
An Internet-Based Multi-Approach Intervention Targeting University Students Suffering from Psychological Problems: Design, Implementation, and Evaluation





 ,
, 


 , , ,
, , ,  and
and 
Abstract
:1. Introduction
Aims and Hypotheses
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Pilot Study Design
Feasibility Measures
- ❖
- ❖
- ❖
- Adherence rates for each lesson and the overall program.
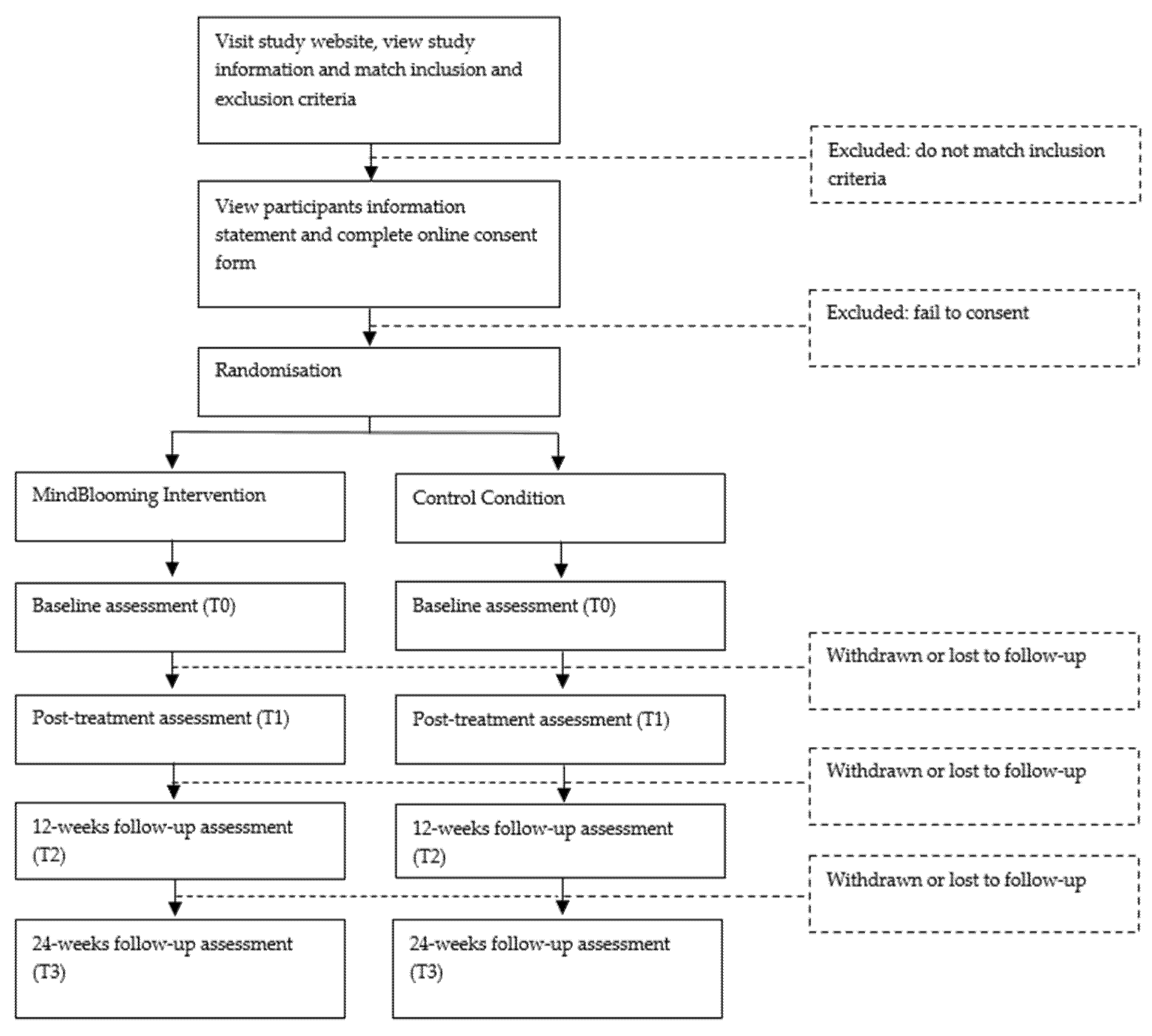
2.3. RCT Design
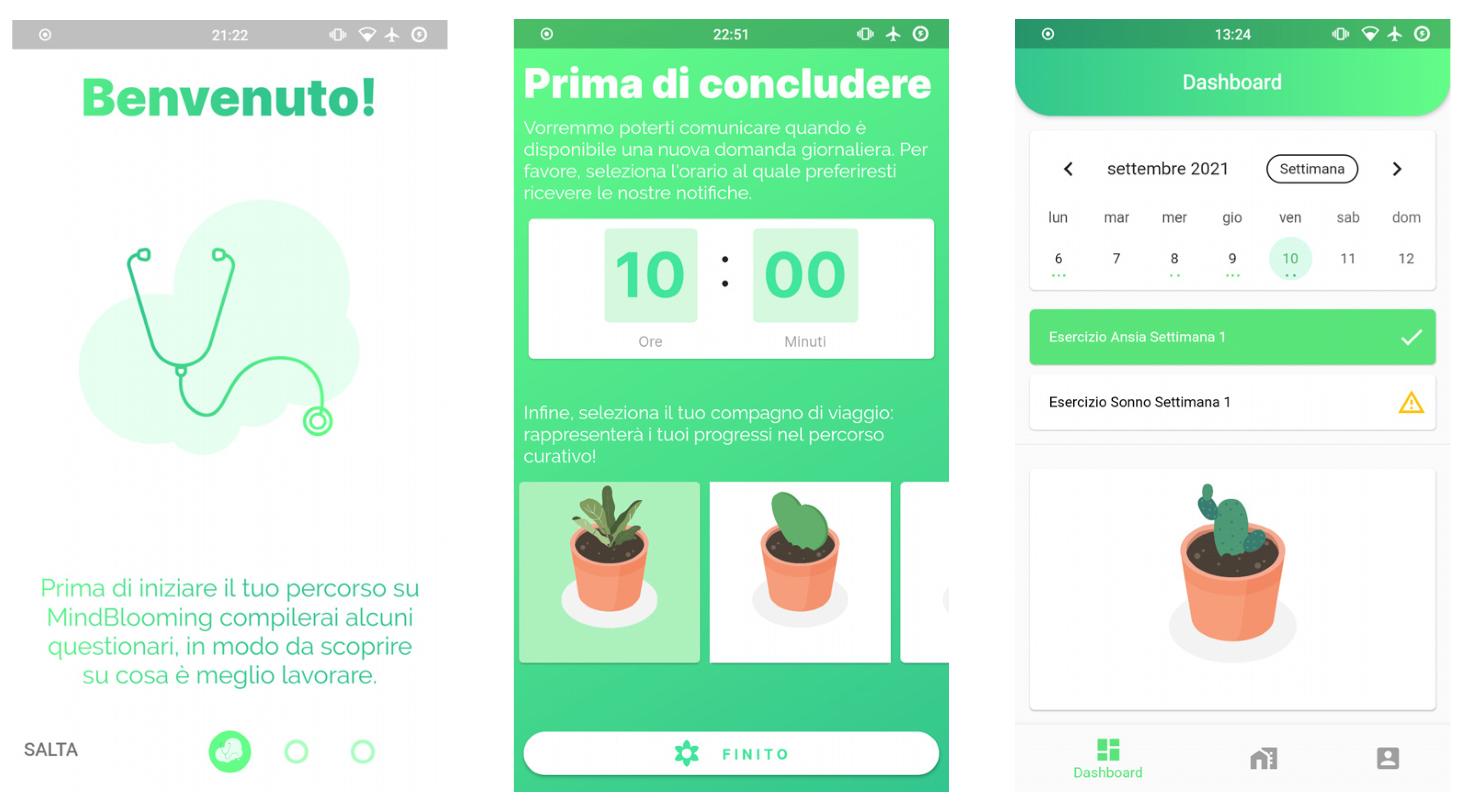
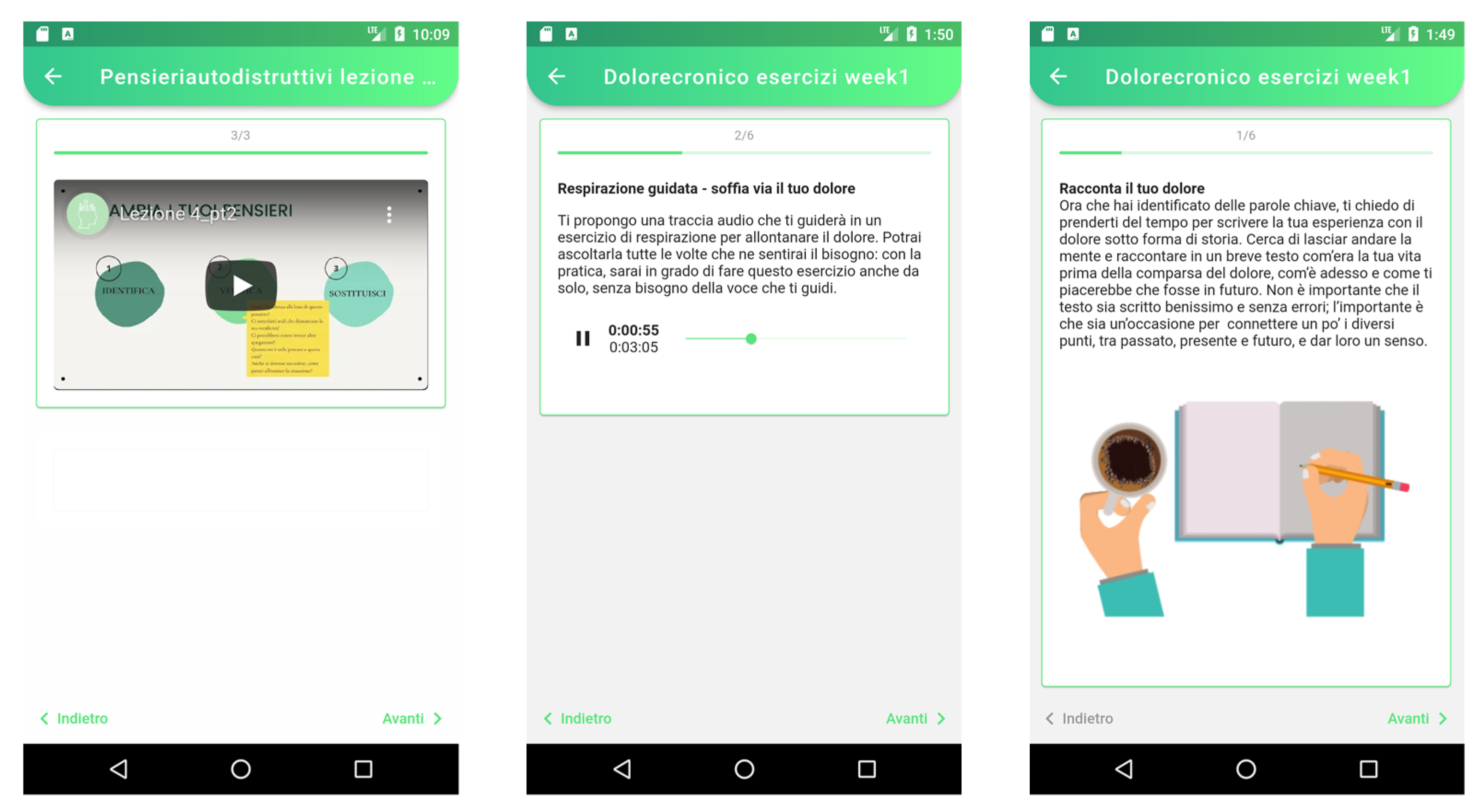
2.4. Intervention
- ○
- 1st week: module 1 and 2 sessions;
