
Comparative Ergonomic Study Examining the Work-Related Musculoskeletal Disorder Symptoms of Taiwanese and Thai Workers in a Tape Manufacturing Factory

Abstract
:1. Introduction
2. Methods
2.1. Participants
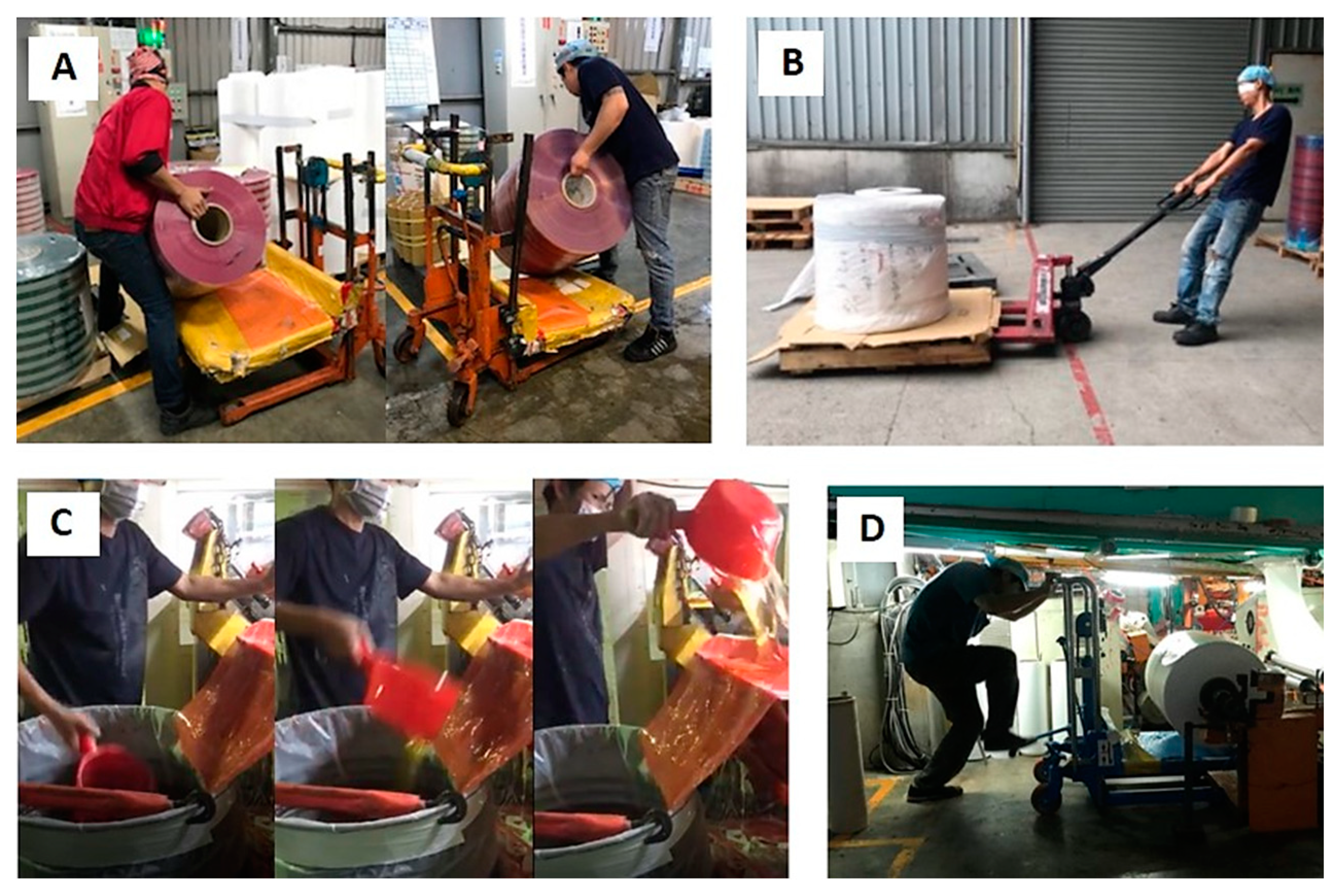
2.2. Task Description
2.3. NMQ
2.4. 3DSSPP
2.5. RULA
2.6. OWAS
2.7. Statistical Analysis
3. Results
3.1. Demographics and Task Characteristics
3.2. WMSDs and Risk Factors
3.3. Body Load Assessments of Specified Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Identification and control of work-released diseases. In Report of a WHO Expert Committee; World Health Organ Technical Report Series; World Health Organization: Geneva, Switzerland, 1985; Volume 714, pp. 1–71. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Work-Related Musculoskeletal Disorders & Ergonomics, Workplace Health Strategies; Centers for Disease Control and Prevention: Atlanta, Georgia, 1997. Available online: https://www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html (accessed on 10 December 2022).
