
The Impact of Post-COVID-19 Syndrome on Self-Reported Physical Activity

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
3.1. Demographics and Characteristics
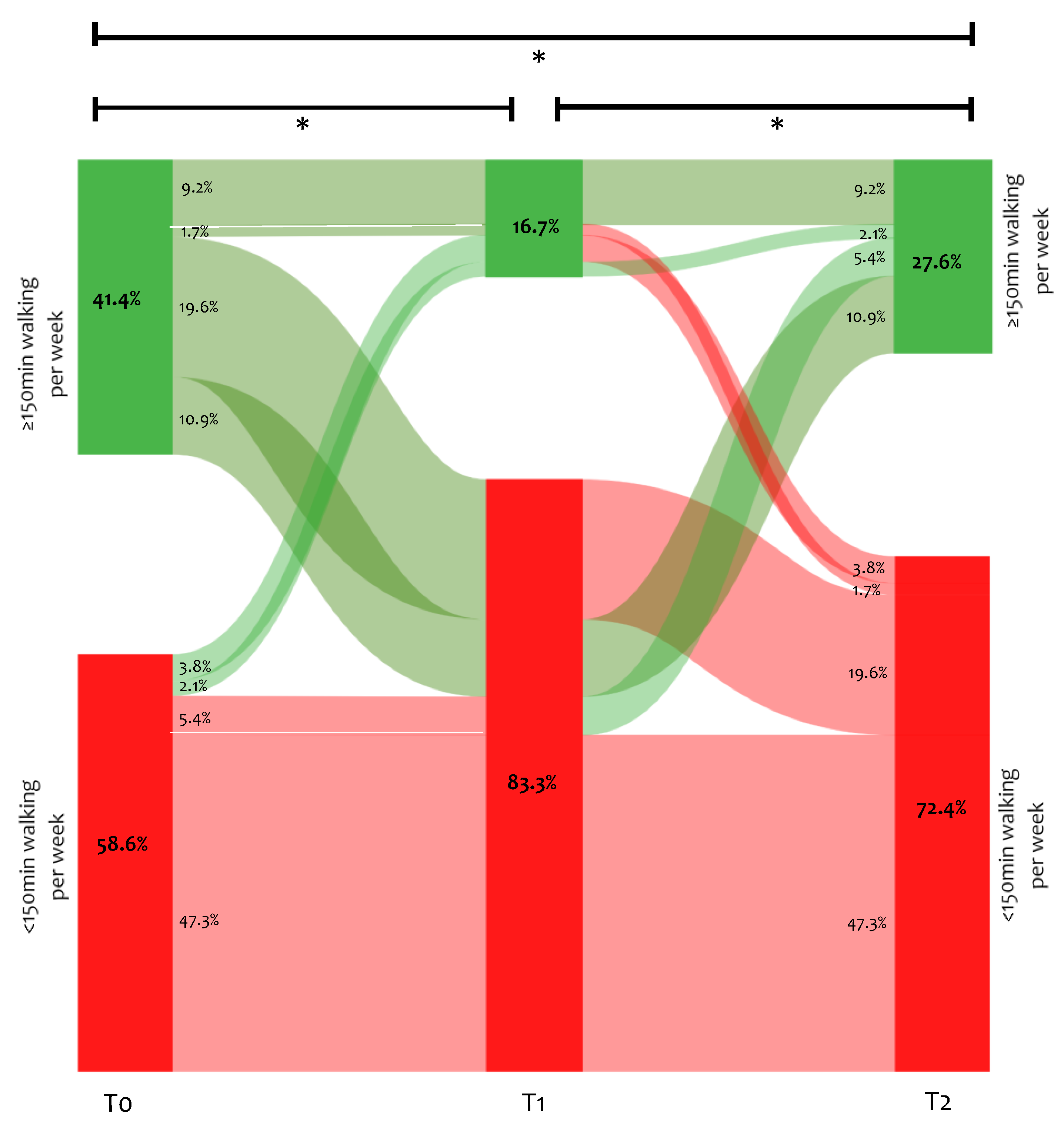
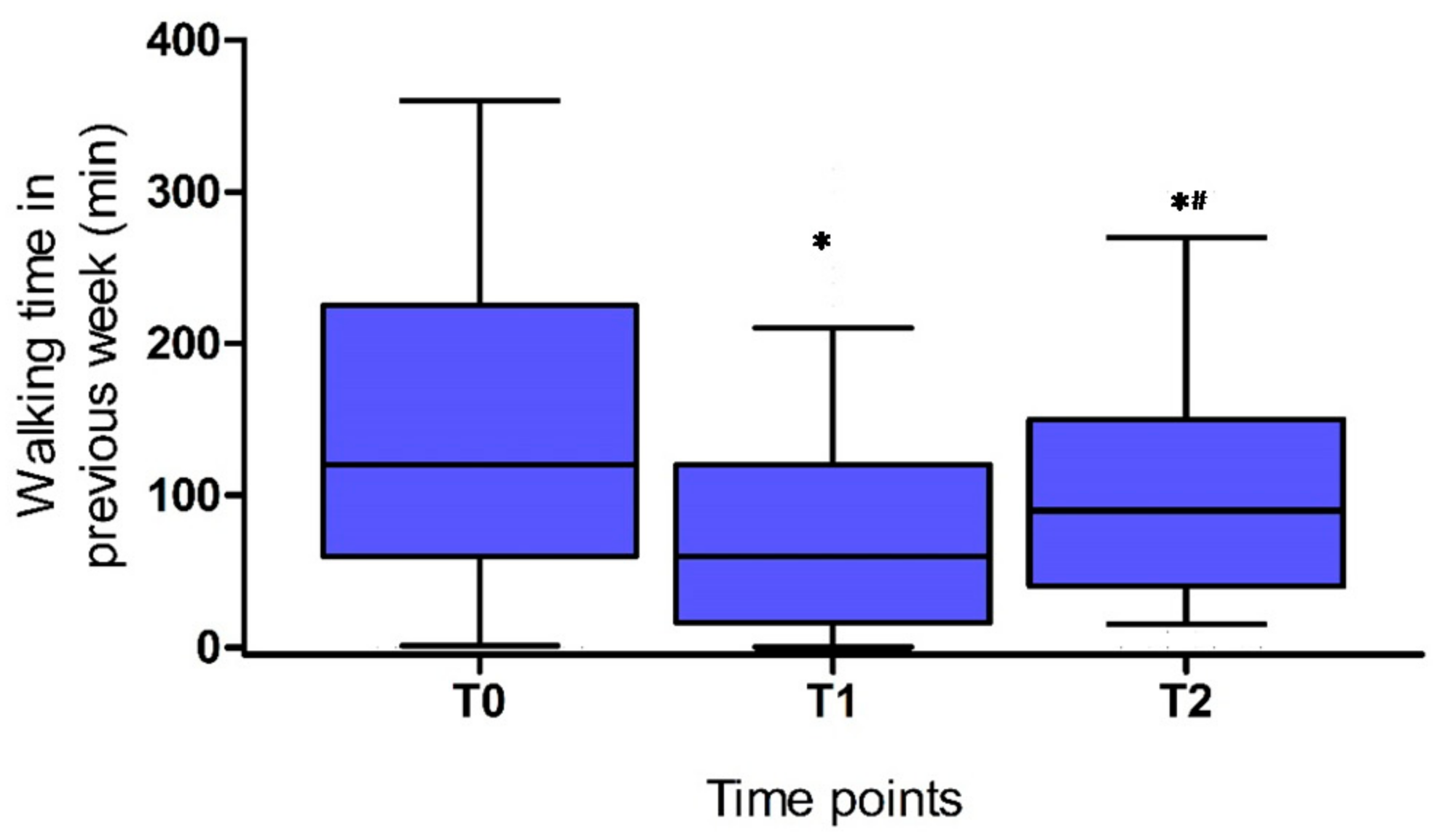
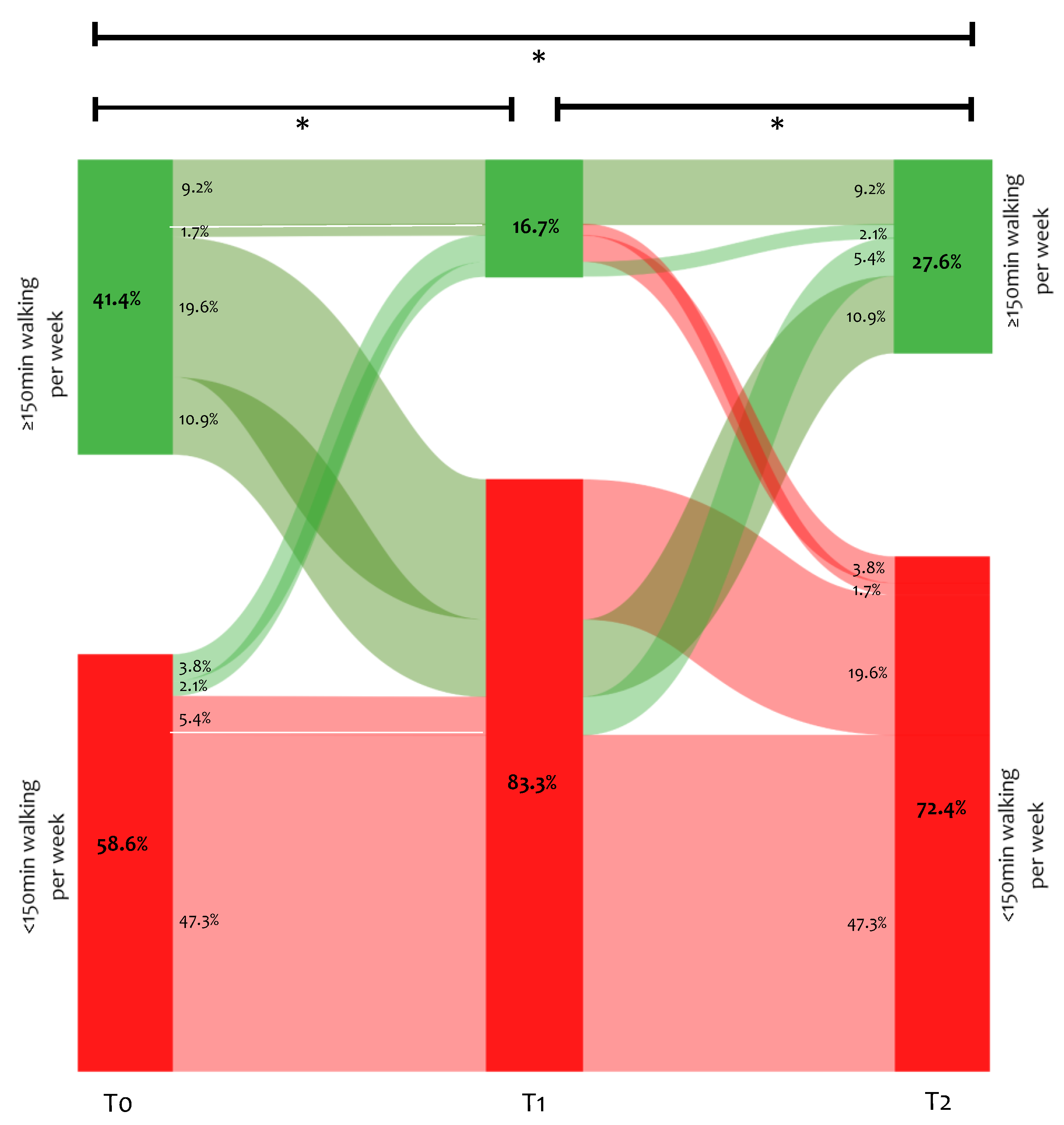
3.2. Self-Reported Walking Time
3.3. Activities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Dal Negro, F.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Goërtz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Van den Borst, B.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.H.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive health assessment three months after recovery from acute COVID-19. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, ciaa1750. [Google Scholar] [CrossRef]
