
Basic Motor Competencies of (Pre)School Children: The Role of Social Integration and Health-Related Quality of Life

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Test Instruments and Data Collection
- Basic motor competencies (BMCs; children tests):
- Social integration (PIQ; teacher questionnaires):
- General health-related quality of life (general HRQoL; parent questionnaires):
- Physical well-being (parent questionnaires):
2.3. Data Analysis
3. Results
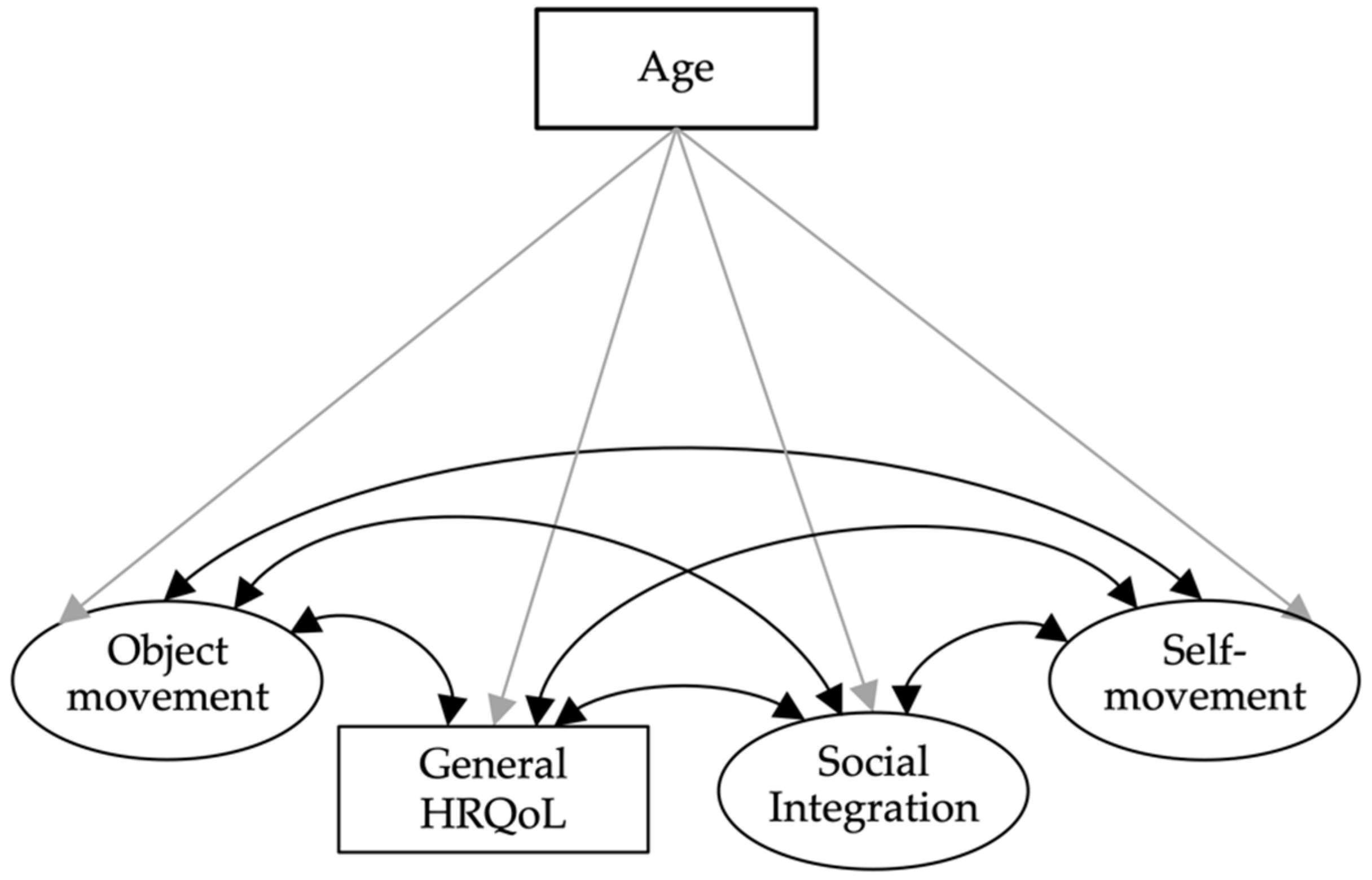
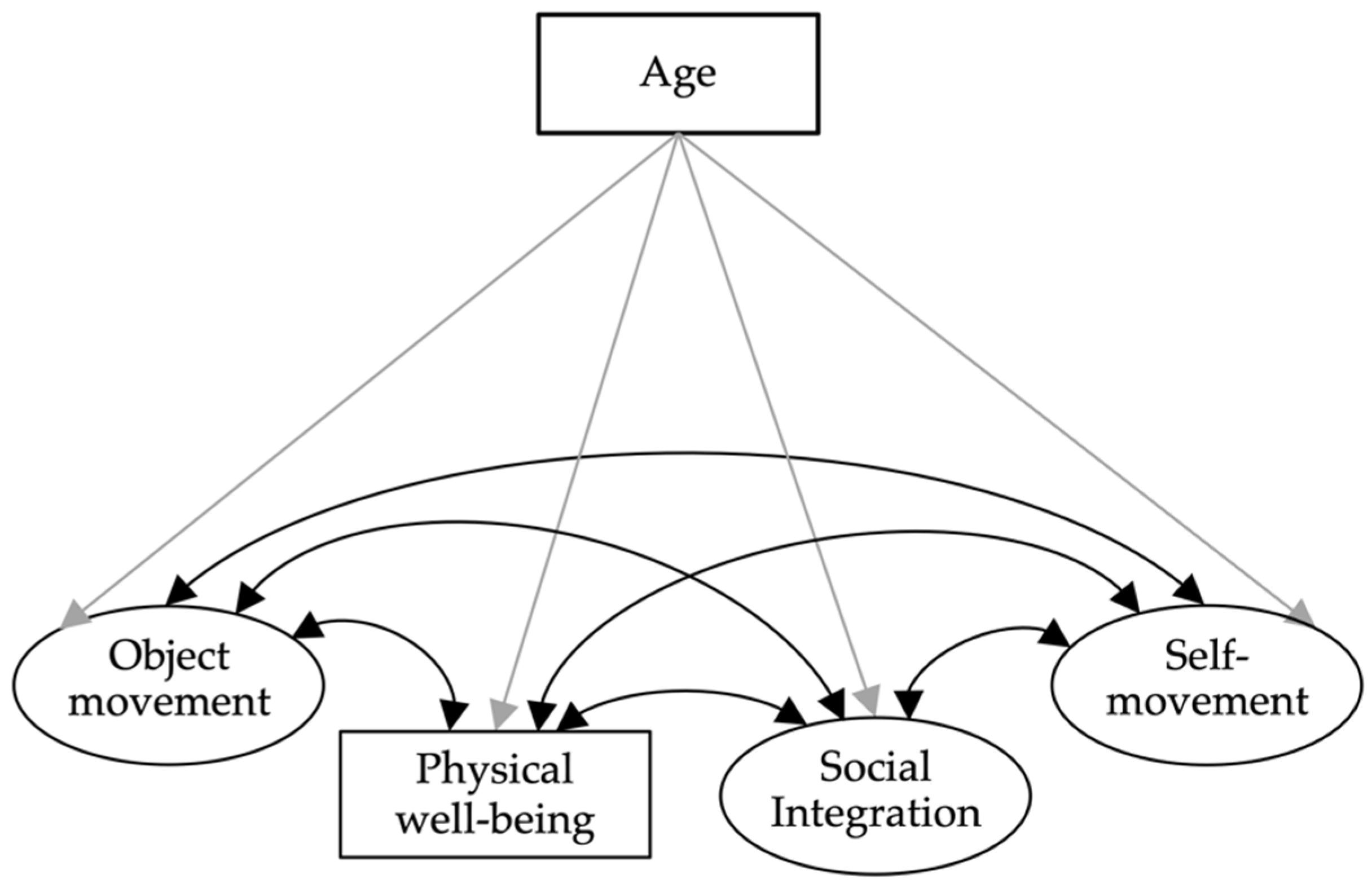
Latent Structural Equation Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrmann, C. MOBAK 1-4: Test Zur Erfassung Motorischer Basiskompetenzen Für Die Klassen 1-4; Hogrefe Schultests: Göttingen, Germany, 2018. [Google Scholar]
- Hulteen, R.M.; Morgan, P.J.; Barnett, L.M.; Stodden, D.F.; Lubans, D.R. Development of Foundational Movement Skills: A Conceptual Model for Physical Activity Across the Lifespan. Sports Med. 2018, 48, 1533–1540. [Google Scholar] [CrossRef] [PubMed]
- Chambers, M.W.; Sudgen, D.A. Early Years Movement Skills: Description, Diagnosis and Intervention; Wiley Publishers Limited: West Sussex, UK, 2006. [Google Scholar]
- Gallahue, D.L.; Ozmun, J.C. Motor Development: A Theoretical Model. Understanding Motor Development: Infants, Children, Adolescents, Adults, 6th ed.; McGraw-Hill: New York, NY, USA, 2006. [Google Scholar]
- Bildungsdirektion des Kantons Zürich. Lehrplan 21 für die Volksschule. Broschüre Bewegung und Sport; Bildungsdirektion des Kantons Zürich: Zurich, Switzerland, 2017. [Google Scholar]
- World Health Organization. Life Skills Education for Children and Adolescents in Schools. Introduction and Guidelines to Facilitate the Development and Implementation of Life Skills Programmes; World Health Organization: Geneva, Switzerland, 1994.
- Bildungsdirektion des Kantons Zürich. Lehrplan 21 für die Volksschule. Gesamtausgabe; Bildungsdirektion des Kantons Zürich: Zürich, Switzerland, 2017. [Google Scholar]
- Rubin, K.H.; Schulz Begle, A.; McDonald, K.L. Peer Relations and Social Competence in Childhood. In Developmental Social Neuroscience and Childhood Brain Insult; Beauchamp, M.H., Anderson, V., Eds.; Guilford Press: New York, NY, USA, 2012; ISBN 978-1-4625-0429-9. [Google Scholar]