- Sekkay, F.; Imbeau, D.; Chinniah, Y.; Dubéa, P.A.; Warina, N.D.M.; Beauregardb, N.; Trépanier, M. Risk factors associated with self-reported musculoskeletal pain among short and long-distance industrial gas delivery truck drivers. Appl. Ergon. 2018, 72, 69–87. [Google Scholar] [CrossRef]
- Joseph, L.; Vasanthan, L.; Standen, M.; Kuisma, R.; Paungmali, A.; Pirunsan, U.; Sitilertpisan, P. Causal relationship between the risk factors and work-related musculoskeletal disorders among professional. drivers: A systematic review. Hum. Factors 2021, 65, 187208211006500. [Google Scholar] [CrossRef]
- Engholm, G.; Holmström, E. Dose-response associations between musculoskeletal disorders and physical and psychosocial factors among construction workers. Scand. J. Work Environ. Health 2005, 31 (Suppl. S2), 57–67. [Google Scholar] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef]
- Yang, Y.; Zeng, J.; Liu, Y.; Wang, Z.; Jia, N.; Wang, Z. Prevalence of musculoskeletal disorders and their associated risk factors among furniture manufacturing workers in Guangdong, China: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 14435. [Google Scholar] [CrossRef]
- Chen, Y.L.; Chiang, H.T. Atilt rolling movement of a gas cylinder: A case study. Work 2014, 49, 473–481. [Google Scholar] [CrossRef]
- Institute of Labor and Occupational Safety and Health (ILOSH). Survey of Perceptions of Safety and Health in the Work Environment in 2016 Taiwan; Project no. ILOSH105-A309; ILOSH: New Taipei, Taiwan, 2017. [Google Scholar]
- Chen, Y.L.; Zhong, Y.T.; Lio, B.N.; Yang, C.C. Musculoskeletal disorders symptoms among Taiwanese bakery workers. Int. J. Environ. Res. Public Health 2020, 17, 2960. [Google Scholar] [CrossRef]
- Govaerts, R.; Tassignon, B.; Ghillebert, J.; Serrien, B.; De Bock, S.; Ampe, T.; El Makrini, I.; Vanderborght, B.; Meeusen, R.; De Pauw, K. Prevalence and incidence of work-related musculoskeletal disorders in secondary industries of 21st century Europe: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2021, 22, 751. [Google Scholar] [CrossRef]
- Chen, Y.L.; Alexander, H.; Hu, Y.M. Self-reported musculoskeletal disorder symptoms among bus drivers in the Taipei metropolitan area. Int. J. Environ. Res. Public Health 2022, 19, 10596. [Google Scholar] [CrossRef]
- Lin, J.H.; Lee, W.; Smith, C.K.; Yragui, N.L.; Foley, M.; Shin, G. Cleaning in the 21st Century: The musculoskeletal disorders associated with the centuries-old occupation—A literature review. Appl. Ergon. 2022, 105, 103839. [Google Scholar] [CrossRef] [PubMed]
- Hulls, P.M.; Richmond, R.C.; Martin, R.M.; Chavez-Ugalde, Y.; de Vocht, F. Workplace interventions that aim to improve employee health and well-being in male-dominated industries: A systematic review. Occup. Environ. Med. 2022, 79, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Keyserling, W. Workplace risk factors and occupational musculoskeletal disorders, Part 2: A review of biomechanical and psychophysical research on risk factors associated with upper extremity disorders. Am. Ind. Hyg. Assoc. J. 2000, 61, 231–243. [Google Scholar] [CrossRef]
- National Development Council (NDC). Number of Migrant Workers Sorted by Nationality; National Development Council: Taipei City, Taiwan, 2022. Available online: https://www.ndc.gov.tw/Content_List.aspx?n=421CC0712EC314BD (accessed on 10 December 2022).