- Wong, A.W.; Shah, A.S.; Johnston, J.C.; Carlsten, C.; Ryerson, C.J. Patient-reported outcome measures after COVID-19: A prospective cohort study. Eur. Respir. J. 2020, 56, 2003276. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of Long-COVID: Analysis of COVID cases and their symptoms collected by the Covid Symptoms Study App. medRxiv 2020. [Google Scholar] [CrossRef]
- D’Cruz, R.F.; Waller, M.D.; Perrin, F.; Periselneris, J.; Norton, S.; Smith, L.J.; Patrick, T.; Walder, D.; Heitmann, A.; Lee, K.; et al. Chest radiography is a poor predictor of respiratory symptoms and functional impairment in survivors of severe COVID-19 pneumonia. ERJ Open Res. 2021, 7. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5-6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2020, 76, 405–407. [Google Scholar] [CrossRef]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.Á.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands—A longitudinal study among non-hospitalized patients. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, ciaa1792. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. COVID-19 Guideline: Management of the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/gid-ng10179/documents/final-scope (accessed on 4 June 2020).
- Collins, F.S. NIH Launches New Initiative to Study “Long COVID”; National Institutes of Health: Bethesda, MD, USA, 2021. Available online: https://www.nih.gov/about-nih/who-we-are/nih-director/statements/nih-launches-new-initiative-study-long-covid (accessed on 4 June 2020).
- Humphreys, H.; Kilby, L.; Kudiersky, N.; Copeland, R. Long COVID and the role of physical activity: A qualitative study. BMJ Open 2021, 11, e047632. [Google Scholar] [CrossRef]
- Nederland, R. Aangescherpte Maatregelen om Het Coronavirus Onder Controle te Krijgen. 2020. Available online: https://www.rijksoverheid.nl/onderwerpen/coronavirus-tijdlijn/nieuws/2020/03/23/aangescherpte-maatregelen-om-het-coronavirus-onder-controle-te-krijgen (accessed on 26 May 2021).
- Federale Overheidsdienst Volksgezondheid, Veiligheid van de Voedselketen en Leefmilieu. Coronavirus: Fase 2 Gehandhaafd, Overgang naar de Federale Fase en Bijkomende Maatregelen. 2020. Available online: https://www.info-coronavirus.be/nl/news/fase-2-gehandhaafd-overgang-naar-de-federale-fase-en-bijkomende-maatregelen/ (accessed on 26 May 2021).
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Narici, M.; Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Public Facebook Group: Corona Ervaringen en Langdurige Klachten (Nederland). 2020. Available online: https://www.facebook.com/groups/236723204035929/ (accessed on 4 June 2020).
- Public Facebook Group: Corona Patiënten met Langdurige Klachten (Vlaanderen). 2020. Available online: https://www.facebook.com/groups/241043323639334/ (accessed on 4 June 2020).
