

Telerehabilitation as a Therapeutic Exercise Tool versus Face-to-Face Physiotherapy: A Systematic Review
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Evaluation of the Quality of the Studies
3. Results
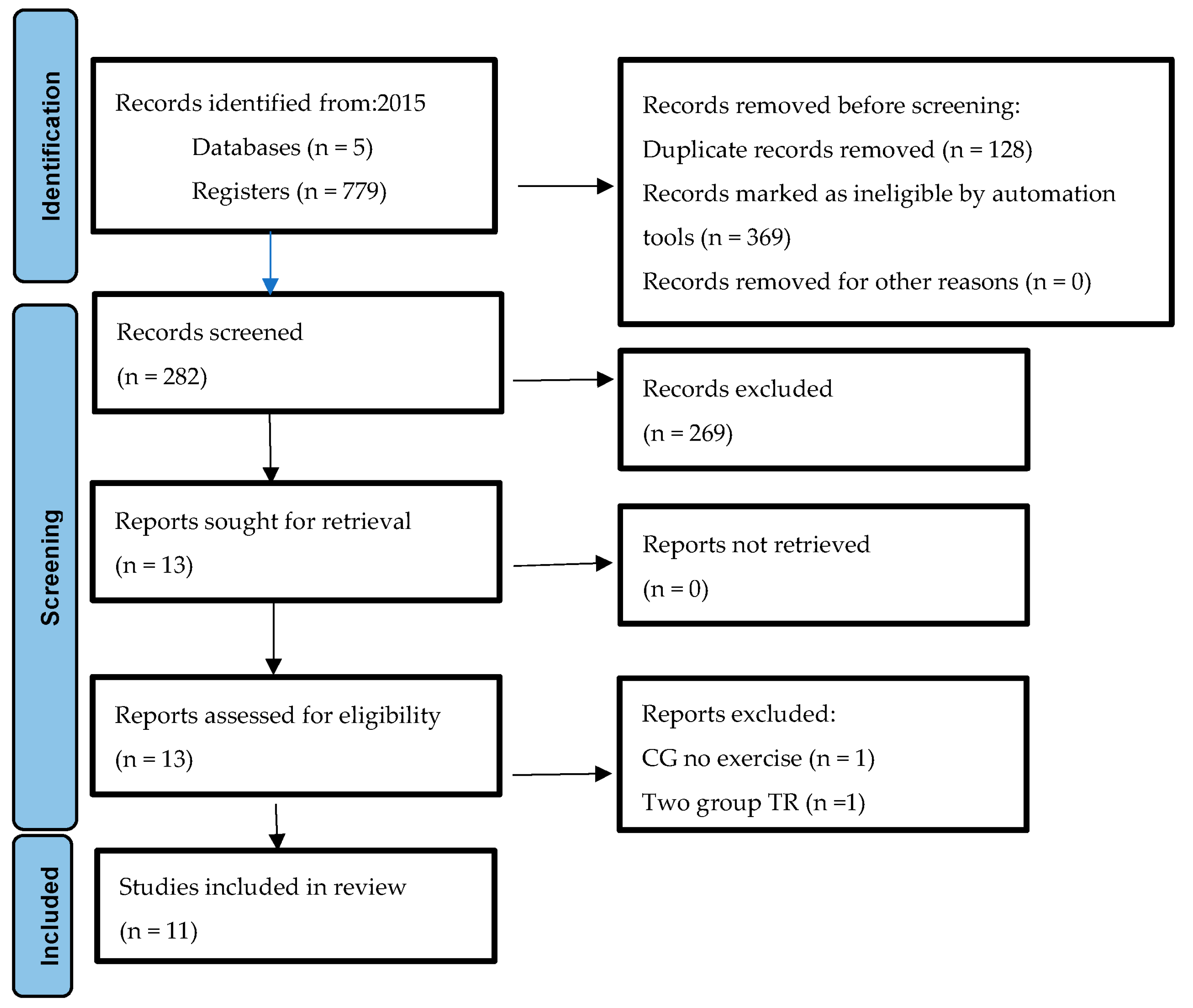
3.1. Literature Search and Screening
3.2. Quality of the Methods in the Included Studies
3.3. Characteristic of the Study
3.4. Participants
3.5. Fields of Activity
3.6. Type of Intervention, Exercise Program
3.7. Type of Device
3.8. Measures Considered
3.8.1. Quality of Life
3.8.2. Physical and Functional Level: Functional Scales
3.8.3. Satisfaction
3.8.4. Adherence
3.8.5. Cost
3.8.6. Pain
3.9. Limitations of the Studies Regarding the Use of Telerehabilitation
3.10. Pathologies Studied
3.11. Type of Device and Effectiveness
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WCPT. Report of the WCPT/INPTRA Digital Physical Therapy. 2020. Available online: https://world.physio/sites/default/files/2020-06/WCPT-INPTRA-Digital-Physical-Therapy-Practice-Task-force-March2020.pdf (accessed on 10 October 2022).
