Alcohol Outlet Density and Deprivation in Six Towns in Bergrivier Municipality before and after Legislative Restrictions


Abstract
:1. Introduction
1.1. Fetal Alcohol Syndrome in South Africa
1.2. Alcohol Outlet Density and Alcohol-Related Harms
1.3. South African Policies
1.4. Study Setting
2. Materials and Methods
2.1. Data Collection
2.2. Alcohol Outlet Densities
2.3. Statistical Analyses
2.3.1. T-tests
2.3.2. Spearman Rank Correlation
2.3.3. Hot Spot Analysis and Deprivation
3. Results
3.1. Study 1 and Study 2 Data Changes
3.2. Liquor Act Impact
3.2.1. Total, Illegal, and Legal Alcohol Outlets
3.2.2. Alcohol Outlet Accessibility and Density—Outlets/1000 persons
3.2.3. Alcohol Outlet Accessibility and Density—Outlets/km2 persons
3.3. SAIMD and Alcohol Outlet Density
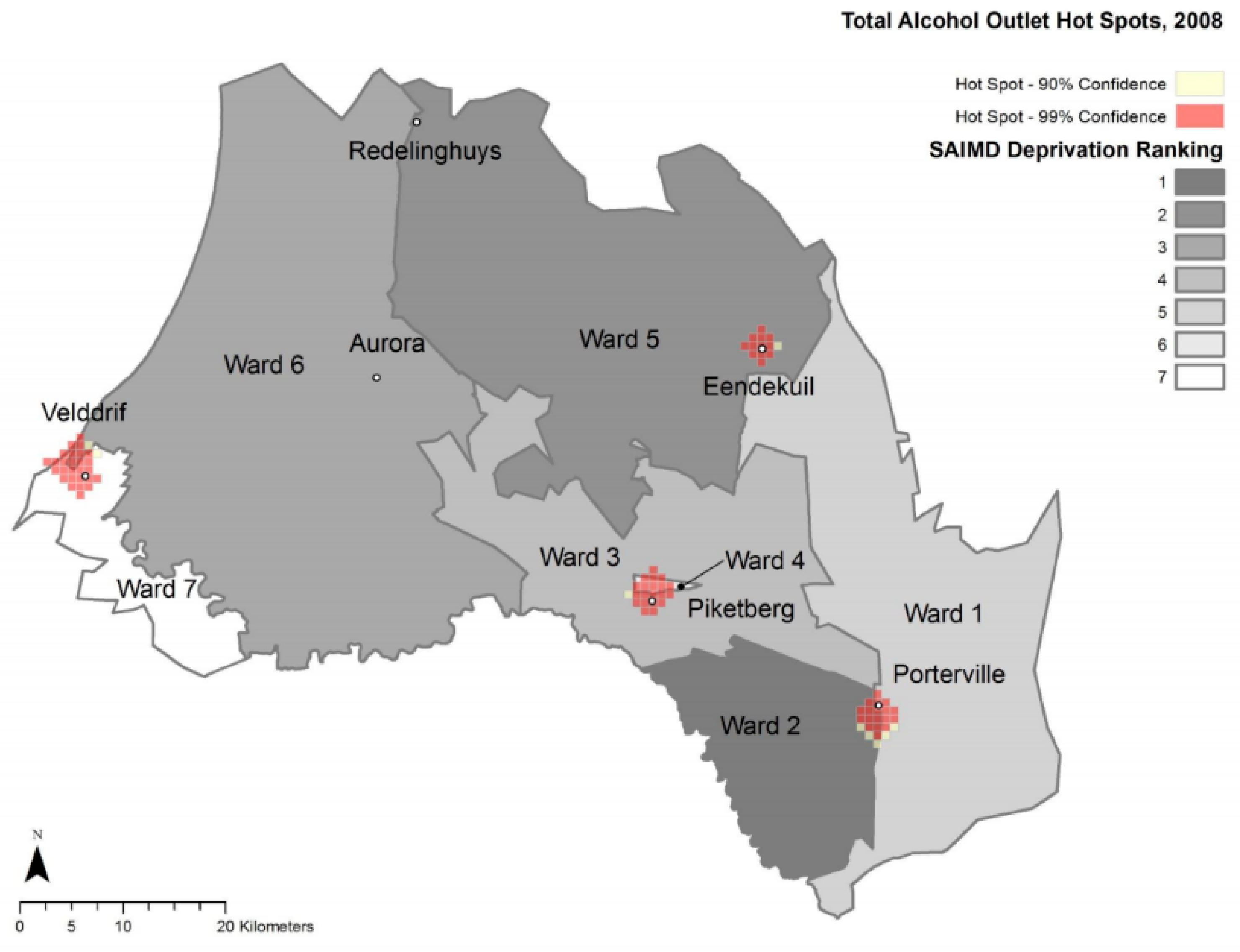
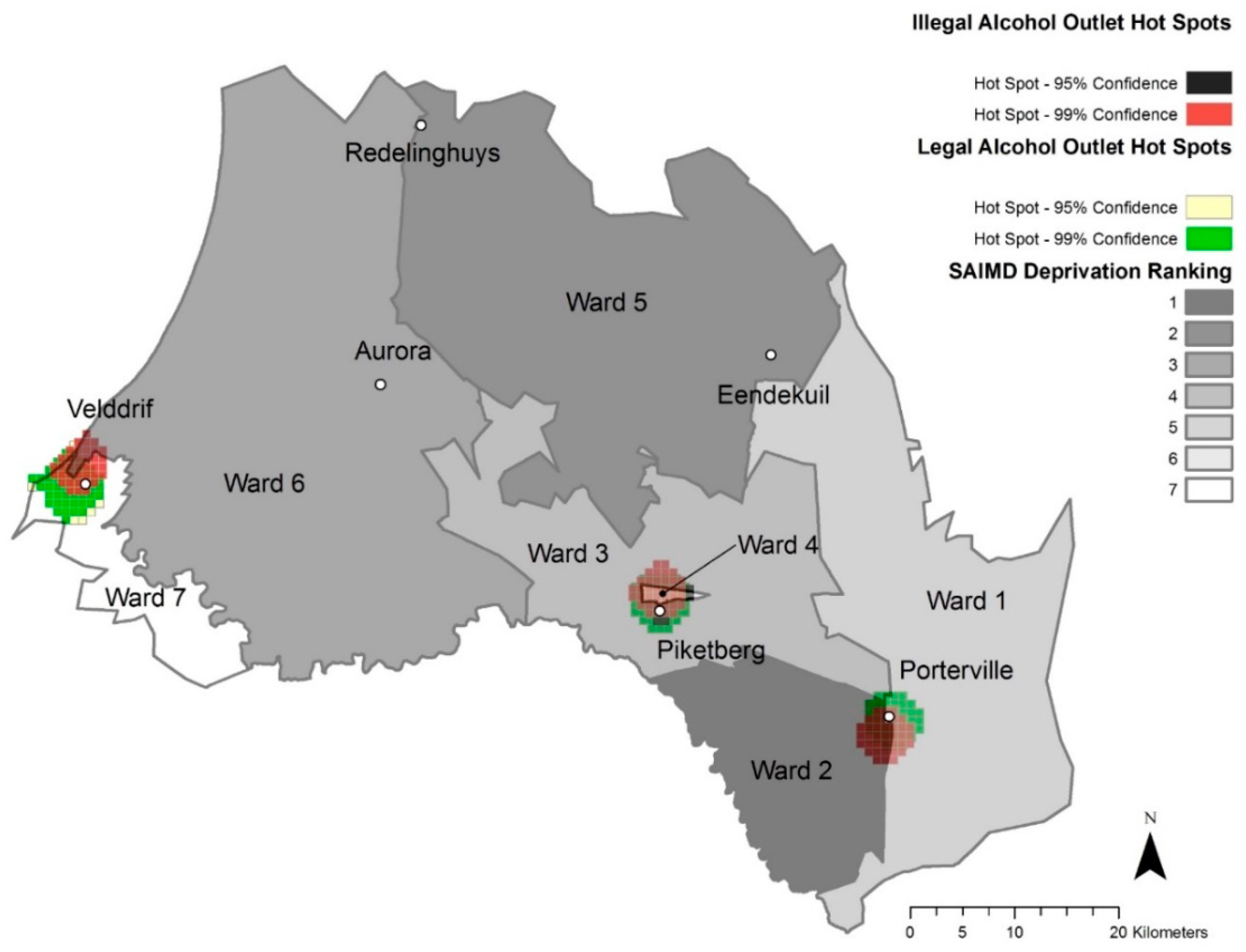
3.4. Maps
3.5. Hot Spot Analyses
4. Discussion
4.1. Study 1 and Study 2 differences
4.2. Alcohol Outlet Density
4.3. Deprivation and Alcohol Outlet Density
4.4. Geospatial Trends
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- May, P.A.; Blankenship, J.; Marais, A.S.; Gossage, J.P.; Kalberg, W.O.; Barnard, R.; Vries, M.D.; Robinson, L.K.; Adnams, C.M.; Buckley, D.; et al. Approaching the Prevalence of the Full Spectrum of Fetal Alcohol Spectrum Disorders in a South African Population-Based Study. Alcohol. Clin. Exp. Res. 2013, 37, 818–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivier, L.; Urban, M.; Chersich, M.; Temmerman, M.; Viljoen, D. Burden of