- ○
- 2nd week: module 1 and 2 sessions;
- ○
- 3rd week: module 1 and 2 sessions;
- ○
- 4th week: module 1 and 2 sessions;
- ○
- 5th week: module 1 and 2 sessions;
- ○
- 6th week: relational problems related to difficulties in emotion regulation and empathy deficits session;
- ○
- 7th week: module 1 and 2 sessions about relapse prevention, future planning by reflecting on how to attain goals and implement behavioral changes, orientation, and conclusion.
2.5. Control Condition
2.6. Outcome Measures
2.6.1. Primary Outcome Measures
- ❖
- Beck Depression Inventory (BDI-II) [58,59], composed of 21 items investigating depressive symptoms (see Supplementary File S1 for a thorough description of the scales).
- ❖
- ❖
- ❖
- Brief version of the Columbia-Suicide Severity Rating Scale (C-SSRS) [64] modified, consisting of 4 items investigating current suicide risk and 5 items investigating lifetime risk.
- ❖
- ❖
- ❖
- ❖
- World Health Organization Quality of Life—short version (WHOQOL-BREF) [73], consisting of 26 items investigating the quality of life.
2.6.2. Secondary Outcome Measures
- ❖
- Visual Analogue Scales (VAS) for psychological and physical pain (6 items) [32].