- Korkmaz, S.; Park, D.J. Comparison of safety perception between foreign and local workers in the construction industry in Republic of Korea. Saf. Health Work 2018, 9, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Carangan, M.; Tham, K.Y.; Seow, E. Work-related injury sustained by foreign workers in Singapore. Ann. Acad. Med. Singap. 2004, 33, 209–213. [Google Scholar] [PubMed]
- Guldenmund, F.; Cleal, B.; Mearns, K. An exploratory study of migrant workers and safety in three European countries. Saf. Sci. 2013, 52, 92–99. [Google Scholar] [CrossRef]
- Corvalan, C.F.; Driscoll, T.R.; Harrison, J.E. Role of migrant factors in work-related fatalities in Australia. Scand. J. Work Environ. Health 1994, 20, 364–370. Available online: https://www.jstor.org/stable/40966277 (accessed on 10 December 2022).
- Ahonen, E.Q.; Benavides, F.G. Risk of fatal and non-fatal occupational injury in foreign workers in Spain. J. Epidemiol. Community Health 2006, 60, 424–426. [Google Scholar] [CrossRef]
- Salami, B.; Meharali, S.; Salami, A. The health of temporary foreign workers in Canada: A scoping review. Can. J. Public Health 2015, 106, e546–e554. [Google Scholar] [CrossRef]
- Cheng, C.W.; Wu, T.C. An investigation and analysis of major accidents involving foreign workers in Taiwan’s manufacture and construction industries. Saf. Sci. 2013, 57, 223–235. [Google Scholar] [CrossRef]
- Orrenius, P.M.; Zavodny, M. Do immigrants work in riskier jobs? Demography 2009, 46, 535–551. [Google Scholar] [CrossRef]
- Moyce, S.C.; Schenker, M. Migrant workers and their occupational health and safety. Ann. Rev. Public Health 2018, 39, 351–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hargreaves, S.; Rustage, K.; Nellums, L.B.; McAlpine, A.; Pocock, N.; Devakumar, D. Occupational health outcomes among international migrant workers: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e872–e882. [Google Scholar] [CrossRef]
- Son, K.S.; Yang, H.K.; Guedes, S.C. Accidents of foreign workers at construction sites in Korea. J. Asian Architect. Build Eng. 2013, 12, 197–203. [Google Scholar] [CrossRef]
- Lee, W.; Neo, A.; Tan, S.; Cook, A.R.; Wong, M.L.; Tan, J. Health-seeking behaviour of male foreign migrant workers living in a dormitory in Singapore. BMC Health Serv. Res. 2014, 14, 300. [Google Scholar] [CrossRef]
- Fernández-Esquer, M.E.; Fernández-Espada, N.; Atkinson, J.A.; Montano, C.F. The influence of demographics and working conditions on self-reported injuries among Latino day laborers. Int. J. Occup. Environ. Health 2015, 21, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Occupational Safety and Health Administration, OSHA (Taiwan). Statistical Overview of Occupational Disease Notification on the National Occupational Injury Diagnosis and Treatment Network in 107; Occupational Safety and Health Administration: Taipei City, Taiwan, 2018. Available online: https://www.osha.gov.tw/48110/48417/48419/86739 (accessed on 10 December 2022).
