Estimating Lifetime Dental Care Expenditure in South Korea: An Abridged Life Table Approach


Abstract
:1. Introduction
2. Methods
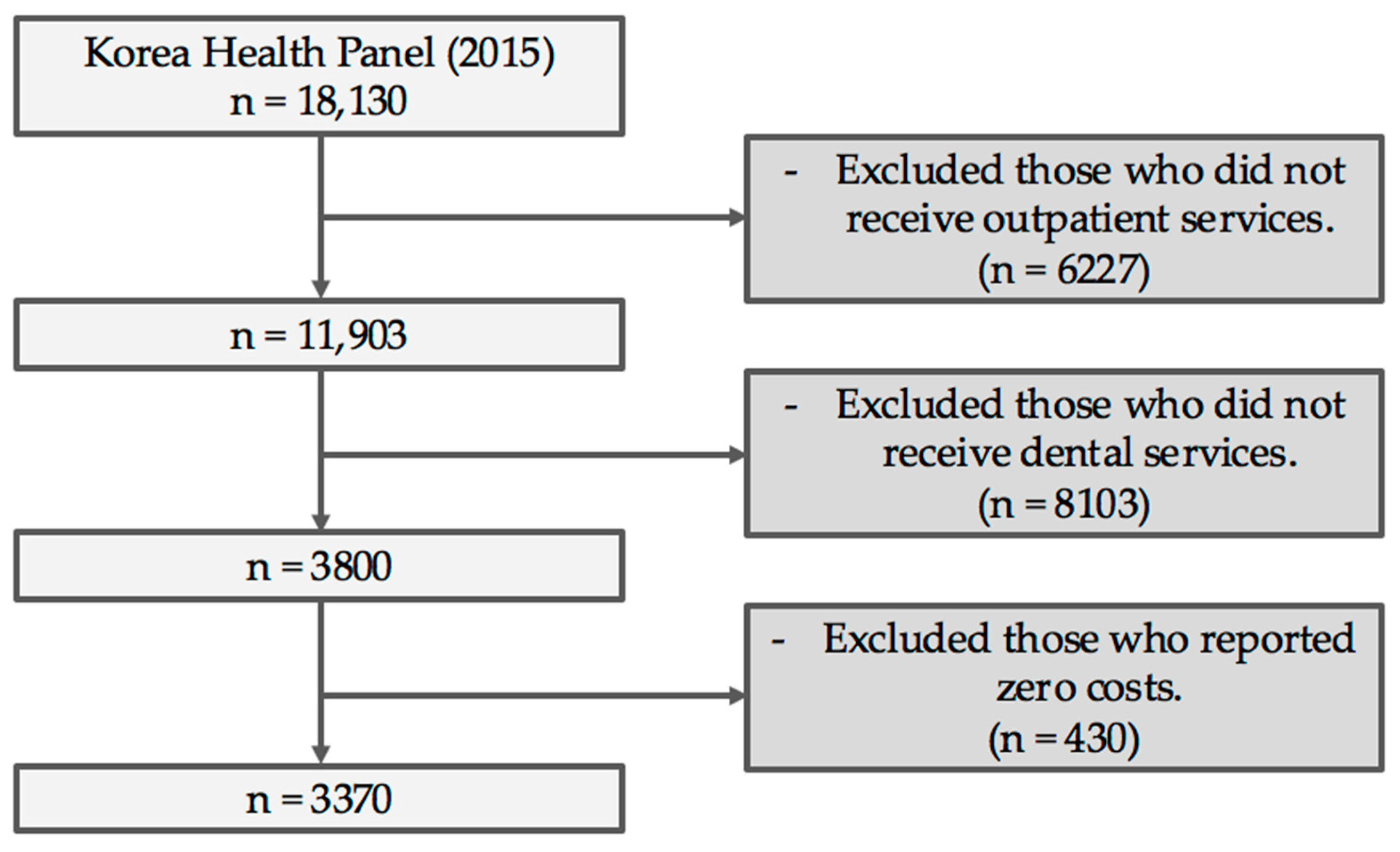
2.1. Study Design and Data Resource
2.2. Analysis
2.3. Estimation of Lifetime Dental Expenditure
3. Results
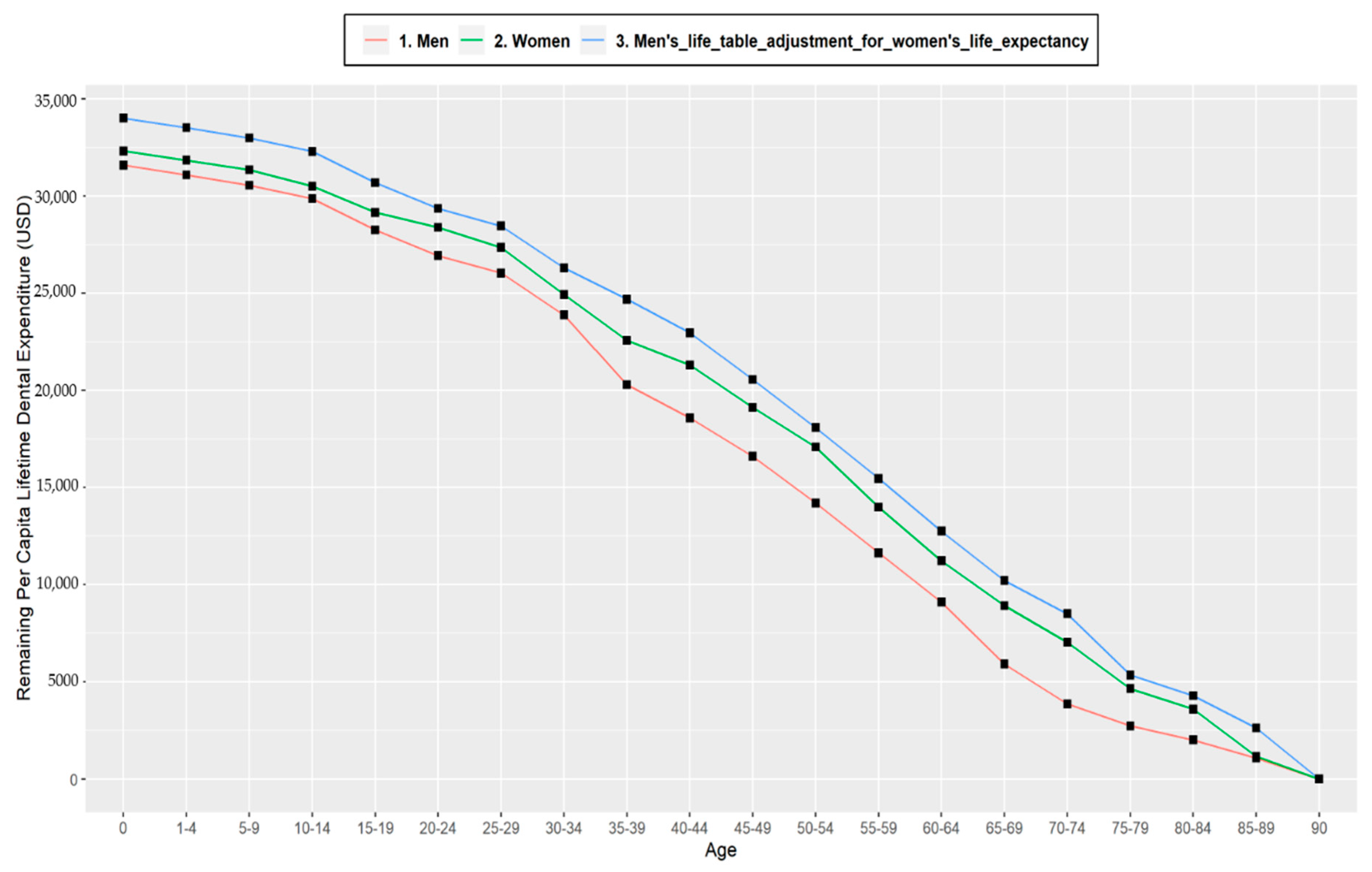
3.1. Remaining Lifetime per Capita Dental Expenditure for Men and Women, Relative Lifetime Dental Expenditures for Life Table Cohort
3.2. Lifetime per Capita Expenditure by Adjustment for Women’s Longer Life Expectancy
3.3. Per Capita Lifetime Dental Expenditures for Men and Women, Relative Lifetime Dental Expenditures for Survivors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health 2015. Available online: https://books.google.com.hk/books?hl=zh-CN&lr=&id=n180DgAAQBAJ&oi=fnd&pg=PP1&dq=World+Report+on+ageing+and+health+&ots=uSL9hsJZl1&sig=yLrFBW49RrvR9yQOX1vOhPUnO2A&redir_esc=y&hl=zh-CN&sourceid=cndr#v=onepage&q=World%20Report%20on%20ageing%20and%20health&f=false (accessed on 8 May 2020).