- Opstoel, K.; Chapelle, L.; Prins, F.J.; De Meester, A.; Haerens, L.; van Tartwijk, J.; De Martelaer, K. Personal and Social Development in Physical Education and Sports: A Review Study. Eur. Phys. Educ. Rev. 2020, 26, 797–813. [Google Scholar] [CrossRef] [Green Version]
- Stanton-Chapman, T.L. Promoting Positive Peer Interactions in the Preschool Classroom: The Role and the Responsibility of the Teacher in Supporting Children’s Sociodramatic Play. Early Child. Educ. J. 2015, 43, 99–107. [Google Scholar] [CrossRef]
- Xiao, S.X.; Hanish, L.D.; Malouf, L.M.; Martin, C.L.; Lecheile, B.; Goble, P.; Fabes, R.A.; DeLay, D.; Bryce, C.I. Preschoolers’ Interactions with Other-Gender Peers Promote Prosocial Behavior and Reduce Aggression: An Examination of the Buddy Up Intervention. Early Child. Res. Q. 2022, 60, 403–413. [Google Scholar] [CrossRef]
- Siegler, R.; Eisenberg, N.; DeLoache, J.; Saffran, J. Beziehungen Zu Gleichaltrigen. In Enwicklungspsychologie im Kindes-und Jugendalter; Siegler, R., Eisenberg, N., DeLoache, J., Saffran, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 483–527. [Google Scholar]
- Martin, C.L.; Kornienko, O.; Schaefer, D.R.; Hanish, L.D.; Fabes, R.A.; Goble, P. The Role of Sex of Peers and Gender-Typed Activities in Young Children’s Peer Affiliative Networks: A Longitudinal Analysis of Selection and Influence. Child Dev. 2013, 84, 921–937. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.J.; Rudolph, K.D. A Review of Sex Differences in Peer Relationship Processes: Potential Trade-Offs for the Emotional and Behavioral Development of Girls and Boys. Psychol. Bull. 2006, 132, 98–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venetz, M.; Zurbriggen, C.L.A.; Schwab, S. What Do Teachers Think About Their Students’ Inclusion? Consistency of Students’ Self-Reports and Teacher Ratings. Front. Psychol. 2019, 10, 1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, C.; Bretz, K.; Kühnis, J.; Seelig, H.; Keller, R.; Ferrari, I. Connection between Social Relationships and Basic Motor Competencies in Early Childhood. Children 2021, 8, 53. [Google Scholar] [CrossRef]
- Livesey, D.; Lum Mow, M.; Toshack, T.; Zheng, Y. The Relationship between Motor Performance and Peer Relations in 9- to 12-Year-Old Children. Child Care Health Dev. 2011, 37, 581–588. [Google Scholar] [CrossRef]
- Mancini, V.O.; Rigoli, D.; Cairney, J.; Roberts, L.D.; Piek, J.P. The Elaborated Environmental Stress Hypothesis as a Framework for Understanding the Association Between Motor Skills and Internalizing Problems: A Mini-Review. Front. Psychol. 2016, 7, 239. [Google Scholar] [CrossRef]
