
Sustainable Service-Learning in Physical Education Teacher Education: Examining Postural Control to Promote ASD Children’s Well-Being

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
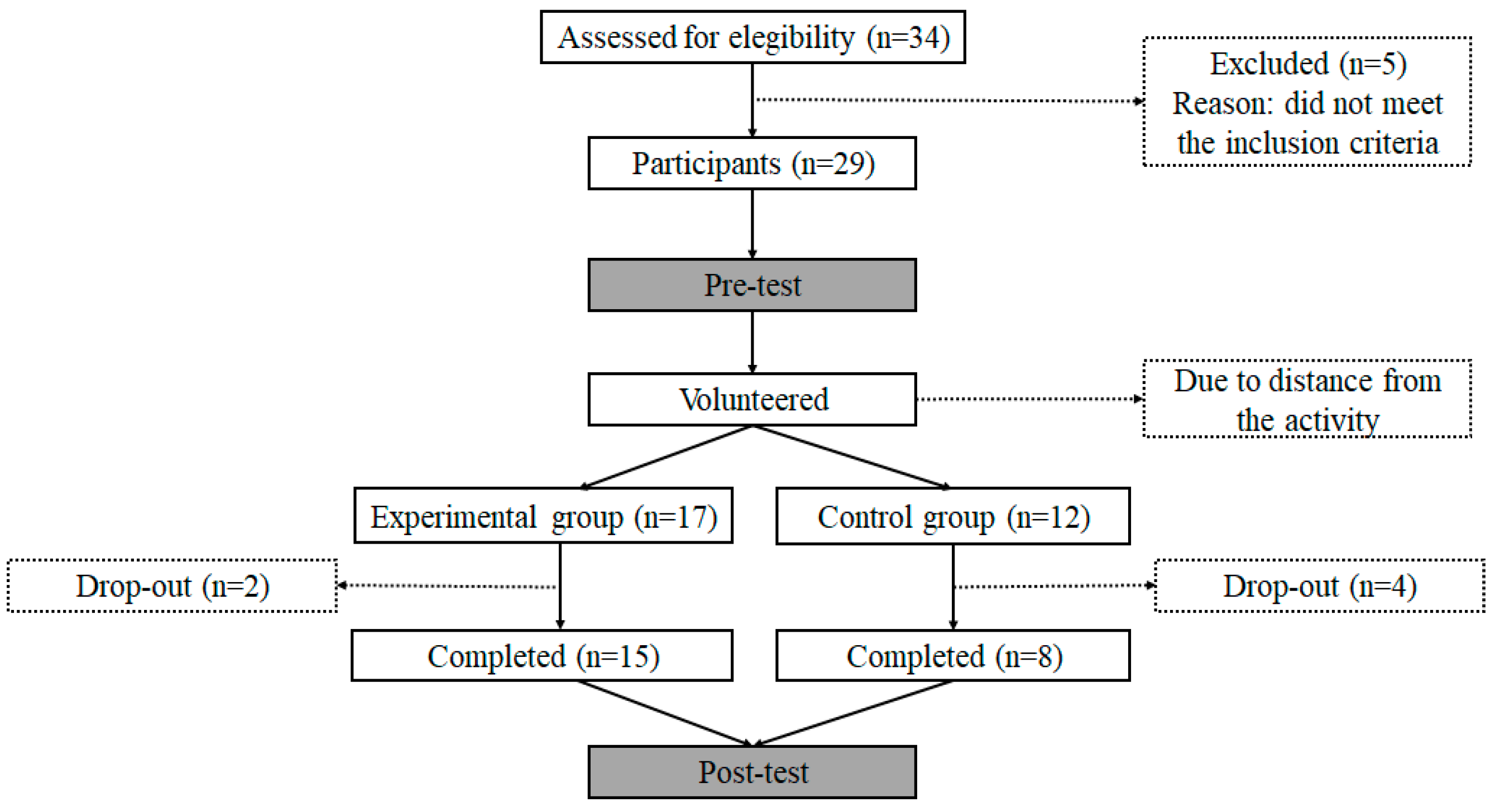
2.2. Sample
2.3. Materials
2.4. Procedures
2.5. Intervention Program
2.6. Data Analysis
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tant, M.; Watelain, E. Forty years later, a systematic literature review on inclusion in physical education (1975–2015): A teacher perspective. Educ. Res. Rev. 2016, 19, 1–17. [Google Scholar] [CrossRef]
- Wilhelmsen, T.; Sørensen, M. Physical education-related home–school collaboration. Eur. Phys. Educ. Rev. 2018, 25, 830–846. [Google Scholar] [CrossRef]
- Bringle, R.G.; Hatcher, J.A. Implementing Service Learning in Higher Education. J. Higher Educ. 1996, 67, 221–239. [Google Scholar] [CrossRef]
- Case, L.; Schram, B.; Jung, J.; Leung, W.; Yun, J. A meta-analysis of the effect of adapted physical activity service-learning programs on college student attitudes toward people with disabilities. Disabil. Rehabil. 2020. [Google Scholar] [CrossRef]
- Cervantes, C.M.; Meaney, K.S. Examining Service-Learning Literature in Physical Education Teacher Education: Recommendations for Practice and Research. Quest 2013, 65, 332–353. [Google Scholar] [CrossRef]
- Chiva-Bartoll, O.; Ruiz-Montero, P.J.; Martín-Moya, R.; Pérez-López, I.; Giles-Girela, J.; García-Suárez, J.; Rivera-García, E. University Service-Learning in Physical Education and Sport Sciences: A systematic review. Rev. Complut. Educ. 2019, 30, 1147–1164. [Google Scholar] [CrossRef]
- Pérez-Ordás, R.; Nuviala, A.; Grao-Cruces, A.; Fernández-Martínez, A. Implementing Service-Learning Programs in Physical Education; Teacher Education as Teaching and Learning Models for All the Agents Involved: A Systematic Review. Int. J. Environ. Public Health 2020, 18, 669. [Google Scholar] [CrossRef]
- Maenner, M.J.; Matthew, J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.-L.; Wiggins, L.D.; Pettygrove, S.; et al. Prevalence of Autism Spectrum DisorderAmong ChildrenAged 8 Years-Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- American Psychiatric Association [APA]. Diagnostic and Statistical Manual-Text. Revision (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Gutstein, S.E.; Whitney, T. Asperger syndrome and thedevelopment of social competence. Focus Autism Other Dev. Disabil. 2002, 17, 161–171. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickless, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Weiss, M.J.; Harris, S.L. Teaching social skills to people with autism. Behav. Modif. 2001, 25, 785–802. [Google Scholar] [CrossRef]
