
Instability Severity Index Score Does Not Predict the Risk of Shoulder Dislocation after a First Episode Treated Conservatively

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
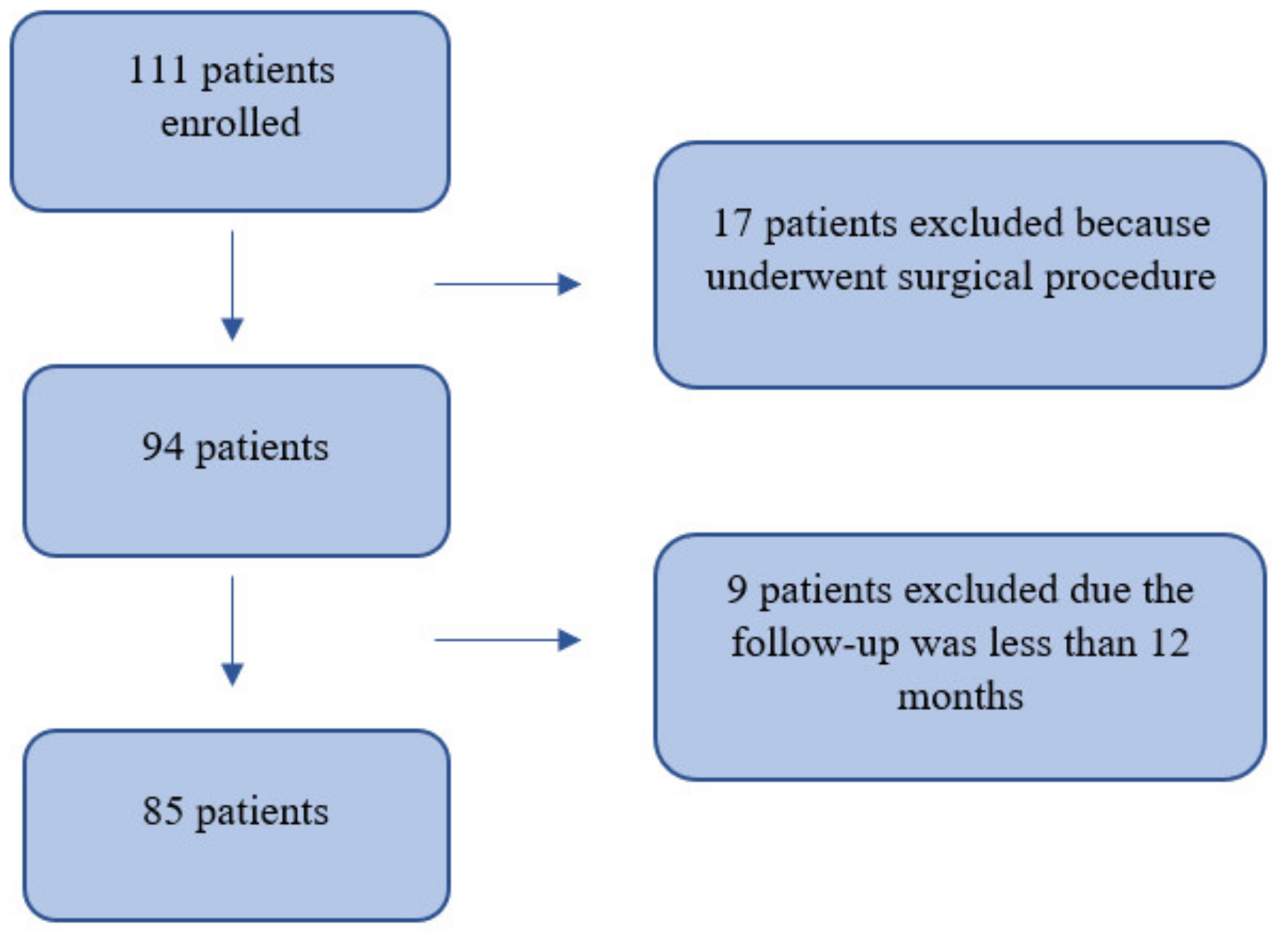
2.1. Participants and Setting
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Predictivity of ISIS for RSD
4.2. Risk Factors of RSD after a First Episode Treated Conservatively
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, R.; Akbarnia, H. Shoulder Dislocations Overview. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Johnson, D.J.; Tadi, P. Multidirectional Shoulder Instability. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Hindle, P.; Davidson, E.K.; Biant, L.C.; Court-Brown, C.M. Appendicular Joint Dislocations. Injury 2013, 44, 1022–1027. [Google Scholar] [CrossRef]
- Owens, B.D.; Agel, J.; Mountcastle, S.B.; Cameron, K.L.; Nelson, B.J. Incidence of Glenohumeral Instability in Collegiate Athletics. Am. J. Sports Med. 2009, 37, 1750–1754. [Google Scholar] [CrossRef] [PubMed]
- Zacchilli, M.A.; Owens, B.D. Epidemiology of Shoulder Dislocations Presenting to Emergency Departments in the United States. J. Bone Jt. Surg. Am. 2010, 92, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Goss, T.P. Anterior Glenohumeral Instability. Orthopedics 1988, 11, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Ciuffreda, M.; Maffulli, N.; Denaro, V. Management of Primary Acute Anterior Shoulder Dislocation: Systematic Review and Quantitative Synthesis of the Literature. Arthroscopy 2014, 30, 506–522. [Google Scholar] [CrossRef] [PubMed]
- Te Slaa, R.L.; Wijffels, M.P.J.M.; Brand, R.; Marti, R.K. The Prognosis Following Acute Primary Glenohumeral Dislocation. J. Bone Jt. Surg. Br. 2004, 86, 58–64. [Google Scholar] [CrossRef]
- Murray, I.R.; Ahmed, I.; White, N.J.; Robinson, C.M. Traumatic Anterior Shoulder Instability in the Athlete. Scand. J. Med. Sci Sports 2013, 23, 387–405. [Google Scholar] [CrossRef] [PubMed]
- Postacchini, F.; Gumina, S.; Cinotti, G. Anterior Shoulder Dislocation in Adolescents. J. Shoulder Elb. Surg. 2000, 9, 470–474. [Google Scholar] [CrossRef]
- Robinson, C.M.; Dobson, R.J. Anterior Instability of the Shoulder after Trauma. J. Bone Jt. Surg. Br. 2004, 86, 469–479. [Google Scholar] [CrossRef]
- Sachs, R.A.; Lin, D.; Stone, M.L.; Paxton, E.; Kuney, M. Can the Need for Future Surgery for Acute Traumatic Anterior Shoulder Dislocation Be Predicted? J. Bone Jt. Surg. Am. 2007, 89, 1665–1674. [Google Scholar] [CrossRef]
