
A Multilevel Perspective on the Health Effect of Social Capital: Evidence for the Relative Importance of Individual Social Capital over Neighborhood Social Capital


 , , and
, , and
Abstract
:1. Introduction
1.1. Different Approaches to and Conceptualizations of Social Capital
1.2. Health Effects of Neighborhood and Individual Social Capital: The Studied Social Processes
- Neighborhoods & social capital: the studied social processes
- Social capital at the individual level: the studied social processes
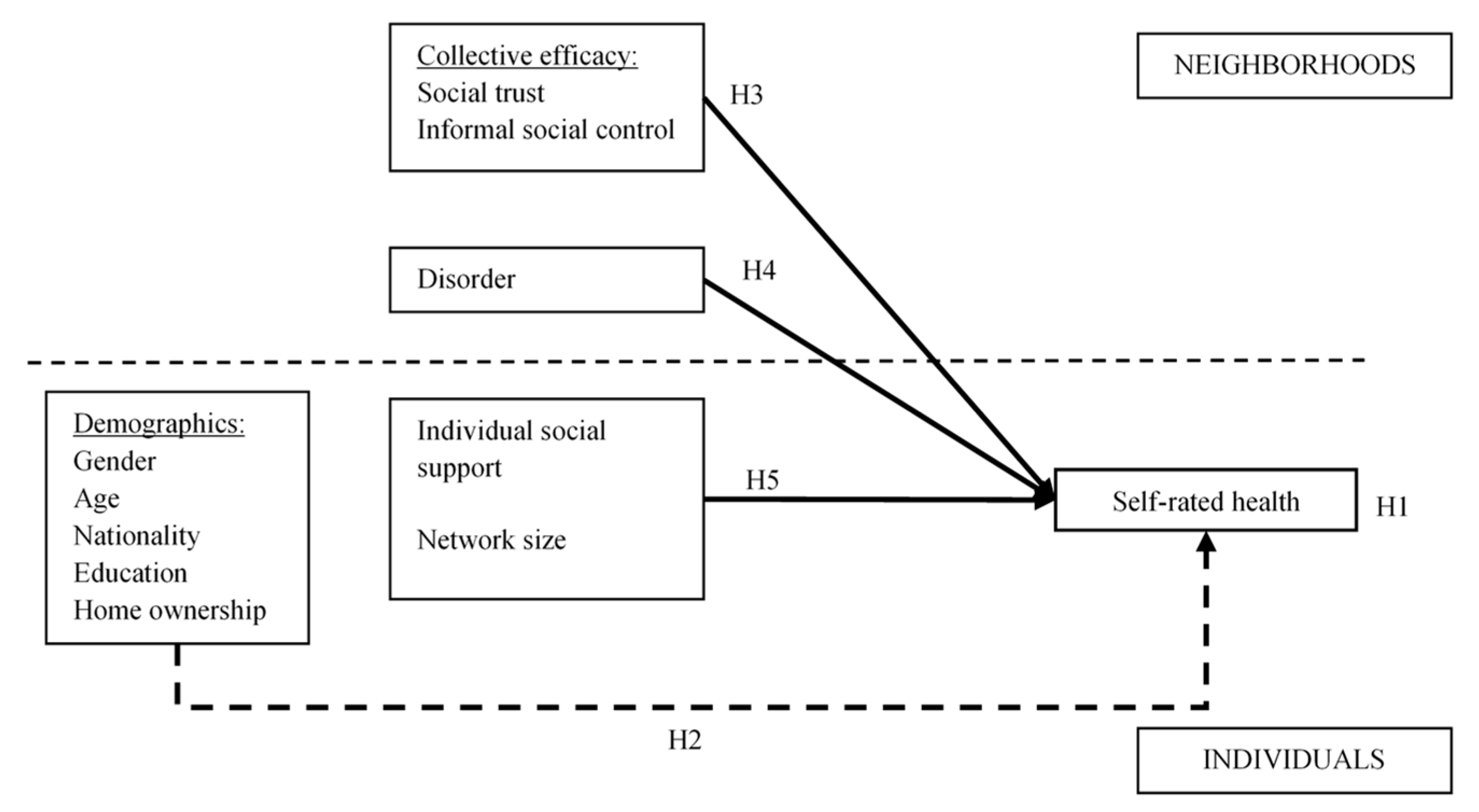
1.3. Conceptual Model and Hypotheses
2. Materials and Methods
2.1. SWING Study
2.2. Measures
2.3. Analytic Strategy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Summative Scale and Individual Items | Coding | Cronbach’s Alpha/Factor Loadings |
|---|---|---|
| Individual characteristics | ||
| Individual social support (individual items were on an 8-point scale) | 0.81 | |
| How many friends, family members or acquaintances | ||
| 1. understand your problems? | 0 → >10 | 0.72 |
| 2. would let you move into their house for a week if you temporarily could not stay at your house? | 0 → >10 | 0.72 |
| 3. would encourage you to go to the doctor if you experience health problems? | 0 → >10 | 0.73 |
| 4. make you feel good? (e.g., make you feel you are useful or make you feel they are glad to know you) | 0 → >10 | 0.70 |
| Neighborhood characteristics | ||
| Social trust (individual items were on an 5-point Likert scale) | 0.80 | |
| 1. People around here are willing to help their neighbors | totally disagree → totally agree | 0.76 |
| 2. This is a close-knit neighbourhood | totally disagree → totally agree | 0.76 |
| 3. People in this neighborhood can be trusted | totally disagree → totally agree | 0.62 |
| 4. Contacts between inhabitants in this neighborhood are generally positive | totally disagree → totally agree | 0.72 |
| Informal social control (individual items were on an 5-point Likert scale) | 0.84 | |
| How likely is it that you could count on neighbors intervening when … | ||
| 1. children were skipping school and hang out on a street corner | very likely → very unlikely | 0.61 |
| 2. children were spray-painting graffiti on a local building | very likely → very unlikely | 0.73 |
| 3. children were showing disrespect to an adult | very likely → very unlikely | 0.69 |
| 4. a fight breaks out in front of their house | very likely → very unlikely | 0.72 |
| 5. children were making too much racket | very likely → very unlikely | 0.72 |
| 6. children are using soft drugs (smoking weed, hasj, etc.) | very likely → very unlikely | 0.63 |
| Disorder (individual items were on an 5-point Likert scale) | 0.85 | |
| 1. Adolescents hanging around on street corners | never → very often | 0.66 |
| 2. Groups of adolescents harassing people to obtain money or goods | never → very often | 0.78 |
| 3. Men drinking alcohol in public | never → very often | 0.67 |
| 4. People selling drugs (hash, weed, etc.) on the streets | never → very often | 0.70 |
| 5. People being threatened on the streets with weapons or knives | never → very often | 0.65 |
| 6. Fights between adolescents on the streets | never → very often | 0.80 |
| Model Parallel to Model 4 in Table 3 B (S.E) | |
|---|---|
| Level 2: Neighborhood-level characteristics (fixed effects) | |
| Social trust (standardized) | −0.102 * (0.049) |
| Informal social control (standardized) | n.s. |
| Disorder (standardized) | 0.110 * (0.050) |
| Level 1: Individual-level characteristics (fixed effects) | |
| Gender (ref. cat. = women) | −0.178 * (0.077) |
| Age (standardized) | 0.459 *** (0.046) |