- ❖
- Insomnia Severity Index (ISI) to investigate the impact of insomnia in the last two weeks (7 items) [74].
- ❖
- ❖
- ❖
- Life Events Checklist (LEC) [79], composed of 16 items investigating the subject’s stressful experiences.
- ❖
- Reasons for Living Inventory (RFLI) [80], consisting of 48 items investigating the subject’s reasons for living.
- ❖
- COVID-19-related questions compiled according to the International Association for Suicide Prevention (IASP) guidelines for suicide prevention research [56].
2.7. Sample Size Calculation
2.8. Statistical Methods
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Di Consiglio, M.; Merola, S.; Pascucci, T.; Violani, C.; Couyoumdjian, A. The Impact of COVID-19 Pandemic on Italian University Students’ Mental Health: Changes across the Waves. Int. J. Environ. Res. Public Health 2021, 18, 9897. [Google Scholar] [CrossRef] [PubMed]
- Herrero, R.; Mira, A.; Cormo, G.; Etchemendy, E.; Baños, R.; García-Palacios, A.; Ebert, D.D.; Franke, M.; Berger, T.; Schaub, M.P.; et al. An Internet Based Intervention for Improving Resilience and Coping Strategies in University Students: Study Protocol for a Randomized Controlled Trial. Internet Interv. 2019, 16, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Adamo, S.; Irene, S.; Emanuele, P.; Rosaria, F.M.; Antonio, P. Brief Psychodynamic Counselling in a University Setting. Procedia-Soc. Behav. Sci. 2010, 5, 1151–1159. [Google Scholar]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. WHO World Mental Health Surveys International College Student Project: Prevalence and Distribution of Mental Disorders. J. Abnorm. Psychol. 2018, 127, 623. [Google Scholar] [CrossRef] [PubMed]
- Oswalt, S.B.; Lederer, A.M.; Chestnut-Steich, K.; Day, C.; Halbritter, A.; Ortiz, D. Trends in College Students’ Mental Health Diagnoses and Utilization of Services, 2009–2015. J. Am. Coll. Health 2020, 68, 41–51. [Google Scholar] [CrossRef]
- Mortier, P.; Cuijpers, P.; Kiekens, G.; Auerbach, R.P.; Demyttenaere, K.; Green, J.G.; Kessler, R.C.; Nock, M.K.; Bruffaerts, R. The Prevalence of Suicidal Thoughts and Behaviours among College Students: A Meta-Analysis. Psychol. Med. 2018, 48, 554–565. [Google Scholar] [CrossRef]
- Rosales-Ricardo, Y.; Rizzo-Chunga, F.; Mocha-Bonilla, J.; Ferreira, J.P. Prevalence of Burnout Syndrome in University Students: A Systematic Review. Salud Ment. 2021, 44, 91–102. [Google Scholar] [CrossRef]
- Sivertsen, B.; Råkil, H.; Munkvik, E.; Lønning, K.J. Cohort Profile: The SHoT-Study, a National Health and Well-Being Survey of Norwegian University Students. BMJ Open 2019, 9, e025200. [Google Scholar] [CrossRef] [Green Version]
- Storrie, K.; Ahern, K.; Tuckett, A. A Systematic Review: Students with Mental Health Problems—A Growing Problem. Int. J. Nurs. Pract. 2010, 16, 1–6. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion Regulation: Affective, Cognitive, and Social Consequences. Psychophysiology 2002, 39, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Cacioppo, J.T.; Hawkley, L.C. Social Isolation and Health, with an Emphasis on Underlying Mechanisms. Perspect. Biol. Med. 2003, 46, S39–S52. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Majeed, A.; Gill, H.; Tamura, J.; Ho, R.C.; Mansur, R.B.; Nasri, F.; Lee, Y.; Rosenblat, J.D.; Wong, E.; et al. The Effect of Loneliness on Distinct Health Outcomes: A Comprehensive Review and Meta-Analysis. Psychiatry Res. 2020, 294, 113514. [Google Scholar] [CrossRef] [PubMed]
- Cludius, B.; Mennin, D.; Ehring, T. Emotion Regulation as a Transdiagnostic Process. Emotion 2020, 20, 37. [Google Scholar] [CrossRef] [PubMed]
- Ishii, T.; Tachikawa, H.; Shiratori, Y.; Hori, T.; Aiba, M.; Kuga, K.; Arai, T. What Kinds of Factors Affect the Academic Outcomes of University Students with Mental Disorders? A Retrospective Study Based on Medical Records. Asian J. Psychiatry 2018, 32, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Harrer, M.; Apolinário-Hagen, J.; Baumeister, H. Digital Interventions for Mental Disorders: Key Features, Efficacy, and Potential for Artificial Intelligence Applications. In Frontiers in Psychiatry; Springer: Singapore, 2019; pp. 583–627. [Google Scholar]
