
Seroprevalence of SARS-CoV-2 Infection and Adherence to Preventive Measures in Cuenca, Ecuador, October 2020, a Cross-Sectional Study

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Testing for COVID-19 Infection
2.3. Assessment of Adherence
2.4. Data Processing and Analysis
3. Results
3.1. Participants Characteristics
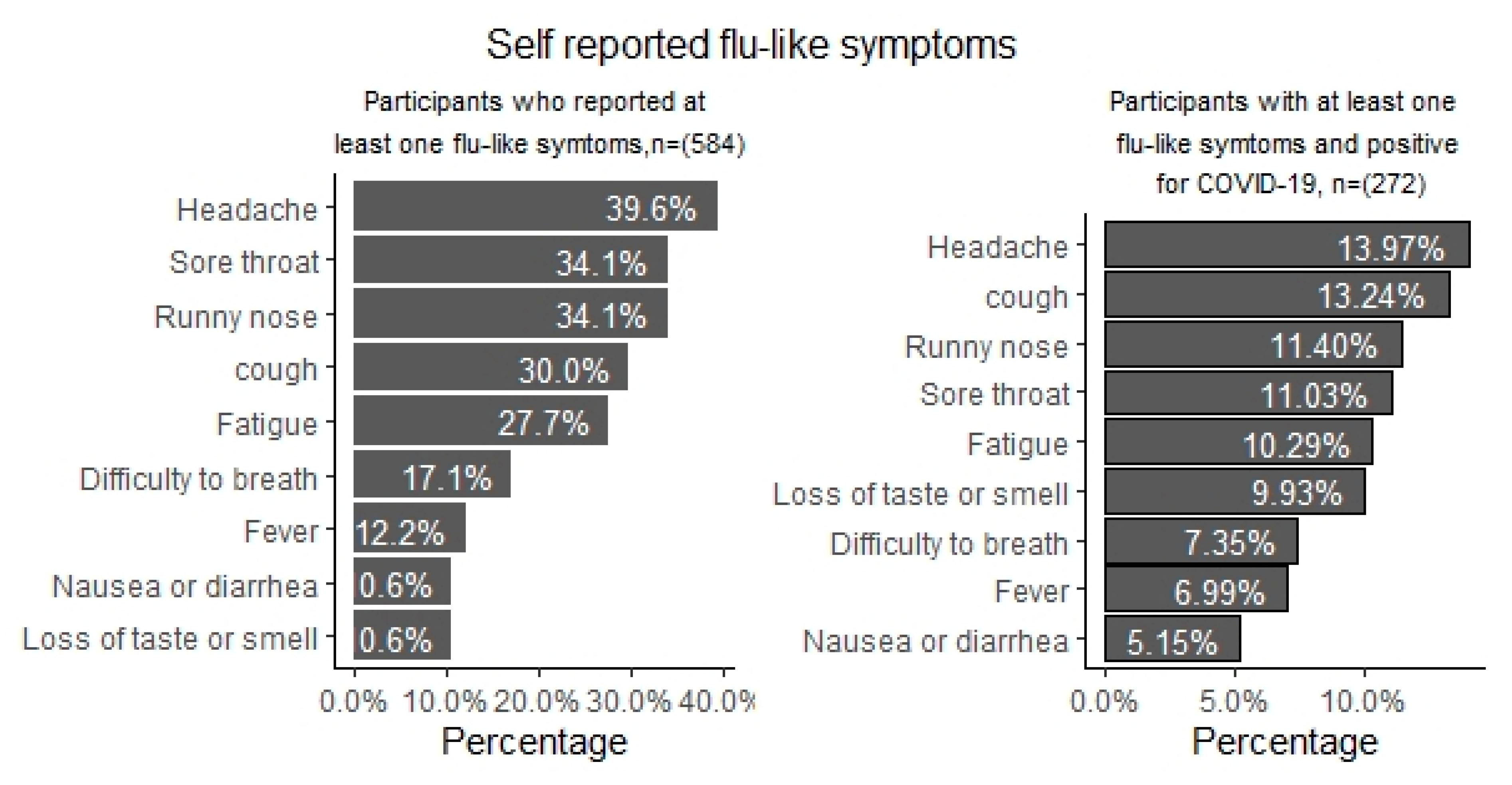
3.2. Flu-Like Symptoms Associated with COVID-19 Infection among Participants
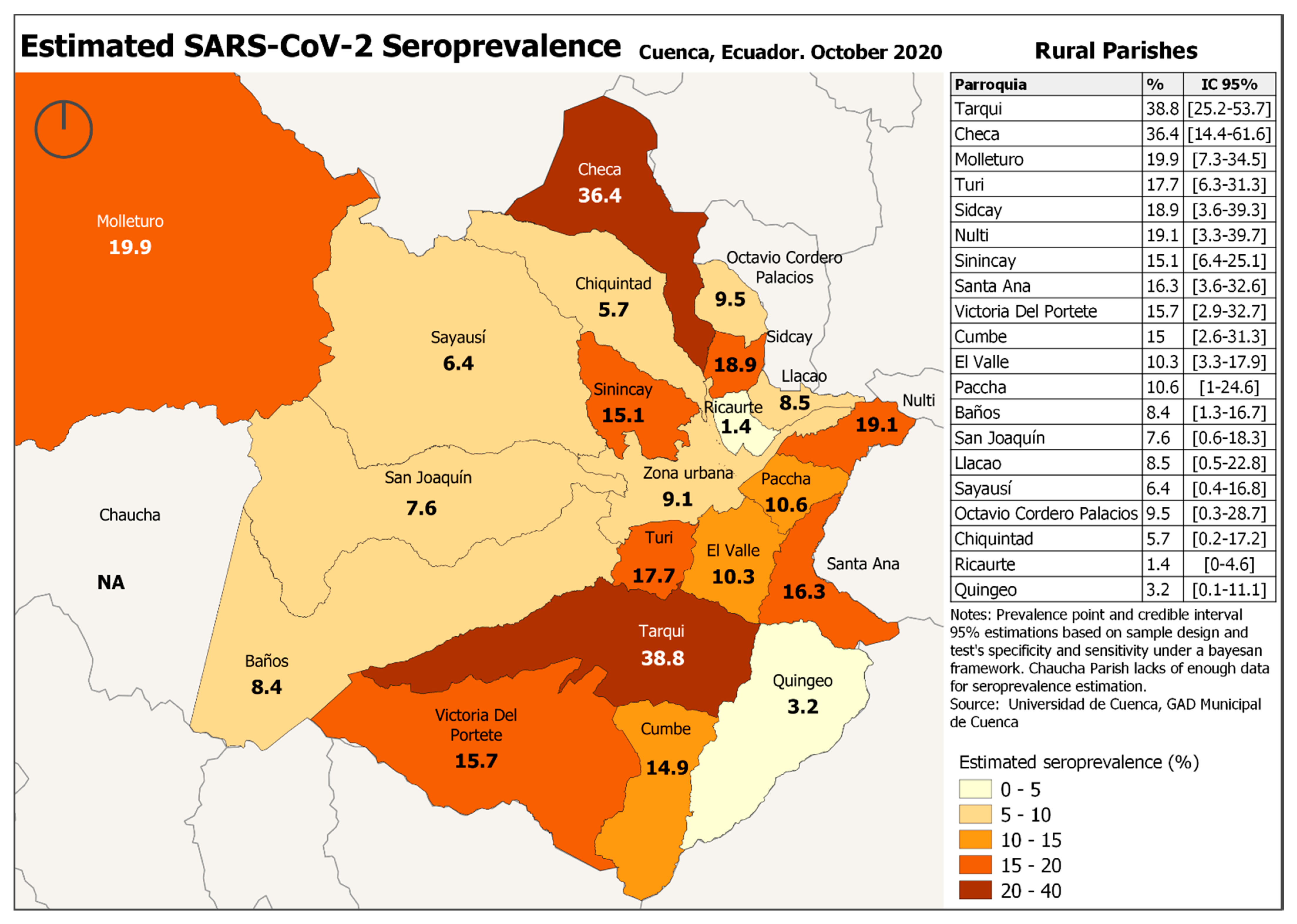
3.3. SARS-CoV-2 Seroprevalence in Cuenca
3.4. Factors Associated with SARS-CoV-2 Seroprevalence
3.5. Adherence to COVID-19 Preventive Measures
4. Discussion
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019–COVID-19. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. COVID-19 Situation Update Worldwide, as of 14 January 2021. ECDC, 2021. Available online: https://www.ecdc.europa.eu/en/covid-19-pandemic (accessed on 14 January 2021).