| Nationality (ref. cat. = Belgian) | n.s. |
| Education (ref. cat. = high) | |
| Low | 0.745 *** (0.114) |
| Middle | 0.350 *** (0.088) |
| Home ownership (ref. cat. = owner) | |
| Tenants in social rented housing | 0.339 * (0.137) |
| Tenants in private rented housing | n.s. |
| Individual social support (standardized) | −0.291 *** (0.043) |
| Network size (ref. cat. = ≥26) | |
| ≤10 | 0.303 ** (0.103) |
| 11–25 | n.s. |
| Intercept (ref. cat. = very good self-rated health) | |
| Very bad self-rated health | −5.683 *** (0.246) |
| Bad self-rated health or worse | −3.884 *** (0.138) |
| Moderate self-rated health or worse | −2.107 *** (0.107) |
| Good self-rated health or worse | 0.694 *** (0.096) |
| Random effects | |
| Neighborhood | 0.005 n.s. |
References
- Kawachi, I.; Berkman, L.F. Neighborhoods and Health; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Carpiano, R.M. Toward a neighborhood resource-based theory of social capital for health: Can Bourdieu and sociology help? Soc. Sci. Med. 2006, 62, 165–175. [Google Scholar] [CrossRef]
- De Silva, M.J.; McKenzie, K.; Harpham, T.; Huttly, S.R.A. Social capital and mental illness: A systematic review. J. Epidemiol. Community Health 2005, 59, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Francq, B.; Wagener, M. Stedenbeleid en armoede. In Armoede in België. Jaarboek 2012; Vranken, J., Lahaye, W., Geerts, A., Coppée, C., Eds.; Acco: Leuven, Belgium, 2012. [Google Scholar]
- Arcaya, M.C.; Tucker-Seeley, R.D.; Kim, R.; Schnake-Mahl, A.; So, M.; Subramanian, S.V. Research on neighborhood effects on health in the United States: A systematic review of study characteristics. Soc. Sci. Med. 2016, 168, 16–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, D.T.; Kawachi, I. Neighborhoods and Health: A Progress Report. In Neighborhoods and Health, 2nd ed.; Duncan, D.T., Kawachi, I., Eds.; Oxford University Press: New York, NY, USA, 2018; pp. 1–18. [Google Scholar]
- Diez Roux, A.V. Investigating neighborhood and area effects on health. Am. J. Public Health 2001, 91, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diez Roux, A.V. Residential environments and cardiovascular risk. J. Urban. Health Bull. N. Y. Acad. Med. 2003, 80, 569–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, M.; Browning, C.R.; Cagney, K.A. Poverty, affluence, and income inequality: Neighborhood economic structure and its implications for health. Soc. Sci. Med. 2003, 57, 843–860. [Google Scholar] [CrossRef]
- Franzini, L.; Caughy, M.; Spears, W.; Fernandez Esquer, M.E. Neighborhood economic conditions, social processes, and self-rated health in low-income neighborhoods in Texas: A multilevel latent variables model. Soc. Sci. Med. 2005, 61, 1135–1150. [Google Scholar] [CrossRef]
- Borrell, C.; Mari-Dell’Olmo, M.; Palencia, L.; Gotsens, M.; Burstrom, B.; Dominguez-Berjon, F.; Rodriguez-Sanz, M.; Dzurova, D.; Gandarillas, A.; Hoffmann, R.; et al. Socioeconomic inequalities in mortality in 16 European cities. Scand. J. Public Heal. 2014, 42, 245–254. [Google Scholar] [CrossRef]
- Hou, F.; Myles, J. Neighbourhood inequality, neighbourhood affluence and population health. Soc. Sci. Med. 2005, 60, 1557–1569. [Google Scholar] [CrossRef]
- Vyncke, V.; De Clercq, B.; Stevens, V.; Costongs, C.; Barbareschi, G.; Jonsson, S.H.; Curvo, S.D.; Kebza, V.; Currie, C.; Maes, L. Does neighbourhood social capital aid in levelling the social gradient in the health and well-being of children and adolescents? A literature review. BMC Public Health 2013, 13, 65. [Google Scholar] [CrossRef] [Green Version]