- Vaes, A.W.; Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Goertz, Y.M.J.; Van Herck, M.; Houben-Wilke, S.; Franssen, F.M.E.; Vijlbrief, H.; Spies, Y.; et al. Care Dependency in Non-Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 2946. [Google Scholar] [CrossRef]
- Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Vaes, A.W.; Goërtz, Y.M.J.; van Herck, M.; Houben-Wilke, S.; Boon, G.; Barco, S.; Burtin, C.; et al. Construct validity of the Post-COVID-19 Functional Status Scale in adult subjects with COVID-19. Health Qual. Life Outcomes 2021, 19, 40. [Google Scholar] [CrossRef]
- Meys, R.; Delbressine, J.M.; Goërtz, Y.M.J.; Vaes, A.W.; Machado, F.V.C.; Van Herck, M.; Burtin, C.; Posthuma, R.; Spaetgens, B.; Franssen, F.M.E.; et al. Generic and Respiratory-Specific Quality of Life in Non-Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 3993. [Google Scholar] [CrossRef]
- Houben-Wilke, S.; Delbressine, J.M.; Vaes, A.W.; Goërtz, Y.M.J.; Meys, R.; Machado, F.V.C.; Van Herck, M.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Understanding and Being Understood: Information and Care Needs of 2113 Patients with Confirmed or Suspected COVID-19. J. Patient Exp. 2021, 8, 2374373521997222. [Google Scholar] [CrossRef]
- Vaes, A.W.; Goërtz, Y.M.J.; Van Herck, M.; Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Houben-Wilke, S.; Gaffron, S.; Maier, D.; Burtin, C.; et al. Recovery from COVID-19: A sprint or marathon? 6 months follow-up data of online long COVID-19 support group members. ERJ Open Res. 2021, 7. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wu, J.; Hao, S.; Yang, M.; Lu, X.; Chen, X.; Li, L. Long term outcomes in survivors of epidemic Influenza A (H7N9) virus infection. Sci. Rep. 2017, 7, 17275. [Google Scholar] [CrossRef] [PubMed]
- Herridge, M.S. Recovery and long-term outcome in acute respiratory distress syndrome. Crit. Care Clin. 2011, 27, 685–704. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, R.O.; Weaver, L.K.; Collingridge, D.; Parkinson, R.B.; Chan, K.J.; Orme, J.F., Jr. Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2005, 171, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Ngai, J.C.; Ko, F.W.; Ng, S.S.; To, K.W.; Tong, M.; Hui, D.S. The long-term impact of severe acute respiratory syndrome on pulmonary function, exercise capacity and health status. Respirology 2010, 15, 543–550. [Google Scholar] [CrossRef] [Green Version]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Long, B.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Cardiovascular complications in COVID-19. Am. J. Emerg. Med. 2020, 38, 1504–1507. [Google Scholar] [CrossRef]
- Gandotra, S.; Lovato, J.; Case, D.; Bakhru, R.N.; Gibbs, K.; Berry, M.; Files, D.C.; Morris, P.E. Physical Function Trajectories in Survivors of Acute Respiratory Failure. Ann. Am. Thorac. Soc. 2019, 16, 471–477. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021. [Google Scholar] [CrossRef]
- Spruit, M.A.; Holland, A.E.; Singh, S.J.; Tonia, T.; Wilson, K.C.; Troosters, T. COVID-19: Interim Guidance on Rehabilitation in the Hospital and Post-Hospital Phase from a European Respiratory Society and American Thoracic Society-coordinated International Task Force. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Salman, D.; Vishnubala, D.; Le Feuvre, P.; Beaney, T.; Korgaonkar, J.; Majeed, A.; McGregor, A.H. Returning to physical activity after covid-19. BMJ 2021, 372, m4721. [Google Scholar] [CrossRef]
- Ladds, E.; Rushforth, A.; Wieringa, S.; Taylor, S.; Rayner, C.; Husain, L.; Greenhalgh, T. Persistent symptoms after Covid-19: Qualitative study of 114 “long Covid” patients and draft quality principles for services. BMC Health Serv. Res. 2020, 20, 1144. [Google Scholar] [CrossRef]
- Assaf, G.; Davis, H.; McCorkell, L.; Wei, H.; Brooke, O.; Akrami, A.; Low, R.; Mercier, J.; Adetutu, A. An Analysis of the Prolonged COVID-19 Symptoms Survey by Patient-Led Research Team. 2020. Available online: https://patientresearchcovid19.com/research/report-1/ (accessed on 15 November 2020).
