
Zirconia Crowns for Primary Teeth: A Systematic Review and Meta-Analyses


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
- Population: Primary teeth OR pediatric patients OR extracted teeth.
- Intervention: Pediatric zirconia crowns.
- Comparator: Other restorative materials OR crowns.
- Outcomes: Periodontal health, parental satisfaction, color stability, crown retention, contour, fracture resistance, marginal integrity, surface roughness, and recurrent caries.
2.2. Search Strategies
2.3. Eligibility Criteria
2.4. Studies Screening and Selection
2.5. Data Extraction
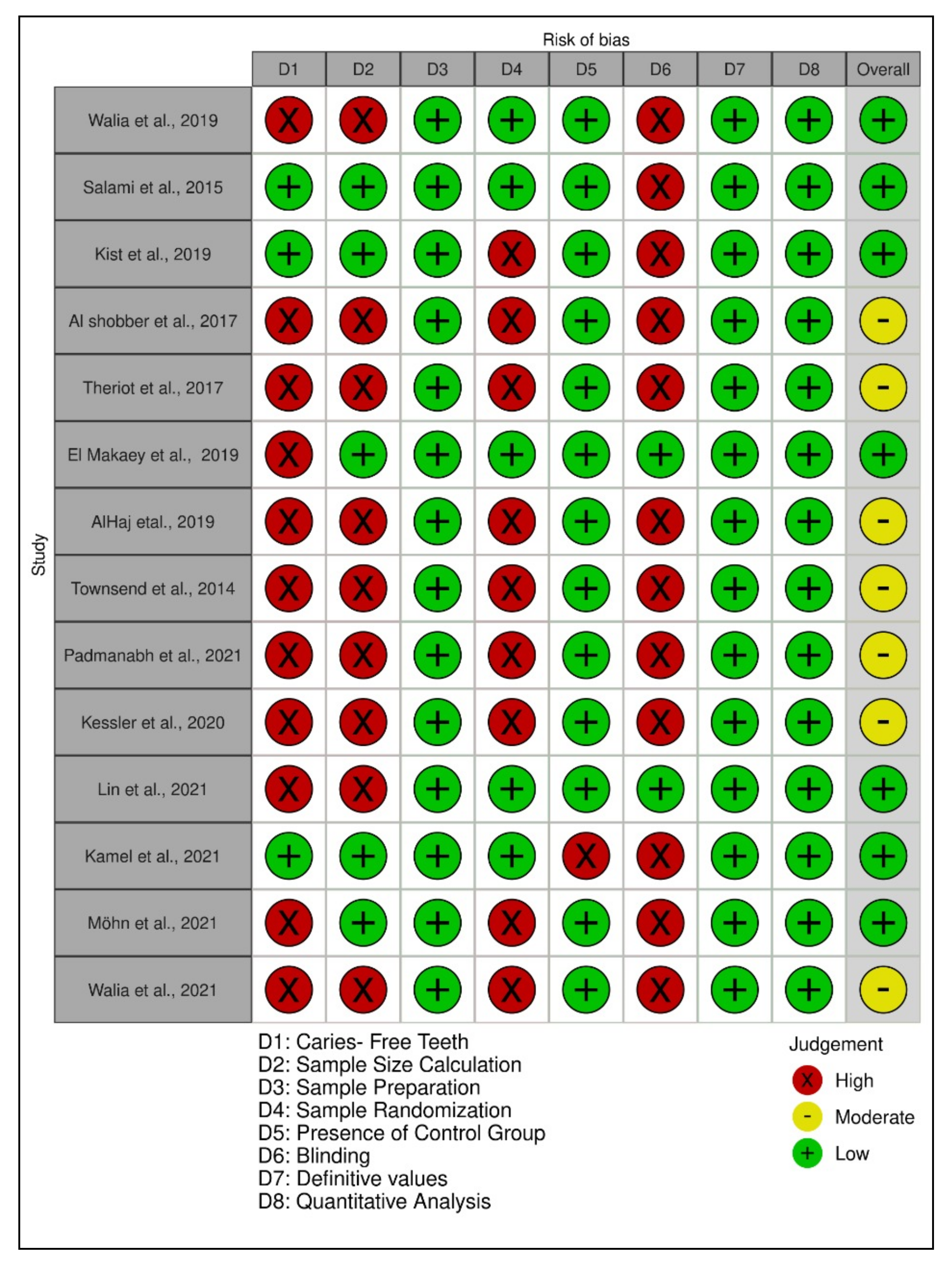
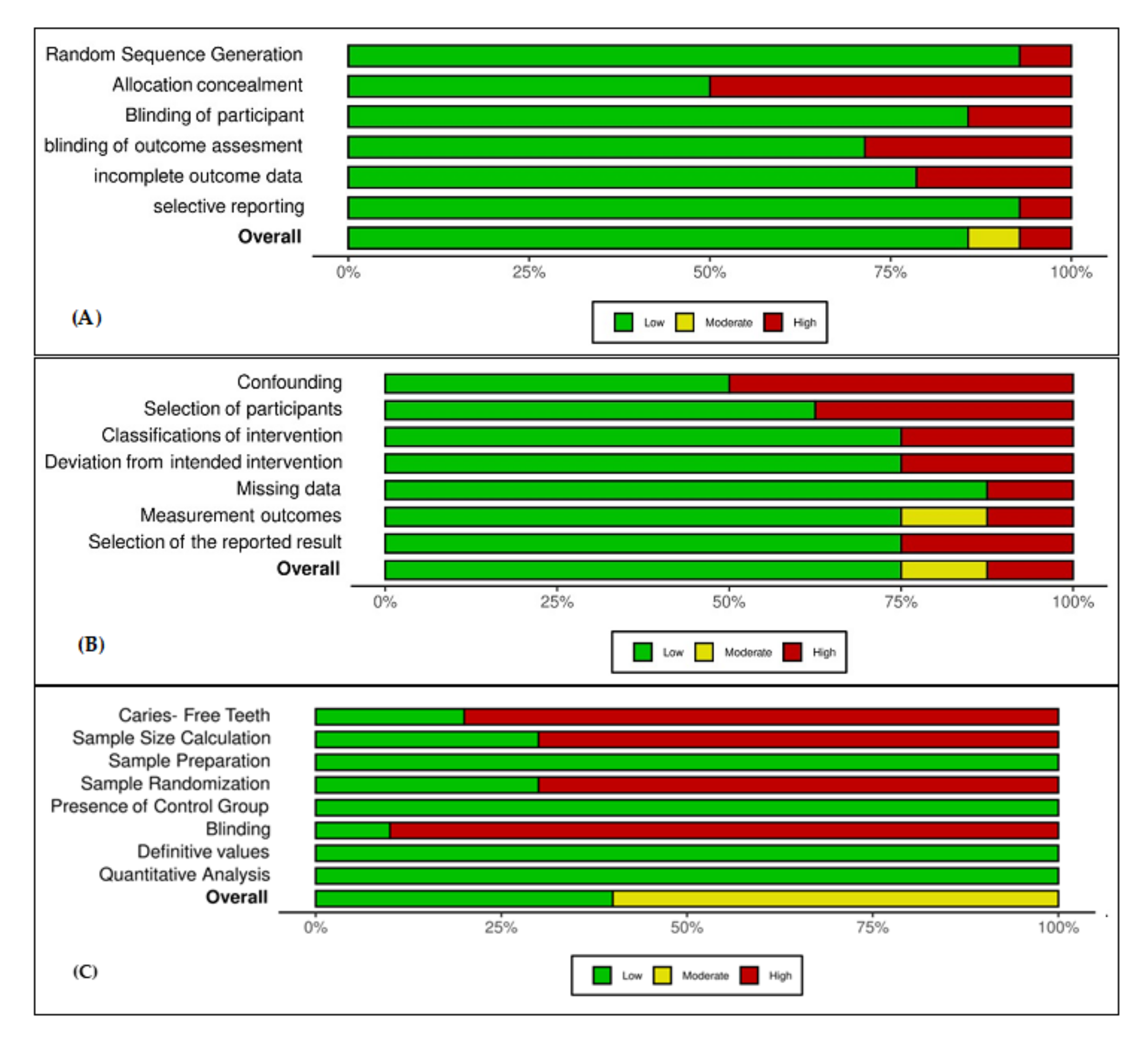
2.6. Quality Assessment
2.7. Data Synthesis
3. Results
3.1. Characteristics of the Included Studies
3.2. Quality Assessment of the Included Studies
3.3. Gingival and Periodontal Health
3.4. Parental Satisfaction
3.5. Color Stability
3.6. Crown Retention
3.7. Fracture Resistance
3.8. Marginal Integrity
3.9. Surface Roughness
3.10. Recurrent Caries
3.11. Crown Contour
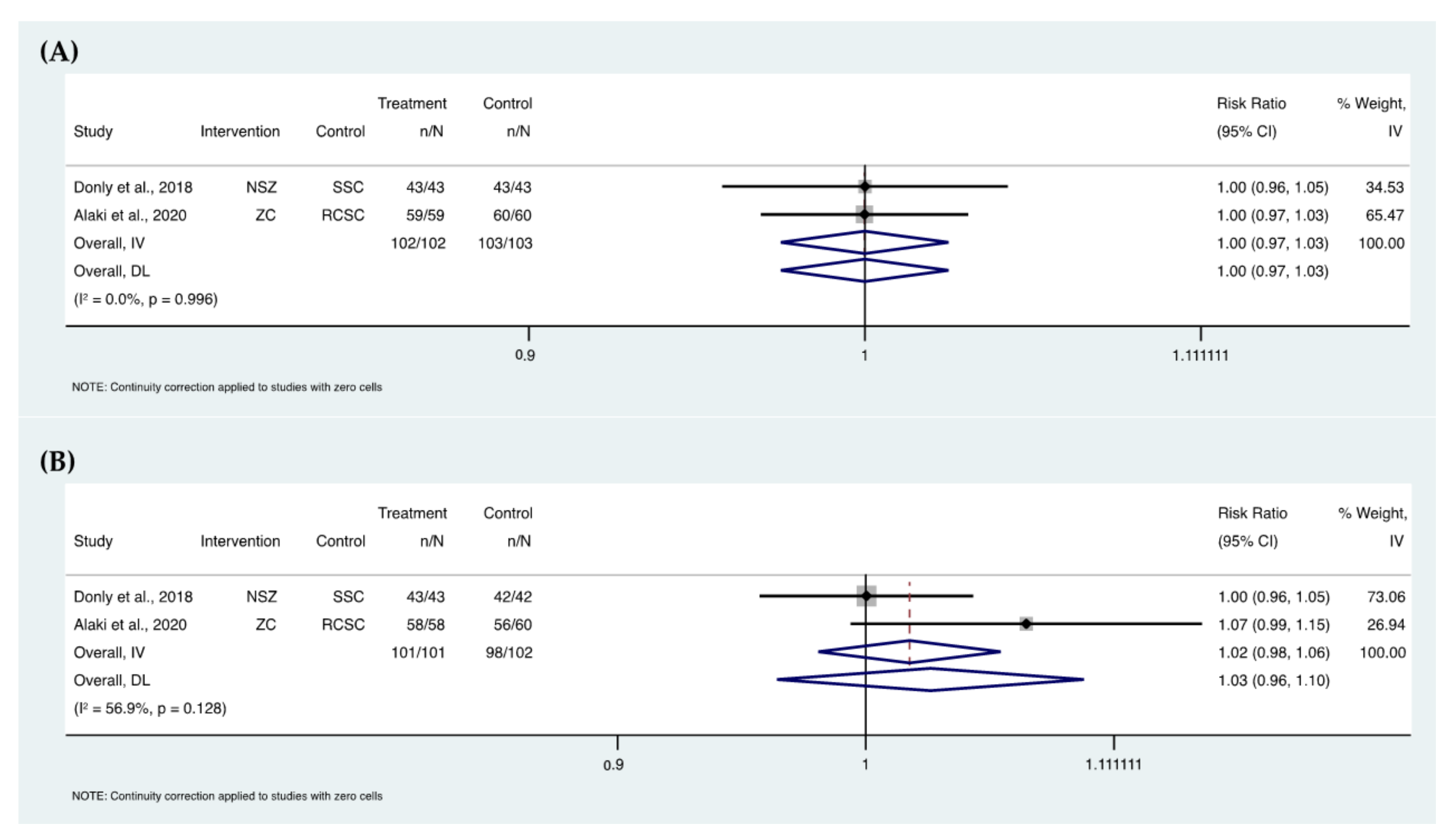
3.12. Meta-Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frencken, J.E.; Sharma, P.; Stenhouse, L.; Green, D.; Laverty, D.; Dietrich, T. Global epidemiology of dental caries and severe periodontitis—A comprehensive review. J. Clin. Periodontol. 2017, 44, S94–S105. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Ozdemir, D. Dental Caries: The Most Common Disease Worldwide and Preventive Strategies. Int. J. Biol. 2013, 5, 55–61. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health. 2012. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 5 March 2020).
- Murthy, A.K.; Pramila, M.; Ranganath, S. Prevalence of clinical consequences of untreated dental caries and its relation to dental fear among 12–15-year-old schoolchildren in Bangalore city, India. Eur. Arch. Paediatr. Dent. 2014, 15, 45–49. [Google Scholar] [CrossRef]
- Bjørndal, L.; Simon, S.; Tomson, P.L.; Duncan, H.F. Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 949–973. [Google Scholar] [CrossRef]
- Parisay, I.; Ghoddusi, J.; Forghani, M. A review on vital pulp therapy in primary teeth. Iran. Endod. J. 2015, 10, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Mendes, F.M.; De Benedetto, M.S.; Zardetto, C.G.D.C.; Wanderley, M.T.; Correa, M.S.N.P. Resin composite restoration in primary anterior teeth using short-post technique and strip crowns: A case report. Quintessence Int. 2004, 35, 689–692. [Google Scholar]
- Roberts, J.F.; Attari, N.; Sherriff, M. The survival of resin modified glass ionomer and stainless steel crown restorations in primary molars, placed in a specialist paediatric dental practice. Br. Dent. J. 2005, 198, 427–431. [Google Scholar] [CrossRef] [Green Version]
- Seale, N.S.; Randall, R.C. The use of stainless steel crowns: A systematic literature review. Pediatric Dent. 2015, 37, 145–160. [Google Scholar]
- Innes NP, T.; Ricketts, D.; Chong, L.Y.; Keightley, A.J.; Lamont, T.; Santamaria, R.M. Preformed crowns for decayed primary molar teeth. Cochrane Database Syst. Rev. 2015, 2015, 7. [Google Scholar] [CrossRef]
- Santamaría, R.M.; Innes NP, T.; Machiulskiene, V.; Schmoeckel, J.; Alkilzy, M.; Splieth, C.H. Alternative Caries Management Options for Primary Molars: 2.5-Year Outcomes of a Randomised Clinical Trial. Caries Res. 2018, 51, 605–614. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, S.; Chakraborty, P. Universal health coverage—There is more to it than meets the eye. J. Fam. Med. Prim. Care 2017, 6, 169–170. [Google Scholar] [CrossRef]