- Ehsan, A.; Klaas, H.S.; Bastianen, A.; Spini, D. Social capital and health: A systematic review of systematic reviews. SSM-Popul. Health 2019, 8, 100425. [Google Scholar] [CrossRef]
- Villalonga-Olives, E.; Almansa, J.; Knott, C.L.; Ransome, Y. Social capital and health status: Longitudinal race and ethnicity differences in older adults from 2006 to 2014. Int. J. Public Health 2020, 65, 291–302. [Google Scholar] [CrossRef]
- Maass, R.; Kloeckner, C.A.; Lindstrom, B.; Lillefjell, M. The impact of neighborhood social capital on life satisfaction and self-rated health: A possible pathway for health promotion? Health Place 2016, 42, 120–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macinko, J.; Starfield, B. The utility of social capital in research on health determinants. Milbank Q. 2001, 79, 387–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poortinga, W. Social capital: An individual or collective resource for health? Soc. Sci. Med. 2006, 62, 292–302. [Google Scholar] [CrossRef]
- Villalonga-Olives, E.; Kawachi, I. The measurement of social capital. Gac. Sanit. 2015, 29, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- House, J.S.; Umberson, D.; Landis, K.R. Structures and Processes of Social Support. Annu. Rev. Sociol. 1988, 14, 293–318. [Google Scholar] [CrossRef]
- Carpiano, R.M. Neighborhood social capital and adult health: An empirical test of a Bourdieu-based model. Health Place 2007, 13, 639–655. [Google Scholar] [CrossRef]
- Mohnen, S.M.; Volker, B.; Flap, H.; Groenewegen, P.P. Health-related behavior as a mechanism behind the relationship between neighborhood social capital and individual health—A multilevel analysis. BMC Public Health 2012, 12, 116. [Google Scholar] [CrossRef] [Green Version]
- Nieuwenhuis, J. Neighborhood social capital and adolescents’ individual health development. Soc. Sci. Med. 2020, 265. [Google Scholar] [CrossRef]
- Macintyre, S.A.; Ellaway, A. Neighborhoods and health: Overview. In Neighborhoods and Health; Kawachi, I., Berkman, L.F., Eds.; Oxford University Press: New York, NY, USA, 2003; p. 2042. [Google Scholar]
- Sampson, R.J. The neighborhood context of well-being. Perspect. Biol. Med. 2003, 46, S53–S64. [Google Scholar] [CrossRef]
- Mohnen, S.M.; Groenewegen, P.R.; Volker, B.; Flap, H. Neighborhood social capital and individual health. Soc. Sci. Med. 2011, 72, 660–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodgers, J.; Valuev, A.V.; Hswen, Y.; Subramanian, S.V. Social capital and physical health: An updated review of the literature for 2007–2018. Soc. Sci. Med. 2019, 236, 112360. [Google Scholar] [CrossRef] [PubMed]
- De Clercq, B.; Vyncke, V.; Hublet, A.; Elgar, F.J.; Ravens-Sieberer, U.; Currie, C.; Hooghe, M.; Ieven, A.; Maes, L. Social capital and social inequality in adolescents’ health in 601 Flemish communities: A multilevel analysis. Soc. Sci. Med. 2012, 74, 202–210. [Google Scholar] [CrossRef]
- Folland, S. Does “community social capital” contribute to population health? Soc. Sci. Med. 2007, 66, 2342–2354. [Google Scholar] [CrossRef]
- Ziersch, A.M.; Baum, F.E.; MacDougall, C.; Putland, C. Neighbourhood life and social capital: The implications for health. Soc. Sci. Med. 2005, 60, 71–86. [Google Scholar] [CrossRef]
- Zock, J.P.; Verheij, R.; Helbich, M.; Volker, B.; Spreeuwenberg, P.; Strak, M.; Janssen, N.A.H.; Dijst, M.; Groenewegen, P. The impact of social capital, land use, air pollution and noise on individual morbidity in Dutch neighbourhoods. Environ. Int. 2018, 121, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.T.; Scheffler, R.M.; Seo, S.; Reed, M. The empirical relationship between community social capital and the demand for cigarettes. Health Econ. 2006, 15, 1159–1172. [Google Scholar] [CrossRef]