- NBSP; Johns Hopkins University Coronavirus Resource Center. COVID-19 Dashboard by the Center for Systems Science and Engi-neering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 29 October 2020).
- Orellana, D. Movilidad en Ecuador Durante la Pandemia de COVID-19. 2020. Available online: https://public.tableau.com/profile/temporalista#!/vizhome/EcuadorMovilidadGoogleReport/Provincias (accessed on 31 January 2021).
- Servicio Nacional de Gestión de Riesgos y Emergencias. Informes de Situación e Infografías—COVID 19—desde el 29 de Febrero del 2020. 2020. Available online: https://www.gestionderiesgos.gob.ec/informes-de-situacion-covid-19-desde-el-13-de-marzo-del-2020/ (accessed on 29 February 2020).
- Orellana, D.; Gómez, A. Evolución Espacial y Temporal del Exceso de Mortalidad durante la Pandemia de COVID-19 en Ecuador; CNG2020; Universidad del Azuay: Cuenca, Ecuador, 2020; in press. [Google Scholar]
- Biocan Diagnostics Inc. Novel Coronavirus (COVID-19) IgG/IgM Antibody Test. Available online: https://www.rapidtest.ca/covid-19 (accessed on 4 February 2021).
- Jeong, H.J. The level of collapse we are allowed: Comparison of different response scales in Safety Attitudes Questionnaire. Biom. Biostat. Int. J. 2016, 4, 128–134. [Google Scholar] [CrossRef]
- IHME COVID-19 Forecasting Team. Modeling COVID-19 scenarios for the United States. Nat. Med. 2021, 27, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Júnior, A.; Dula, J.; Mahumane, S.; Koole, O.; Enosse, S.; Fodjo, J.; Colebunders, R. Adherence to COVID-19 Preventive Measures in Mozambique: Two Consecutive Online Surveys. Int. J. Environ. Res. Public Health 2021, 18, 1091. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Vilches, T.N.; Tariq, M.; Galvani, A.P.; Moghadas, S.M. The impact of mask-wearing and shelter-in-place on COVID-19 outbreaks in the United States. Int. J. Infect. Dis. 2020, 101, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Ngonghala, C.N.; Iboi, E.A.; Gumel, A.B. Could masks curtail the post-lockdown resurgence of COVID-19 in the US? Math. Biosci. 2020, 329, 108452. [Google Scholar] [CrossRef] [PubMed]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Reyes-Vega, M.F.; Soto-Cabezas, M.; Cárdenas, F.; Martel, K.S.; Valle, A.; Valverde, J.; Vidal-Anzardo, M.; Falcón, M.E.; Munayco, C.V. SARS-CoV-2 prevalence associated to low socioeconomic status and overcrowding in an LMIC megacity: A population-based seroepidemiological survey in Lima, Peru. EClinicalMedicine 2021, 34, 100801. [Google Scholar] [CrossRef] [PubMed]
- de Janeiro, R. Pesquisa Inédita do HEMORIO Revela Aumento do Número de Pessoas com Anticorpos Contra a COVID-19 na População [Internet]. Rio de Janeiro: Governo do Estado. 2020 [updated 2020 May 13; cited 2020 May 31]. Available online: https://coronavirus.rj.gov.br/pesquisa-inedita-do-hemorio-revela-aumento-no-numero-de-pessoas-com-anticorpos-contra-a-covid-19-na-populacao/ (accessed on 20 November 2020).