- Garg, V.; Panda, A.; Jolly Shah, P.P. Crowns in pediatric dentistry: A review. Crowns Pediatric Dent. 2015, 4, 41–46. [Google Scholar] [CrossRef]
- Randall, R.C.; Vrijhoef, M.M.; Wilson, N.H. Efficacy of Preformed Metal Crowns vs. Amalgam Restorations in Primary Molars: A Systematic Review. J. Am. Dent. Assoc. 2000, 131, 337. [Google Scholar] [CrossRef]
- Zahdan, B.A.; Szabo, A.; Gonzalez, C.D.; Okunseri, E.M.; Okunseri, C.E. Survival rates of stainless steel crowns and multi-surface composite restorations placed by dental students in a pediatric clinic. J. Clin. Pediatric Dent. 2018, 42, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S. The longevity of posterior restorations in primary teeth. Evid. Based Dent. 2018, 19, 44. [Google Scholar] [CrossRef]
- Einwag, J.; Dünninger, P. Stainless Steel Crown Versus Multisurface Amalgam Restorations: An 8-Year Longitudinal Clinical Study. Quintessence Int. 1996, 27, 321–323. [Google Scholar]
- Zafar, S.; Siddiqi, A. Biological responses to pediatric stainless steel crowns. J. Oral Sci. 2020, 62, 245–249. [Google Scholar] [CrossRef]
- Taylor, G.D. Aesthetic preformed crowns for primary teeth. Evid. Based Dent. 2017, 18, 43–44. [Google Scholar] [CrossRef]
- Salami, A.; Walia, T.; Bashiri, R. Comparison of parental satisfaction with three tooth-colored full-coronal restorations in primary maxillary incisors. J. Clin. Pediatric Dent. 2015, 39, 423–428. [Google Scholar] [CrossRef]
- Hamrah, M.H.; Mokhtari, S.; Hosseini, Z.; Khosrozadeh, M.; Hosseini, S.; Ghafary, E.S.; Hamrah, M.H.; Tavana, N. Evaluation of the Clinical, Child, and Parental Satisfaction with Zirconia Crowns in Maxillary Primary Incisors: A Systematic Review. Int. J. Dent. 2021, 2021, 7877728. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.; Lee, J.Y.; Wright, J.T. Clinical evaluation of and parental satisfaction with resin-faced stainless steel crowns. Pediatric Dent. 2001, 23, 28–31. [Google Scholar]
- Espelid, I.; Cairns, J.; Askildsen, J.E.; Qvist, V.; Gaarden, T.; Tveit, A.B. Preferences over dental restorative materials among young patients and dental professionals. Eur. J. Oral Sci. 2006, 114, 15–21. [Google Scholar] [CrossRef]
- Fishman, R.; Guelmann, M.; Bimstein, E. Children’s Selection of Posterior Restorative Materials. J. Clin. Pediatric Dent. 2006, 31, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ashima, G.; Bhatia, S.K.; Gauba, K.; Mittal, H.C. Zirconia crowns for rehabilitation of decayed primary incisors: An Esthetic alternative. J. Clin. Pediatric Dent. 2014, 39, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Walia, T.; Salami, A.A.; Bashiri, R.; Hamoodi, O.M.; Rashid, F. A randomised controlled trial of three aesthetic full-coronal restorations in primary maxillary teeth. Eur. J. Paediatr. Dent. 2014, 15, 113–118. [Google Scholar] [PubMed]
- Pozo, P.P.; Fuks, A.B. Zirconia Crowns—An Esthetic and Resistant Restorative Alternative For ECC Affected Primary Teeth. J. Clin. Pediatr. Dent. 2014, 38, 193–196. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Microtensile bond strength of different components of core veneered all-ceramic restorations: Part II: Zirconia veneering ceramics. Dent. Mater. 2006, 22, 857–863. [Google Scholar] [CrossRef]