- Thorlindsson, T.; Valdimarsdottir, M.; Jonsson, S.H. Community social structure, social capital and adolescent smoking: A multi-level analysis. Health Place 2012, 18, 796–804. [Google Scholar] [CrossRef]
- Tobler, A.L.; Komro, K.A.; Maldonado-Molina, M.M. Early Adolescent, Multi-ethnic, Urban Youth’s Exposure to Patterns of Alcohol-related Neighborhood Characteristics. J. Commun. Health 2009, 34, 361–369. [Google Scholar] [CrossRef] [Green Version]
- Neutens, T.; Vyncke, V.; De Winter, D.; Willems, S. Neighborhood differences in social capital in Ghent (Belgium): A multilevel approach. Int. J. Health Geogr 2013, 12, 52. [Google Scholar] [CrossRef] [Green Version]
- Lindstrom, M.; Merlo, J.; Ostergren, P.O. Individual and neighbourhood determinants of social participation and social capital: A multilevel analysis of the city of Malmo, Sweden. Soc. Sci. Med. 2002, 54, 1779–1791. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Lochner, K.A.; Kawachi, I. Neighborhood differences in social capital: A compositional artifact or a contextual construct? Health Place 2003, 9, 33–44. [Google Scholar] [CrossRef]
- Vyncke, V. Do We All Get by with a Little Help from Our Friends? An Exploration of Social Capital’s Differential Association with Health in the Context of Health Inequity; Ghent University: Ghent, Belgium, 2015. [Google Scholar]
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Diez Roux, A. The Examination of Neighborhood Effects on Health: Conceptual and Methodological Issues Related to the Presence of Multiple Levels of Organization. In Neighborhoods and Health; Kawachi, I., Berkman, L.F., Eds.; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Kawachi, I.; Subramanian, S.V.; Kim, D. Social capital and health: A decade of progress and beyond. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D., Eds.; Springer Science: New York, NY, USA, 2008; pp. 1–26. [Google Scholar]
- Pauwels, L.; Hardyns, W. Measuring Community (Dis) Organizational Processes through Key Informant Analysis. Eur. J. Criminol. 2009, 6, 401–417. [Google Scholar] [CrossRef]
- Hardyns, W.; Snaphaan, T.; Pauwels, L.J.R.; Vyncke, V.; Willems, S. A Multilevel Analysis of Collective Efficacy, Neighborhood Disorder, and Individual Social Capital on Avoidance Behavior. Crime Delinq. 2019, 65, 994–1021. [Google Scholar] [CrossRef]
- Ferlander, S. The importance of different forms of social capital for health. Acta Sociol. 2007, 50, 115–128. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.; Haines, V.; Hawe, P.; Shiell, A. Lost in translation: A genealogy of the “social capital” concept in public health. J. Epidemiol. Community Health 2006, 60, 729–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putnam, R. Bowling Alone: America’s Declining Social Capital. J. Democr. 1995, 6, 65–78. [Google Scholar] [CrossRef] [Green Version]
- Song, L. Your Body Knows Who You Know: Social Capital and Health Inequality. Ph.D. Thesis, Duke University, Durham, CA, USA, 2009. [Google Scholar]
- Flap, H. Creation and returns of social capital: A new research program. In Creation and Returns of Social Capital. Theory, Research and Measurement; Flap, H., Völker, B., Eds.; Routledge: London, UK, 2004. [Google Scholar]
- Lin, N. Social Capital: A Theory of Structure and Action; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Bourdieu, P.; Wacquant, L. Invitation to Reflexive Sociology; University of Chicago Press: Chicago, IL, USA, 1992. [Google Scholar]
