4.1. Perceptions
Our results showed that adults of childbearing age in Ille-et-Vilaine were poorly informed about indoor environmental pollution. Twenty-nine percent of the study participants had never heard of it, whereas 10% had never heard of it in the French 2007 health barometer among the 6007 French people questioned [
41]. However, these two studies had several differences: the age of the population studied (18 to 75 years for health barometer versus 18 to 45 years for ours), study location (throughout France for health barometer versus one French department in ours), and modality of interview (by telephone for health barometer versus hand-delivered self-administered questionnaire in ours). This may have resulted in differences in selection (inclusion by telephone was confronted with many refusals to participate, potentially from people who were perhaps uninformed and refused to answer out of disinterest) and differences in classification due to differences in the study modalities and age of participants (older participants are more likely to have heard about indoor pollution) possibly explain this discrepancy between the two studies. Twenty-six percent of respondents “strongly agreed” with the statement “chemicals are so ubiquitous that they cannot be avoided”. These results are similar to those of Barett et al. [
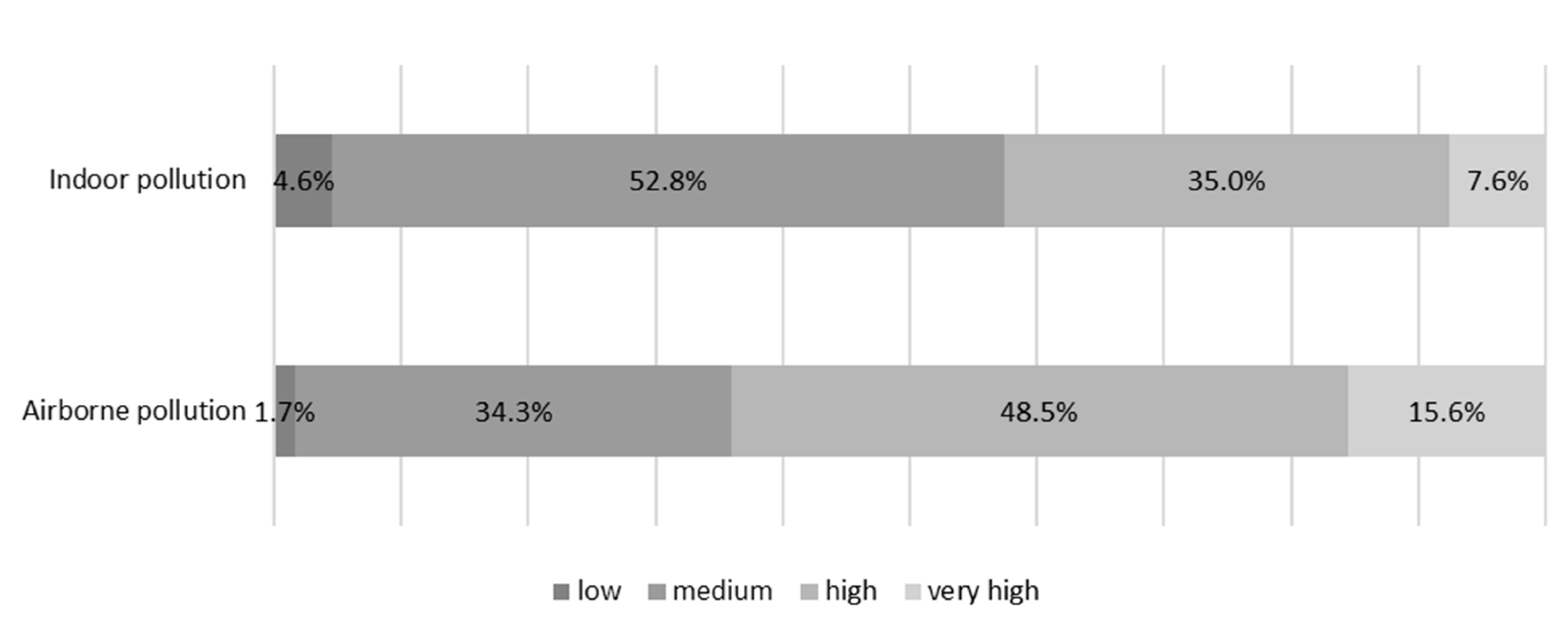
36], who found that 25% of a cohort of pregnant women (mean age 31.3 years) who volunteered to participate and were interviewed by self-questionnaire strongly agreed with this statement. Once again, the results are difficult to compare due to study differences. Forty-two percent of respondents considered the risk due to indoor environmental pollution to the French to be “high” or “very high” versus 48.2% in the 2007 health barometer survey [
41]. The question was slightly different, as it concerned “Indoor air pollution in buildings: homes, schools, offices” and not just the home and only indoor air and not the entire indoor environment. The perceived health risk of the participants was higher for outdoor pollution than indoor environmental pollution. This was also observed in the barometer study, with 84.4% of respondents perceiving a high or very high risk due to outdoor air pollution for the French versus 64.1% in our study [
41]. Indeed, the impact of outdoor pollution on health is known and is classified as carcinogenic by the IARC (International Agency for Research on Cancer) [
42]. This result is therefore logical.