- Taran, P.K.; Kaya, M.S. A comparison of periodontal health in primary molars restored with prefabricated stainless steel and zirconia crowns. Pediatric Dent. 2018, 40, 334–339. [Google Scholar]
- Bashaer, A.; Abdullah, M.; Alaki, S.; Alamoudi, N.; Attar, M. Clinical evaluation between zirconia crowns and stainless steel crowns in primary molars teeth. J. Pediatric Dent. 2017, 5, 21. [Google Scholar] [CrossRef]
- Clark, L.; Wells, M.H.; Harris, E.F.; Lou, J. Comparison of amount of primary tooth reduction required for anterior and posterior zirconia and stainless steel crowns. Pediatric Dent. 2016, 38, 42–46. [Google Scholar]
- D’Addazio, G.; Santilli, M.; Rollo, M.L.; Cardelli, P.; Rexhepi, I.; Murmura, G.; Husain NA, H.; Sinjari, B.; Traini, T.; Özcan, M.; et al. Fracture resistance of Zirconia-reinforced lithium silicate ceramic crowns cemented with conventional or adhesive systems: An in vitro study. Materials 2020, 13, 2012. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Sailer, I.; Zwahlen, M.; Hämmerle, C.H.F. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin. Oral Implant. Res. 2007, 18 (Suppl. 3), 73–85. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Garcia, I.M.; Kensara, A.; Balhaddad, A.A.; Collares, F.M.; Williams, M.A.; Ibrahim, A.S.; Lin, N.J.; Weir, M.D.; Xu, H.H.K.; et al. How we are assessing the developing antibacterial resin-based dental materials? A scoping review. J. Dent. 2020, 99, 103369. [Google Scholar] [CrossRef]
- Alamri, A.; Salloot, Z.; Alshaia, A.; Ibrahim, M.S. The Effect of Bioactive Glass-Enhanced Orthodontic Bonding Resins on Prevention of Demineralization: A Systematic Review. Molecules 2020, 25, 2495. [Google Scholar] [CrossRef] [PubMed]
- Holsinger, D.M.; Wells, M.H.; Scarbecz, M.; Donaldson, M. Clinical evaluation and parental satisfaction with pediatric Zirconia anterior crowns. Pediatric Dent. 2016, 38, 192–197. [Google Scholar]
- Walia, T.; Brigi, C.; KhirAllah, A.R.M.M. Comparative evaluation of surface roughness of posterior primary zirconia crowns. Eur. Arch. Paediatr. Dent. 2019, 20, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Jing, L.; Chen, J.W.; Roggenkamp, C.; Suprono, M.S. Effect of Crown Preparation Height on Retention of a Prefabricated Primary Posterior Zirconia Crown. Pediatric Dent. 2019, 41, 229–233. [Google Scholar]
- Madhavan, S.; Mathew, M.G. Assessment of the knowledge, attitude, and awareness among dental students about prevention of dental caries in pediatric patients. Drug Invent. Today 2019, 11, 21–25. [Google Scholar]
- Pani, S.C.; Saffan, A.A.; AlHobail, S.; Bin Salem, F.; AlFuraih, A.; AlTamimi, M. Esthetic Concerns and Acceptability of Treatment Modalities in Primary Teeth: A Comparison between Children and Their Parents. Int. J. Dent. 2016, 2016, 3163904. [Google Scholar] [CrossRef] [Green Version]
- Mathew, M.G.; Samuel, S.R.; Soni, A.J.; Roopa, K.B. Evaluation of adhesion of Streptococcus mutans, plaque accumulation on zirconia and stainless steel crowns, and surrounding gingival inflammation in primary molars: Randomized controlled trial. Clin. Oral Investig. 2020, 24, 3275–3280. [Google Scholar] [CrossRef] [PubMed]