- McConnell, S.R. Interventions to facilitate social interaction for young children with autism: Review of available research and recommendations for educational intervention and future research. J. Autism Dev. Disord. 2002, 32, 351–372. [Google Scholar] [CrossRef] [PubMed]
- Baranek, G.T.; David, F.J.; Poe, M.D.; Stone, W.L.; Watson, L.R. Sensory Experiences Questionnaire: Discriminating sensory features in young children with autism, developmental delays, and typical development. J. Child. Psychol. Psychiatry 2006, 47, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Trivedi, M.H.; Garver, C.R.; Grannemann, B.D.; Andrews, A.A.; Savla, J.S.; Johnson, D.A.; Mehta, J.A.; Schroeder, J.L. The pattern of sensory processing abnormalities in autism. Autism 2006, 10, 480–494. [Google Scholar] [CrossRef]
- Leekam, S.R.; Nieto, C.; Libby, S.J.; Wing, L.; Gould, J. Describing the sensory abnormalities of children and adults with autism. J. Autism Dev. Disord. 2007, 37, 894–910. [Google Scholar] [CrossRef] [PubMed]
- Liss, M.; Saulnier, C.; Fein, D.; Kinsbourne, M. Sensory and attention abnormalities in autistic spectrum disorders. Autism 2006, 10, 155–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, S.J.; Ozonoff, S. Annotation: What do we know about sensory dysfunction in autism? A critical review of the empirical evidence. J. Child. Psychol. Psychiatry 2005, 46, 1255–1268. [Google Scholar] [CrossRef]
- American Psychiatric Association [APA]. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Koegel, R.L.; Koegel, L.K.; McNerney, E.K. Pivotal areas in intervention for autism. J. Clin. Child. Adolesc. Psychol. 2001, 30, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.; Russell, J.; Robbins, T.W. Evidence for executive dysfunction in autism. Neuropsychologia 1994, 32, 477–492. [Google Scholar] [CrossRef]
- Fournier, K.A.; Kimberg, C.I.; Radonovich, K.J.; Tillman, M.D.; Chow, J.W.; Lewis, M.H.; Bodfish, J.W.; Hass, C.J. Decreased static and dynamic postural control in children with autism spectrum disorders. Gait Posture 2010, 32, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Breslin, C.M. Fine and gross motor performance of the MABC-2 by children with autism spectrum disorder and typically developing children. Res. Autism Spectr. Disord. 2013, 7, 1244–1249. [Google Scholar] [CrossRef]
- Memari, A.H.; Ghaheri, B.; Ziaee, V.; Kordi, R.; Hafizi, S.; Moshayedi, P. Physical activity in children and adolescents with autism assessed by triaxial accelerometry. Pediatr. Obes. 2013, 8, 150–158. [Google Scholar] [CrossRef]