- Franzoi, I.G.; D’Ovidio, F.; Costa, G.; d’Errico, A.; Granieri, A. Self-Rated Health and Psychological Distress among Emerging Adults in Italy: A Comparison between Data on University Students, Young Workers and Working Students Collected through the 2005 and 2013 National Health Surveys. Int. J. Environ. Res. Public Health 2021, 18, 6403. [Google Scholar] [CrossRef]
- Cuijpers, P.; Kleiboer, A.; Karyotaki, E.; Riper, H. Internet and Mobile Interventions for Depression: Opportunities and Challenges. Depress. Anxiety 2017, 34, 596–602. [Google Scholar] [CrossRef]
- Ebert, D.D.; Van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.L.; et al. Internet-and Mobile-Based Psychological Interventions: Applications, Efficacy, and Potential for Improving Mental Health. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Andersson, G.; Cuijpers, P.; Carlbring, P.; Riper, H.; Hedman, E. Guided Internet-based vs. Face-to-face Cognitive Behavior Therapy for Psychiatric and Somatic Disorders: A Systematic Review and Meta-analysis. World Psychiatry 2014, 13, 288–295. [Google Scholar] [CrossRef]
- Olthuis, J.V.; Watt, M.C.; Bailey, K.; Hayden, J.A.; Stewart, S.H. Therapist-supported Internet Cognitive Behavioural Therapy for Anxiety Disorders in Adults. Cochrane Database Syst. Rev. 2016, 3, CD011565. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Andersson, G. Internet-Administered Cognitive Behavior Therapy for Health Problems: A Systematic Review. J. Behav. Med. 2008, 31, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Baños, R.M.; Etchemendy, E.; Mira, A.; Riva, G.; Gaggioli, A.; Botella, C. Online Positive Interventions to Promote Well-Being and Resilience in the Adolescent Population: A Narrative Review. Front. Psychiatry 2017, 8, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, E.B.; Morriss, R.; Glazebrook, C. Computer-Delivered and Web-Based Interventions to Improve Depression, Anxiety, and Psychological Well-Being of University Students: A Systematic Review and Meta-Analysis. J. Med Internet Res. 2014, 16, e130. [Google Scholar] [CrossRef] [Green Version]
- Berrouiguet, S.; Baca-García, E.; Brandt, S.; Walter, M.; Courtet, P. Fundamentals for Future Mobile-Health (MHealth): A Systematic Review of Mobile Phone and Web-Based Text Messaging in Mental Health. J. Med. Internet Res. 2016, 18, e5066. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Adam, S.H.; Baumeister, H.; Cuijpers, P.; Karyotaki, E.; Auerbach, R.P.; Kessler, R.C.; Bruffaerts, R.; Berking, M.; Ebert, D.D. Internet Interventions for Mental Health in University Students: A Systematic Review and Meta-Analysis. Int. J. Methods Psychiatr. Res. 2019, 28, e1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunzler, A.M.; Helmreich, I.; König, J.; Chmitorz, A.; Wessa, M.; Binder, H.; Lieb, K. Psychological Interventions to Foster Resilience in Healthcare Students. Cochrane Database Syst. Rev. 2020, 7, CD013684. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekar, P. Do Mental Health Mobile Apps Work: Evidence and Recommendations for Designing High-Efficacy Mental Health Mobile Apps. Mhealth 2018, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Wilks, C.R.; Lungu, A.; Ang, S.Y.; Matsumiya, B.; Yin, Q.; Linehan, M.M. A Randomized Controlled Trial of an Internet Delivered Dialectical Behavior Therapy Skills Training for Suicidal and Heavy Episodic Drinkers. J. Affect. Disord. 2018, 232, 219–228. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H. Review of Randomised Controlled Trials of Internet Interventions for Mental Disorders and Related Conditions. Clin. Psychol. 2006, 10, 16–29. [Google Scholar] [CrossRef]
- Design. Available online: https://material.io/design (accessed on 10 September 2021).