- Hovelius, L.; Olofsson, A.; Sandström, B.; Augustini, B.-G.; Krantz, L.; Fredin, H.; Tillander, B.; Skoglund, U.; Salomonsson, B.; Nowak, J.; et al. Nonoperative Treatment of Primary Anterior Shoulder Dislocation in Patients Forty Years of Age and Younger. a Prospective Twenty-Five-Year Follow-Up. J. Bone Jt. Surg. Am. 2008, 90, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.L.; Kuhn, J.E. Operative versus Nonoperative Treatment of Acute Shoulder Dislocation in the Athlete. Curr. Sports Med. Rep. 2008, 7, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Chahal, J.; Leiter, J.; McKee, M.D.; Whelan, D.B. Generalized Ligamentous Laxity as a Predisposing Factor for Primary Traumatic Anterior Shoulder Dislocation. J. Shoulder Elb. Surg. 2010, 19, 1238–1242. [Google Scholar] [CrossRef]
- Hovelius, L.; Augustini, B.G.; Fredin, H.; Johansson, O.; Norlin, R.; Thorling, J. Primary Anterior Dislocation of the Shoulder in Young Patients. A Ten-Year Prospective Study. J. Bone Jt. Surg. Am. 1996, 78, 1677–1684. [Google Scholar] [CrossRef] [PubMed]
- Balg, F.; Boileau, P. The Instability Severity Index Score. A Simple Pre-Operative Score to Select Patients for Arthroscopic or Open Shoulder Stabilisation. J. Bone Jt. Surg. Br. 2007, 89, 1470–1477. [Google Scholar] [CrossRef] [Green Version]
- Gao, B.; Gao, W.; Chen, C.; Wang, Q.; Lin, S.; Xu, C.; Huang, D.; Su, P. What Is the Difference in Morphologic Features of the Thoracic Pedicle Between Patients with Adolescent Idiopathic Scoliosis and Healthy Subjects? A CT-Based Case-Control Study. Clin. Orthop. Relat. Res. 2017, 475, 2765–2774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobby, J.; Griffin, D.; Dunbar, M.; Boileau, P. Is Arthroscopic Surgery for Stabilisation of Chronic Shoulder Instability as Effective as Open Surgery? A Systematic Review and Meta-Analysis of 62 Studies Including 3044 Arthroscopic Operations. J. Bone Jt. Surg. Br. 2007, 89, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Itoi, E.; Hatakeyama, Y.; Sato, T.; Kido, T.; Minagawa, H.; Yamamoto, N.; Wakabayashi, I.; Nozaka, K. Immobilization in External Rotation after Shoulder Dislocation Reduces the Risk of Recurrence. A Randomized Controlled Trial. J. Bone Jt. Surg. Am. 2007, 89, 2124–2131. [Google Scholar] [CrossRef]
- ESSKA. 360° around Shoulder Instability; Brzóska, R., Milano, G., Randelli, P.S., Kovačič, L., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; ISBN 978-3-662-61073-2. [Google Scholar]
- Ellman, H.; Hanker, G.; Bayer, M. Repair of the Rotator Cuff. End-Result Study of Factors Influencing Reconstruction. J. Bone Jt. Surg. Am. 1986, 68, 1136–1144. [Google Scholar] [CrossRef]
- Roy, J.-S.; Macdermid, J.C.; Faber, K.J.; Drosdowech, D.S.; Athwal, G.S. The Simple Shoulder Test Is Responsive in Assessing Change Following Shoulder Arthroplasty. J. Orthop. Sports Phys. Ther. 2010, 40, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Roach, K.E.; Budiman-Mak, E.; Songsiridej, N.; Lertratanakul, Y. Development of a Shoulder Pain and Disability Index. Arthritis Care Res. 1991, 4, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Phadnis, J.; Arnold, C.; Elmorsy, A.; Flannery, M. Utility of the Instability Severity Index Score in Predicting Failure after Arthroscopic Anterior Stabilization of the Shoulder. Am. J. Sports Med. 2015, 43, 1983–1988. [Google Scholar] [CrossRef] [PubMed]