- Kroeger, K.A.; Schultz, J.R.; Newsom, C. A comparison of two group-delivered social skills programs for young children with autism. J. Autism Dev. Disord. 2007, 37, 808–817. [Google Scholar] [CrossRef]
- Günal, A.; Bumin, G.; Huri, M. The Effects of Motor and Cognitive Impairments on Daily Living Activities and Quality of Life in Children with Autism. J. Occup. Ther. Sch. Early Interv. 2019, 44, 444–454. [Google Scholar] [CrossRef]
- Mattard-Labrecque, C.; Amor, L.B.; Couture, M.M. Children with autism and attention difficulties: A pilot study of the association between sensory, motor, and adaptive behaviors. J. Can. Acad. Child. Adolesc. Psychiatry 2013, 22, 139. [Google Scholar]
- Massion, J. Postural control system. Curr. Opin. Neurobiol. 1994, 4, 877–887. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, ii7–ii11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Hallac, R.R.; Conroy, K.C.; White, S.P.; Kane, A.A.; Collinsworth, A.L.; Sweeney, J.A.; Mosconi, M.W. Postural orientation and equilibrium processes associated with increased postural sway in autism spectrum disorder (ASD). J. Neurodev. Disord. 2016, 8, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westcott, S.L.; Lowes, L.P.; Richardson, P.K. Evaluation of postural stability in children: Current theories and assessment tools. Phys. Ther. 1997, 77, 629–645. [Google Scholar] [CrossRef]
- Han, T.R.; Paik, N.J.; Im, M.S. Quantification of the path of center of pressure (COP) using an F-scan in-shoe transducer. Gait Posture 1999, 10, 248–254. [Google Scholar] [CrossRef]
- Hasan, S.S.; Robin, D.W.; Shiavi, R.G. Drugs and postural sway: Quantifying balance as a tool to measure drug effects. IEEE Eng. Med. Biol. Mag. 1992, 11, 35–41. [Google Scholar] [CrossRef]
- Cheldavi, H.; Shakerian, S.; Boshehri, S.N.S.; Zarghami, M. The effects of balance training intervention on postural control of children with autism spectrum disorder: Role of sensory information. Res. Autism Spectr. Disord. 2014, 8, 8–14. [Google Scholar] [CrossRef]
- Kim, Y.; Todd, T.; Fujii, T.; Lim, J.C.; Vrongistinos, K.; Jung, T. Effects of Taekwondo intervention on balance in children with autism spectrum disorder. J. Exerc. Rehabil. 2016, 12, 314–319. [Google Scholar] [CrossRef]
- Molloy, C.A.; Dietrich, K.N.; Bhattacharya, A. Postural stability in children with autism spectrum disorder. J. Autism Dev. Disord. 2003, 33, 643–652. [Google Scholar] [CrossRef]