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of Client/Patient Satisfaction: Development of a General Scale. Eval. Program Plan. 1979, 2, 197–207. [Google Scholar] [CrossRef]
- Olié, E.; Guillaume, S.; Jaussent, I.; Courtet, P.; Jollant, F. Higher Psychological Pain during a Major Depressive Episode May Be a Factor of Vulnerability to Suicidal Ideation and Act. J. Affect. Disord. 2010, 120, 226–230. [Google Scholar] [CrossRef]
- Brooke, J. SUS-A Quick and Dirty Usability Scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D.; The CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T. Thinking and Depression: II. Theory and Therapy. Arch. Gen. Psychiatry 1964, 10, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change; Guilford Press: New York, NY, USA, 2011; ISBN 1-60918-962-0. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Irving, J.A.; Segal, Z.V. Mindfulness-Based Cognitive Therapy: Current Status and Future Applications. Sante Ment. Que. 2013, 38, 65–82. [Google Scholar] [CrossRef] [Green Version]
- Kabat-Zinn, J. An Outpatient Program in Behavioral Medicine for Chronic Pain Patients Based on the Practice of Mindfulness Meditation: Theoretical Considerations and Preliminary Results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Linehan, M. Skills Training Manual for Treating Borderline Personality Disorder; Guilford Press: New York, NY, USA, 1993; Volume 29. [Google Scholar]
- Taskforce, A.P. Evidence Based Practice in Psychology: APA Presidential Taskforce on Evidence Based Practice. Am. Psychol. 2006, 61, 271–285. [Google Scholar]
- Klerman, G.L.; Weissman, M.M. Interpersonal Psychotherapy of Depression: A Brief, Focused, Specific Strategy; Jason Aronson, Incorporated: Lanham, MD, USA, 1994; ISBN 1-4616-2900-4. [Google Scholar]
- Beck, J.S. Cognitive Behavior Therapy: Basics and Beyond; The Guilford Press: New York, NY, USA, 2011; ISBN 1609185048. [Google Scholar]
- Simos, G.; Hofmann, S.G. CBT for Anxiety Disorders: A Practitioner Book; John Wiley & Sons: Hoboken, NJ, USA, 2013; ISBN 1-118-31676-2. [Google Scholar]
- Morin, C.M.; Bootzin, R.R.; Buysse, D.J.; Edinger, J.D.; Espie, C.A.; Lichstein, K.L. Psychological and Behavioral Treatment of Insomnia: Update of the Recent Evidence (1998–2004). Sleep 2006, 29, 1398–1414. [Google Scholar] [CrossRef]
- Sharma, M.P.; Andrade, C. Behavioral Interventions for Insomnia: Theory and Practice. Indian J. Psychiatry 2012, 54, 359. [Google Scholar] [CrossRef]
- Hoffman, J.E.; Taylor, K.; Manber, R.; Trockel, M.; Gehrman, P.; Woodward, S.; Ruzek, J.I. CBT-i Coach; Version 1.0; Mobile Application Software; US Department of Veterans Affairs: Washington, DC, USA, 2013. [Google Scholar]
- Edinger, J.D.; Carney, C.E. Overcoming Insomnia: A Cognitive-Behavioral Therapy Approach, Therapist Guide; Oxford University Press: Oxford, UK, 2014; ISBN 0-19-933939-2. [Google Scholar]
- Jacobson, E. Progressive Relaxation; Midway Reprint; The University of Chicago Press: Chicago, IL, USA, 1974. [Google Scholar]
- Lichstein, K.L.; Riedel, B.W.; Wilson, N.M.; Lester, K.W.; Aguillard, R.N. Relaxation and Sleep Compression for Late-Life Insomnia: A Placebo-Controlled Trial. J. Consult. Clin. Psychol. 2001, 69, 227. [Google Scholar] [CrossRef]
- Bryan, C.J.; Rudd, M.D. Brief Cognitive-Behavioral Therapy for Suicide Prevention; Guilford Publications: New York, NY, USA, 2018; ISBN 1-4625-3666-2. [Google Scholar]
- Bryan, C.J. Cognitive Behavioral Therapy for Suicide Prevention (CBT-SP): Implications for Meeting Standard of Care Expectations with Suicidal Patients. Behav. Sci. Law 2019, 37, 247–258. [Google Scholar] [CrossRef]
- Stanley, B.; Brown, G.; Brent, D.A.; Wells, K.; Poling, K.; Curry, J.; Kennard, B.D.; Wagner, A.; Cwik, M.F.; Klomek, A.B.; et al. Cognitive-Behavioral Therapy for Suicide Prevention (CBT-SP): Treatment Model, Feasibility, and Acceptability. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 1005–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeCou, C.R.; Comtois, K.A.; Landes, S.J. Dialectical Behavior Therapy Is Effective for the Treatment of Suicidal Behavior: A Meta-Analysis. Behav. Ther. 2019, 50, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M.M.; Korslund, K.E.; Harned, M.S.; Gallop, R.J.; Lungu, A.; Neacsiu, A.D.; McDavid, J.; Comtois, K.A.; Murray-Gregory, A.M. Dialectical Behavior Therapy for High Suicide Risk in Individuals with Borderline Personality Disorder: A Randomized Clinical Trial and Component Analysis. JAMA Psychiatry 2015, 72, 475–482. [Google Scholar] [CrossRef] [PubMed]
- International Association for Suicide Prevention (ICSPRC). Advice on Questions/Survey Tools Relevant to Suicide Prevention Research in Relation to COVID-19. Available online: https://iasp.info/wp-content/uploads/ICSPRC_COVID_advice_on_questions.pdf (accessed on 5 March 2021).
