Social Capital and Mental Health among Older Adults Living in Urban China in the Context of COVID-19 Pandemic


Abstract
1. Introduction
1.1. The Theoretical Framework of Social Capital
1.2. Cognitive Social Capital, Structural Social Capital, and Mental Health
2. Materials and Methods
2.1. Sampling
2.2. Measurements
2.2.1. Outcome Variable
2.2.2. Social Capital Variable
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
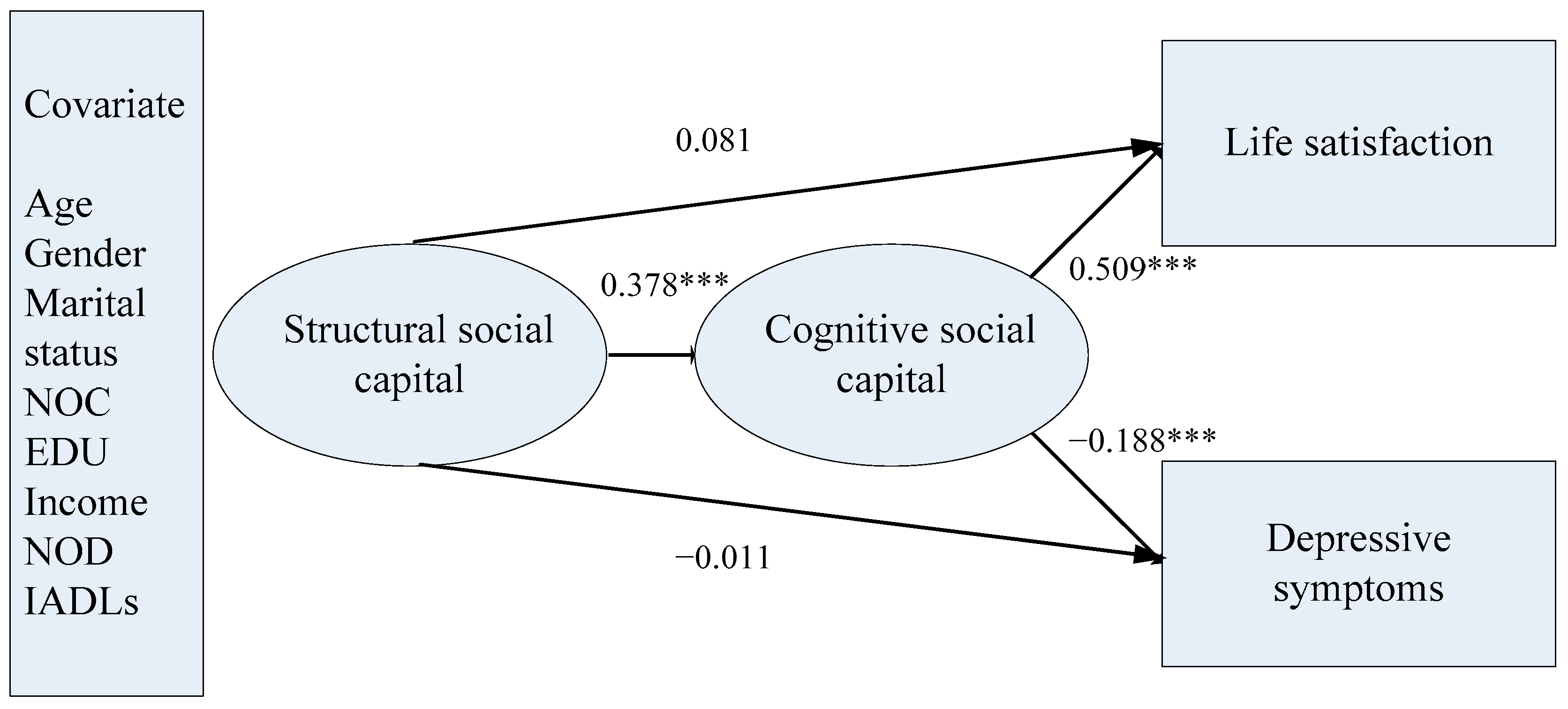
3.2. Structural Equation Modeling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wu, B. Social isolation and loneliness among older adults in the context of COVID-19: A global challenge. Glob. Health Res. Policy 2020, 5, 27. [Google Scholar] [CrossRef] [PubMed]
- Marroquín, B.; Vine, V.; Morgan, R. Mental health during the COVID-19 pandemic: Effects of stay-at-home policies, social distancing behavior, and social resources. Psychiatry Res. 2020, 293, 113419. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Rodela, T.T.; Sultana, A.; McKyer, E.L.J.; Bhattacharya, S.; Hossain, M. Social Capital and Mental Health during the COVID-19 Pandemic. Available online: osf.io/preprints/socarxiv/zrkgh (accessed on 15 October 2020).