fetal alcohol syndrome in a rural West Coast area of South Africa. S. Afr. Med J. 2013, 103, 402–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, P.A.; Brooke, L.; Gossage, J.P.; Croxford, J.; Adnams, C.; Jones, K.L.; Robinson, L.; Viljoen, D. Epidemiology of fetal alcohol syndrome in a South African community in the Western Cape Province. Am. J. Public Health 2000, 90, 1905–1912. [Google Scholar] [PubMed] [Green Version]
- May, P.A.; Gossage, J.P.; Marais, A.S.; Adnams, C.M.; Hoyme, H.E.; Jones, K.L.; Robinson, L.K.; Khaole, N.C.O.; Snell, C.; Kalberg, W.O.; et al. The epidemiology of fetal alcohol syndrome and partial FAS in a South African community. Drug Alcohol Depend. 2007, 88, 259–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viljoen, D.L.; Philip Gossage, J.; Brooke, L.; Adnams, C.M.; Jones, K.L.; Robinson, L.K.; Hoyme, H.E.; Snell, C.; Khaole, N.C.O.; Kodituwakku, P.; et al. Fetal Alcohol Syndrome Epidemiology in a South African Community: A Second Study of a Very High Prevalence Area. J. Stud. Alcohol 2005, 66, 593–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organization. World Health Statistics 2014 a Wealth of Information on Global Public Health; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Smith, C.; Morrison, K. Disaggregating Relationships between off-Premise Alcohol Outlets and Trauma; Foundation for Alcohol Research and Education: Deakin West, Australia, 2015. [Google Scholar]