- Nawrocka, A.; Mynarski, W.; Powerska, A.; Grabara, M.; Groffik, D.; Borek, Z. Health-oriented physical activity in prevention of musculoskeletal disorders among young Polish musicians. Int. J. Occup. Med. Environ. Health 2014, 27, 28–37. [Google Scholar] [CrossRef]
- Takekawa, K.S.; Goncalves, J.S.; Moriguchi, C.S.; Coury, H.J.C.G. Can a self-administered questionnaire identify workers with chronic or recurring low back pain? Ind. Health 2015, 53, 340–345. [Google Scholar] [CrossRef]
- Deakin, J.M.; Stevenson, J.M.; Vail, G.R.; Nelson, J.M. The use of the Nordic Questionnaire in an industrial setting: A case study. Appl. Ergon. 1994, 25, 182–185. [Google Scholar] [CrossRef]
- Lu, J.M.; Twu, L.J.; Wang, M.J.J. Risk assessments of work-related musculoskeletal disorders among the TFT-LCD manufacturing operators. Int. J. Ind. Ergon. 2016, 52, 40–51. [Google Scholar] [CrossRef]
- Chen, Y.L.; Yu, C.Y.; Lin, D.Y. Musculoskeletal disorders caused by gas-cylinder handling tasks: A case study report. Work 2017, 56, 403–407. [Google Scholar] [CrossRef]
- Pugh, J.D.; Gelder, L.; Williams, A.M.; Twigg, D.E.; Wilkinson, A.M.; Blazevich, A.J. Validity and reliability of an online extended version of the Nordic Musculoskeletal Questionnaire (NMQ-E2) to measure nurses’ fitness. J. Clin. Nurs. 2015, 24, 3550–3563. [Google Scholar] [CrossRef] [PubMed]
- Center for Ergonomics. User’s Manual 3D Static Strength Prediction ProgramTM Version 7.0.0; The University of Michigan: Ann Arbor, MI, USA, 2017; Available online: https://c4e.engin.umich.edu/assets/3DSSPP-Version-7.0.0-Manual.pdf (accessed on 10 December 2022).
- McAtamney, L.; Corlett, E. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Kee, D. Systematic comparison of OWAS, RULA, and REBA based on a literature review. Int. J. Environ. Res. Public Health 2022, 19, 595. [Google Scholar] [CrossRef] [PubMed]
- Karhu, O.; Kansi, P.; Kuorinka, I. Correcting working postures in industry: A practical method for analysis. Appl. Ergon. 1977, 8, 199–201. [Google Scholar] [CrossRef]
- Li, K.W.; Lee, C.L. Postural analysis of four jobs on two building construction sites: An experience of using the OWAS method in Taiwan. J. Occup. Health 1999, 41, 183–190. [Google Scholar] [CrossRef]
- Enez, K.; Nalbantoğlu, S.S. Comparison of ergonomic risk assessment outputs from OWAS and REBA in forestry timber harvesting. Int. J. Ind. Ergon. 2019, 70, 51–57. [Google Scholar] [CrossRef]
- Lins, C.; Hein, A. Classification of body postures using smart workwear. BMC Musculoskelet. Disord. 2022, 23, 921. [Google Scholar] [CrossRef]
- National Institute for Occupational Safety and Health (NIOSH). Work Practice Guide for Manual Lifting (Pub. no: 81–122); U.S. Department of Health and Human Service, Centers for Disease Control: Washington, DC, USA, 1981.