- Rostila, M. Social Capital and Health Inequality in European Welfare States; Palgrave Macmillan: Basingstoke, UK, 2013. [Google Scholar]
- Villalonga-Olives, E.; Kawachi, I. The dark side of social capital: A systematic review of the negative health effects of social capital. Soc. Sci. Med. 2017, 194, 105–127. [Google Scholar] [CrossRef]
- Moore, S.; Daniel, M.; Gauvin, L.; Dube, L. Not all social capital is good capital. Health Place 2009, 15, 1071–1077. [Google Scholar] [CrossRef]
- Portes, A. Social capital: Its origins and application in modern sociology. Annu. Rev. Sociol. 1998, 24, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Derose, K.P.; Varda, D.M. Social Capital and Health Care Access: A Systematic Review. Med. Care Res. Rev. 2009, 66, 272–306. [Google Scholar] [CrossRef] [Green Version]
- Putnam, R. Bowling Alone: The Collapse and Revival of American Community; Simon & Schuster: New York, NY, USA, 2000. [Google Scholar]
- Sampson, R.J.; Raudenbush, S.W.; Earls, F. Neighborhoods and violent crime: A multilevel study of collective efficacy. Science 1997, 277, 918–924. [Google Scholar] [CrossRef]
- Drukker, M.; Buka, S.L.; Kaplan, C.; McKenzie, K.; Van Os, J. Social capital and young adolescents’ perceived health in different sociocultural settings. Soc. Sci. Med. 2005, 61, 185–198. [Google Scholar] [CrossRef]
- Drukker, M.; Kaplan, C.; Feron, F.; van Os, J. Children’s health-related quality of life, neighbourhood socio-economic deprivation and social capital. A contextual analysis. Soc. Sci. Med. 2003, 57, 825–841. [Google Scholar] [CrossRef]
- Novak, D.; Suzuki, E.; Kawachi, I. Are family, neighbourhood and school social capital associated with higher self-rated health among Croatian high school students? A population-based study. BMJ Open 2015, 5, e007184. [Google Scholar] [CrossRef] [Green Version]
- Furuta, M.; Ekuni, D.; Takao, S.; Suzuki, E.; Morita, M.; Kawachi, I. Social capital and self-rated oral health among young people. Community Dent. Oral. 2012, 40, 97–104. [Google Scholar] [CrossRef]
- Kim, J. Neighborhood disadvantage and mental health: The role of neighborhood disorder and social relationships. Soc. Sci. Res. 2010, 39, 260–271. [Google Scholar] [CrossRef]
- Ruijsbroek, A.; Droomers, M.; Hardyns, W.; Groenewegen, P.P.; Stronks, K. The interplay between neighbourhood characteristics: The health impact of changes in social cohesion, disorder and unsafety feelings. Health Place 2016, 39, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Steenbeek, W. Social and Physical Disorder. In How Community, Business Presence and Entrepreneurs Influence Disorder in Dutch Neighborhoods; Utrecht University Press: Utrecht, The Netherlands, 2011. [Google Scholar]
- Sampson, R.J.; Wikström, P. The social order of violence in Chicago and Stockholm neighborhoods: A comparative study. In Order, Conflict, and Violence; Kalyvas, S.N., Shapiro, I., Masoud, T.E., Eds.; Cambridge University Press: Cambridge, UK, 2008; Volume 97–119. [Google Scholar]
- Taylor, R.B. Human Territorial Functioning: An Empirical, Evolutionary Perspective on Individual and Small Group Territorial Cognitions, Behaviors, and Consequences; Cambridge University Press: Cambridge, UK, 1988. [Google Scholar]
- Wilson, J.Q.; Kelling, G.L. Broken windows: The police and neighborhood safety. Atlantic 1982, 249, 29–38. [Google Scholar]
- Skogan, W.G. Disorder and Decline; The Free Press: New York, NY, USA, 1990. [Google Scholar]
- Bertotti, M.; Watts, P.; Netuveli, G.; Yu, G.; Schmidt, E.; Tobi, P.; Lais, S.; Renton, A. Types of Social Capital and Mental Disorder in Deprived Urban Areas: A Multilevel Study of 40 Disadvantaged London Neighbourhoods. PLoS ONE 2013, 8, e80127. [Google Scholar] [CrossRef]