- Lezhnieva, N.; Fredriksen, P.M.; Bekkhus, M. Peer Relationships and Quality of Life in 11–12-Year-Old Children: The Health Oriented Pedagogical Project (HOPP). Scand. J. Public Health 2018, 46, 74–81. [Google Scholar] [CrossRef] [PubMed]
- The World Health Organization Quality of Life Assessment (WHOQOL): Position Paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [CrossRef]
- Solans, M.; Pane, S.; Estrada, M.-D.; Serra-Sutton, V.; Berra, S.; Herdman, M.; Alonso, J.; Rajmil, L. Health-Related Quality of Life Measurement in Children and Adolescents: A Systematic Review of Generic and Disease-Specific Instruments. Value Health 2008, 11, 742–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravens-Sieberer, U.; Gosch, A.; Abel, T.; Auquier, P.; Bellach, B.M.; Bruil, J.; Dür, W.; Power, M.; Rajmil, L.; European KIDSCREEN Group. Quality of Life in Children and Adolescents: A European Public Health Perspective. Soz. Prav. 2001, 46, 294–302. [Google Scholar] [CrossRef]
- Barthel, D.; Ravens-Sieberer, U.; Nolte, S.; Thyen, U.; Klein, M.; Walter, O.; Meyrose, A.-K.; Rose, M.; Otto, C. Predictors of Health-Related Quality of Life in Chronically Ill Children and Adolescents over Time. J. Psychosom. Res. 2018, 109, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Tébar, A.; Ruiz-Hermosa, A.; Martínez-Vizcaíno, V.; Martín-Espinosa, N.M.; Notario-Pacheco, B.; Sánchez-López, M. Health-Related Quality of Life in Developmental Coordination Disorder and Typical Developing Children. Res. Dev. Disabil. 2021, 119, 104087. [Google Scholar] [CrossRef]
- Goswami, H. Social Relationships and Children’s Subjective Well-Being. Soc. Indic. Res. 2012, 107, 575–588. [Google Scholar] [CrossRef]
- Redondo-Tébar, A.; Fatouros, I.G.; Martinez-Vizcaino, V.; Ruíz-Hermosa, A.; Notario-Pacheco, B.; Sanchez-Lopez, M. Association between Gross Motor Competence and Health-Related Quality of Life in (Pre)Schoolchildren: The Mediating Role of Cardiorespiratory Fitness. Phys. Educ. Sport Pedagog. 2021, 26, 51–64. [Google Scholar] [CrossRef]
- Masini, A.; Gori, D.; Marini, S.; Lanari, M.; Scrimaglia, S.; Esposito, F.; Campa, F.; Grigoletto, A.; Ceciliani, A.; Toselli, S.; et al. The Determinants of Health-Related Quality of Life in a Sample of Primary School Children: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3251. [Google Scholar] [CrossRef]