- Del Brutto, O.H.; Costa, A.F.; Mera, R.M.; Recalde, B.Y.; Bustos, A.J.; García, H.H. SARS-CoV-2 in rural Latin America. A population-based study in coastal Ecuador. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Buss, L.F.; Prete, C.A.; Abrahim, C.M.; Mendrone, A.; Salomon, T.; de Almeida-Neto, C.; França, R.F.; Belotti, M.C.; Carvalho, M.P.; Costa, A.G.; et al. Three-quarters attack rate of SARS-CoV-2 in the Brazilian Amazon during a largely unmiti-gated epidemic. Science 2020, 371, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Carlos Álvarez, A.; Meza-Sánchez, G.; Carlos, C.; Wilma, C.; Cristiam, C.; Freddy, A.; Hugo, R.F.; Quispe, A.M. Seroprev-alence of anti-SARS-CoV-2 antibodies in Iquitos, Loreto, Peru. MedRxiv. 2021. Available online: https://doi.org/10.1101/2021.01.17.21249913 (accessed on 25 January 2021).
- Ministerio De La Salud Publica. Inició la Vacunación Contra la COVID-19 en Ecuado. Available online: https://www.salud.gob.ec/tercera-entrega-de-vacunas-de-pfizer-llega-hoy-a-ecuador/ (accessed on 21 January 2021).
- Wang, Q.; Yu, C. The role of masks and respirator protection against SARS-CoV-2. Infect. Control. Hosp. Epidemiol. 2020, 41, 746–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noh, J.Y.; Seong, H.; Yoon, J.G.; Song, J.Y.; Cheong, H.J.; Kim, W.J. Social Distancing against COVID-19: Implication for the Control of Influenza. J. Korean Med. Sci. 2020, 35, e182. [Google Scholar] [CrossRef] [PubMed]
- Jang, W.M.; Jang, D.H.; Lee, J.Y. Social Distancing and Transmission-reducing Practices during the 2019 Coronavirus Disease and 2015 Middle East Respiratory Syndrome Coronavirus Outbreaks in Korea. J. Korean Med. Sci. 2020, 35. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Scoring | Interpretation | |
|---|---|---|---|
| I follow the 1.5–2 m physical distance rule | Yes no | 1 0 | 1 point for yes, 0 points for no |
| I wash my hands regularly or I use hand sanitiser regularly | Yes No | 1 0 | If any (or both) questions have answered yes, 1 point, 0 points for no |
| I stay at home when I have flu symptoms | Yes no | 1 0 | 1 point for yes, 0 points for no |
| I wear a face mask when I go out | Yes no | 1 0 | 1 point for yes, 0 points for no |
| I respect not going out to overcrowded places | Yes no | 1 0 | 1 point for yes, 0 points for no |
| Total adherence score (maximum): 5 | |||
| Variables | Response | No. of Positive/No. of Subjects | SARS-CoV-2 Seroprevalence (95% CI) |
|---|---|---|---|
| Sex | Male, n (%) | 118/997 | 12% (10–14) |
| Female, n (%) | 207/1460 | 14.2% (12.5–16.1) | |
| Age group | 0–19 years, n (%) | 45/402 | 11.2% (8.4–14.8) |
| 20–34 years, n (%) | 79/675 | 11.7% (9.4–14.3) | |
| 35–49 years, n (%) | 100/624 | 16% (13.3–19.2) | |
| 50–64 years, n (%) | 63/461 | 13.7% (10.7–17.2) | |
| 65+ years, n (%) | 38/295 | 13% (9.3–17.4) | |
| Parish | Rural, n (%) | 168/1231 | 13.6% (11.8–15.7) |
| Urban, n (%) | 157/1226 | 12.8% (11–14.8) | |
| Marital status | Divorced, n (%) | 27/193 | 14% (9.5–20) |
| Single, n (%) | 95/797 | 12% (9.8–14.4) | |