- Bottoni, C.R.; Wilckens, J.H.; DeBerardino, T.M.; D’Alleyrand, J.-C.G.; Rooney, R.C.; Harpstrite, J.K.; Arciero, R.A. A Prospective, Randomized Evaluation of Arthroscopic Stabilization versus Nonoperative Treatment in Patients with Acute, Traumatic, First-Time Shoulder Dislocations. Am. J. Sports Med. 2002, 30, 576–580. [Google Scholar] [CrossRef]
- Southgate, D.F.L.; Bokor, D.J.; Longo, U.G.; Wallace, A.L.; Bull, A.M.J. The Effect of Humeral Avulsion of the Glenohumeral Ligaments and Humeral Repair Site on Joint Laxity: A Biomechanical Study. Arthroscopy 2013, 29, 990–997. [Google Scholar] [CrossRef]
- Wheeler, J.H.; Ryan, J.B.; Arciero, R.A.; Molinari, R.N. Arthroscopic versus Nonoperative Treatment of Acute Shoulder Dislocations in Young Athletes. Arthroscopy 1989, 5, 213–217. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Loppini, M.; Locher, J.; Buchmann, S.; Maffulli, N.; Denaro, V. Multidirectional Instability of the Shoulder: A Systematic Review. Arthroscopy 2015, 31, 2431–2443. [Google Scholar] [CrossRef] [PubMed]
- Locher, J.; Wilken, F.; Beitzel, K.; Buchmann, S.; Longo, U.G.; Denaro, V.; Imhoff, A.B. Hill-Sachs Off-Track Lesions as Risk Factor for Recurrence of Instability after Arthroscopic Bankart Repair. Arthroscopy 2016, 32, 1993–1999. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Romeo, G.; Huijsmans, P.E.; Denaro, V. Glenoid and Humeral Head Bone Loss in Traumatic Anterior Glenohumeral Instability: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 392–414. [Google Scholar] [CrossRef]
- Olds, M.; Ellis, R.; Donaldson, K.; Parmar, P.; Kersten, P. Risk Factors Which Predispose First-Time Traumatic Anterior Shoulder Dislocations to Recurrent Instability in Adults: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2015, 49, 913–922. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, B.W.; Johannsen, H.V.; Suder, P.; Søjbjerg, J.O. Primary Repair versus Conservative Treatment of First-Time Traumatic Anterior Dislocation of the Shoulder: A Randomized Study with 10-Year Follow-Up. Arthroscopy 2007, 23, 118–123. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
|
|
|
|
|
|
|
|
| |
|
| Age | Mean age: 40 ± 14.7 (range 18–65 years) |
| Gender | Males = 67, Females = 18 |
| Affected side | Right = 60, Left = 25 |
| Dominant arm | Yes = 57, No = 28 |
| Family history of dislocations | Yes = 0, No = 85 |
| Hyperlaxity | Yes = 2, No = 83 |