- Mathew, M.G.; Roopa, K.B.; Soni, A.J.; Khan, M.M.; Kauser, A. Evaluation of Clinical Success, Parental and Child Satisfaction of Stainless Steel Crowns and Zirconia Crowns in Primary Molars. J. Fam. Med. Prim. Care 2020, 6, 169–170. [Google Scholar] [CrossRef]
- Kist, S.; Stawarczyk, B.; Kollmuss, M.; Hickel, R.; Huth, K.C. Fracture load and chewing simulation of zirconia and stainless-steel crowns for primary molars. Eur. J. Oral Sci. 2019, 127, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Al Shobber, M.Z.; Alkhadra, T.A. Fracture resistance of different primary anterior esthetic crowns. Saudi Dent. J. 2017, 29, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Theriot, A.L.; Frey, G.N.; Ontiveros, J.C.; Badger, G. Gloss and surface roughness of anterior pediatric zirconia crowns. J. Dent. Child. 2017, 84, 115–119. [Google Scholar]
- El Makawi, Y.; Khattab, N. In vitro comparative analysis of fracture resistance of lithium disilicate endocrown and prefabricated zirconium crown in pulpotomized primary molars. Open Access Maced. J. Med. Sci. 2019, 7, 4094–4100. [Google Scholar] [CrossRef]
- Al-Haj Ali, S.N. In vitro comparison of marginal and internal fit between stainless steel crowns and esthetic crowns of primary molars using different luting cements. Dent. Res. J. 2019, 16, 366–371. [Google Scholar] [CrossRef]
- Townsend, J.A.; Knoell, P.; Yu, Q.; Zhang, J.; Wang, Y.; Zhu, H.; Beattie, S.; Xu, X. Fracture Resistance of Three Commercially Available Zirconia Crowns for. Urology 1993, 41, 125–129. [Google Scholar] [CrossRef]
- Azab, M.M.; Moheb, D.M.; El Shahawy, O.I.; Rashed, M.A.M. Influence of luting cement on the clinical outcomes of Zirconia pediatric crowns: A 3-year split-mouth randomized controlled trial. Int. J. Paediatr. Dent. 2020, 30, 314–322. [Google Scholar] [CrossRef]
- Donly, K.J.; Mendez, M.J.C.; Contreras, C.I.; Liu, J.A. Prospective Randomized Clinical Trial of Primary Molar Crowns: 24-Month Results. Am. J. Dent. 2018, 33, 165–168. [Google Scholar]
- El Shahawy, O.I.; O’Connell, A.C. Successful Restoration of Severely Mutilated Primary Incisors Using a Novel Method to Retain Zirconia Crowns—Two Year Results. J. Clin. Pediatric Dent. 2016, 40, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Hanafi, L.; Altinawi, M.; Comisi, J.C. Evaluation and comparison two types of prefabricated zirconia crowns in mixed and primary dentition: A randomized clinical trial. Heliyon 2021, 7, e06240. [Google Scholar] [CrossRef] [PubMed]
- Davangere Padmanabh, S.K.; Patel, V. The effect of sterilization and disinfection on the physical-mechanical properties of preformed crowns. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 53–60. [Google Scholar] [CrossRef]
- Karthikeyan, G.; Ravindran, V.; Ramamurthy, J. Prevalence of usage of stainless steel crown, strip crown and zirconia in anterior teeth for paediatric dental patients in different age groups. Int. J. Res. Pharm. Sci. 2020, 11, 1511–1516. [Google Scholar] [CrossRef]
- Manthra Prathoshni, S.; Ravindran, V.; Ramanathan, V. Use of stainless steel crowns and zirconia crowns in posterior primary teeth for children in different age groups. Int. J. Res. Pharm. Sci. 2020, 11, 1540–1545. [Google Scholar] [CrossRef]
- Alaki, S.M.; Abdulhadi, B.S.; AbdElBaki, M.A.; Alamoudi, N.M. Comparing zirconia to anterior strip crowns in primary anterior teeth in children: A randomized clinical trial. BMC Oral Health 2020, 20, 313. [Google Scholar] [CrossRef] [PubMed]