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- Lee, K.S.; Park, H.S.; Chun, Y.H. The validity of the revised NIOSH weight limit in a Korean young male population: A psychophysical approach. Int. J. Ind. Ergon. 1996, 18, 181–186. [Google Scholar] [CrossRef]
- Ahmad, S.; Muzammil, M. Predicting the load constant of the revised NIOSH lifting equation based on demographics. Int. J. Occup. Saf. Ergon. 2022, 1–9. [Google Scholar] [CrossRef]
- Leemon, D.; Schimelpfenig, T. Wilderness injury, illness, and evacuation: National Outdoor Leadership School’s incident profiles, 1999–2002. Wilderness Environ. Med. 2003, 14, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Bubric, K.; Hedge, A. Differential patterns of laptop use and associated musculoskeletal discomfort in male and female college students. Work 2016, 55, 663–671. [Google Scholar] [CrossRef]
- Imagama, S.; Ando, K.; Kobayashi, K.; Seki, T.; Hamada, T.; Machino, M.; Ota, K.; Tanaka, S.; Morozumi, M.; Kanbara, S.; et al. Shoulder pain has most impact on poor quality of life among various types of musculoskeletal pain in middle-aged and elderly people: Yakumo study. Mod. Rheumatol. 2020, 30, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.C.; Lin, L.L.; Liu, C.J.; Fang, C.K.; Lin, M.H. Exploring the factors affecting musculoskeletal disorders risk among hospital nurses. PLoS ONE 2020, 15, e0231319. [Google Scholar] [CrossRef]
- Waongenngarm, P.; van der Beek, A.J.; Akkarakittichoke, N.; Janwantanakul, P. Perceived musculoskeletal discomfort and its association with postural shifts during 4-h prolonged sitting in office workers. Appl. Ergon. 2020, 89, 103225. [Google Scholar] [CrossRef] [PubMed]
- Besharati, A.; Daneshmandi, H.; Zareh, K.; Fakherpour, A.; Zoaktafi, M. Work-related musculoskeletal problems and associated factors among office workers. Int. J. Occup. Saf. Ergon. 2020, 26, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Cagnie, B.; Danneels, L.; Van Tiggelen, D.; De Loose, V.; Cambier, D. Individual and work related risk factors for neck pain among office workers: A cross sectional study. Eur. Spine J. 2007, 16, 679–686. [Google Scholar] [CrossRef]
- Cohen, S.P.; Hooten, W.M. Advances in the diagnosis and management of neck pain. BMJ 2017, 358, J3221. [Google Scholar] [CrossRef]
- Thetkathuek, A.; Meepradit, P. Work-related musculoskeletal disorders among workers in an MDF furniture factory in Eastern Thailand. Int. J. Occup. Saf. Ergon. 2016, 24, 207–217. [Google Scholar] [CrossRef]
- Bispo, L.G.M.; Moreno, C.F.; de Oliveira Silva, G.H.; de Albuquerque, N.L.B.; da Silva, J.M.N. Risk factors for work-related musculoskeletal disorders: A study in the inner regions of Alagoas and Bahia. Saf. Sci. 2022, 153, 105804. [Google Scholar] [CrossRef]
- Wu, T.N.; Liou, S.H.; Hsu, C.C.; Chao, S.L.; Liou, S.F.; Ko, K.N. Epidemiologic study of occupational injuries among foreign and native workers in Taiwan. Am. J. Ind. Med. 1997, 31, 623–630. [Google Scholar] [CrossRef]
- Gagnon, M.; Smyth, G. Biomechanical exploration on dynamic modes of lifting. Ergonomics 1992, 35, 329–345. [Google Scholar] [CrossRef] [PubMed]