- Davido, B.; Seang, S.; Tubiana, R.; de Truchis, P. Post-COVID-19 chronic symptoms: A postinfectious entity? Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 1448–1449. [Google Scholar] [CrossRef]
- Dyrstad, S.M.; Hansen, B.H.; Holme, I.M.; Anderssen, S.A. Comparison of self-reported versus accelerometer-measured physical activity. Med. Sci. Sports Exerc. 2014, 46, 99–106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| All Participants (n = 239) | |
|---|---|
| Hospitalized due to COVID-19, n (%) | 62 (25.9) |
| Women, n (%) | 198 (82.8) |
| Age, years, median (IQR) | 50.0 (39.0–56.0) |
| Body mass index (BMI), kg/m2, median (IQR) | 26.0 (23.4–30.5) |
| Marital status—married/living with partner, n (%) | 173 (72.4) |
| Education level, n (%) | |
| Low | 6 (2.5) |
| Medium | 126 (52.7) |
| High | 107 (44.8) |
| Self-reported pre-existing comorbidities, n (%) | |
| None | 142 (59.4) |
| 1 comorbidity | 62 (25.9) |
| ≥2 comorbidities | 35 (14.6) |
| Received care | |
| No care needed, % | |
| Between infection and 3 months of follow-up | 14.6 |
| Between 3 and 6 months of follow-up | 14.2 |
| Physiotherapy, % | |
| Between infection and 3 months of follow-up | 31.8 |
| Between 3 and 6 months of follow-up | 61.9 # |
| Rehabilitation, % | |
| Between infection and 3 months of follow-up | 4.2 |
| Between 3 and 6 months of follow-up | 11.7 # |
| Sport/Activity, n (%) | All Participants (n = 239) | |||
|---|---|---|---|---|
| T0 | T1 | T2 | ||
| 1 | Walking | 127(53.1) | 99(41.1) * | 163(68.2) *# |
| 2 | Cycling outdoors | 84(35.1) | 51(21.3) * | 101(42.3) # |
| 3 | (Physio)fitness/exercise groups | 72(30.1) | 24(10.0) * | 92(38.5) # |
| 4 | Swimming | 24(10.0) | 9(3.8) * | 14(5.9) * |
| 5 | Running | 24(10.0) | 7(2.9) * | 28(11.7) # |
| 6 | Yoga/Pilates | 12(5.0) | 0(0.0) * | 7(2.9) |
| 7 | Racket sports | 10(4.2) | 1(1.3) * | 4(1.7) * |
| 8 | Team sports | 8(3.3) | 0(0.0) * | 2(0.8) |
| 9 | Martial arts | 5(2.1) | 1(0.4) | 0(0.0) * |
| Cycling indoors | 5(2.1) | 10(4.2) | 28(11.7) *# | |
| Work-related activities | 5(2.1) | 0(0.0) * | 0(0.0) * | |
| 10 | Dancing | 4(1.7) | 0(0.0) * | 0(0.0) * |
| No sports/activities, regardless of COVID-19 | 27(11.3) | 9(3.8) * | 5(2.1) * | |
| No sports/activities, due to COVID-19 | N.A. | 104(43.5) | 28(11.7) # | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delbressine, J.M.; Machado, F.V.C.; Goërtz, Y.M.J.; Van Herck, M.; Meys, R.; Houben-Wilke, S.; Burtin, C.; Franssen, F.M.E.; Spies, Y.; Vijlbrief, H.; et al. The Impact of Post-COVID-19 Syndrome on Self-Reported Physical Activity. Int. J. Environ. Res. Public Health 2021, 18, 6017. https://doi.org/10.3390/ijerph18116017
Delbressine JM, Machado FVC, Goërtz YMJ, Van Herck M, Meys R, Houben-Wilke S, Burtin C, Franssen FME, Spies Y, Vijlbrief H, et al. The Impact of Post-COVID-19 Syndrome on Self-Reported Physical Activity. International Journal of Environmental Research and Public Health. 2021; 18(11):6017. https://doi.org/10.3390/ijerph18116017
Chicago/Turabian StyleDelbressine, Jeannet M., Felipe V. C. Machado, Yvonne M. J. Goërtz, Maarten Van Herck, Roy Meys, Sarah Houben-Wilke, Chris Burtin, Frits M. E. Franssen, Yvonne Spies, Herman Vijlbrief, and et al. 2021. "The Impact of Post-COVID-19 Syndrome on Self-Reported Physical Activity" International Journal of Environmental Research and Public Health 18, no. 11: 6017. https://doi.org/10.3390/ijerph18116017