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (accessed on 15 October 2020).
- Bian, Y.; Miao, X.; Lu, X.; Ma, X.; Guo, X. The Emergence of a COVID-19 Related Social Capital: The Case of China. Int. J. Sociol. 2020, 50, 419–433. [Google Scholar] [CrossRef]
- Kim, D.; Baum, C.F.; Ganz, M.; Subramanian, S.; Kawachi, I. The contextual effects of social capital on health: A cross-national instrumental variable analysis. Soc. Sci. Med. 2011, 30, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nyqvist, F.; Forsman, A.K.; Giuntoli, G.; Cattan, M. Social capital as a resource for mental well-being in older people: A systematic review. Aging Ment. Health 2012, 17, 394–410. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef]
- Lou, V.W.Q. Spiritual Well-Being of Chinese Older Adults Conceptualization, Measurement and Intervention; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Kim, H.J.; Hong, S.; Kim, M. Living arrangement, social connectedness, and life satisfaction among Korean older adults with physical disabilities: The results from the national survey on persons with disabilities. J. Dev. Phys. Disabil. 2015, 27, 307–321. [Google Scholar] [CrossRef]
- Li, C.; Chi, I.; Zhang, X.; Cheng, Z.; Zhang, L.; Chen, G. Urban and rural factors associated with life satisfaction among older Chinese adults. Aging Ment. Health 2015, 19, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chi, I.; Xu, L. Life satisfaction of older Chinese adults living in rural communities. J. Cross-Cult. Gerontol. 2013, 28, 153–165. [Google Scholar] [CrossRef]
- Ng, S.T.; Tey, N.P.; Asadullah, M.N. What matters for life satisfaction among the oldest-old? Evidence from China. PLoS ONE 2017, 12, e0171799. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Spencer, M.; Sun, Q.; Lou, V.W.Q. Family social capital and life satisfaction among older adults living alone in urban China: The moderating role of functional health. Aging Ment. Health 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Xu, L.; Lou, V.W.Q.; Chi, I. Intergenerational relationships and the trajectory of depressive symptoms among older Chinese adults in rural migrant families. Aging Ment. Health 2018, 22, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Bassett, E.; Moore, S. Social capital and depressive symptoms: The association of psychosocial and network dimensions of social capital with depressive symptoms in Montreal, Canada. Soc. Sci. Med. 2013, 86, 96–102. [Google Scholar] [CrossRef]
- Cao, W.; Li, L.; Zhou, X.; Zhou, C. Social capital and depression: Evidence from urban elderly in China. Aging Ment. Health 2015, 19, 418–429. [Google Scholar] [CrossRef]
- Schwarzbach, M.; Luppa, M.; Forstmeier, S.; Konig, H.; Riedelheller, S.G. Social relations and depression in late life-A systematic review. Int. J. Geriatr. Psychiatry 2014, 29, 1–21. [Google Scholar] [CrossRef]
- Lu, N.; Jiang, N.; Lou, V.W.Q.; Zeng, Y.; Liu, M. Does gender moderate the relationship between social capital and life satisfaction? Evidence from urban China. Res. Aging 2018. [Google Scholar] [CrossRef]
- Lu, N.; Lum, T.Y.S.; Lou, V.W.Q. The impacts of community social capital on the life satisfaction of older adults in Hong Kong: The moderator role of intergenerational family capital. Aging Ment. Health 2016, 20, 1213–1220. [Google Scholar] [CrossRef]
- Lu, N.; Peng, C. Community-based structural social capital and depressive symptoms of older urban Chinese adults: The mediating role of cognitive social capital. Arch. Gerontol. Geriatr. 2019, 82, 74–80. [Google Scholar] [CrossRef]
- Zhang, J.Y.; Lu, N. Community-based cognitive social capital and depressive symptoms among older adults in urban China: The moderating role of family social capital. Int. J. Aging Hum. Dev. 2019. [Google Scholar] [CrossRef]
- Bartscher, A.K.; Seitz, S.; Sieglich, S.; Slotwinski, M.; Wehrhöfer, N.; Siegloch, S. Social Capital and the Spread of Covid-19: Insights from European Countries. Available online: https://ideas.repec.org/p/ces/ceswps/_8346.html (accessed on 14 October 2020).