- Alhissan, A.S.; Pani, S.C. Factors Influencing the Survival of Preformed Zirconia Crowns in Children Treated under General Anesthesia. Int. J. Dent. 2021, 2021, 5515383. [Google Scholar] [CrossRef]
- Gill, A.; Garcia, M.; Won An, S.; Scott, J.A.; Seminario, A.L. Clinical Comparison of Three Esthetic Full-Coverage Restorations in Primary Maxillary Incisors at 12 Months. Pediatric Dent. 2020, 42, 367–372. [Google Scholar]
- Nischal, M.; Gupta, T.; Mehra, M.; Sadana, G. Clinical comparison of three tooth-colored full-coronal restorations in primary maxillary incisors. Int. J. Clin. Pediatric Dent. 2020, 13, 622–629. [Google Scholar] [CrossRef]
- Kessler, A.; Kapor, S.; Erdelt, K.; Hickel, R.; Edelhoff, D.; Syrek, A.; Güth, J.F.; Kühnisch, J. Two-body wear and fracture behaviour of an experimental paediatric composite crown in comparison to zirconia and stainless steel crowns dependent on the cementation mode. Dent. Mater. 2021, 37, 264–271. [Google Scholar] [CrossRef]
- Sharma, M.; Khatri, A.; Kalra, N.; Tyagi, R. Evaluation and comparison of strip crowns and primary anterior zirconia crowns in 3–5 years old children at one year. Pediatric Dent. J. 2021, 31, 136–144. [Google Scholar] [CrossRef]
- Yanover, L.; Tickotsky, N.; Waggoner, W.; Kupietzky, A.; Moskovitz, M. Zirconia crown performance in primary maxillary anterior teeth: A retrospective photographic and radiographic cohort study. Eur. Arch. Paediatr. Dent. 2021, 22, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Talekar, A.L.; Chaudhari, G.S.; Waggoner, W.F.; Chunawalla, Y.K. An 18-Month Prospective Randomized Clinical Trial Comparing Zirconia Crowns with Glass-reinforced Fiber Composite Crowns in Primary Molar Teeth. Pediatric Dent. 2021, 43, 355–362. [Google Scholar]
- Lin, B.; Khatri, A.; Hong, M. Comparison of Fracture Strengths among different Commonly Placed Anterior Esthetic Restorations for Primary Dentition: An in vitro study. J. Clin. Pediatric Dent. 2021, 45, 171–176. [Google Scholar] [CrossRef]
- Yanover, L.; Waggoner, W.; Kupietzky, A.; Moskovitz, M.; Tickotsky, N. Parental and Dentist Satisfaction with Primary Anterior Zirconia Crowns: A Case Series Analysis. Children 2021, 8, 451. [Google Scholar] [CrossRef]
- Walia, T.; Brigi, C.; Ziadkhani, M.M.; Khayat, A.A.; Tabibzadeh, Z. Retention Force of Glass Ionomer Based Luting Cements with Posterior Primary Zirconium Crowns—A Comparative in Vitro Study. J. Clin. Pediatric Dent. 2021, 45, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Sabbah, A.A.H.; Kamel, M.H. Fracture Resistance of Primary Molars Restored with Endocrowns Versus Fracture Resistance of Primary Molars Restored with Endocrowns Versus Zirconia Crowns (An in Vitro Study). Braz. Dent. Sci. 2021, 24, 2. [Google Scholar] [CrossRef]
- Möhn, M.; Frankenberger, R.; Krämer, N. Wear and marginal quality of aesthetic crowns for primary molars. Int. J. Paediatr. Dentistry. 2021, 32, 273–283. [Google Scholar] [CrossRef]
- González-Martín, M.L.; Labajos-Broncano, L.; Jańczuk, B.; Bruque, J.M. Wettability and surface free energy of zirconia ceramics and their constituents. J. Mater. Sci. 1999, 34, 5923–5926. [Google Scholar] [CrossRef]
- Li, W.; Chen, J.; Li, Z.; Chen, F.; Zou, L.; Zhao, J.; Gao, Z.; Wang, Y.; Lu, Y. BaTiO3 optimized 3Y-TZP ceramic with improved osteoblasts growth and enhanced osteogenic activity. Ceram. Int. 2021, 47, 23413–23422. [Google Scholar] [CrossRef]