As in other studies, higher age [
28,
36,
41] and education level [
29,
36,
41] were associated with being better informed and having a better perception of the risks concerning indoor environmental pollutants.
4.2. Knowledge
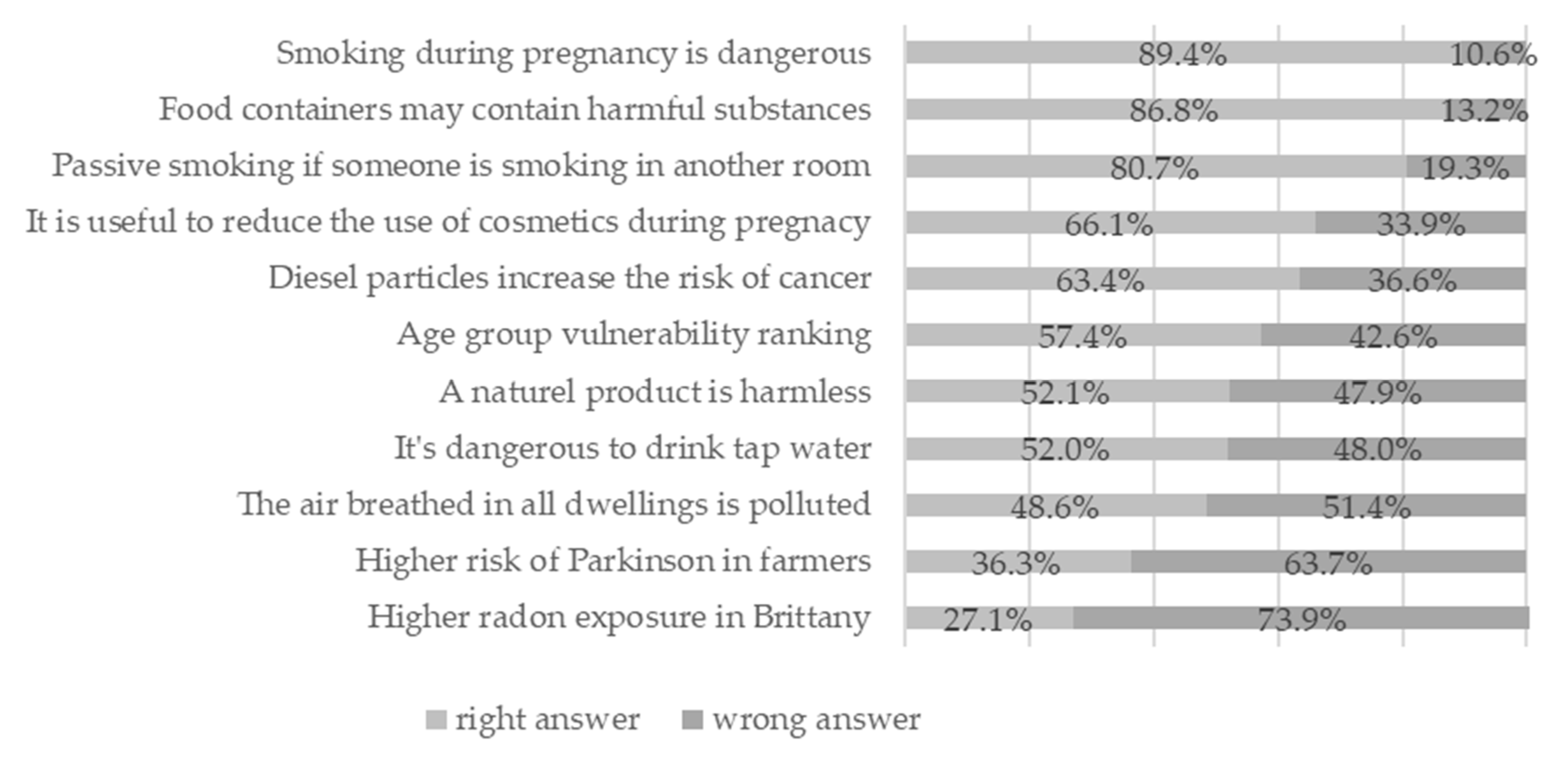
The proportion of correct answers varied greatly depending on the question, showing there to be areas of environmental risk that are still largely unknown to the general public. More than 80% of respondents correctly answered three questions (smoking during pregnancy is dangerous, food containers may contain harmful substances, passive smoking if someone is smoking in another room) and less than 50% correctly answered three questions (the air breathed in all dwellings is polluted, higher risk of Parkinson in farmers, higher radon exposure in Brittany). As already observed for perceptions, the public underestimated indoor air pollution. Although Parkinson’s disease appeared to be known by the public, its recognition as an occupational disease following exposure to pesticides was largely unknown, no doubt because this change is recent and concerns few professionals (2012) [
43]. The fact that radon is a localized natural hazard and that current legislation does not require measuring radon levels for each dwelling may explain the lack of knowledge of this type of exposure [
44]. The mean knowledge score was not very high, as it was 6.6 out of 11. There have not been many studies on this subject. Rouillon et al. [
27] also observed a low score in 2017. They evaluated knowledge about endocrine disruptors in a population of 300 pregnant women with a 100-item questionnaire in an interview. The average knowledge score was 42.9/100. The difference could be explained by the fact that our questionnaire approached the environment in a global manner with simple and general questions, in contrast to the study of Rouillon et al., which dealt in depth with endocrine disruptors. In the 2007 health barometer, 67.2% of the respondents had already heard of the nine topics (excluding radon) and felt well informed about 5/9 topics on average [
41]. This difference could be explained by the fact that the population surveyed was older and the questions asked were simply whether they were an environmental issue.