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzatiet, M. Future life expectancy in 35 industrialised countries: Projections with a Bayesian model ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef] [Green Version]
- Hyun, K.R.; Kang, S.; Lee, S. Population aging and healthcare expenditure in Korea. Health Econ. 2016, 25, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Jeong, G.W.; Kim, Y.J.; Park, S.; Kim, H.; Kwonet, O. Associations of recommended food score and physical performance in Korean elderly. BMC Public Health 2019, 19, 128. [Google Scholar] [CrossRef]
- Statistics Korea. Population Projections for Korea. Available online: http://kostat.go.kr/portal/eng/pressReleases/8/8/index.board (accessed on 8 May 2020).
- Tchoe, B.; Nam, S.-H. Aging risk and health care expenditure in Korea. Int. J. Environ. Res. Public Health 2010, 7, 3235–3254. [Google Scholar] [CrossRef]
- Matsuyama, Y.; Tsakos, G.; Listl, S.; Aida, J.; Watt, R.G. Impact of Dental Diseases on Quality-Adjusted Life Expectancy in US Adults. J. Dent. Res. 2019, 98, 510–516. [Google Scholar] [CrossRef]
- Mittal, R.; Wong, M.L.; Koh, G.C.H.; Ong, D.L.S.; Lee, Y.H.; Tan, M.N.; Allenet, P.F. Factors affecting dental service utilisation among older Singaporeans eligible for subsidized dental care–A qualitative study. BMC Public Health 2019, 19, 1075. [Google Scholar] [CrossRef]
- Jin, L.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriyaet, S. Global burden of oral diseases: Emerging concepts, management and interplay with systemic health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef]
- OECD. A Glance 2013: OECD Indicators. Available online: https://www.oecd-ilibrary.org/docserver/health_glance-2013en.pdf?expires=1588946606&id=id&accname=guest&checksum=34F8D36094F5F1DDB833713673D616C3 (accessed on 8 May 2020).
- Listl, S.; Galloway, J.; Mossey, P.A.; Marcenes, W. Global economic impact of dental diseases. J. Dental Res. 2015, 94, 1355–1361. [Google Scholar] [CrossRef]
- The State of Oral Health in Europe. Report Commissioned by the Platform for better Oral Health in Europe. Available online: http://www.oralhealthplatform.eu/about-us/oral-health/ (accessed on 22 April 2020).
- Health Insurance Review and Assessment Service and National Health Insurance Service. 2017. Available online: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020045020000&brdScnBltNo=4&brdBltNo=2310&pageIndex=1 (accessed on 8 May 2020).
- Heilmann, A.; Tsakos, G.; Watt, R.G. A life course perspective on health trajectories and transitions. Oral Health Life Course 2015, 39–59. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Palència, L.; Espelt, A.; Cornejo-Ovalle, M.; Borrell, C. Socioeconomic inequalities in the use of dental care services in Europe: What is the role of public coverage. Community Dent. Oral Epidemiol. 2014, 42, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Teusner, D.; Smith, V.; Gnanamanickam, E.; Brennan, D. Examining dental expenditure and dental insurance accounting for probability of incurring expenses. Community Dent. Oral Epidemiol. 2017, 45, 101–111. [Google Scholar] [CrossRef]
- Lee, W.; Kim, S.-J.; Albert, J.M.; Nelson, S. Community factors predicting dental care utilization among older adults. J. Am. Dent. Assoc. 2014, 145, 150–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.C.; Lee, C.; Chang, Y.H.; Ku, L.J.; Li, C.Y. Demographic and rural--urban variations in dental service utilization in Taiwan. Rural Remote Health 2017, 17, 4161. [Google Scholar] [CrossRef]
- Reda, S.M.; Krois, J.; Reda, S.F.; Thomson, W.M.; Schwendicke, F. The impact of demographic, health-related and social factors on dental services utilization: Systematic review and meta-analysis. Int. J. Dent. 2018, 75, 1–6. [Google Scholar] [CrossRef]
- Alemayehu, B.; Warner, K.E. The lifetime distribution of health care costs. Health Serv. Res. 2004, 39, 627–642. [Google Scholar] [CrossRef]
- Basu, R.; Krueger, P.M.; Lairson, D.R.; Franziniet, L. Lifetime medical expenditures among hypertensive men and women in the United States. Women Health Issues 2011, 21, 246–253. [Google Scholar] [CrossRef]
- Statics Korea. 2016. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/2/7/index.board?bmode=read&aSeq=357847&pageNo=&rowNum=10&amSeq=&sTarget=&sTxt= (accessed on 17 December 2019).