- Campbell, C.A.; Hahn, R.A.; Elder, R.; Brewer, R.; Chattopadhyay, S.; Fielding, J.; Naimi, T.S.; Toomey, T.; Lawrence, B.; Middleton, J.C. The Effectiveness of Limiting Alcohol Outlet Density as a Means of Reducing Excessive Alcohol Consumption and Alcohol-Related Harms. Am. J. Prev. Med. 2009, 37, 556–569. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ‘Best Buys’ and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Leslie, H.H.; Ahern, J.; Pettifor, A.E.; Twine, R.; Kahn, K.; Gómez-Olivé, F.X.; Lippman, S.A. Collective efficacy, alcohol outlet density, and young men’s alcohol use in rural South Africa. Health Place 2015, 34, 190–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niehaus, I.; Stadler, J. Muchongolo Dance Contests: Deep Play in the South African Lowveld. Ethnology 2004, 43, 363–380. [Google Scholar] [CrossRef]
- Matzopoulos, R.; Berens, C.; Bowman, B.; Bloch, K.; Langa, M.; Kotze, E.; Lloyd, S.; Makanga, P.; Mureithi, L.; Schuurman, N. A Mixed-Methods Study of the Nature and Extent of the Alcohol Trade in Khayelitsha—Resources—SaferSpaces. Available online: https://www.saferspaces.org.za/resources/entry/a-mixed-methods-study-of-the-nature-and-extent-of-the-alcohol-trade-in-khay (accessed on 30 October 2019).
- Informal Liquor Retailing. 2015. Available online: http://livelihoods.org.za/wp-content/uploads/2015/05/SLF-Informal-Liquor-final.pdf (accessed on 30 October 2019).
- Impact Assessment on the Effectiveness of the Liquor Act 59 of 2003. 2013. Available online: https://www.thedti.gov.za/business_regulation/docs/nla/Liquor_report_DNA_Economics.pdf (accessed on 30 October 2019).