The level of knowledge was higher for those living as a couple and with a higher educational level. Better knowledge for couples can be explained by the fact that the experience and knowledge of the two individuals is additive. Rouillon also observed that a high level of education was associated with better knowledge of endocrine disruptors [
28]. In the 2007 health barometer [
41], being 18 to 25 years old and having less than a French secondary school diploma were associated with an increased risk of being under-informed.
Better knowledge was associated with higher recognition of environmental chemicals as being potentially dangerous. The study of Rouillon et al. [
28] also observed that a higher average risk perception score was associated with a higher level of knowledge.
4.3. Practices
Our results show certain recommended practices concerning indoor environment pollution were well integrated (by more than 80% of respondents). They were, in decreasing order: annual chimney and stove sweeping, maintenance of the temperature in the dwelling between 18 and 22 degrees, aeration of the dwelling during renovation, banning smoking inside the home, no-use of incense, and daily ventilation of the dwelling for more than 10 min in summer. Other practices were moderately implemented (by 60% to 80% of participants) and were, in decreasing order: prohibiting children from entering the room being renovated, not mixing cleaning products, ventilation of the renovated room several weeks after the work is completed, the ventilation of the entire dwelling during renovation work, not using scented candles, keeping pregnant women out of the room during works, and checking of the heating system. Finally, certain recommended practices were not well followed (by less than 60% of participants). They were, in decreasing order: washing textiles before first use, examining the composition of work and decoration products, annual cleaning of CMV systems, not using air fresheners, removing dust with a damp cloth, daily ventilation of the dwelling for more than 10 min in winter, paying attention to the composition of do-it-yourself products (38.3%), putting on a mask during renovation work, paying attention to the composition of cosmetic products, using homemade or eco-labeled detergent, airing the textile before the first use if it is not washed, paying attention to the precautions for use and danger pictograms for cleaning products, ventilating more often after buying new furniture to limit the accumulation of volatile organic compounds that escape from it, and using an application to choose hygiene products.
To date, studies to compare our results are rare. Daily ventilation was carried out in winter by 84.1% of the people questioned in the 2007 health barometer (compared to 40.0% in our study) [
41]. Furthermore, 64.0% of people had not had their ventilation system checked in the last 12 months (compared to 53.1% in our study) [
41]. This difference may be explained by the different methodologies used (general population versus primary care population, interviewed by telephone versus self-questionnaire, 18–75 years old versus 18–45). It is also important to pay attention to the composition of cosmetic products to reduce exposure to chemical substances that can have an adverse effect on fertility and embryogenesis. However, in the study of Cecile and al. [
31], even though 54.8% of women believed there to be a risk in using cosmetics during pregnancy, very few changed their habits, except for nail polish and nail polish remover. In addition, in the regional survey “Indoor environmental health, behaviors and risks of exposure to indoor pollutants” conducted in Aquitaine in 2018, only 27.0% of women interviewed after leaving the maternity ward considered the existence of an eco-label as the main purchasing criterion for cosmetics, ahead of the brand and price [
45]. To end, the dangerousness of new furniture due to their composition (agglomerates, glues, treatments, plastics, …) was little known by the population of our study, but also by that of the regional study conducted by the ARS of Aquitaine [
45] since 35% of women interviewed considered that the composition of furniture had no real or no consequences on health against 7% for the paint.