- Sagna, A.; Kemp, M.L.S.; DiNitto, D.M.; Choi, N.G. Impact of suicide mortality on life expectancy in the United States, 2011 and 2015: Age and sex decomposition. Public Health 2020, 179, 76–83. [Google Scholar] [CrossRef]
- Khang, Y.H.; Bahk, J.; Lim, D.; Kang, H.Y.; Lim, H.K.; Kim, Y.Y.; Park, J.H. Trends in inequality in life expectancy at birth between 2004 and 2017 and projections for 2030 in Korea: Multiyear cross-sectional differences by income from national health insurance data. BMJ Open 2019, 9, 030683. [Google Scholar] [CrossRef] [Green Version]
- Lauritano, D.; Moreo, G.; Vella, F.D.; Stasio, D.D.; Carinci, F.; Lucchese, A.; Petruzzi, M. Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christian, B.; Chattopadhyay, A. Determinants and trends in dental expenditures in the adult US population: Medical Expenditure Panel Survey 1996-2006. Community Dent. Health 2014, 31, 99–104. [Google Scholar] [PubMed]
- Korea Centers for Disease Control and Prevention. 2016. Available online: https://knhanes.cdc.go.kr/knhanes/sub04/sub04_03.do?classType=7 (accessed on 8 May 2020).
- Moon, S.H.; Hong, G.R.S. Predictors of chewing discomfort among community dwelling elderly. J. Korean Acad. Community Health Nurs. 2017, 28, 302–312. [Google Scholar] [CrossRef]
- Naavaal, S.; Griffin, S.O.; Jones, J.A. Impact of making dental care affordable on quality of life in adults aged 45 years and older. J. Aging Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Spillman, B.C.; Lubitz, J. The effect of longevity on spending for acute and long-term care. N. Engl. J. Med. 2000, 342, 1409–1415. [Google Scholar] [CrossRef]
- Che, X.; Sohn, M.; Park, H.J. Unmet dental care needs in South Korea: How do they differ by insurance system. J. Health Serv. Res. Pol. 2019, 24, 164–171. [Google Scholar] [CrossRef]
- Sohn, M.; Park, S.; Lim, S.; Park, H.J. Children’s Dental Sealant Use and Caries Prevalence Affected by National Health Insurance Policy Change: Evidence from the Korean National Health and Nutrition Examination Survey (2007–2015). Int. J. Environ. Res. Public Health 2019, 16, 2773. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Lee, J.S.; Choi, J.K.; Kweon, H.I.; Kim, Y.T.; Choi, S.H. National dental policies and socio-demographic factors affecting changes in the incidence of periodontal treatments in Korean: A nationwide population-based retrospective cohort study from 2002–2013. BMC Oral Health 2016, 16, 118. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Lee, J.H.; Park, S.; Kim, T.I. Trends in the utilization of dental outpatient services affected by the expansion of health care benefits in South Korea to include scaling: A 6-year interrupted time-series study. J. Periodontal. Implant. Sci. 2018, 48, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Lee, J.H.; Park, S.; Kim, T.I. Changes in dental care access upon health care benefit expansion to include scaling. J. Periodontal. Implant Sci. 2016, 46, 405–414. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Age | Death Rate | Dental Expenditure per Capita | Lifetime Dental Expenditure | |||
|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | |
| 0 | 0.00292 | 0.00251 | - | - | $31,587 | $32,318 |
| 1–4 | 0.00073 | 0.00055 | $124.86 | $118.30 | $31,089 | $31,846 |