- Bjornstrom, E.E.; Ralston, M.L.; Kuhl, D.C. Social cohesion and self-rated health: The moderating effect of neighborhood physical disorder. Am. J. Community Psychol. 2003, 52, 302–3012. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Neighborhood disadvantage, disorder, and health. J. Health Soc. Behav. 2001, 42, 258–276. [Google Scholar] [CrossRef] [Green Version]
- Bourdieu, P. The forms of capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J., Ed.; Greenwood: New York, NY, USA, 1986; pp. 241–258. [Google Scholar]
- Coyne, J.C.; Downey, G. Social-Factors and Psychopathology—Stress, Social Support, and Coping Processes. Annu. Rev. Psychol 1991, 42, 401–425. [Google Scholar] [CrossRef]
- Thoits, P.A. Mechanisms Linking Social Ties and Support to Physical and Mental Health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.C. Measuring personal networks with daily contacts: A single-item survey question and the contact diary. Soc. Netw. 2005, 27, 169–186. [Google Scholar] [CrossRef]
- Hardyns, W.; Vyncke, V.; Pauwels, L.; Willems, S. Study protocol: SWING—Social capital and well-being in neighborhoods in Ghent. Int. J. Equity Health 2015, 14, 36. [Google Scholar] [CrossRef] [Green Version]
- Raudenbush, S.W.; Sampson, R.J. Ecometrics: Toward a science of assessing ecological settings, with application to the systematic social observation of neighborhoods. Sociol. Methodol. 1999, 29, 1–41. [Google Scholar] [CrossRef]
- Kaplan, G.A.; Goldberg, D.E.; Everson, S.A.; Cohen, R.D.; Salonen, R.; Tuomilehto, J.; Salonen, J. Perceived health status and morbidity and mortality: Evidence from the Kuopio ischaemic heart disease risk factor study. Int. J. Epidemiol. 1996, 25, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, P.; Guéguen, A.; Schmaus, A.; Nakache, J.P.; Goldberg, M. Longitudinal study of associations between perceived health status and self reported diseases in the French Gazel cohort. J. Epidemiol. Community Health 2001, 55, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 320. [Google Scholar] [CrossRef] [Green Version]
- Oberwittler, D.; Wikström, P. Why small is better: Advancing the study of the role of behavioral contexts in crime causation. In Putting Crime in Its Place: Units of Analysis in Geographic Criminology; Bruinsma, G.J.N., Weisburd, D., Bernasco, W., Eds.; Springer: New York, NY, USA, 2009; pp. 33–58. [Google Scholar]
- Hox, J.J. Multilevel Analysis: Techniques and Applications; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Heck, R.H.; Thomas, S.L.; Tabata, L.N. Multilevel and Longitudinal Modeling with SPSS; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Kim, D.; Subramanian, S.V.; Kawachi, I. Social capital and physical health: A systematic review of the literature. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D., Eds.; Springer: New York, NY, USA, 2008; pp. 139–190. [Google Scholar]
- Giordano, G.N.; Lindstrom, M. Trust and health: Testing the reverse causality hypothesis. J. Epidemiol. Community Health 2016, 70, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I. Commentary: Social capital and health: Making the connections one step at a time. Int. J. Epidemiol. 2006, 35, 989–993. [Google Scholar] [CrossRef] [Green Version]
- Rocco, L.; Fumagalli, E.; Suhrcke, M. From Social Capital to Health and Back. Health Econ. 2014, 23, 586–605. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, S.V.; Jones, K.; Duncan, C. Multilevel methods for public health research. In Neighborhoods and Health; Kawachi, I., Berkman, L., Eds.; Oxford University Press: New York, NY, USA, 2003; pp. 65–111. [Google Scholar]