- Elqadir, A.J.; Shapira, J.; Ziskind, K.; Ram, D. Esthetic restorations of primary anterior teeth. Refu’at Ha Peh Veha Shinayim 2013, 30, 54–60. [Google Scholar]
- Diener, V.; Polychronis, G.; Erb, J.; Zinelis, S.; Eliades, T. Surface, microstructural, and mechanical characterization of prefabricated pediatric zirconia crowns. Materials 2019, 12, 3280. [Google Scholar] [CrossRef] [Green Version]
- Mundim, F.M.; Garcia LD, F.R.; Pires-de-Souza, F.D.C.P. Effect of staining solutions and repolishing on color stability of direct composites. J. Appl. Oral Sci. 2010, 18, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Tote, J.; Godhane, A.; Das, G.; Soni, S.; Jaiswal, K.; Vidhale, G. Posterior Esthetic Crowns in Pediatric Dentistry. Int. J. Dent. Med. Res. 2015, 1, 197–201. [Google Scholar]
- Stepp, P.; Morrow, B.R.; Wells, M.; Tipton, D.A.; Garcia-Godoy, F. Microleakage of cements in prefabricated zirconia crowns. Pediatric Dent. 2018, 40, 136–139. [Google Scholar]
- Hmaidouch, R.; Weigl, P. Tooth wear against ceramic crowns in posterior region. Int. J. Oral Sci. 2013, 5, 183–190. [Google Scholar] [CrossRef]
- Alrashdi, M.; Ardoin, J.; Liu, J.A. Zirconia crowns for children: A systematic review. Int. J. Paediatr. Dent. 2022, 32, 66–81. [Google Scholar] [CrossRef] [PubMed]
- Behr, M.; Rosentritt, M.; Regnet, T.; Lang, R.; Handel, G. Marginal adaptation in dentin of a self-adhesive universal resin cement compared with well-tried systems. Dent. Mater. 2004, 20, 191–197. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database: PubMed | Results |
|---|---|
| ((child*)[tiab] OR (Primary)[tiab] OR (deciduous)[tiab] OR (tooth, deciduous)[MeSH] OR (Pediatric)[tiab] OR (Paediatric)[tiab])) AND ((zirconia)[tiab])) | 491 |
| Database: Scopus | Results |
| (TITLE-ABS-KEY ((child* OR deciduous OR pediatric*))) AND (TITLE-ABS-KEY (zirconia)) | 160 |
| Database: Web of Science | Results |
| ((child*) OR (Primary) OR (decisdous) OR (tooth, deciduous) OR (Pediatric) OR (Paediatric) AND (zirconia) | 1456 |
| Database: Ovid | Results |
| ((child* or primary or deciduous or pediatric* or paediatric).af.) AND (zirconia.af.) | 293 |
| Study | Type of Study | Sample Size per Group | Participant Characteristics | Outcome Measures | Intervention | Comparator | Cement Type |
|---|---|---|---|---|---|---|---|
| Taran et al., 2018 [30] | Clinical | 15 | Age (A) = 6–9 Y Number of patients (T) = 15 Female (F) = 9 Male (M) = 6 | Crown retention Gingival marginal extension Stain resistance Fracture resistance Plaque index (PI) Gingival index (GI) Simplified oral Hygiene index | NuSmile zirconia crown (NSZ) | Intact contralateral teeth stainless steel crown (SSC) | SSC: Glass ionomer cement (GIC) NSZ: Resin modified glass ionomer cement (RMGIC) |
| Walia et al., 2014 [27] | Clinical | 43 | A = 3–5 Y T = 39 M = 21 F = 18 | Crown retention Tooth wear GI | Zirkiz zirconia Crown (ZZC) | Resin Composite Strip Crown (RCSC) Pre-veneered stainless steel crown (PVSSC) | RCSC: (3M, Scotchbond-Universal-Adhesive-Refill-Vial-41258®) PVSSC: GIC-II ZZC: GIC-II |
| Holsinger et al., 2016 [37] | Observational | 57 | A = 2–6 Y T = 18 F = 6 M = 12 | Crown retention GI Stain resistance Crown contour Marginal integrity Tooth wear Recurrent caries Parent acceptability | EZ Pedo crown (EZP) | - | EZP: GIC |