The associations observed differed depending on the level of integration of a practice. Well-integrated practices were preferentially associated with socio-demographic characteristics (age, being in a couple, and having children). Only one (temperature in dwelling) was associated with knowledge. The under-integrated practices fell into two groups. On one hand, ventilation in winter, annual cleaning of CMV systems, and examining do-it yourself product composition showed no association for the first, and unexpected ones for the other two: cleaning CMV systems was more frequent when the level of education and knowledge were lower, and examining do-it yourself product composition was more frequent for younger participants. On the other hand, paying attention to the composition of cosmetic products or the use of an application, choice of detergents, precautionary use of cleaning products, and ventilation after the purchase of new furniture were mostly associated with knowledge and perceptions and the unique associated socio-demographic factor was the level of education.
4.5. Indoor Environment and Sex
To date, most studies on this subject have focused on women. According to our findings, being a woman was associated with a higher likelihood of having already heard of indoor environmental pollution. More women also fully agreed with the ubiquity of chemicals in the environment than men. These findings are in accordance with those in the literature, which show that gender is a dominant factor; women tend to express higher levels of concern about the environment than men [
47]. The French barometer study [
41] interviewed men and noted that women were significantly more likely than men to perceive environmental health risks as “high” or “very high”.
We did not observe any significant difference in knowledge between the sexes. We also did not observe any significant gender difference in practices, except for the number of cosmetics applied (more for women than men). There are no studies on the level of knowledge or practices among men with which to compare our results.
It would be worthwhile to inform men in the same way as women during a consultation or as a joint information campaign for couples.
4.6. Source of Information
The media (TV, Internet or other techniques of distribution of information) was very widely cited by respondents as the source of received information, whereas health professionals were only very rarely mentioned. This was shown by the study of Chabert et al. [
29], which showed that better informed women were more likely to obtain the information themselves (Internet, media) and that of Teysseire et al. [
30], in which 82.6% of pregnant women had received information via the Internet and 57% via television, whereas health practitioners were less frequently mentioned. However, in the aforementioned study [
30], approximately one third of the women cited a health professional as one of their main sources of information, whereas they were cited by only 3% of our respondents. This can be explained by the fact that pregnancy is a period with close medical and para-medical follow-up, whereas our study surveyed all adults of childbearing age, men and women. In addition, our question was open-ended, asking for sources to be cited, whereas in other studies, the various sources of information were suggested, which increases the frequency with which they are mentioned.
Although few of our respondents had been informed by a health professional and many had been informed through the Internet, television, or the media, the distribution of responses concerning the desired source of information was more moderate: the media were highly represented (49.7%) but so were health professionals (39.0%). The importance of the media in our society no longer needs to be demonstrated, but this suggests that health professionals also have a role to play in providing information about environmental risks. Marie et al. [
31] showed that only a minority of health professionals asked women during pregnancy about their exposure to chemicals and advised them to reduce exposure. There is thus room for improvement, especially as more than 65.0% of the women interviewed by Marie et al. [
31] wished to be better informed by health professionals about the risks of using cosmetics, whether outside or during pregnancy. On this point, Rouillon et al. [
28] have suggested that healthcare providers counsel pregnant women on exposure to environmental chemicals, while being careful not to increase their anxiety by advising them and taking into account their knowledge, perceptions, and possibilities for action.
Of note, brochures were the most represented (58.7%) source of information, but again, this question was closed, whereas that concerning the media and health professionals was open and they had to be specified.
4.7. Strengths and Limitations
Our study had several strengths. The size of our sample was large (554), allowing more precise measurements. The method of recruitment by stratified random draw limited selection bias and allowed inclusion from different urban zones. The presence of the interviewers in the waiting room allowed good individual participant rates and correct completion of the questionnaires despite its length, since only seven questionnaires were excluded due to missing data. The questionnaire included questions drawn from previous studies and pre-existing official health recommendations. In addition, the questions concerning knowledge were defined by an expert group using a validated methodology.
Our study also had several limitations. The RPPS database is not completely up to date, as the GPs selected could have retired, are replacement doctors, or have a practice other than a general practice in a private practice. In addition, the participation rate of eligible GPs was approximately 50%, which may have introduced a selection bias if the GP’s participation is note random. Inclusions in stratum 3 were quite low. However, weighting allowed rebalancing between strata. In addition, three different investigators carried out the collection and could have influenced the recruitment due to their different personalities. However, the arguments were harmonized beforehand to eliminate such bias. The knowledge part of the questionnaire, created for this study using a validated method, was not validated, which may induce a lack of precision in the case of poor reliability or measurement bias in the case of poor validity. Finally, not all sources of domestic environmental pollutants were investigated including pesticides (which were, however, investigated through the “Pesti-Home” study) and food and water, as these are other routes of exposure.




{kind=link}
{kind=link}