- Holland, A.E. Telephysiotherapy: Time to Get Online. J. Physiother. 2017, 63, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-Time Telerehabilitation for the Treatment of Musculoskeletal Conditions Is Effective and Comparable to Standard Practice: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; O’Leary, S.P.; Swete-Kelly, P.; Elwell, B.; Hess, S.; Litchfield, M.A.; McLoughlin, I.; Tweedy, R.; Raymer, M.; Hill, A.J.; et al. Agreement between Telehealth and In-Person Assessment of Patients with Chronic Musculoskeletal Conditions Presenting to an Advanced-Practice Physiotherapy Screening Clinic. Musculoskelet. Sci. Pract. 2018, 38, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, K.M.; Hodder, R.K.; Wiggers, J.; Williams, A.; Campbell, E.; Wolfenden, L.; Yoong, S.L.; Tzelepis, F.; Kamper, S.J.; Williams, C.M. Effectiveness of Telephone-Based Interventions for Managing Osteoarthritis and Spinal Pain: A Systematic Review and Meta-Analysis. PeerJ 2018, 6, e5846. [Google Scholar] [CrossRef] [PubMed]
- Rawstorn, J.C.; Gant, N.; Direito, A.; Beckmann, C.; Maddison, R. Telehealth Exercise-Based Cardiac Rehabilitation: A Systematic Review and Meta-Analysis. Heart 2016, 102, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Daines, L.; Campbell, C.; Mckinstry, B.; Weller, D.; Pinnock, H. Telehealth Interventions to Support Self-Management of Long-Term Conditions: A Systematic Metareview of Diabetes, Heart Failure, Asthma, Chronic Obstructive Pulmonary Disease, and Cancer. J. Med. Internet Res. 2017, 19, e172. [Google Scholar] [CrossRef]
- Hinman, R.S.; Nelligan, R.K.; Bennell, K.L.; Delany, C. “Sounds a Bit Crazy, But It Was Almost More Personal:” A Qualitative Study of Patient and Clinician Experiences of Physical Therapist–Prescribed Exercise For Knee Osteoarthritis Via Skype. Arthritis Care Res. 2017, 69, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-NCoV) Infection Is Suspected Interim Guidance V1.2. 13 March 2020. Available online: https://www.who.int/publications/i/item/10665-332299 (accessed on 5 September 2022).
- aefi Reordenación de La Actividad de Fisioterapia En Atención Primaria. 2020. Available online: https://world.physio/sites/default/files/2020-06/Reordenacion-actividad-UFAP-Abril-2020.pdf (accessed on 8 July 2022).