- Tsuang, Y.H.; Schipplein, O.D.; Trafimow, J.H.; Andersson, G.B.J. Influence of body segment dynamics on loads at the lumbar spine during lifting. Ergonomics 1992, 35, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Diraneyya, M.M.; Ryu, J.; Abdel-Rahman, E.; Haas, C.T. Inertial motion capture-based whole-body inverse dynamics. Sensors 2021, 21, 7353. [Google Scholar] [CrossRef]
- Kee, D.; Karwowski, W. A comparison of three observational techniques for assessing postural loads in industry. Int. J. Occup. Saf. Ergon. 2007, 13, 3–14. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Taiwanese (n = 114) | Thai (n = 57) | |||
|---|---|---|---|---|
| Item | Mean | Standard Deviation | Mean | Standard Deviation |
| Age (years) | 38.5 | 8.7 | 36.5 | 7.5 |
| Stature (cm) | 166.0 | 7.8 | 166.5 | 5.9 |
| Body mass (kg) | 66.5 | 15.2 | 67.1 | 10.1 |
| Job tenure (years) | 6.3 | 7.3 | 3.6 | 3.8 |
| Workdays per week (days) | 5.1 | 0.3 | 5.2 | 0.4 |
| Sleeptime per day (hours) | 7.0 | 0.7 | 7.2 | 1.0 |
| Variable | Category | Taiwanese, n (%) | Thai, n (%) |
|---|---|---|---|
| Individual factors | |||
| Gender | Male Female | 81 (71.1) 33 (28.9) | 53 (93.0) 4 (7.0) |
| Dominant hands | Right Left | 82 (71.9) 21 (18.4) | 74 (66.7) 12 (21.0) |
| Others | 11 (9.7) | 14 (12.3) | |
| Exercise habits | None Sometimes or regular | 46 (40.3) 68 (59.7) | 5 (8.8) 52 (91.2) |
| Tobacco smoking | Yes | 89 (78.0) | 28 (49.1) |
| Alcohol drinking | Yes | 77 (67.5) | 49 (85.9) |
| Historical injuries | |||
| Musculoskeletal disorders | Yes | 74 (64.9) | 25 (43.9) |
| (from n = 74 or 25) | Neck/shoulder pain | 26 (35.1) | 2 (8.0) |
| Lower back pain | 18 (24.3) | 7 (28.0) | |
| Knee pain Scoliosis | 9 (12.2) 7 (9.6) | 4 (16.0) 0 (0) | |
| Full recovery (from n = 74 or 25) | No | 33 (45.0) | 7 (28.0) |
| Daily primary tasks | Computer operation | 40 (35.1) | 0 (0) |
| Roll production | 48 (42.1) | 26 (45.6) | |
| Gluing | 11 (9.6) | 18 (31.6) | |
| Cutting | 9 (7.9) | 9 (15.8) | |
| Packaging | 6 (5.3) | 4 (7.0) | |
| Task requirements (per day) | |||
| Sitting time | >4 h | 42 (36.8) | 4 (7.0) |
| Standing time | >4 h | 41 (36.0) | 51 (89.5) |
| Walking time | >4 h | 30 (26.3) | 49 (86.0) |
| Deep bending | >20 times | 46 (40.4) | 35 (61.4) |
| Twisting the waist | >20 times | 49 (42.9) | 30 (52.6) |
| Handling materials (>20 kg) | >20 times | 43 (37.7) | 36 (63.2) |
| Carrying distance | >5 m | 78 (68.4) | 28 (49.1) |
| Assistive devices usage | |||
| Assistive for carrying (from n = 77 or 50) | Yes Cart Hydraulic trolley Pallet truck | 77 (67.6) 23 (30.0) 13 (16.9) 16 (20.8) | 50 (87.7) 7 (14.0) 29 (58.0) 1 (2.0) |
| Personal protective equipment (from n = 23 or 46) | Yes Back support Wrist protector | 23 (20.2) 17 (73.9) 19 (82.6) | 46 (80.7) 43 (93.5) 6 (12.3) |
| The Present Study | ILOSH [9] | ||||
|---|---|---|---|---|---|
| Body Parts | Taiwanese (n = 114) | Thai (n = 57) | Difference between Two Groups | Entire Working Population (n = 17,757) | Manufacturing Industry (n = 3401) |
| Neck | 43.9 | 17.5 | −26.4 *** | 32.3 | 29.7 |
| Shoulders | 57.0 | 36.8 | −20.2 *** | 41.3 | 38.3 |