| Walia et al., 2019 [38] | Laboratory | 10 | - | Surface roughness | NSZ Spring EZ crown (SEC) Cheng crown zirconia (CCZ) Kinder Krown zirconia crown (KKZ) | - | - |
| Salami et al., 2015 [21] | Observational | 43 | A = 3–5 Y T = 39 F = 18 M = 21 | Parental satisfaction | ZZC | RCSC PVSSC | - |
| Jing et al., 2019 [39] | Laboratory | 15 | - | Crown retention of zirconia Crown (ZC) for primary teeth with various Occluso-Cervical Hights (OCH) crown preparation | SEC | - | SEC: GIC |
| Vaishali et al., 2019 [40] | Observational | 125 | A = 6–8 Y | Parent acceptability | Questionnaire | - | - |
| Pani et al., 2016 [41] | Observational | 107 | A = 5–8 Y | Parent acceptability | Questionnaire | - | - |
| Mathew et al., 2020 [42] | Clinical | 30 | A = 6–9 Y T = 30 F = 18 M = 12 | GI PI CFU/mL count of S. mutans | KKZ | SSC | - |
| Mathew et al., 2020 [43] | Clinical | 30 | A = 6–8 Y | Crown retention GI PI Stain resistance Gingival marginal extension Occlusion Proximal contact Parent acceptability | KKZ | SSC | All: GIC-I |
| Kist et al., 2019 [44] | Laboratory | 85 | - | Fracture resistance | SEC KKZ NSZ | Computer-aided manufacturing/computer-aided modeling zirconia crown (CAD/CAM) ZC PVSSC SSC | All: GIC |
| Al shobber et al., 2017 [45] | Laboratory | 16 | - | Fracture resistance | CCZ NSZ | PVSSC Cheng crown pre-veneered (CCP) | All: GIC |
| Theriot et al., 2017 [46] | Laboratory | 20 | - | Surface roughness Surface gloss | NSZ SEC KKZ | - | - |
| El Makawi et al., 2019 [47] | Laboratory | 10 | - | Fracture resistance | NSZ | Lithium disilicate endocrown (LDE) | All: resin composite (RC) |
| Alhaj et al., 2019 [48] | Laboratory | 12 | - | Marginal and internal gap | NSZ | SSC PVSSC | All: RC, GIC, or RMGIC |
| Townsend et al., 2014 [49] | Laboratory | 20 | - | Fracture resistance Crown thickness | EZP NSZ KKZ | PVSSC | All: GIC |
| Azab et al. [50] | Clinical | 25 | A = 4–7 Y T = 25 F = 11 M = 14 | Crown retention Fracture resistance GI | NSZ | Different types of cements | NSZ: GIC-IX or bioactive cement |
| Donly et al., 2018 [51] | Clinical | 50 | A = 3–7 Y | GI Occlusion Surface roughness Stain resistance Tooth wear Color match Anatomic form Marginal integrity Marginal discoloration Proximal contact Recurrent caries | NSZ | SSC | NSZ: Bioceramic Cement SSC: RMGIC |
| El Shahawy et al., 2016 [52] | Clinical | 86 | A = 2–5 Y | Crown Retention | NSZ | - | NSZ: GIC-IX |
| Hanafi et al., 2021 [53] | Clinical | (CAD/CAM) ZC = 31 NSZ = 32 | A = 5–9 Y T = 44 F = 16 M = 28 | GI PI Bleeding on probing (BOP) Crown marginal extension | (CAD/CAM) ZC | NSZ | All: GIC |
| Padmanabh et al., 2021 [54] | Laboratory | 20 | - | Stain resistance Crazing Dimensional stability Fracture resistance | KKZ | SSC PVSSC | - |
| Ravindran et al., 2020 [55] | Observational | 107 | A = 2–7 Y T = 107 F = 42 M = 65 | Prevalence | ZC | RCSC SSC | - |
| Ravindran et al., 2020 [56] | Observational | 1496 | A = 0–10 Y T = 1496 F = 628 M = 868 | Prevalence | NSZ | SSC | All: Type I GIC |
| Alaki et al., 2020 [57] | Clinical | 60 | A = 4–6 Y T = 32 F = 20 M = 12 | GI PI Recurrent caries Restoration failure Proximal contact Marginal integrity Occlusion Tooth wear | ZC | RCSC | ZC: RC |
| Alhissan et al., 2021 [58] | Observational | 70 | A = 3–5 Y T = 20 F = 11 M = 9 | Restoration failure | NSZ | With/without pulp therapy | - |