- Bowers, Y.; Rendall-Mkosi, K.; Davids, A.; Nel, E.; Jacobs, N.; London, L. Liquor outlet density, deprivation and implications for foetal alcohol syndrome prevention in the Bergriver municipality in the Western Cape, South Africa. S. Afr. Geogr. J. 2014, 96, 153–165. [Google Scholar] [CrossRef] [Green Version]
- Grinzi, P.; Phillips, R.L.; Bazemore, A. Navigating general practice: The use of geographic information systems. Aust. Fam. Physician 2008, 37, 855. [Google Scholar] [PubMed]
- Meng, G.; Law, J.; Thompson, M.E. Small-scale health-related indicator acquisition using secondary data spatial interpolation. Int. J. Health Geogr. 2010, 9, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reducing alcohol-related harms in the Western Cape Adapted from the Western Cape Alcohol Related Harms Reduction Policy White Paper 2017. Available online: https://www.westerncape.gov.za/text/2017/November/reducing_alcohol-related_harms_in_the_western_cape-flyer-2017.pdf (accessed on 8 October 2019).
- Matzopoulos, R.G.; Truen, S.; Bowman, B.; Corrigall, J. The cost of harmful alcohol use in South Africa. SAMJ S. Afr. Med. J. 2014, 104, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Western Cape Liquor Authority. Annual Report: Western Cape Liquor Authority, Cape Town, South Africa 2012/2013. Available online: https://www.wcpp.gov.za/sites/default/files/WCLA_AR_2012-2013_published_version[1].pdf (accessed on 8 October 2019).
- Department of the Premier Western Cape Government. Western Cape Alcohol-Related Harms Reduction Policy White Paper; Western Cape Government: Cape Town, South Africa, 2017. Available online: https://www.westerncape.gov.za/text/2017/September/white_paper_alcohol-related_harms_reduction.pdf (accessed on 8 October 2019).
- Olivier, L.; Curfs, L.; Viljoen, D. Fetal alcohol spectrum disorders: Prevalence rates in South Africa. S. Afr. Med. J. 2016, 106, 103–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- High Level of Foetal Alcohol Syndrome Found in Saldanha Bay|GroundUp. Available online: https://www.groundup.org.za/article/high-level-foetal-alcohol-syndrome-found-saldhana-bay/ (accessed on 30 October 2019).
- What is GIS? Geographic Information System Mapping Technology. Available online: https://www.esri.com/en-us/what-is-gis/overview (accessed on 5 December 2019).
- Noble, M.; Zembe, W.; Wright, G.; Avenell, D.; Noble, S. Income Poverty at Small Area Level in South Africa in 2011. Cape Town SASPRI. 2014, pp. 3–4. Available online: https://www.saspri.org/wp-content/uploads/Docs/Income_Poverty_at_ward_level_National_Report_for_Web.pdf (accessed on 8 October 2019).
- Municipality, Bergrivier. Ward plan: Ward 1: Fourth Integrated Development Plan 2017–2022. Bergrivier Municipality South Africa, 2017. Available online: https://www.bergmun.org.za/download_document/1344 (accessed on 8 October 2019).
- Keller, G. Statistics for Management and Economics; Cengage Learning: Boston, MA, USA, 2014; ISBN 978-0-538-47749-9. [Google Scholar]
- Optimized Hot Spot Analysis—Help|ArcGIS Desktop. Available online: http://desktop.arcgis.com/en/arcmap/10.3/tools/spatial-statistics-toolbox/optimized-hot-spot-analysis.htm (accessed on 8 October 2019).
- Africa, S.S. Local Municipality|Statistics South Africa. Available online: http://www.statssa.gov.za/?page_id=993 (accessed on 9 December 2019).
- SuperWEB2(tm)—Datasets. Available online: http://superweb.statssa.gov.za/webapi/jsf/dataCatalogueExplorer.xhtml (accessed on 9 December 2019).
- Census 2011: Local Municipality: Bergrivier. Available online: https://census2011.adrianfrith.com/place/162 (accessed on 9 December 2019).