- Smidt, N.; de Vet, H.C.W.; Bouter, L.M.; Dekker, J.; Arendzen, J.H.; de Bie, R.A.; Bierma-Zeinstra, S.M.A.; Helders, P.J.M.; Keus, S.H.J.; Kwakkel, G.; et al. Effectiveness of Exercise Therapy: A Best-Evidence Summary of Systematic Reviews. Aust. J. Physiother. 2005, 51, 71–85. [Google Scholar] [CrossRef] [Green Version]
- Sampath Kumar, A.; Maiya, A.G.; Shastry, B.A.; Vaishali, K.; Ravishankar, N.; Hazari, A.; Gundmi, S.; Jadhav, R. Exercise and Insulin Resistance in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Ann. Phys. Rehabil. Med. 2019, 62, 98–103. [Google Scholar] [CrossRef]
- Girdler, S.J.; Confino, J.E.; Woesner, M.E. Exercise as a Treatment for Schizophrenia: A Review. Psychopharmacol. Bull. 2019, 49, 56–69. [Google Scholar]
- Pedersen, B.K.; Saltin, B. Exercise as Medicine—Evidence for Prescribing Exercise as Therapy in 26 Different Chronic Diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horton, E.J.; Mitchell, K.E.; Johnson-Warrington, V.; Apps, L.D.; Sewell, L.; Morgan, M.; Taylor, R.S.; Singh, S.J. Comparison of a Structured Home-Based Rehabilitation Programme with Conventional Supervised Pulmonary Rehabilitation: A Randomised Non-Inferiority Trial. Thorax 2018, 73, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Tsai, L.L.Y.; McNamara, R.J.; Moddel, C.; Alison, J.A.; McKenzie, D.K.; McKeough, Z.J. Home-Based Telerehabilitation via Real-Time Videoconferencing Improves Endurance Exercise Capacity in Patients with COPD: The Randomized Controlled TeleR Study. Respirology 2017, 22, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Stepnowska, M.; Leszczyńska-Iwanicka, K.; Piotrowska, D.; Kowalska, M.; Tylka, J.; Piotrowski, W.; Piotrowicz, R. Quality of Life in Heart Failure Patients Undergoing Home-Based Telerehabilitation versus Outpatient Rehabilitation—A Randomized Controlled Study. Eur. J. Cardiovasc. Nurs. 2015, 14, 256–263. [Google Scholar] [CrossRef]
- Verhagen, A.P.; de Vet, H.C.W.; de Bie, R.A.; Kessels, A.G.H.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Jin, W.; Dong, W.S.; Jin, Y.; Qiao, F.L.; Zhou, Y.F.; Ren, C.C. Effects of Home-Based Telesupervising Rehabilitation on Physical Function for Stroke Survivors with Hemiplegia: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2017, 96, 152–160. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Arroyo-Morales, M.; Lozano-Lozano, M.; Fernández-Lao, C.; Martín-Martín, L.; Del-Moral-Ávila, R.; Cantarero-Villanueva, I. Effect of an Internet-Based Telehealth System on Functional Capacity and Cognition in Breast Cancer Survivors: A Secondary Analysis of a Randomized Controlled Trial. Support. Care Cancer 2017, 25, 3551–3559. [Google Scholar] [CrossRef]
- Hwang, R.; Bruning, J.; Morris, N.R.; Mandrusiak, A.; Russell, T. Home-Based Telerehabilitation Is Not Inferior to a Centre-Based Program in Patients with Chronic Heart Failure: A Randomised Trial. J. Physiother. 2017, 63, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moffet, H.; Tousignant, M.; Nadeau, S.; Mérette, C.; Boissy, P.; Corriveau, H.; Marquis, F.; Cabana, F.; Belzile, É.L.; Ranger, P.; et al. Patient Satisfaction with In-Home Telerehabilitation after Total Knee Arthroplasty: Results from a Randomized Controlled Trial. Telemed. e-Health 2017, 23, 80–87. [Google Scholar] [CrossRef]