- Williams Institute Data Collection Archives. Available online: https://williamsinstitute.law.ucla.edu/issues/data-collection/ (accessed on 5 March 2021).
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory (BDI-II); Pearson: London, UK, 1996; Volume 10. [Google Scholar]
- Ghisi, M.; Flebus, G.B.; Montano, A.; Sanavio, E.; Sica, C. Manuale BDI-II. Beck Depression Inventory–II; Organizzazioni Speciali, Adattamento Italiano: Firenze, Italy, 2006. [Google Scholar]
- Pedrabissi, L.; Santinello, M. Verifica Della Validità Dello STAI Forma Y Di Spielberger. Giunti Organizzazioni Speciali 1989, 191–192, 11–14. [Google Scholar]
- Spielberger, C.D. State-Trait Anxiety Inventory for Adults; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S. The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings from Three Multisite Studies with Adolescents and Adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [Green Version]
- Fiorilli, C.; Galimberti, V.; De Stasio, S.; Di Chiacchio, C.; Albanese, O. L’utilizzazione Dello School Burnout Inventory (SBI) Con Studenti Italiani Di Scuola Superiore Di Primo e Secondo Grado. Psicol. Clin. Svilupp. 2014, 18, 403–424. [Google Scholar]
- Salmela-Aro, K.; Kiuru, N.; Leskinen, E.; Nurmi, J.-E. School Burnout Inventory (SBI) Reliability and Validity. Eur. J. Psychol. Assess. 2009, 25, 48–57. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Lausi, G.; Quaglieri, A.; Burrai, J.; Mari, E.; Giannini, A.M. Development of the DERS-20 among the Italian Population: A Study for a Short Form of the Difficulties in Emotion Regulation Scale. Mediterr. J. Clin. Psychol. 2020, 8. [Google Scholar] [CrossRef]
- Davis, M.H. A Multidimensional Approach to Individual Differences in Empathy; The University of Texas: Austin, TX, USA, 1980. [Google Scholar]
- Ingoglia, S.; Lo Coco, A.; Albiero, P. Development of a Brief Form of the Interpersonal Reactivity Index (B–IRI). J. Personal. Assess. 2016, 98, 461–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caraceni, A.; Mendoza, T.R.; Mencaglia, E.; Baratella, C.; Edwards, K.; Forjaz, M.J.; Martini, C.; Serlin, R.C.; de Conno, F.; Cleeland, C.S. A Validation Study of an Italian Version of the Brief Pain Inventory (Breve Questionario per La Valutazione Del Dolore). Pain 1996, 65, 87–92. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K. The Brief Pain Inventory; The University of Texas MD Anderson Cancer Center, Pain Research Group: Houston, TX, USA, 1991; Volumes 143–147. [Google Scholar]
- WHOQOL Group. Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castronovo, V.; Galbiati, A.; Marelli, S.; Brombin, C.; Cugnata, F.; Giarolli, L.; Anelli, M.M.; Rinaldi, F.; Ferini-Strambi, L. Validation Study of the Italian Version of the Insomnia Severity Index (ISI). Neurol. Sci. 2016, 37, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The Twenty-Item Toronto Alexithymia Scale—I: Item Selection and Cross-Validation of the Factor Structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Bressi, C.; Taylor, G.; Parker, J.; Bressi, S.; Brambilla, V.; Aguglia, E.; Allegranti, I.; Bongiorno, A.; Giberti, F.; Bucca, M.; et al. Cross Validation of the Factor Structure of the 20-Item Toronto Alexithymia Scale: An Italian Multicenter Study. J. Psychosom. Res. 1996, 41, 551–559. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing Coping Strategies: A Theoretically Based Approach. J. Personal. Soc. Psychol. 1989, 56, 267. [Google Scholar] [CrossRef]
- Foà, C.; Tonarelli, A.; Caricati, L.; Fruggeri, L. COPE-NVI-25: Validazione Italiana Della Versione Ridotta Della Coping Orientation to the Problems Experienced (COPE-NVI). Psicol. Salut. 2015, 123–140. [Google Scholar] [CrossRef]