- Fontes Marx, M.; London, L.; Harker Burnhams, N.; Ataguba, J. Usability of existing alcohol survey data in South Africa: A qualitative analysis. BMJ Open 2019, 9, 31560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, M.; Pettifor, A.; Rie, A.V.; Thirumurthy, H.; Emch, M.; Miller, W.C.; Gómez-Olivé, F.X.; Twine, R.; Hughes, J.P.; Laeyendecker, O.; et al. The Relationship between Alcohol Outlets, HIV Risk Behavior, and HSV-2 Infection among South African Young Women: A Cross-Sectional Study. PLoS ONE 2015, 10, 125510. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Town | 2001 Total Population [31] | 2011 Total Population [31] |
|---|---|---|
| Aurora | 342 | 578 |
| Eendekuil | 841 | 1530 |
| Piketberg | 9271 | 12,075 |
| Porterville | 5864 | 7057 |
| Redelinghuys | 581 | 574 |
| Velddrif | 7327 | 11,017 |
| Total Study Area | 24,226 | 32,831 |
| Town | 2008 Total Outlets | 2016 Total Outlets | 2008 Percent Illegal Outlets | 2016 Percent Illegal Outlets | 2008 Outlets/km2 [32] | 2016 Outlets/km2 [32] | 2008 Outlets/1000 Persons | 2016 Outlets/1000 Persons |
|---|---|---|---|---|---|---|---|---|
| Aurora | 3 | 3 | 33.33 | 0 | 1.84 | 1.84 | 8.76 | 5.19 |
| Eendekuil | 8 | 4 | 75.00 | 75.00 | 9.41 | 4.69 | 9.51 | 2.61 |
| Piketberg | 39 | 25 | 43.59 | 36.00 | 2.94 | 1.88 | 4.21 | 2.07 |
| Porterville | 19 | 20 | 31.58 | 40.00 | 2.38 | 2.51 | 3.24 | 2.83 |
| Redelinghuys | 3 | 4 | 33.33 | 50.00 | 1.42 | 1.89 | 5.17 | 6.97 |
| Velddrif | 40 | 43 | 40.00 | 48.84 | 4.51 | 4.85 | 5.46 | 3.90 |
| Total Study Area | 112 | 99 | 41.96 | 43.43 | 3.23 | 2.85 | 4.62 | 3.02 |
| Town | Total Outlets/1000 Persons (difference) | Illegal Outlets/1000 (difference) | Legal Outlets/1000 (difference) |
|---|---|---|---|
| Aurora | (−3.57) | (−2.92) | (−0.65) |
| Eendekuil | (−6.90) | (−5.17) | (−1.73) |
| Piketberg | (−2.14) | (−1.08) | (−1.04) |
| Porterville | (−0.41) | (+0.11) | (−0.52) |
| Redelinghuys | (+1.8) | (+1.76) | (+0.03) |
| Velddrif | (−1.56) | (−0.27) | (−1.28) |
| Town | Total Outlets/km2 (difference) | Illegal Outlets/km2 (difference) | Legal Outlets/km2 (difference) |
|---|---|---|---|
| Aurora | (0) | (−0.61) | (+0.61) |
| Eendekuil | (−4.72) | (−3.53) | (−1.17) |
| Piketberg | (−1.06) | (−0.6) | (−0.45) |
| Porterville | (+0.13) | (+0.25) | (−0.13) |
| Redelinghuys | (+0.47) | (+0.47) | (0) |
| Velddrif | (+0.34) | (+0.57) | (−0.23) |
| SAIMD Rank 1 | WARD | Illegal Alcohol Outlets/1000 persons | Legal Alcohol Outlets/1000 persons | Total Alcohol Outlets/1000 persons |
|---|---|---|---|---|
| 1 most deprived | 2 | 1.41 | 0.35 | 1.76 |
| 2 | 5 | 0.35 | 0.21 | 0.56 |
| 3 | 6 | 5.28 | 1.01 | 6.29 |
| 4 | 3 | 0 | 1.16 | 1.16 |
| 5 | 1 | 0 | 0.87 | 0.87 |
| 6 | 4 | 0.87 | 0.48 | 1.36 |
| 7 least deprived | 7 | 0 | 1.71 | 1.71 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowers, Y.; Davids, A.; London, L. Alcohol Outlet Density and Deprivation in Six Towns in Bergrivier Municipality before and after Legislative Restrictions. Int. J. Environ. Res. Public Health 2020, 17, 697. https://doi.org/10.3390/ijerph17030697
Bowers Y, Davids A, London L. Alcohol Outlet Density and Deprivation in Six Towns in Bergrivier Municipality before and after Legislative Restrictions. International Journal of Environmental Research and Public Health. 2020; 17(3):697. https://doi.org/10.3390/ijerph17030697
Chicago/Turabian StyleBowers, Yasmin, Adlai Davids, and Leslie London. 2020. "Alcohol Outlet Density and Deprivation in Six Towns in Bergrivier Municipality before and after Legislative Restrictions" International Journal of Environmental Research and Public Health 17, no. 3: 697. https://doi.org/10.3390/ijerph17030697