| Gill et al., 2020 [59] | Clinical | 135 | A = 2–4 Y T = 47 | Crown fit Proximal contact Color match Crown retention Facing integrity Marginal integrity GI Recurrent caries Parent satisfaction | NSZ | RCSC PVSSC | RCSC: (Scotchbond Universal, 3M ESPE, St. Paul, MN, USA) PVSSC: GIC NSZ: RMGIC |
| Nischal et al., 2020 [60] | Clinical | 45 | T = 45 | Surface roughness Anatomical form Marginal integrity Marginal discoloration Recurrent caries | ZC | RCSC Luxa crown | RCSC: bonding agent ZC: RMGIC Luxa crown: RMGIC |
| Kessler et al., 2020 [61] | Laboratory | - | - | Crown wear Fracture | NSZ | Composite crown SSC | All: RMGIC and two self-adhesive cements (SACs; RelyX Unicem Automix 2, 3M; BioCem, NuSmile) |
| Sharma et al., 2021 [62] | Clinical | 20 | A = 3–5 Y T = 24 | GI PI Tooth wear Color Restoration failure | ZC | RCSC | RCSC: Light cure bonding adhesive (3M, Scotchbond-Universal Adhesive-Refill-Vial-41258®) ZC: Type II GIC |
| Yanover et al., 2020 [63] | Observational | 131 | A = 2–5 Y T = 36 F = 5 M = 31 | Marginal integrity GI Restoration failure | SEC NSZ CCZ | - | - |
| Talekar et al. 2021 [64] | Clinical | 33 | A = 4–9 Y T = 30 | Color match Stain resistance GI Crown retention PI Occlusal wear Parent satisfaction | NSZ | Glass fiber-reinforced composite crown—Figaro Crowns (GFRC) | NSZ: RMGIC GFRC crowns: Type I GIC |
| Lin et al., 2021 [65] | Laboratory | 15 | - | Fracture resistance | EZP Polycarbonate crowns—PedoNatural RCSC | - | EZP: Type I GIC and self-adhesive resin cement (RelyX Unicem, 3M ESPE Polycarbonate crowns: polymer-reinforced zinc oxide-eugenol cement (IRM Dentsply). |
| Yanover et al., 2021 [66] | Observational | 131 | A = 2–5 Y T = 37 F = 10 M = 27 | Parent satisfaction | EZP NSZ CCZ | - | - |
| Walia et al., 2021 [67] | Laboratory | 24 | - | Crown retention | NSZ SEC KKZ CCZ | - | FujiCEM® 2 (GC America, Alsip, IL, USA) KetacTM Cem Maxicap (3M ESPE, St. Paul, MN, USA) BioCem (NuSmile, Houston, TX, USA) |
| Sabbah et al., 2020 [68] | Laboratory | 6 | - | Fracture resistance | NSZ | Nano-Ceramic Composite Endocrowns | NSZ: GIC NCCE: self-adhesive universal dual cured resin cement |
| Mohn et al., 2021 [69] | Laboratory | 144 | - | Marginal integrity Tooth wear Crown fracture | RCSC (CAD/CAM) ZC | SSC ZC | All: GIC RMGIC dual-cure self-adhesive resin cement (SAC) RC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzanbaqi, S.D.; Alogaiel, R.M.; Alasmari, M.A.; Al Essa, A.M.; Khogeer, L.N.; Alanazi, B.S.; Hawsah, E.S.; Shaikh, A.M.; Ibrahim, M.S. Zirconia Crowns for Primary Teeth: A Systematic Review and Meta-Analyses. Int. J. Environ. Res. Public Health 2022, 19, 2838. https://doi.org/10.3390/ijerph19052838
Alzanbaqi SD, Alogaiel RM, Alasmari MA, Al Essa AM, Khogeer LN, Alanazi BS, Hawsah ES, Shaikh AM, Ibrahim MS. Zirconia Crowns for Primary Teeth: A Systematic Review and Meta-Analyses. International Journal of Environmental Research and Public Health. 2022; 19(5):2838. https://doi.org/10.3390/ijerph19052838
Chicago/Turabian StyleAlzanbaqi, Sara Douf, Rakan Mishaal Alogaiel, Mohammed Ali Alasmari, Ahmed Mohammed Al Essa, Layla Nizar Khogeer, Basim Salem Alanazi, Eyad Sami Hawsah, Ahmed Mohammed Shaikh, and Maria Salem Ibrahim. 2022. "Zirconia Crowns for Primary Teeth: A Systematic Review and Meta-Analyses" International Journal of Environmental Research and Public Health 19, no. 5: 2838. https://doi.org/10.3390/ijerph19052838