| Married, n (%) | 155/1122 | 13.8% (12–16) | |
| Cohabitation, n (%) | 30/186 | 16.1% (11.3–22.4) | |
| Widower, n (%) | 11/96 | 11.5% (6.1–20) | |
| Education | None, n (%) | 15/103 | 14.6% (8.6–23) |
| Primary, n (%) | 148/859 | 17.2% (14.8–20) | |
| Secondary, n (%) | 116/883 | 13.1% (11–15.6) | |
| Tertiary, n (%) | 45/602 | 7.5% (5.5–10) | |
| Monthly income | Less than 200 $, n (%) | 108/682 | 15.8% (13.2–18.8) |
| From 200 $ to 519 $, n (%) | 144/1052 | 13.7% (11.7–16) | |
| From 520 $ to 1500 $, n (%) | 61/531 | 11.5% (9–14.5) | |
| More than 1500 $, n (%) | 7/95 | 7.4% (3.3–15.1) | |
| Nationality | Ecuador, n (%) | 319/2400 | 13.3% (12–14.7) |
| Foreigner, n (%) | 6/57 | 10.5% (4.3–22) | |
| Housing conditions | House with Garden, n (%) | 145/1166 | 12.4% (10.6–14.5) |
| House without Garden n (%) | 140/980 | 14.3% (12.2–16.7) | |
| Apartment, n (%) | 23/202 | 11.4% (7.5–16.7) | |
| Quarters, n (%) | 14/96 | 14.6% (8.5–23.6) | |
| Cabin, n (%) | 3/13 | 23.1% (6.2–54) | |
| Means of transport to work | On Foot, n (%) | 65/529 | 12.6% (9.6–15.5) |
| Bicycle/Moto/Trolley car, n (%) | 12/106 | 11.3% (6.2–19.3) | |
| Private car, n (%) | 99/912 | 11% (9–13.1) | |
| Public (Bus/Taxi), n (%) | 135/742 | 18.2% (15.5–21.2) | |
| Occupation | None, n (%) | 66/610 | 10.8% (8.5–13.6) |
| Daily workers/House help, n (%) | 39/197 | 20% (14.6–26.2) | |
| Private business owners, n (%) | 134/1102 | 12.2% (10.3–14.3) | |
| Street sellers, n (%) | 4/31 | 13% (4.2–30.8) | |
| Small farm owners, n (%) | 26/85 | 30.6% (21.3–41.7) | |
| Pensioners, n (%) | 10/121 | 8.3% (4.3–15.1) | |
| Others, n (%) | 43/214 | 20% (15.1–26.2) |
| Covariates | Crude OR (95% CI) | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|
| Gender | |||
| Male | Ref | Ref | |
| Female | 1.24 (0.95–1.56) | 1.12 (0.88–1.46) | 0.190 |
| Age | |||
| 0–19 years, | Ref | Ref | |
| 20–34 years, | 1.10 (0.74–1.66) | 1.07 (0.69–1.64) | 0.751 |
| 35–49 years, | 1.53 (1.04–2.27) | 1.56 (1.07–2.46) | 0.023 |
| 50–64 years, | 1.34 (0.83–2.06) | 1.38 (0.96–2.35) | 0.078 |
| 65+ years, | 1.36 (0.84–2.21) | 1.45 (0.87–2.43) | 0.153 |
| Enough resources for living | |||
| No | Ref | Ref | |
| Yes | 0.65 (0.51–0.84) | 0.64 (0.49–0.84) | 0.001 |
| Means of transport | |||
| Private (own car, foot, bicycle) | Ref | Ref | |
| Public (bus/taxi) | 1.73 (1.36–2.21) | 1.65 (1.28–2.14) | <0.001 |
| Has anyone in your house had COVID-19? | |||
| No | Ref | Ref | |
| Yes | 5.91 (4.01–8.7) | 6.21 (4.12–9.37) | <0.001 |
| Being in contact with someone outside your home with flu-like symptoms, | |||
| No | Ref | Ref | |
| Yes | 1.90 (1.40–2.57) | 1.83 (1.32–2.53) | <0.001 |
| No of people in house | |||
| Living alone | Ref | Ref | |
| 2–4 people | 1.08 (0.72–1.61) | 1.07 (0.71–1.63) | 0.739 |
| 5–6 people | 1.05 (0.68–1.63) | 1.02 (0.64–1.6) | 0.945 |
| >6 people | 2.41 (1.47–3.95) | 2.21 (1.3–3.75) | 0.003 |
| Physical contact * with someone outside the household | |||
| No | Ref | Ref | |
| Yes | 1.49 (1.17–1.89) | 1.54 (1.20–1.98) | <0.001 |