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric Properties of the Life Events Checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Linehan, M.M.; Goodstein, J.L.; Nielsen, S.L.; Chiles, J.A. Reasons for Staying Alive When You Are Thinking of Killing Yourself: The Reasons for Living Inventory. J. Consult. Clin. Psychol. 1983, 51, 276. [Google Scholar] [CrossRef] [PubMed]
- Heber, E.; Ebert, D.D.; Lehr, D.; Cuijpers, P.; Berking, M.; Nobis, S.; Riper, H. The Benefit of Web-and Computer-Based Interventions for Stress: A Systematic Review and Meta-Analysis. J. Med. Internet Res. 2017, 19, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schönbrodt, F.D.; Wagenmakers, E.-J. Bayes Factor Design Analysis: Planning for Compelling Evidence. Psychon. Bull. Rev. 2018, 25, 128–142. [Google Scholar] [CrossRef] [PubMed]
- Rouder, J.N.; Speckman, P.L.; Sun, D.; Morey, R.D.; Iverson, G. Bayesian t Tests for Accepting and Rejecting the Null Hypothesis. Psychon. Bull. Rev. 2009, 16, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Rouder, J.N.; Morey, R.D.; Speckman, P.L.; Province, J.M. Default Bayes Factors for ANOVA Designs. J. Math. Psychol. 2012, 56, 356–374. [Google Scholar] [CrossRef]
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly Jr, D.W.; Schuler, T.C. Understanding the Minimum Clinically Important Difference: A Review of Concepts and Methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning; Springer: Cham, Switzerland, 2013; Volume 112. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Module | Psychoeducation | Exercises | Approaches |
|---|---|---|---|
| Depression |
|
|
|
| Anxiety |
|
|
|
| Sleep problems |
|
|
|
| Self-disruptive thoughts |
|
|
|
| Job- and study-related stress and burnout |
|
| |
| Chronic pain |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Fabritiis, M.; Trisolini, F.; Bertuletti, G.; Fagadau, I.D.; Ginelli, D.; Lalopa, K.P.; Peverelli, L.; Pirola, A.; Sala, G.; Maisto, M.; et al. An Internet-Based Multi-Approach Intervention Targeting University Students Suffering from Psychological Problems: Design, Implementation, and Evaluation. Int. J. Environ. Res. Public Health 2022, 19, 2711. https://doi.org/10.3390/ijerph19052711
De Fabritiis M, Trisolini F, Bertuletti G, Fagadau ID, Ginelli D, Lalopa KP, Peverelli L, Pirola A, Sala G, Maisto M, et al. An Internet-Based Multi-Approach Intervention Targeting University Students Suffering from Psychological Problems: Design, Implementation, and Evaluation. International Journal of Environmental Research and Public Health. 2022; 19(5):2711. https://doi.org/10.3390/ijerph19052711
Chicago/Turabian StyleDe Fabritiis, Marlene, Federica Trisolini, Gloria Bertuletti, Ionut Daniel Fagadau, Davide Ginelli, Katiuscia Pia Lalopa, Lisa Peverelli, Alessia Pirola, Gaia Sala, Marta Maisto, and et al. 2022. "An Internet-Based Multi-Approach Intervention Targeting University Students Suffering from Psychological Problems: Design, Implementation, and Evaluation" International Journal of Environmental Research and Public Health 19, no. 5: 2711. https://doi.org/10.3390/ijerph19052711
APA StyleDe Fabritiis, M., Trisolini, F., Bertuletti, G., Fagadau, I. D., Ginelli, D., Lalopa, K. P., Peverelli, L., Pirola, A., Sala, G., Maisto, M., Madeddu, F., Lopez-Castroman, J., Romano, D., Gabbiadini, A., Preti, E., Micucci, D., & Calati, R. (2022). An Internet-Based Multi-Approach Intervention Targeting University Students Suffering from Psychological Problems: Design, Implementation, and Evaluation. International Journal of Environmental Research and Public Health, 19(5), 2711. https://doi.org/10.3390/ijerph19052711