- Kennedy-Behr, A.; Rodger, S.; Mickan, S. Play or Hard Work: Unpacking Well-Being at Preschool. Res. Dev. Disabil. 2015, 38, 30–38. [Google Scholar] [CrossRef]
- Cairney, J.; Rigoli, D.; Piek, J. Developmental Coordination Disorder and Internalizing Problems in Children: The Environmental Stress Hypothesis Elaborated. Dev. Rev. 2013, 33, 224–238. [Google Scholar] [CrossRef]
- Katagiri, M.; Ito, H.; Murayama, Y.; Hamada, M.; Nakajima, S.; Takayanagi, N.; Uemiya, A.; Myogan, M.; Nakai, A.; Tsujii, M. Fine and Gross Motor Skills Predict Later Psychosocial Maladaptation and Academic Achievement. Brain Dev. 2021, 43, 605–615. [Google Scholar] [CrossRef] [PubMed]
- Giske, R.; Ugelstad, I.; Meland, A.T.; Kaltvedt, E.; Eikeland, S.; Tonnessen, F.; Reikerås, E. Toddlers’ Social Competence, Play, Movement Skills and Well-Being: An Analysis of Their Relationship Based on Authentic Assessment in Kindergarten. Eur. Early Child. Educ. Res. J. 2018, 26, 362–374. [Google Scholar] [CrossRef]
- Herrmann, C.; Ferrari, I.; Wälti, M.; Wacker, S.; Kühnis, J. MOBAK-KG: Motorische Basiskompetenzen Im Kindergarten: Testmanual, 3rd ed.; Pädagogische Hochschule Zürich: Zurich, Switzerland, 2020. [Google Scholar] [CrossRef]
- Herrmann, C.; Gerlach, E.; Seelig, H. Motorische Basiskompetenzen in der Grundschule. Sportwissenschaft 2016, 46, 60–73. [Google Scholar] [CrossRef]
- Herrmann, C.; Heim, C.; Seelig, H. Construct and Correlates of Basic Motor Competencies in Primary School-Aged Children. J. Sport Health Sci. 2019, 8, 63–70. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; Mc-Graw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Robitail, S.; Ravens-Sieberer, U.; Simeoni, M.-C.; Rajmil, L.; Bruil, J.; Power, M.; Duer, W.; Cloetta, B.; Czemy, L.; Mazur, J.; et al. Testing the Structural and Cross-Cultural Validity of the KIDSCREEN-27 Quality of Life Questionnaire. Qual. Life Res. 2007, 16, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U. The Kidscreen Questionnaires: Quality of Life Questionnaires for Children and Adolescents: Handbook, 3rd ed.; Pabst Science Publishers: Lengerich, Germany, 2016; ISBN 3-89967-334-4. [Google Scholar]
- IBM Corp. IBM SPSS Statistics, Version 28; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide: Statistical Analysis with Latent Variables, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2002; ISBN 978-0-7619-1904-9. [Google Scholar]
