaeding, C.; Phillips, G.; Jarjoura, D.; Wadley, G.; Mastronarde, J.G. Prevalence of exercise-induced bronchospasm in a cohort of varsity college athletes. Med. Sci. Sports Exerc. 2007, 39, 1487–1492. [Google Scholar] [CrossRef]
- Bonini, M.; Braido, F.; Baiardini, I.; Del Giacco, S.; Gramiccioni, C.; Manara, M.; Tagliapietra, G.; Scardigno, A.; Sargentini, V.; Brozzi, M. AQUA: Allergy questionnaire for athletes. Development and validation. Med. Sci. Sports Exerc. 2009, 41, 1034–1041. [Google Scholar] [CrossRef] [Green Version]
- Helenius, I.J.; Tikkanen, H.O.; Sarna, S.; Haahtela, T. Asthma and increased bronchial responsiveness in elite athletes: Atopy and sport event as risk factors. J. Allergy Clin. Immunol. 1998, 101, 646–652. [Google Scholar] [CrossRef]
- Frischhut, C.; Kennedy, M.D.; Niedermeier, M.; Faulhaber, M. Effects of a heat and moisture exchanger on respiratory function and symptoms post–cold air exercise. Scand. J. Med. Sci. Sports 2020, 30, 591–601. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Female (n = 9) | Male (n = 9) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | (Range) | Mean | SD | (Range) | ||
| Age (year) | 24 | 3 | (20–27) | 24 | 2 | (21–26) | 0.83 |
| Height (cm) | 166 | 6 | (158–172) | 180 | 5 | (177–184) | <0.01 |
| Weight (kg) | 59 | 6 | (51–65) | 75 | 5 | (71–79) | <0.01 |
| BMI (kg/m2 ) | 21 | 1 | (20–23) | 23 | 2 | (22–25) | <0.01 |
| Maximal oxygen uptake (mL/min/kg) | 49 | 3 | (45–56) | 58 | 7 | (50–70) | <0.01 |
| Maximal heart rate (bpm) | 196 | 7 | (180–203) | 200 | 7 | (190–210) | 0.19 |
| Maximal rating of perceived exertion | 19.2 | 0.4 | (19–20) | 19.1 | 0.3 | (19–20) | 0.73 |
| Maximal speed (km/h) | 11.0 | 1.0 | (10–12) | 13.5 | 1.0 | (12–16) | <0.01 |
| Baseline FEV1 (L) | 4.1 | 1.0 | (3.4–5.3) | 6.0 | 0.5 | (5.5–7.1) | <0.01 |
| FEV1 (% predicted) | 121.2 | 18.1 | (93.5–151.2) | 128.9 | 12.4 | (115.0–148.4) | 0.75 |
| Baseline FVC (L) | 5.3 | 1.1 | (4.3–7.2) | 7.2 | 0.8 | (5.6–8.3) | <0.01 |
| FVC (% predicted) | 129.8 | 25.8 | (86.5–169.3) | 126.7 | 13.3 | (100.3–142.2) | 0.31 |
| FEV1/FVC ratio | 0.8 | 0.1 | (0.6–0.9) | 0.8 | 0.1 | (0.7 – 1.0) | 0.32 |
| FEV1/FVC ratio (% predicted) | 95.5 | 14.1 | (68.5–113.0) | 101.6 | 10.1 | (92.2–125.6) | 0.31 |
| Baseline FEF50 (L/min) | 4.7 | 1.0 | (3.3–6.31) | 7.1 | 1.0 | (5.6–8.7) | <0.01 |
| Baseline FEF25–75 (L/min) | 4.0 | 1.1 | (2.7–6.0) | 6.2 | 1.2 | (5.0–8.3) | <0.01 |
| Baseline FEF25–75 (% predicted) | 112.0 | 26.0 | (78.7–158.7) | 128.9 | 25.8 | (103.0–173.7) | 0.18 |
| Temperature | Variable | Female (n = 9) | Male (n = 9) | p-Value | Effect Size |
|---|---|---|---|---|---|
| 0 °C | Number of symptoms (M ± SD) (range) | 1.2 ± 0.7 (0–2) | 1.1 ± 1.2 (0–3) | 0.796 | 0.10 a |
| Cough (%) | 11 | 44 | 0.110 | 0.16 b | |
| Wheeze (%) | 0 | 0 | <1.000 | n.a. c | |
| Chest tightness (%) | 33 | 33 | <1.000 | 1.00 b | |
| Mucus (%) | 78 | 33 | 0.058 | 7.00 b | |
| −20 °C | Number of symptoms (M ± SD) (range) | 2.3 ± 1.0 (1–4) | 2.4 ± 0.5 (2–3) | 0.796 | −0.13 a |
| Cough (%) | 78 | 89 | 0.527 | 0.00 b | |
| Wheeze (%) | 11 | 0 | 0.303 | n.a. c | |
| Chest tightness (%) | 78 | 78 | <1.000 | 1.00 b | |
| Mucus (%) | 67 | 78 | 0.599 | 0.57 b |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kennedy, M.D.; Lenz, E.; Niedermeier, M.; Faulhaber, M. Are Respiratory Responses to Cold Air Exercise Different in Females Compared to Males? Implications for Exercise in Cold Air Environments. Int. J. Environ. Res. Public Health 2020, 17, 6662. https://doi.org/10.3390/ijerph17186662
Kennedy MD, Lenz E, Niedermeier M, Faulhaber M. Are Respiratory Responses to Cold Air Exercise Different in Females Compared to Males? Implications for Exercise in Cold Air Environments. International Journal of Environmental Research and Public Health. 2020; 17(18):6662. https://doi.org/10.3390/ijerph17186662
Chicago/Turabian StyleKennedy, Michael D., Elisabeth Lenz, Martin Niedermeier, and Martin Faulhaber. 2020. "Are Respiratory Responses to Cold Air Exercise Different in Females Compared to Males? Implications for Exercise in Cold Air Environments" International Journal of Environmental Research and Public Health 17, no. 18: 6662. https://doi.org/10.3390/ijerph17186662