- Pastora-Bernal, J.M.; Martín-Valero, R.; Barón-López, F.J.; Moyano, N.G.; Estebanez-Pérez, M.J. Telerehabilitation after Arthroscopic Subacromial Decompression Is Effective and Not Inferior to Standard Practice: Preliminary Results. J. Telemed. Telecare 2018, 24, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Maddison, R.; Rawstorn, J.C.; Stewart, R.A.H.; Benatar, J.; Whittaker, R.; Rolleston, A.; Jiang, Y.; Gao, L.; Moodie, M.; Warren, I.; et al. Effects and Costs of Real-Time Cardiac Telerehabilitation: Randomised Controlled Non-Inferiority Trial. Heart 2019, 105, 122–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, M.; Bourke, M.; Crossley, K.; Russell, T. Telerehabilitation Is Non-Inferior to Usual Care Following Total Hip Replacement—A Randomized Controlled Non-Inferiority Trial. Physiotherapy 2020, 107, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettger, J.P.; Green, C.L.; Holmes, D.N.; Chokshi, A.; Iii, R.C.M.; Hoch, B.T.; De Leon, A.J.; Aluisio, F.; Seyler, T.M.; Del Gaizo, D.J.; et al. Effects of Virtual Exercise Rehabilitation In-Home. J. Bone Joint Surg. Am. 2020, 0, 101–109. [Google Scholar]
- Tarakci, E.; Tarakci, D.; Hajebrahimi, F.; Budak, M. Supervised Exercises versus Telerehabilitation. Benefits for Persons with Multiple Sclerosis. Acta Neurol. Scand. 2021, 144, 303–311. [Google Scholar] [CrossRef]
- Özden, F.; Sarı, Z.; Karaman, Ö.N.; Aydoğmuş, H. The Effect of Video Exercise-Based Telerehabilitation on Clinical Outcomes, Expectation, Satisfaction, and Motivation in Patients with Chronic Low Back Pain. Ir. J. Med. Sci. 2021, 191, 1229–1239. [Google Scholar] [CrossRef]
- Lee, Y.; Jung, K.B. Effect of Physiotherapy to Correct Rounded Shoulder Posture in 30 Patients During the COVID-19 Pandemic in South Korea Using a Telerehabilitation Exercise Program to Improve Posture, Physical Function, and Reduced Pain, with Evaluation of Patient Satisfac. Med. Sci. Monit. 2022, 28, e938926. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Álvarez-Bueno, C.; Cavero-Redondo, I.; Torres-Costoso, A.; Pozuelo-Carrascosa, D.P.; Reina-Gutiérrez, S.; Pascual-Morena, C.; Martínez-Vizcaíno, V. Best Exercise Options for Reducing Pain and Disability in Adults with Chronic Low Back Pain: Pilates, Strength, Core-Based, and Mind-Body. A Network Meta-Analysis. J. Orthop. Sports Phys. Ther. 2022, 52, 505–521. [Google Scholar] [CrossRef]
- Borisovskaya, A.; Chmelik, E.; Karnik, A. Exercise and Chronic Pain. Adv. Exp. Med. Biol. 2020, 1228, 233–253. [Google Scholar] [CrossRef]
- Ma, Y.; Luo, J.; Wang, X.Q. The Effect and Mechanism of Exercise for Post-Stroke Pain. Front. Mol. Neurosci. 2022, 15, 1074205. [Google Scholar] [CrossRef]
- Rutkowski, S. Management Challenges in Chronic Obstructive Pulmonary Disease in the COVID-19 Pandemic: Telehealth and Virtual Reality. J. Clin. Med. 2020, 10, 1261. [Google Scholar] [CrossRef]
- Torriani-Pasin, C.; Domingues, V.L.; de Freitas, T.B.; da Silva, T.A.; Caldeira, M.F.; Júnior, R.P.A.; Lara, A.R.F.; Antonio, B.D.A.; Palma, G.C.D.S.; Makhoul, M.P.; et al. Adherence Rate, Barriers to Attend, Safety and Overall Experience of a Physical Exercise Program via Telemonitoring during COVID-19 Pandemic for Individuals with Parkinson’s Disease: A Feasibility Study. Physiother. Res. Int. 2022, 27, e1959. [Google Scholar] [CrossRef] [PubMed]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise Prescription for Patients with Multiple Sclerosis; Potential Benefits and Practical Recommendations. BMC Neurol. 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Kampshoff, C.S.; Jansen, F.; van Mechelen, W.; May, A.M.; Brug, J.; Chinapaw, M.J.M.; Buffart, L.M. Determinants of Exercise Adherence and Maintenance among Cancer Survivors: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 80. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Zadravec, K.; Bland, K.A.; Chesley, E.; Wolf, F.; Janelsins, M.C. The Effect of Exercise on Cancer-Related Cognitive Impairment and Applications for Physical Therapy: Systematic Review of Randomized Controlled Trials. Phys. Ther. 2020, 100, 523–542. [Google Scholar] [CrossRef]