- Dimitrov, D. Comparing Groups on Latent Variables: A Structural Equation Modeling Approach. Work 2006, 26, 429–436. [Google Scholar]
- Geiser, C. Datenanalyse Mit Mplus: Eine Anwendungsorientierte Einführung; Springer: Wiesbaden, Germany, 2011; ISBN 978-3-531-18002-1. [Google Scholar]
- Widaman, K.F.; Reise, S.P. Exploring the Measurement Invariance of Psychological Instruments: Applications in the Substance Use Domain. In The science of prevention; Bryant, K.J., Windle, M.T., West, S.G., Eds.; American Psychological Association: Washington, DC, USA, 1997; pp. 281–324. ISBN 1-55798-439-5. [Google Scholar]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Peterson, R.A.; Brown, S.P. On the Use of Beta Coefficients in Meta-Analysis. J. Appl. Psychol. 2005, 90, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Urban, D.; Mayerl, J. Strukturgleichungsmodellierung: Ein Ratgeber Für Die Praxis; Springer: Wiesbaden, Germany, 2014; ISBN 978-3-658-01919-8. [Google Scholar]
- Michel, G.; Bisegger, C.; Fuhr, D.C.; Abel, T. The KIDSCREEN group Age and Gender Differences in Health-Related Quality of Life of Children and Adolescents in Europe: A Multilevel Analysis. Qual. Life Res. 2009, 18, 1147. [Google Scholar] [CrossRef]
- Wuang, Y.-P.; Wang, C.-C.; Huang, M.-H. Health-Related Quality of Life in Children with Developmental Coordination Disorder and Their Parents. OTJR Occup. Particip. Health 2012, 32, 142–150. [Google Scholar] [CrossRef]
- Karras, H.C.; Morin, D.N.; Gill, K.; Izadi-Najafabadi, S.; Zwicker, J.G. Health-Related Quality of Life of Children with Developmental Coordination Disorder. Res. Dev. Disabil. 2019, 84, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Erhart, M.; Rajmil, L.; Herdman, M.; Auquier, P.; Bruil, J.; Power, M.; Duer, W.; Abel, T.; Czemy, L.; et al. Reliability, Construct and Criterion Validity of the KIDSCREEN-10 Score: A Short Measure for Children and Adolescents’ Well-Being and Health-Related Quality of Life. Qual. Life Res. 2010, 19, 1487–1500. [Google Scholar] [CrossRef] [Green Version]
- Rajmil, L.; Herdman, M.; Ravens-Sieberer, U.; Erhart, M.; Alonso, J.; The European KIDSCREEN Group. Socioeconomic Inequalities in Mental Health and Health-Related Quality of Life (HRQOL) in Children and Adolescents from 11 European Countries. Int. J. Public Health 2014, 59, 95–105. [Google Scholar] [CrossRef]