| Covariates | Frequency (%) | Crude OR (95% CI) | Adjusted OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Non Adherence | High Adherence | ||||
| Gender | |||||
| Male | 117 (11.7) | 880 (88.3) | Ref | Ref | |
| Female | 122 (8.36) | 1338 (91.6) | 1.45 (1.11–1.9) | 1.28 (0.95–1.74) | 0.107 |
| Age | |||||
| 0–19 years, | 39 (9.7) | 363 (90.3) | Ref | Ref | |
| 20–34 years, | 88 (13) | 587 (87) | 0.71 (0.47–1.08) | 0.56 (0.35–0.9) | 0.017 |
| 35–49 years, | 53 (8.5) | 571 (91.5) | 1.18 (0.76–1.85) | 0.96 (0.58–1.58) | 0.872 |
| 50–64 years, | 36 (7.8) | 425 (92.2) | 1.25(0.77–2.03) | 0.84 (0.49–1.43) | 0.518 |
| 65+ years, | 23 (7.8) | 272 (92.2) | 1.22 (0.71–2.11) | 0.99 (0.54–1.84) | 0.993 |
| Do you know anyone who has Corona | |||||
| No | 195 (10.7) | 1619 (89.3) | Ref | Ref | |
| Yes | 44 (6.8) | 599 (93.2) | 1.78 (1.26–2.53) | 1.75 (1.2–2.54) | 0.004 |
| Education | |||||
| None | 26 (25.2) | 77 (74.8) | Ref | Ref | |
| Primary | 46 (5.4) | 813 (94.6) | 6.3 (3.66–10.85) | 5.31(2.86–9.88) | <0.001 |
| Secondary | 70 (8) | 813 (92) | 4.16 (2.5–6.95) | 3.59 (1.94–6.65) | <0.001 |
| Tertiary | 97 (16) | 505 (84) | 1.82 (1.11–3) | 1.59 (0.84–3.01) | 0.154 |
| Monthly income | |||||
| Less than 200$ | 64 (9.4) | 618 (90.6) | Ref | Ref | |
| From 200$ to 519$ | 87 (8.3) | 965 (91.7) | 1.15 (0.82–1.61) | 0.6 (0.4–0.9) | 0.014 |
| From 520$ to 1500$ | 69 (13) | 462 (87) | 0.69 (0.48–0.99) | 0.43 (0.26–0.68) | <0.001 |
| More than 1500$ | 14 (14.7) | 81 (85.3) | 0.6 (0.32–1.12) | 0.25 (0.12–0.54) | <0.001 |
| Enough resources for living | |||||
| No | 157 (20) | 629 (80) | Ref | Ref | |
| Yes | 82 (5) | 1589 (95) | 5.08 (3.82–6.77) | 7.14 (5.09–10) | <0.001 |
| Number of people in house | |||||
| Living alone | 18 (6) | 276 (94) | Ref | Ref | |
| 2–4 people | 94 (7.2) | 1214 (92.8) | 0.87 (0.52–1.47) | 0.79 (0.45–1.38) | 0.413 |
| 5–6 people | 115 (17.4) | 547 (82.6) | 0.33 (0.19–0.55) | 0.35 (0.2–0.61) | <0.001 |
| >6 people | 12 (6.2) | 181 (93.8) | 1.11 (0.51–2.4) | 1.04 (0.46–2.36) | 0.931 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acurio-Páez, D.; Vega, B.; Orellana, D.; Charry, R.; Gómez, A.; Obimpeh, M.; Verhoeven, V.; Colebunders, R. Seroprevalence of SARS-CoV-2 Infection and Adherence to Preventive Measures in Cuenca, Ecuador, October 2020, a Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4657. https://doi.org/10.3390/ijerph18094657
Acurio-Páez D, Vega B, Orellana D, Charry R, Gómez A, Obimpeh M, Verhoeven V, Colebunders R. Seroprevalence of SARS-CoV-2 Infection and Adherence to Preventive Measures in Cuenca, Ecuador, October 2020, a Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4657. https://doi.org/10.3390/ijerph18094657
Chicago/Turabian StyleAcurio-Páez, David, Bernardo Vega, Daniel Orellana, Ricardo Charry, Andrea Gómez, Michael Obimpeh, Veronique Verhoeven, and Robert Colebunders. 2021. "Seroprevalence of SARS-CoV-2 Infection and Adherence to Preventive Measures in Cuenca, Ecuador, October 2020, a Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 9: 4657. https://doi.org/10.3390/ijerph18094657