| Upper back | 25.4 | 28.1 | 2.7 | 22.3 | 20.8 |
| Elbows | 19.3 | 12.3 | −7.0 * | 20.5 | 19.6 |
| Lower back | 47.4 | 22.8 | −24.6 *** | 31.0 | 28.4 |
| Hands/wrists | 28.9 | 42.1 | 13.2 ** | 26.5 | 25.5 |
| Buttocks/legs | 17.5 | 31.6 | 14.1 ** | 11.8 | 10.3 |
| Knees | 36.8 | 15.8 | −21.0 *** | 16.9 | 12.6 |
| Ankles | 18.4 | 28.1 | 9.7 ** | 14.6 | 12.2 |
| Body Parts (Prevalence %) | Risk Factors | Category | n | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Taiwanese workers (n = 114) | Shoulders (57.0%) | Se Exercise habits Handling materials (>20 kg) Standing time Walking time | Male Female None Sometimes or regular ≤20 times per day >20 times per day ≤4 h per day >4 h per day ≤4 h per day >4 h per day | 81 33 46 68 71 43 73 41 84 30 | 1.00 4.55 ** 1.00 3.54 ** 1.00 5.48 ** 1.00 7.18 * 1.00 2.66 * | — 2.41–9.70 — 1.87–8.89 — 2.82–13.83 — 1.72–18.37 — 1.31–8.51 |
| Lower back (43.9%) | Deep bending Handling materials (>20 kg) Twisting the waist | ≤20 times per day >20 times per day ≤20 times/per day >20 times/per day ≤20 times/per day >20 times/per day | 68 46 71 43 65 49 | 1.00 4.23 * 1.00 3.186 * 1.00 4.51 ** | — 1.31–13.66 — 1.83–11.47 — 1.95–10.43 | |
| Neck (43.9%) | Sitting time Handling materials (>20 kg) Tobacco smoking | ≤4 h per day >4 h per day ≤20 times/per day >20 times/per day No Yes | 72 42 71 43 25 89 | 1.00 2.75 * 1.00 2.38 * 1.00 2.58 * | — 1.39–6.45 — 1.20–5.33 — 1.39–6.04 | |
| Knees (36.8%) | Age Handling materials (>20 kg) Standing time | ≤45 years >45 years ≤20 times/per day >20 times/per day ≤4 h per day >4 h per day | 74 40 71 43 73 41 | 1.00 3.97 ** 1.00 2.03 * 1.00 2.74 * | — 2.01–8.74 — 1.67–6.55 — 1.21–6.83 | |
| Thai workers (n = 57) | Hands/wrists (42.1%) | Handling materials (>20 kg) | ≤20 times/per day >20 times/per day | 21 36 | 1.00 1.96 * | — 1.18–4.15 |
| Shoulders (36.8%) | Handling materials (>20 kg) Tobacco smoking | ≤20 times/per day >20 times/per day No Yes | 21 36 29 28 | 1.00 2.11 * 1.00 2.77 * | — 1.27–5.93 — 1.85–9.50 | |
| Buttocks/legs (31.6%) | Standing time Carrying distance | ≤4 h per day >4 h per day ≤5 m >5 m | 6 51 29 28 | 1.00 7.82 * 1.00 3.89 ** | — 1.20–40.52 0.09–0.39 1.30–13.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-L.; Luo, W.-H. Comparative Ergonomic Study Examining the Work-Related Musculoskeletal Disorder Symptoms of Taiwanese and Thai Workers in a Tape Manufacturing Factory. Int. J. Environ. Res. Public Health 2023, 20, 2958. https://doi.org/10.3390/ijerph20042958
Chen Y-L, Luo W-H. Comparative Ergonomic Study Examining the Work-Related Musculoskeletal Disorder Symptoms of Taiwanese and Thai Workers in a Tape Manufacturing Factory. International Journal of Environmental Research and Public Health. 2023; 20(4):2958. https://doi.org/10.3390/ijerph20042958
Chicago/Turabian StyleChen, Yi-Lang, and Wen-Hua Luo. 2023. "Comparative Ergonomic Study Examining the Work-Related Musculoskeletal Disorder Symptoms of Taiwanese and Thai Workers in a Tape Manufacturing Factory" International Journal of Environmental Research and Public Health 20, no. 4: 2958. https://doi.org/10.3390/ijerph20042958