- Gramespacher, E.; Herrmann, C.; Ennigkeit, F.; Heim, C.; Seelig, H. Geschlechtsspezifische Sportsozialisation Als Prädiktor Motorischer Basiskompetenzen–Ein Mediationsmodell. Motorik 2020, 43, 69–77. [Google Scholar] [CrossRef]
- Kress, J.; Seelig, H.; Bretz, K.; Ferrari, I.; Keller, R.; Kühnis, J.; Storni, S.; Herrmann, C. Associations between Basic Motor Competencies, Club Sport Participation, and Social Relationships among Primary School Children. CISS 2022. (submitted). [Google Scholar]



{kind=link}
{kind=link}
| MOBAK-KG | MOBAK-1-2 | |
|---|---|---|
| Object movement | ||
| Throwing | The child throws six juggling balls at a target of 1.1 m height from a distance of 1.5 m with overhead throws. | The child throws six juggling balls at a target of 1.3 m height from a distance of 2.0 m. |
| Catching | The tester drops a small basketball to the ground from a height of 1.5 m so that the ball bounces back up at least 1.1 m from the ground. The child catches the ball after it has reached the highest point. | The tester drops a small ball to the ground from a height of 2.0 m so that the ball bounces back up at least 1.3 m from the ground. The child catches the ball after it has reached the highest point. |
| Bouncing | The child bounces a small volleyball with both hands and catches it again without losing the ball. | The child bounces a small basketball through a marked corridor (5.0 × 1.0 m) without losing the ball. |
| Dribbling | The child dribbles a futsal ball through a marked corridor (2.8 × 9.0 m) around two obstacles without stopping or losing the ball. | The child dribbles a futsal ball through a marked corridor (5.0 × 1.0 m) without losing the ball. |
| Self-movement | ||
| Balancing | The child walks across an overturned long bench without stepping off the bench. | The child walks across an overturned see-sawing long bench without stepping off the bench. |
| Rolling | The child performs a forward roll down an inclined mat and is able to land fluently in a standing position on his/her feet. | The child performs a forward roll on a mat and is able to land fluently in a standing position on his/her feet. |
| Jumping | The child jumps a distance of 3.0 m on one foot, turns around, and jumps back 3.0 m on the other foot. | The child jumps between and beneath carpet tiles fluently with one leg between the tiles and with straddled legs beneath the tiles. |