- Minshew, N.J.; Sung, K.; Jones, B.L.; Furman, J.M. Underdevelopment of the postural control system in autism. Neurology 2004, 63, 2056–2061. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.P.; Doyen, C.; Contenjean, Y.; Kaye, K. The effect of performing a dual task on postural control in children with autism. ISRN Neurosci. 2013, 2013, 796174. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.C.; Tsai, C.L. A light fingertip touch reduces postural sway in children with autism spectrum disorders. Gait Posture 2016, 43, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Wade, M.G.; Stoffregen, T.A.; Hsu, C.Y.; Pan, C.Y. Visual tasks and postural sway in children with and without autism spectrum disorders. Res. Dev. Disabil. 2010, 31, 1536–1542. [Google Scholar] [CrossRef]
- Fournier, K.A.; Amano, S.; Radonovich, K.J.; Bleser, T.M.; Hass, C.J. Decreased dynamical complexity during quiet stance in children with autism spectrum disorders. Gait Posture 2014, 39, 420–423. [Google Scholar] [CrossRef]
- Smoot Reinert, S.; Jackson, K.; Bigelow, K. Using posturography to examine the immediate effects of vestibular therapy for children with autism spectrum disorders: A feasibility study. Phys. Occup. Ther. Pediatr. 2015, 35, 365–380. [Google Scholar] [CrossRef]
- Sarabzadeh, M.; Azari, B.B.; Helalizadeh, M. The effect of six weeks of Tai Chi Chuan training on the motor skills of children with Autism Spectrum Disorder. J. Bodyw. Mov. Ther. 2019, 23, 284–290. [Google Scholar] [CrossRef]
- Giagazoglou, P.; Kokaridas, D.; Sidiropoulou, M.; Patsiaouras, A.; Karra, C.; Neofotistou, K. Effects of a trampoline exercise intervention on motor performance and balance ability of children with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 2701–2707. [Google Scholar] [CrossRef] [PubMed]
- Yaremko, R.M.; Harari, H.; Harrison, R.C.; Lynn, E. Handbook of Research and Quantitative Methods in Psychology; Taylor and Francis Group, Psychology Press: New York, NY, USA, 2013. [Google Scholar]
- Reinders, N.J.; Branco, A.; Wright, K.; Fletcher, P.C.; Bryden, P.J. Scoping review: Physical activity and social functioning in young people with autism spectrum disorder. Front. Psychol. 2019, 10, 120. [Google Scholar] [CrossRef] [Green Version]
- Fong, S.S.M.; Cheung, C.K.Y.; Ip, J.Y.; Chiu, J.H.N.; Lam, K.L.H.; Tsang, W.W.N. Sport-specific balance ability in Taekwondo practitioners. J. Hum. Sport Exerc. 2012, 7, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Jacoby, B. Service-Learning Essentials: Questions, Answers, and Lessons Learned; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- Ruggeri, A.; Dancel, A.; Johnson, R.; Sargent, B. The effect of motor and physical activity intervention on motor outcomes of children with autism spectrum disorder: A systematic review. Autism 2019, 24, 544–568. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1998. [Google Scholar]