- Liu, X.; Wang, Y.Q.; Xie, J. Effects of Breathing Exercises on Patients with Lung Cancer. Oncol. Nurs. Forum 2019, 46, 303–317. [Google Scholar] [CrossRef]
- Batalik, L.; Pepera, G.; Papathanasiou, J.; Rutkowski, S.; Líška, D.; Batalikova, K.; Hartman, M.; Felšőci, M.; Dosbaba, F. Is the Training Intensity in Phase Two Cardiovascular Rehabilitation Different in Telehealth versus Outpatient Rehabilitation? J. Clin. Med. 2021, 10, 4069. [Google Scholar] [CrossRef]
- Bei, Y.; Xu, T.; Lv, D.; Yu, P.; Xu, J.; Che, L.; Das, A.; Tigges, J.; Toxavidis, V.; Ghiran, I.; et al. Exercise-Induced Circulating Extracellular Vesicles Protect against Cardiac Ischemia–Reperfusion Injury. Basic Res. Cardiol. 2017, 112, 38, Erratum in Basic Res. Cardiol. 2019, 114, 44. [Google Scholar] [CrossRef] [Green Version]
- Chumbler, N.R.; Li, X.; Quigley, P.; Morey, M.C.; Rose, D.; Griffiths, P.; Sanford, J.; Hoenig, H. A Randomized Controlled Trial on Stroke Telerehabilitation: The Effects on Falls Self-Efficacy and Satisfaction with Care. J. Telemed. Telecare 2015, 21, 139–143. [Google Scholar] [CrossRef] [Green Version]
- Lawford, B.J.; Delany, C.; Bennell, K.L.; Hinman, R.S. “I Was Really Pleasantly Surprised”: Firsthand Experience and Shifts in Physical Therapist Perceptions of Telephone-Delivered Exercise Therapy for Knee Osteoarthritis—A Qualitative Study. Arthritis Care Res. 2019, 71, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Liu, W.; He, D.; Huang, B.; Xiao, D.; Peng, Y.; He, Y.; Hu, H.; Chen, M.; Huang, D. Telehealth Interventions versus Center-Based Cardiac Rehabilitation of Coronary Artery Disease: A Systematic Review and Meta-Analysis. Eur. J. Prev. Cardiol. 2015, 22, 959–971. [Google Scholar] [CrossRef] [PubMed]
- Suso-Martí, L.; La Touche, R.; Herranz-Gómez, A.; Angulo-Díaz-Parreño, S.; Paris-Alemany, A.; Cuenca-Martínez, F. Effectiveness of Telerehabilitation in Physical Therapist Practice: An Umbrella and Mapping Review with Meta-Meta-Analysis. Phys. Ther. 2021, 101, pzab075. [Google Scholar] [CrossRef] [PubMed]
- Stefanakis, M.; Batalik, L.; Antoniou, V.; Pepera, G. Safety of Home-Based Cardiac Rehabilitation: A Systematic Review. Heart Lung 2022, 55, 117–126. [Google Scholar] [CrossRef]


{kind=link}
| Database | Strategy | Results |
|---|---|---|
| Pubmed | (“telerehabilitation”[MeSH Terms] OR “telerehabilitation”) AND (“Exercise Therapy”[Mesh] OR “Exercise Therapy”) | 295 |
| Embase | (“telerehabilitation”/exp OR telerehabilitation) AND “exercise therapy”: ti,ab,kw | 51 |
| PEDro | telerehabilitation exercise | 88 |
| Scopus | (TITLE-ABS-KEY (telerehabilitation) AND TITLE-ABS-KEY (“exercise therapy”) | 338 |
| SPORTDiscus | TI telerehabilitation AND AB exercise therapy | 7 |
| Parameters | Description |
|---|---|
| Review Question | Therapeutic physical exercise programs carried out through telerehabilitation are as effective as face-to-face exercise. |
| Population | The people in this study are over 18 years of age and have been prescribed an exercise program as a treatment. |