| Working activity | High-risk jobs (paratrooper, bricklayer, military, police, mechanic, jockey, warehouse worker) = 15; Non-high-risk jobs (painter, housewife, pensioner, pharmacist, engineer, waiter, student, driver, fisherman, chef, employee, doctor, computer scientist, trader, hairdresser) = 70 |
| Sports activity practised | Sports that require contact or overhead forced (basket, soccer, martial arts, weightlifting, bodybuilding, rugby, military, tennis, motorbike, swimming and volleyball) = 39; Other sports (fitness exercise, cycling, horseback riding, jogging, skiing, immersion, athletics) = 46 |
| Level of sport | No sport = 29, Non-Competitive = 46, Competitive = 10 |
| Post-reduction physiokinesitherapy | Yes = 52, No = 33 |
| Time to return to sports | From 1 to 8 months |
| Hill-Sachs | Yes = 14, No = 71 |
| Bony Bankart | Yes = 5, No = 80 |
| Rotator cuff injury | Yes = 17, No = 68 |
| Greater tuberosity fracture | Yes = 3, No = 82 |
| UCLA Score | Mean score: 17.4 ± 3.5 |
| SST Score | Mean score: 9.2 ± 18.1 |
| SPADI Score | Mean score: 84.7 ± 26.4 |
| ISIS Score | Score 0–2 = 65, score 3–6 = 19, score > 6 = 1 |
| Variables | p-Value |
|---|---|
| ISIS | 0.441 |
| High-risk working activities | 0.024 * |
| Rotator cuff injury | <0.001 * |
| Contact or overhead sports | 0.127 |
| Sex | 0.389 |
| Age | 0.435 |
| Dominant limb | 0.777 |
| Familiar history | N/A |
| Hyperlaxity | 0.577 |
| Competitive sport | 0.383 |
| Post-reduction physiokinesitherapy | 0.180 |
| Return to sports activity time | 0.977 |
| Hill-Sachs lesion | 0.252 |
| Bony_Bankart lesion | 0.999 |
| Great tuberosity fracture | 0.999 |
| UCLA Score | 0.369 |
| SPADI Score | 0.879 |
| SST Score | 0.806 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Papalia, R.; Ciapini, G.; De Salvatore, S.; Casciaro, C.; Ferrari, E.; Cosseddu, F.; Novi, M.; Piergentili, I.; Parchi, P.; et al. Instability Severity Index Score Does Not Predict the Risk of Shoulder Dislocation after a First Episode Treated Conservatively. Int. J. Environ. Res. Public Health 2021, 18, 12026. https://doi.org/10.3390/ijerph182212026
Longo UG, Papalia R, Ciapini G, De Salvatore S, Casciaro C, Ferrari E, Cosseddu F, Novi M, Piergentili I, Parchi P, et al. Instability Severity Index Score Does Not Predict the Risk of Shoulder Dislocation after a First Episode Treated Conservatively. International Journal of Environmental Research and Public Health. 2021; 18(22):12026. https://doi.org/10.3390/ijerph182212026
Chicago/Turabian StyleLongo, Umile Giuseppe, Rocco Papalia, Gianluca Ciapini, Sergio De Salvatore, Carlo Casciaro, Elisa Ferrari, Fabio Cosseddu, Michele Novi, Ilaria Piergentili, Paolo Parchi, and et al. 2021. "Instability Severity Index Score Does Not Predict the Risk of Shoulder Dislocation after a First Episode Treated Conservatively" International Journal of Environmental Research and Public Health 18, no. 22: 12026. https://doi.org/10.3390/ijerph182212026