- Coleman, J.S. Social capital in the creation of human capital. Am. J. Sociol. 1988, 94, 95–120. [Google Scholar] [CrossRef]
- Bourdieu, P. The Forms of Capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J.G., Ed.; Greenwood Press: New York, NY, USA, 1986. [Google Scholar]
- Putnam, R.D.; Leonardi, R.; Nanetti, R. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1993. [Google Scholar]
- De Silva, M.J.; Huttly, S.R.; Harpham, T.; Kenward, M.G. Social capital and mental health: A comparative analysis of four low income countries. Soc. Sci. Med. 2007, 64, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Lu, N.; Jiang, N.; Lou, V.W.Q. Intention to use respite services among informal care-givers of frail older adults in China: The role of care needs change. Ageing Soc. 2020, 1–20. [Google Scholar] [CrossRef]
- Peng, C.; Burr, J.A.; Kim, K.; Lu, N. Home and community-based service utilization among older adults in urban China:The role of social capital. J. Gerontol. Soc. Work 2020. [Google Scholar] [CrossRef]
- Lu, N.; Jiang, N.; Sun, Q.; Lou, V.W.Q. Community social capital and positive caregiving experiences among adult-children caregivers of older adults with disabilities in urban China. Res. Aging 2019. [Google Scholar] [CrossRef] [PubMed]
- Ehsan, A.; Klaas, H.S.; Bastianen, A.; Spini, D. Social capital and health: A systematic review of systematic reviews. Ssm-Popul. Health 2019, 8, 100425. [Google Scholar] [CrossRef] [PubMed]
- Ajrouch, K. Resources and well-being among Arab-American elders. J. Cross-Cult. Gerontol. 2007, 22, 167–182. [Google Scholar] [CrossRef]
- Theurer, K.; Wister, A. Altruistic behaviour and social capital as predictors of well-being among older Canadians. Ageing Soc. 2010, 30, 157–181. [Google Scholar] [CrossRef]
- Yamaoka, K. Social capital and health and well-being in East Asia: A population-based study. Soc. Sci. Med. 2008, 66, 885–899. [Google Scholar] [CrossRef]
- Chiao, C.; Weng, L.; Botticello, A.L. Social participation reduces depressive symptoms among older adults: An 18-year longitudinal analysis in Taiwan. BMC Public Health 2011, 11, 292. [Google Scholar] [CrossRef]
- Yip, W.; Subramanian, S.V.; Mitchell, A.D.; Lee, D.T.S.; Wang, J.; Kawachi, I. Does social capital enhance health and well-being? Evidence from rural China. Soc. Sci. Med. 2007, 64, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Norstrand, J.A.; Xu, Q. Social capital and health outcomes among older adults in China: The urban–rural dimension. Gerontologist 2011, 52, 325–334. [Google Scholar] [CrossRef] [PubMed]
- De Silva, M.J.; McKenzie, K.; Harpham, T.; Huttly, S. Social capital and mental illness: A systematic review. J. Epidemiol. Community Health 2005, 59, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Brehm, J.; Rahn, W.M. Individual-level evidence for the causes and consequences of social capital. Am. J. Political Sci. 1997, 41, 999–1023. [Google Scholar] [CrossRef]
- Lindstrom, M. Social capital, the miniaturisation of community and self-reported global and psychological health. Soc. Sci. Med. 2004, 59, 595–607. [Google Scholar] [CrossRef]
- Lu, N.; Peng, C.; Jiang, N.; Lou, V.W.Q. Cognitive social capital and formal volunteering among older adults in urban China: Does gender matter? J. Appl. Gerontol. 2018. [Google Scholar] [CrossRef]
- Lu, N.; Zhang, J. Social capital and self-rated health among older adults living in urban China: A mediation model. Sustainability 2019, 11, 5566. [Google Scholar] [CrossRef]