- Chan, A.S.; Sze, S.L. Shaolin mind-body exercise as a neuropsychological intervention. In Health, Wellbeing, Competence and Aging; World Scientific Publishing: Hackensack, NJ, USA, 2013; pp. 201–211. [Google Scholar]
- Gatts, S. Neural mechanisms underlying balance control in tai chi. In Tai Chi Chuan. Med. Sport Sci. 2008, 52, 87–103. [Google Scholar]
- Van Pons Dijk, G.; Lenssen, A.; Leffers, P.; Kingma, H.; Lodder, J. Taekwondo training improves balance in volunteers over 40. Front. Aging Neurosci. 2013, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Lidstone, D.E.; Miah, F.Z.; Poston, B.; Beasley, J.F.; Dufek, J.S. Examining the specificity of postural control deficits in children with Autism Spectrum Disorder using a cross-syndrome approach. Res. Autism Spectr. Disord. 2020, 72, 101514. [Google Scholar] [CrossRef]
- Agostini, V.; Sbrollini, A.; Cavallini, C.; Busso, A.; Pignata, G.; Knaflitz, M. The role of central vision in posture: Postural sway adaptations in Stargardt patients. Gait Posture 2016, 43, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Paulus, W.M.; Straube, A.; Brandt, T.H. Visual stabilization of posture: Physiological stimulus characteristics and clinical aspects. Brain 1984, 107, 1143–1163. [Google Scholar] [CrossRef]
- Peterka, R.J. Sensorimotor integration in human postural control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [Green Version]
- Kohen-Raz, R.; Volkman, F.R.; Cohen, D.J. Postural control in children with autism. J. Autism Dev. Disord. 1992, 22, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Bartoll, O.; Maravé-Vivas, O.; Salvador-García, C.; Valverde, T. Impact of a Physical Education Service-Learning programme on ASD children: A mixed-methods approach. Child. Youth Serv. Rev. 2021, 126, 106008. [Google Scholar] [CrossRef]
- Chiva-Bartoll, O.; Ruiz-Montero, P.J.; Olivencia, J.J.L.; Grönlund, H. The effects of service-learning on physical education teacher education: A case study on the border between Africa and Europe. Eur. Phys. Educ. Rev. 2021. [Google Scholar] [CrossRef]
- Daum, D.N.; Marttinen, R.; Banville, D. Service-learning experiences for pre-service teachers: Cultural competency and behavior management challenges when working with a diverse low-income community. Phys. Educ. Sport Pedagog. 2021. [Google Scholar] [CrossRef]