- Uphoff, E.P.; Pickett, K.E.; Cabieses, B.; Small, N.; Wright, J. A systematic review of the relationships between social capital and socioeconomic inequalities in health: A contribution to understanding the psychosocial pathway of health inequalities. Int. J. Equity Health 2013, 12, 54. [Google Scholar] [CrossRef] [Green Version]
- Villalonga-Olives, E.; Wind, T.R.; Kawachi, I. Social capital interventions in public health: A systematic review. Soc. Sci. Med. 2018, 212, 203–218. [Google Scholar] [CrossRef]
- Delpierre, C.; Lauwers-Cances, V.; Datta, G.D.; Lang, T.; Berkman, L. Using self-rated health for analysing social inequalities in health: A risk for underestimating the gap between socioeconomic groups? J. Epidemiol. Community Health 2009, 63, 426–432. [Google Scholar] [CrossRef]
- Dowd, J.B.; Zajacova, A. Does the predictive power of self-rated health for subsequent mortality risk vary by socioeconomic status in the US? Int. J. Epidemiol. 2007, 36, 1214–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merton, R.K.; Rossi, A.S. Contributions to the Theory of Reference Group Behavior. In Social Theory and Social Structure; Merton, R.K., Ed.; Free Press: New York, NY, USA, 1968; pp. 279–334. [Google Scholar]
- Maclennan, D. Neighbourhoods: Evolving Ideas, Evidence and Changing Policies. In Neighbourhood Effects or Neighbourhood Based Problems? Manley, D., van Ham, M., Bailey, N., Simpson, L., Maclennan, D., Eds.; Springer: Dordrecht, The Netherlands, 2013; Volume 269–292. [Google Scholar]
- Musterd, S.; Murie, A. The Spatial Dimensions of Urban Social Exclusion and Integration. In Neighbourhoods of Poverty. Urban Social Exclusion and Integration in Europe; Musterd, S., Murie, A., Kesteloot, C., Eds.; Palgrave Macmillan: Basingstoke, UK, 2006. [Google Scholar]
- Van Cauwenberg, J.; Van Holle, V.; De Bourdeaudhuij, I.; Van Dyck, D.; Deforche, B. Neighborhood walkability and health outcomes among older adults: The mediating role of physical activity. Health Place 2016, 37, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.; Braen, C.; Boyer, G.; Mercille, G.; Rehany, E.; Deslauriers, V.; Bilodeau, A.; Potvin, L. Neighbourhood community life and health: A systematic review of reviews. Health Place 2020, 61, 102238. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Alvarez, E.; Kawachi, I.; Riera-Romani, J. Neighbourhood social capital and obesity: A systematic review of the literature. Obes. Rev. 2019, 20, 119–141. [Google Scholar] [CrossRef] [Green Version]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social Capital and Health: A Review of Prospective Multilevel Studies. J. Epidemiol. 2012, 22, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirowsky, J.; Ross, C.E. Education, Social Status, and Health; Aldine de Gruyter: New York, NY, USA, 2003. [Google Scholar]
- Link, B.G.; Phelan, J. Social Conditions as Fundamental Causes of Disease. J. Health Soc. Behav. 1995, 35, 80–94. [Google Scholar] [CrossRef] [Green Version]
- Link, B.G.; Phelan, J.C. Understanding sociodemographic differences in health—The role of fundamental social causes. Am. J. Public Health 1996, 86, 471–473. [Google Scholar] [CrossRef] [Green Version]

| Mean/Percentage | Standard Deviation | Min. | Max. | |
|---|---|---|---|---|
| Self-rated health | 4.06 | 0.79 | 1 | 5 |
| Individual characteristics | ||||
| Gender | ||||
| Man | 48.00% | |||
| Woman | 52.00% | |||
| Age | 47.97 | 18.76 | 18 | 95 |
| Nationality | ||||
| Belgian | 90.30% | |||
| Other | 9.70% | |||
| Home ownership | ||||
| Owners | 68.60% | |||