| Intervention | Supervised physical exercise program through telerehabilitation |
| Comparator | Physical exercise program carried out on-site |
| Outcomes | Functionality, quality of life, level of satisfaction, adherence to treatment, pain and costs. |
| Study Design | Randomized clinical trials (RCT) |
| Trial | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | PEDro Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Piotrowicz E. 2015 [18] | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 5 |
| Chen J. 2017 [20] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Galiano-Castillo N. 2017 [21] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Hwuang R. 2017 [22] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Moffet H. 2017 [23] | Yes | No | Yes | No | No | Yes | Yes | No | Yes | Yes | 6 |
| Pastora-Bernal JM. 2018 [24] | Yes | No | Yes | No | No | Yes | Yes | No | Yes | Yes | 6 |
| Maddison R. 2019 [25] | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Nelson M. 2020 [26] | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Prvu Bettger J. 2020 [27] | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Tarakci E. 2021 [28] | Yes | No | Yes | No | No | Yes | No | No | Yes | Yes | 5 |
| Özden F. 2022 [29] | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Author and Year | Country | Participants | N Gender % | Age (Average) | Sample Size Groups | Study Objectives | Pathology | Quality |
|---|---|---|---|---|---|---|---|---|
| Piotrowicz E. 2015 [18] | Warsaw (Poland) | 152 | M: 117 (65) TR 64 CG 53 F: 63 (35) TR 21 CG 42 | TR 56.4 ± 10.9 CG 60.05 ± 8.8 | TR: 77 GC: 75 | To assess changes in the quality of life of patients with heart failure | Cardiac | 5 |
| Chen J. 2017 [20] | Shangahi (China) | 54 | M: 33 (61.11) TR 18 CG 15 F: 21 (38.89) TR 9 CG 12 | TR 66.52 ± 12.08 CG 66.15 ± 12.33 | TR: 27 CG: 27 | To assess physical function and determine whether it can be helpful to caregivers | Neurologic | 8 |
| Galiano-Castillo N. 2017 [21] | Granada (Spain) | 81 | F: 76 (100) TR 39 CG 37 | TR 47.4 ± 9.6 GC 49.2 ± 7.9 | TR: 40 CG: 41 | To improve functional capacity and cognition | Breast cancer | 8 |
| Hwang R. 2017 [22] | Brisbane (Australia) | 53 | M: 40 (75) TR 19 CG 21 F: 13 (25) TR 5 CG 8 | TR 68 ± 14 CG 67 ± 11 | TR: 24 CG: 29 | To prove non-inferiority in terms of functional capacity, muscle strength, quality of life, patient satisfaction and attendance rates | Cardiac | 8 |
| Moffet H. 2017 [23] | Québec (Canada) | 205 | M: 89 (48.9) TR 35 CG 54 F: 93 (51.1) TR 49 CG 44 | TR 65 ± 8 CG 67 ± 8 | TR: 84 CG: 98 | To compare patients’ satisfaction levels | Musculoskeletal; total knee arthroplasty | 6 |
| Pastora-Bernal JM. 2018 [24] | Málaga (Spain) | 18 | M: 10 (55.55) TR 4 CG 6 F: 8 (44.45) TR 4 GC 4 | TR 49.63 ± 10.08 CG 54.8 ± 11.84 | TR: 8 CG: 10 | To assess the feasibility and effectiveness of customizable telerehabilitation intervention | Musculoskeletal (shoulder) | 6 |
| Maddison R. 2019 [25] | Auckland y Tauranga (New Zealand) | 162 | M: 139 TR 69 CG 70 F: 23 (14.2) TR 13 CG 10 | TR 61.0 ± 13.3 CG 61.5 ± 12.2 | TR: 82 CG: 80 | To compare the effects and costs of cardiac telerehabilitation | Cardiac | 8 |
| Nelson M. 2020 [26] | Brisbane (Australia) | 70 | M: 26 (37.14) TR 12 CG 14 F: 44 (62.86) TR 23 GC 21 | TR 62 ± 9 CG 67 ± 11 | TR: 35 CG: 35 | To determine whether outpatient physiotherapy using telerehabilitation is as effective as face-to-face physiotherapy after total hip replacement | Musculoskeletal PTC | 7 |