| 5–9 | 0.00051 | 0.00035 | $106.73 | $98.23 | $30,557 | $31,356 |
| 10–14 | 0.00053 | 0.00032 | $138.07 | $171.24 | $29,870 | $30,504 |
| 15–19 | 0.00130 | 0.00075 | $323.92 | $471.36 | $28,259 | $29,156 |
| 20–24 | 0.00214 | 0.00112 | $266.21 | $355.53 | $26,937 | $28,388 |
| 25–29 | 0.00298 | 0.00168 | $182.31 | $409.08 | $26,034 | $27,355 |
| 30–34 | 0.00365 | 0.00241 | $435.88 | $425.83 | $23,883 | $24,931 |
| 35–39 | 0.00504 | 0.00300 | $731.21 | $275.73 | $20,289 | $22,568 |
| 40–44 | 0.00826 | 0.00413 | $349.67 | $257.50 | $18,581 | $21,299 |
| 45–49 | 0.01384 | 0.00580 | $409.36 | $445.08 | $16,604 | $19,117 |
| 50–54 | 0.02156 | 0.00766 | $507.69 | $417.66 | $14,194 | $17,083 |
| 55–59 | 0.03097 | 0.01078 | $543.84 | $642.80 | $11,630 | $13,981 |
| 60–64 | 0.04578 | 0.01627 | $568.39 | $578.40 | $9102 | $11,226 |
| 65–69 | 0.06852 | 0.02677 | $759.56 | $495.49 | $5914 | $8916 |
| 70–74 | 0.11724 | 0.05289 | $537.49 | $419.32 | $3859 | $7035 |
| 75–79 | 0.20762 | 0.10752 | $350.95 | $574.93 | $2730 | $4655 |
| 80–84 | 0.33656 | 0.21343 | $300.69 | $302.55 | $2020 | $3595 |
| 85–89 | 0.50259 | 0.38194 | $668.40 | $974.11 | $1091 | $1172 |
| 90– | 1.00000 | 1.00000 | $144.35 | $642.99 | - | - |
| Age | Men | Women | ||
|---|---|---|---|---|
| Lifetime per Capita Dental Expenditure | Relative Lifetime Dental Expenditure | Lifetime per Capita Dental Expenditure | Relative Lifetime Dental Expenditure | |
| 0 | $31,587 | 100% | $32,318 | 100% |
| 20 | $26,937 | 89.5% | $28,388 | 87.1% |
| 40 | $18,581 | 64.3% | $21,299 | 69.8% |
| 50 | $14,194 | 52.6% | $17,083 | 59.1% |
| 65 | $5914 | 28.9% | $8916 | 34.7% |
| 75 | $2730 | 12.3% | $4655 | 21.7% |
| Age | Men | Women | ||
|---|---|---|---|---|
| Lifetime per Capita Dental Expenditure | Relative Lifetime Dental Expenditure | Lifetime per Capita Dental Expenditure | Relative Lifetime Dental Expenditure | |
| 0 | $38,932 | 100% | $37,772 | 100% |
| 20 | $34,261 | 91.4% | $31,819 | 88.9% |
| 40 | $25,786 | 70.7% | $24,987 | 65.9% |
| 50 | $21,240 | 61.0% | $20,687 | 60.2% |
| 65 | $12,104 | 40.5% | $12,172 | 38.6% |
| 75 | $7978 | 24.5% | $7389 | 26.7% |
| Age Intervals | Life Table Cohort | Survivors | ||
|---|---|---|---|---|
| Men | Women | Men | Women | |
| 0–19 | 10.5% | 12.9% | 8.6% | 11.1% |
| 20–39 | 25.2% | 17.3% | 20.7% | 23.0% |
| 40–49 | 11.7% | 10.7% | 9.7% | 5.7% |
| 50–64 | 23.7% | 24.4% | 20.5% | 21.6% |
| 65–74 | 16.6% | 13.0% | 16.0% | 11.9% |
| 75 | 12.3% | 21.8% | 24.5% | 26.7% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sohn, M.; Che, X.; Lim, S.; Park, H.-J. Estimating Lifetime Dental Care Expenditure in South Korea: An Abridged Life Table Approach. Int. J. Environ. Res. Public Health 2020, 17, 3308. https://doi.org/10.3390/ijerph17093308
Sohn M, Che X, Lim S, Park H-J. Estimating Lifetime Dental Care Expenditure in South Korea: An Abridged Life Table Approach. International Journal of Environmental Research and Public Health. 2020; 17(9):3308. https://doi.org/10.3390/ijerph17093308
Chicago/Turabian StyleSohn, Minsung, Xianhua Che, Sungwon Lim, and Hee-Jung Park. 2020. "Estimating Lifetime Dental Care Expenditure in South Korea: An Abridged Life Table Approach" International Journal of Environmental Research and Public Health 17, no. 9: 3308. https://doi.org/10.3390/ijerph17093308