| Running | The child runs forward along a corridor (0.6 m × 4.0 m) to a wall, touches it with his/her hand, and then runs back backwards. | The child moves sideways from one cone to another placed at a distance of 3 m from each other. |
| Preschool | Primary School | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | Boys | Girls | Overall | Boys | Girls | |||||
| M [95% CI] | ICC | M [95% CI] | M [95% CI] | d | M [95% CI] | ICC | M [95% CI] | M [95% CI] | d | |
| Object movement a | 4.0 [3.8; 4.1] | 0.02 | 4.4 [4.2; 4.5] | 3.5 [3.4; 3.7] | 0.42 | 5.5 [5.4; 5.6] | 0.12 | 5.9 [5.7; 6.0] | 5.1 [5.0; 5.3] | 0.43 |
| Self-movement a | 4.5 [4.4; 4.7] | 0.05 | 4.3 [4.1; 4.5] | 4.8 [4.6; 5.0] | 0.21 | 4.9 [4.8; 5.1] | 0.14 | 4.8 [4.6; 5.0] | 5.1 [4.9; 5.3] | 0.14 |
| Social integration a | 13.5 [13.4; 13.7] | 0.19 | 13.4 [13.2; 13.5] | 13.7 [13.6; 13.9] | 0.17 | 13.7 [13.6; 13.8] | 0.25 | 13.5 [13.3; 13.8] | 13.9 [13.7; 14.1] | 0.15 |
| General HRQoL sum score b | 41.5 [41.2; 41.7] | 0.04 | 41.4 [41.1; 41.8] | 41.5 [41.1; 41.8] | 0.004 | 41.2 [40.9; 41.5] | 0.03 | 40.8 [40.4; 41.2] | 41.5 [41.2; 41.9] | 0.18 |
| General HRQoL t-value 1,b | 51.9 [51.4; 52.4] | 0.02 | 51.8 [51.1; 52.5] | 51.9 [51.2; 52.7] | 0.02 | 51.7 [51.1; 52.2] | 0.02 | 51.1 [50.3; 51.8] | 52.3 [51.5; 53.1] | 0.15 |
| Physical well-being sum score c | 21.9 [21.7; 22.2] | 0.04 | 22.3 [21.9; 22.6] | 21.6 [21.1; 22.0] | 0.27 | |||||
| Physical well-being t-value 1,c | 53.2 [52.6; 53.8] | 0.003 | 54.1 [53.3; 54.8] | 52.2 [51.3; 53.1] | 0.33 | |||||
| Model | Analysis | Sample | n | χ2 | df | p | CFI | RMSEA |
|---|---|---|---|---|---|---|---|---|
| 1a | MIMIC | SS 1 preschool | 943 | 115.947 | 69 | <0.001 | 0.961 | 0.027 |
| 1b | MIMIC | SS 1 primary school | 880 | 92.865 | 69 | 0.029 | 0.967 | 0.020 |
| 2a | MGM | SS 1 preschool | 943 | 201.069 | 160 | 0.015 | 0.971 | 0.023 |
| 2b | MGM | SS 1 primary school | 880 | 180.123 | 160 | 0.132 | 0.977 | 0.017 |
| 3 | MIMIC | SS 2 preschool | 384 | 88.459 | 69 | 0.057 | 0.962 | 0.027 |
| 4 | MGM | SS 2 preschool | 384 | 175.645 | 160 | 0.188 | 0.971 | 0.023 |
| Factors | Preschool (Model 1a) | Primary School (Model 1b) | ||||||
|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (1) | (2) | (3) | (4) | |
| (1) Object movement | ||||||||
| (2) Self-movement | 0.74 *** | 0.56 *** | ||||||
| (3) Social integration | 0.27 *** | 0.26 *** | 0.22 *** | 0.18 ** | ||||
| (4) General HRQoL | 0.01 | 0.04 | 0.04 | 0.003 | 0.14 ** | 0.13 *** | ||