| Tenants in social rented housing | 10.50% | |||
| Tenants in private rented housing | 20.90% | |||
| Education level | ||||
| Low | 18.90% | |||
| Middle | 33.80% | |||
| High | 47.40% | |||
| Individual social support | 17.25 | 6.32 | 0 | 28 |
| Social contacts per day | ||||
| ≤10 | 44.62% | |||
| 11–25 | 25.27% | |||
| ≥26 | 30.11% | |||
| Neighborhood characteristics | ||||
| Social trust | 14.22 | 1.34 | 10.33 | 17.25 |
| Informal social control | 18.37 | 2.20 | 12.00 | 24.50 |
| Disorder | 12.62 | 3.26 | 6.38 | 20.63 |
| 1 | 2 | 3 | |
|---|---|---|---|
| 1. Social trust | 1 | ||
| 2. Informal social control | 0.13 n.s. | 1 | |
| 3. Disorder | −0.57 *** | 0.09 n.s. | 1 |
| Model 0 B (S.E) | Model 1 B (S.E.) | Model 2 B (S.E.) | Model 3 B (S.E.) | Model 4 B (S.E.) | |
|---|---|---|---|---|---|
| Level 2: Neighborhood-level characteristics (fixed effects) | |||||
| Social trust (standardized) | 0.07 *** (0.02) | 0.04 * (0.02) | 0.04 * (0.02) | ||
| Informal social control (stand.) | n.s. | n.s. | n.s. | ||
| Disorder (standardized) | −0.06 ** (0.02) | −0.05 * (0.02) | |||
| Level 1: Individual-level characteristics (fixed effects) | |||||
| Gender (ref. cat. = women) | 0.07 * (0.03) | 0.07 * (0.03) | 0.07 * (0.03) | 0.06 * (0.03) | |
| Age (standardized) | −0.21 *** (0.02) | −0.21 *** (0.02) | −0.21 *** (0.02) | −0.16 *** (0.02) | |
| Nationality (ref. cat. = Belgian) | n.s. | n.s. | n.s. | n.s. | |
| Education (ref. cat. = high) | |||||
| Low | −0.34 *** (0.04) | −0.34 *** (0.04) | −0.34 *** (0.04) | −0.27 *** (0.04) | |
| Middle | −0.17 *** (0.03) | −0.17 *** (0.03) | −0.17 *** (0.03) | −0.12 *** (0.03) | |
| Home ownership (ref. cat. = owner) | |||||
| Tenants in social rented housing | −0.25 *** (0.05) | −0.21 *** (0.05) | −0.18 *** (0.05) | −0.13 * (0.05) | |
| Tenants in private rented housing | −0.10 ** (0.04) | −0.09 * (0.04) | −0.08 * (0.04) | n.s. | |
| Individual social support (stand.) | 0.11 *** (0.02) | ||||
| Network size (ref. cat. = ≥26) | |||||
| ≤10 | -0.13 ** (0.04) | ||||
| 11–25 | n.s. | ||||
| Intercept | 4.06 *** (0.02) | 4.20 *** (0.03) | 4.19 *** (0.03) | 4.18 *** (0.03) | 4.20 *** (0.04) |
| Random effects | |||||
| Neighborhood | 0.018 ** | 0.006 n.s. | 0.002 n.s. | 0.001 n.s. | 0.002 n.s. |
| Individual | 0.610 *** | 0.540 *** | 0.539 *** | 0.539 *** | 0.524 *** |
| ICC | 2.86% | 1.18% | 0.46% | 0.24% | 0.33% |
| Δ Deviance (Δ df) | 425 (4) *** | 8 (2) * | n.s. 3 (1) | 163 (2) *** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lagaert, S.; Snaphaan, T.; Vyncke, V.; Hardyns, W.; Pauwels, L.J.R.; Willems, S. A Multilevel Perspective on the Health Effect of Social Capital: Evidence for the Relative Importance of Individual Social Capital over Neighborhood Social Capital. Int. J. Environ. Res. Public Health 2021, 18, 1526. https://doi.org/10.3390/ijerph18041526
Lagaert S, Snaphaan T, Vyncke V, Hardyns W, Pauwels LJR, Willems S. A Multilevel Perspective on the Health Effect of Social Capital: Evidence for the Relative Importance of Individual Social Capital over Neighborhood Social Capital. International Journal of Environmental Research and Public Health. 2021; 18(4):1526. https://doi.org/10.3390/ijerph18041526
Chicago/Turabian StyleLagaert, Susan, Thom Snaphaan, Veerle Vyncke, Wim Hardyns, Lieven J. R. Pauwels, and Sara Willems. 2021. "A Multilevel Perspective on the Health Effect of Social Capital: Evidence for the Relative Importance of Individual Social Capital over Neighborhood Social Capital" International Journal of Environmental Research and Public Health 18, no. 4: 1526. https://doi.org/10.3390/ijerph18041526