- García-Rico, L.; Martínez-Muñoz, L.F.; Santos-Pastor, M.L.; Chiva-Bartoll, O. Service-learning in physical education teacher education: A pedagogical model towards sustainable development goals. Int. J. Sustain. High. Educ. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Acronym | Test | Afferent Input |
|---|---|---|
| EO_QS | Feet on platform, eyes open | Visual, somatosensory, vestibular |
| EC_QS | Feet on platform, eyes closed | Somatosensory, vestibular |
| EO_FS | Feet on foam, eyes open | Visual, vestibular, modified somatosensory |
| EC_FS | Feet on foam, eyes closed | Vestibular, modified somatosensory |
| ASDE | ASDC | Group × Time Effect | |||
|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||
| (M ± SD) | (M ± SD) | (M ± SD) | (M ± SD) | p-Value | |
| Somatosensorial | 1.41 ± 0.63 | 2.06 ± 2.38 | 1.08 ± 0.56 | 1.17 ± 0.43 | p = 0.204 |
| Visual | 2.07 ± 0.79 | 2.79 ± 1.54 | 1.93 ± 0.75 | 1.95 ± 0.89 | p = 0.115 |
| Vestibular | 3.68 ± 2.37 | 4.96 ± 2.76 ** | 5.09 ± 5.01 | 5.15 ± 4.68 | p = 0.016 |
| ASDE | ASDC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||||||
| Stability Quotient | Gra/s (M ± SD) | Gra/s (M ± SD) | IC95% | p-Value | Cohen’s d | Gra/s (M ± SD) | Gra/s (M ± SD) | IC95% | p-Value | Cohen’s d |
| EO_QS | 0.85 ± 0.45 | 0.76 ± 0.40 | −0.152, 0.309 | 0.398 | 0.20 | 0.94 ± 0.88 | 1.18 ± 1.65 | −0.951, 0.476 | 0.457 | −0.12 |
| EC_QS | 3.12 ± 7.76 | 1.64 ± 2.66 | −3.303, 5.989 | 0.493 | 0.19 | 0.71 ± 0.24 | 1.16 ± 1.44 | −1.484, 0.584 | 0.338 | −0.15 |
| EO_FS | 1.54 ± 0.71 | 1.76 ± 1.00 | −0.785, 0.343 | 0.205 | −0.23 | 1.39 ± 0.67 | 1.39 ± 0.76 | −0.245, 0.245 | 1.000 | −0.26 |
| EC_FS | 2.54 ± 1.22 | 2.99 ± 1.05 | −0.938, 0.532 | 0.488 | −0.52 | 2.73 ± 1.06 | 2.88 ± 1.45 | −1.145, 0.845 | 0.732 | −0.22 |
| ASDE | ASDC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age Group | Pre | Post | IC95% | d | p-Value | Pre | Post | IC95% | d | p-Value |
| Stability Quotient | º/s (M ± SD) | º/s (M ± SD) | º/s (M ± SD) | º/s (M ± SD) | ||||||
| EO_RL | 9.69 ± 2.84 | 9.66 ± 3.48 | −1.257, 1.324 | −0.009 | 0.957 | 8.2 ± 4.7 | 9.5 ± 3.8 | −4.942, 2.292 | 0.304 | 0.415 |
| EO_LL | 11.76 ± 0.91 | 11.50 ± 1.27 | −0.266, 0.780 | −0.235 | 0.308 | 10.7 ± 3.7 | 12.0 ± 0.0 | −4.374, 1.774 | 0.50 | 0.351 |
| EC_RL | 8.98 ± 3.70 | 8.04 ± 3.89 | −0.728, 2.599 | −0.248 | 0.246 | 9.2 ± 3.6 | 9.4 ± 3.0 | −4.469, 3.969 | 0.060 | 0.893 |
| EC_LL | 11.28 ± 1.43 | 11.74 ± 0.96 | −1.526, 0.597 | 0.186 | 0.362 | 12.0 ± 0.0 | 12.0 ± 0.0 | 0, 0 | 0 | 1.000 |
| Reaction Time (s) | LOS (%) | MV (º/s) | DCL (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre (Range) | Post (Range) | F, p-Value | Pre (Range) | Post (Range) | F, p-Value | Pre (Range) | Post (Range) | F, p-Value | Pre (Range) | Post (Range) | F, p-Value | ||