- Pfeiffer, E. A Short Portable Mental Status Questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Lou, V.W.Q.; Chi, I.; Mjelde-Mossey, L.A. Development and validation of a life satisfaction scale for Chinese elders. Int. J. Aging Hum. Dev. 2008, 67, 149–170. [Google Scholar] [CrossRef]
- Rankin, S.H.; Galbraith, M.E. Reliability and validity data for a Chinese translation of the Center for Epidemiological Studies-Depression. Psychol. Rep. 1993, 73, 1291–1298. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Grootaert, C.; Narayan, D.; Jones, V.N.; Woolcock, M. Integrated Questionnaire for the Measurement of Social Capital; World Bank: Washington, DC, USA, 2004. [Google Scholar]
- Agampodi, T.C.; Agampodi, S.B.; Glozier, N.; Siribaddana, S. Measurement of social capital in relation to health in low and middle income countries: A systematic review. Soc. Sci. Med. 2015, 128, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Wu, B.; Jiang, N.; Dong, T. Association between childhood conditions and arthritis among middle-aged and older adults in China: The China Health and Retirement Longitudinal Study. Ageing Soc. 2020, 1–18. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Qin, X.; Wang, S.; Hsieh, C. The prevalence of depression and depressive symptoms among adults in China: Estimation based on a National Household Survey. China Econ. Rev. 2016, 51, 271–282. [Google Scholar] [CrossRef]


{kind=link}
| N (%) | M (SD) | |
|---|---|---|
| Age | 68.37 (6.69) | |
| 60–70 | 329 (69.7) | |
| 71 or older | 142 (30.1) | |
| Gender | ||
| Men | 206 (43.6) | |
| Women | 266 (56.4) | |
| Married | 392(83.1) | |
| Educational attainment | ||
| Secondary school or lower | 199 (42.2) | |
| High school or above | 273 (57.8) | |
| Monthly household income | ||
| 0–9999 RMB | 224 (47.5) | |
| 10,000 RMB or more | 235 (49.8) | |
| Number of children | 1.19 (0.62) | |
| Number of chronic diseases | 1.37 (1.41) | |
| IADL | 0.02 (0.10) | |
| Life satisfaction | 4.27 (0.48) | |
| Depressive symptoms | 3.14 (3.64) |
| Estimate | SD | Standardized Estimate | SD | |
|---|---|---|---|---|
| Cognitive social capital | ||||
| Trust in local community | 1.000 | 0.000 | 0.869 * | 0.040 |
| Perceived helpfulness of others | 0.995 * | 0.095 | 0.897 * | 0.042 |
| Willingness to cooperate with others | 1.021 * | 0.097 | 0.913 * | 0.042 |
| Feelings of belonging | 0.874 * | 0.029 | 0.884 * | 0.042 |
| Structural social capital | ||||
| Organization memberships | 1.000 | 0.000 | 0.586 * | 0.073 |
| Citizenship activities | 1.246 * | 0.297 | 0.625 * | 0.081 |
| Volunteering | 0.662 * | 0.153 | 0.702 * | 0.083 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Q.; Lu, N. Social Capital and Mental Health among Older Adults Living in Urban China in the Context of COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7947. https://doi.org/10.3390/ijerph17217947
Sun Q, Lu N. Social Capital and Mental Health among Older Adults Living in Urban China in the Context of COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(21):7947. https://doi.org/10.3390/ijerph17217947
Chicago/Turabian StyleSun, Qian, and Nan Lu. 2020. "Social Capital and Mental Health among Older Adults Living in Urban China in the Context of COVID-19 Pandemic" International Journal of Environmental Research and Public Health 17, no. 21: 7947. https://doi.org/10.3390/ijerph17217947
APA StyleSun, Q., & Lu, N. (2020). Social Capital and Mental Health among Older Adults Living in Urban China in the Context of COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 17(21), 7947. https://doi.org/10.3390/ijerph17217947