| (5) Age | 0.59 *** | 0.47 *** | 0.15 *** | −0.01 | 0.49 *** | 0.33 *** | 0.10 | <0.01 |
| Factors | Preschool (Model 2a) | Primary School (Model 2b) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (1) | (2) | (3) | (4) | (5) | |
| (1) Object movement | 0.85 *** | 0.34 *** | −0.01 | 0.53 *** | 0.64 *** | 0.21 ** | 0.11 | 0.44 *** | ||
| (2) Self-movement | 0.84 *** | 0.22 * | 0.01 | 0.44 *** | 0.68 *** | 0.12 | 0.12 | 0.26 *** | ||
| (3) Social integration | 0.26 *** | 0.27 *** | 0.07 | 0.15 *** | 0.32 *** | 0.24 ** | 0.16 ** | 0.09 | ||
| (4) General HRQoL | 0.06 | 0.05 | 0.01 | −0.02 | −0.03 | 0.18 ** | 0.10 | −0.001 | ||
| (5) Age | 0.71 *** | 0.52 *** | 0.15 *** | −0.02 | 0.58 *** | 0.44 *** | 0.10 | −0.001 | ||
| Factors | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| (1) Object movement | ||||
| (2) Self-movement | 0.79 *** | |||
| (3) Social integration | 0.29 *** | 0.40 *** | ||
| (4) Physical well-being | 0.20 ** | 0.29 *** | 0.07 | |
| (5) Age | 0.54 *** | 0.39 *** | 0.17 ** | −0.04 |
| Factors | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (1) | (2) | (3) | (4) | |
| (1) Object movement | ||||||||
| (2) Self-movement | 0.83 *** | 0.88 *** | ||||||
| (3) Social integration | 0.40 *** | 0.26 ** | 0.24 ** | 0.48 *** | ||||
| (4) Physical well-being | 0.21 ** | 0.35 *** | 0.05 | 0.15 | 0.34 ** | 0.18 | ||
| (5) Age | 0.45 *** | 0.29 *** | 0.19 *** | −0.05 | 0.68 *** | 0.58 *** | 0.20 *** | −0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bretz, K.; Seelig, H.; Ferrari, I.; Keller, R.; Kühnis, J.; Storni, S.; Herrmann, C. Basic Motor Competencies of (Pre)School Children: The Role of Social Integration and Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 14537. https://doi.org/10.3390/ijerph192114537
Bretz K, Seelig H, Ferrari I, Keller R, Kühnis J, Storni S, Herrmann C. Basic Motor Competencies of (Pre)School Children: The Role of Social Integration and Health-Related Quality of Life. International Journal of Environmental Research and Public Health. 2022; 19(21):14537. https://doi.org/10.3390/ijerph192114537
Chicago/Turabian StyleBretz, Kathrin, Harald Seelig, Ilaria Ferrari, Roger Keller, Jürgen Kühnis, Simone Storni, and Christian Herrmann. 2022. "Basic Motor Competencies of (Pre)School Children: The Role of Social Integration and Health-Related Quality of Life" International Journal of Environmental Research and Public Health 19, no. 21: 14537. https://doi.org/10.3390/ijerph192114537