| Forward | E C | 0.80 (0.70–1.12) 1.17 (1.01–1.35) | 0.90 (0.31–1.19) 0.95 (0.41–1.18) | F = 0.99 p = 0.40 | 64.00 (36.00–88.00) 78.00 (48.00– 89.00) | 78.00 (55.00–85.00) 72.00 (31.00–98.00) | F = 0.94 p = 0.43 | 4.00 (1.40–8.50) 3.50 (2.30–5.60) | 3.50 (3.10–7.00) 4.90 (2.20–6.10) | F = 2.28 p = 0.09 | 67.00 (65.00–81.00) 80.00 (34.00–86.00) | 73.00 (49.00–83.00) 63.00 (47.00–83.00) | F = 2.30 p = 0.09 |
| Right Forward | E C | 0.70 (0.58–1.22) 0.99 (0.39–1.20) | 0.68 (0.62–1.38) 1.1 (0.53–1.24) | F = 0.69 p = 0.56 | 73.00 (46.00–95.00) 84.00 (60.00–111.00) | 63.00 (55.00–95.00) 85.00 (75.00–89.00) | F = 1.90 p = 0.14 | 4.90 (3.10–9.30) 6.20 (4.10–7.80) | 5.10 (3.15–7.65) 5.10 (4.50–6.10) | F = 0.62 p = 0.60 | 43.00 (18.00–65.00) 54.00 (28.00–74.00) | 40.00 (5.00–64.00) 60.00 (48.00–64.00) | F = 4.35 p = 0.10 |
| Right | E C | 0.79 (0.70–1.03) 0.79 (0.55–1.19) | 0.81 (0.66–1.17) 0.75 (0.56–0.83) | F = 1.72 p = 0.18 | 79.50 (57.25–87.25) 88.00 (62.00–97.00) | 78.00 (72.00–87.00) 72.00 (55.00–85.00) | F = 2.71 p = 0.05 | 5.35 (2.40–7.18) 6.40 (5.20–7.40) | 6.40 (5.10–10.10) 6.80 (6.60–7.40) | F = 2.38 p = 0.08 | 70.50 (48.00–77.75) 77.00 (70.00–82.00) * | 73.00 (54.00–81.00) 72.00 (58.00–74.00) * | F = 3.03 p = 0.04 |
| Right Backward | E C | 0.95 (0.35–1.02) 0.56 (0.35–1.27) | 0.81 (0.49–0.98) 0.85 (0.72–0.98) | F = 1.03 p = 0.39 | 67.00 (48.00–88.00) 54.00 (49.00–75.00) | 86.00 (51.00–101.00) 73.00 (54.00–90.00) | F = 0.95 p = 0.42 | 4.80 (2.30–5.50) 3.5 (3.10–6.20) | 4.30 (3.30–6.50) 3.70 (3.40–6.00) | F = 0.57 p = 0.64 | 50.00 (17.00–79.00) 31.00 (5.00–61.00) | 29.00 (10.00–62.00) 42.00 (0–56.00) | F = 0.11 p = 0.95 |
| Backward | E C | 0.71 (0.35–1.07) 0.87 (0.57–1.02) | 0.75 (0.62–1.04) 0.81 (0.76–1.09) | F = 1.26 p = 0.30 | 63.50 (57.00–75.00) * 64.00 (54.00–94.00) | 70.00 (56.00–92.00) * 65.00 (59.00–85.00) | F = 0.30 p = 0.82 | 2.10 (1.63–3.73) * 2.8 (2.20–3.10) | 3.70 (2.80–4.70) * 3.30 (2.90–4.20) | F = 0.50 p = 0.69 | 56.00 (31.50–69.75) 57.00 (14.00–70.00) | 60.00 (37.00–66.00) 58.00 (47.00–70.00) | F = 0.29 p = 0.83 |
| Left Backward | E C | 1.03 (0.70–1.62) 0.72 (0.50–1.42) | 0.86 (0.48–1.10) 0.82 (0.60–1.22) | F = 2.05 p = 0.12 | 67.00 (37.50–89.50) 88.00 (59.00–92.00) | 79.00 (64.00–99.00) 60.00 (57.00–65.00) | F = 4.38 p = 0.01 | 4.25 (2.68–4.80) 6.10 (4.80–6.90) | 4.90 (3.40–6.70) 4.30 (2.90–5.80) | F = 0.25 p = 0.86 | 27.50 (14.50–58.00) 52.00 (33.00–59.00) | 36.00 (7.00–56.00) 42.00 (31.00–57.00) | F = 0.89 p = 0.46 |
| Left | E C | 0.92 (0.73–1.08) 0.59 (0.55–0.81) | 1.20 (0.65–1.73) 0.82 (0.60–1.22) | F = 1.02 p = 0.39 | 73.50 (51.00–86.00) 84.00 (73.00–88.00) | 84.00 (71.00–86.75) 66.00 (58.00–88.00) | F = 2.55 p = 0.07 | 5.38 (2.60–8.03) 7.30 (6.20–9.00) | 6.25 (3.75–9.68) 5.60 (5.00–6.70) | F = 2.53 p = 0.07 | 63.00 (48.25–73.75) 73.00 (71.00–87.00) * | 70.00 (54.25–81.75) 63.00 (53.00–81.00) * | F = 2.94 p = 0.04 |
| Left Forward | E C | 0.96 (0.61–1.39) 0.98 (0.59–1.33) | 0.85 (0.62–1.57) 0.73 (0.68–1.07) | F = 2.51 p = 0.07 | 58.00 (45.50–91.50) 76.00 (64.00–83.00) | 71.5 (61.00–78.75) 81.00 (53.00–99.00) | F = 1.46 p = 0.24 | 5.10 (2.18–7.68) 6.10 (5.60–7.30) | 3.80 (2.70–8.13) 7.90 (5.70–10.30) | F = 1.70 p = 0.18 | 58.00 (32.00–65.25) 62.00 (51.00–78.00) | 48.5 (22.00–79.00) 74.00 (54.00–86.00) | F = 2.64 p = 0.06 |
| ASDE | ASDC | |||||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||
| (M ± SD) | (M ± SD) | d | (M ± SD) | (M ± SD) | d | |
| CoP_EO_QS_ML | 0.00 ± 0.86 | 0.10 ± 0.59 | −0.07 | 0.34 ± 0.98 | −0.30 ± 0.51 | −0.27 |
| CoP_EC_QS_ML | 0.14 ± 0.97 | −0.29 ± 0.68 | 0.06 | 0.12 ± 0.97 | −0.99 ± 0.25 | −0.36 |
| CoP_EO_FS_ML | 0.80 ± 0.67 | 0.55 ± 0.97 | 0.52 | −0.11 ± 0.47 | −0.23 ± 0.19 | 0 |
| CoP_EC_FS_ML | 0.43 ± 0.80 | 0.04 ± 0.99 | 0.26 | −0.24 ± 0.38 | 0.10 ± 0.73 | 0 |
| CoP_EO_QS_AP | −0.48 ± 0.89 | −0.53 ± 0.93 | 0.40 | −0.80 ± 1.13 | −0.69 ± 2.80 | −0.14 |
| CoP_EC_QS_AP | −0.40 ± 0.67 | −0.61 ± 0.78 | 0.64 | −0.80 ± 0.99 | −0.79 ± 0.18 | −0.02 |
| CoP_EO_FS_AP | 0.63 ± 0.80 * | 0.21 ± 0.99 * | 0.38 | 0.99 ± 1.17 | 0.43 ± 0.42 | −0.23 |
| CoP_EC_FS_AP | 0.38 ± 1.32 | 0.92 ± 1.20 | −0.21 | 0.84 ± 0.99 | 0.90 ± 1.40 | −0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valverde-Esteve, T.; Salvador-Garcia, C.; Gil-Gómez, J.; Maravé-Vivas, M. Sustainable Service-Learning in Physical Education Teacher Education: Examining Postural Control to Promote ASD Children’s Well-Being. Int. J. Environ. Res. Public Health 2021, 18, 5216. https://doi.org/10.3390/ijerph18105216
Valverde-Esteve T, Salvador-Garcia C, Gil-Gómez J, Maravé-Vivas M. Sustainable Service-Learning in Physical Education Teacher Education: Examining Postural Control to Promote ASD Children’s Well-Being. International Journal of Environmental Research and Public Health. 2021; 18(10):5216. https://doi.org/10.3390/ijerph18105216
Chicago/Turabian StyleValverde-Esteve, Teresa, Celina Salvador-Garcia, Jesús Gil-Gómez, and María Maravé-Vivas. 2021. "Sustainable Service-Learning in Physical Education Teacher Education: Examining Postural Control to Promote ASD Children’s Well-Being" International Journal of Environmental Research and Public Health 18, no. 10: 5216. https://doi.org/10.3390/ijerph18105216