| Prvu Bettger J. 2020 [27] | North Caroline (USA) | 306 | M: 114 (37.5) TR 61 CG 53 F: 190 (62.5) TR 90 GC 100 | TR 65.4 ± 7.7 CG 65.1 ± 9.2 | TR: 151 CG: 153 | To determine whether outpatient physiotherapy using telerehabilitation is as effective as face-to-face physiotherapy | Musculoskeletal; total knee arthroplasty. | 6 |
| Tarakci E. 2021 [28] | Estambúl (Turkey) | 41 | M: 7 (23.33) TR 4 CG 3 F: 23 (76.66) TR 11 GC 12 | TR 39.46 ± 10.59 CG 41.00 ± 11.09 | TR: 15 CG: 15 | To evaluate the effectiveness of telerehabilitation on fatigue, health status, quality of life and daily life activities | Neurologic; multiple sclerosis | 5 |
| Özden F. 2022 [29] | Muğla Sıtkı Koçman (Turkey) | 54 | M: 19 (38) TR 11 CG 8 F: 31 (62) TR 14 GC 17 | TR 40.1 ± 1.6 CG 42.3 ± 1.6 | TR: 25 CG: 25 | To assess pain, function, quality of life, expectations, satisfaction and motivation in patients with chronic low back pain | Musculoskeletal; chronic low back pain | 8 |
| Author and Year | Type of Device | Type of Exercise | Outcome | Time of Measuring | Session Frequency/Treatment Duration | Test | Result |
|---|---|---|---|---|---|---|---|
| Piotrowicz E. 2015 [18] | Remote equipment for telemonitoring and supervised exercise training (EHO 6 device transmit the ECG) and a mobile phone | Cardiac rehabilitation through gait training. Telematic TR and CG with cycloergometer. | Quality of life | At baseline and at 8 weeks, Quality of life | 3 times per week/8 weeks | SF-36 | Both groups significantly improved quality of life. GI patients improved mainly in mental categories. GC improved their overall physical well-being. |
| Chen J. 2017 [20] | Audio-video system (videoconferencing), biofeedback instrument and data logging | TR individualized physical exercise plan + neuromuscular stimulation (ETNS) and CG performs ambulatory RHB with the same type of exercises as TR. | Functionality | At baseline, at end (12 weeks) and follow-up at 24 weeks | 1 h 2 times per day/12 weeks | BARTHEL, MBI, BBS, MRS | TR as effective as conventional RHB for functional recovery in stroke. It is a way to overcome barriers for stroke survivors living in rural areas. It is likely to reduce costs and travel times. |
| Galiano-Castillo N. 2017 [21] | Web application “e-CUIDATE” | Both groups exercise program aimed at functional and cognitive recovery | Functionality, Adherence to treatment | At baseline, at the end of the intervention (8 weeks) and follow-up (6-month follow up) | 90 min per day, 3 times per week/8 weeks | 6MWT, ACT, TMT, Diarios de ejercicios | Both groups showed improvements in 6MWT and also differences between groups with better results for TR. ACT total TR improves compared to CG. TMT unchanged. |
| Hwang R. 2017 [22] | Program web-based exercises using videoconferencing software | TR cardiac RHB exercises and education in real time and CG traditional hospital program with same frequency and same duration as TR | Functionality, quality of life, level of satisfaction | At start-up, 12 weeks and 24 weeks | Twice a week/12 weeks | 6MWD, BOOMER, TUGT, EQ-5D, MLWHFQ, CSQ-8 | The intervention is at least as effective as rehabilitation without telerehabilitation, promotes higher frequency of attendance and improves equity of access to cardiac RHB programs |
| Moffet H. 2017 [23] | TR platform and videoconferencing system | Similar exercise program for both groups based on functionality. Exercises aimed at mobility recovery and strengthening. | Functionality, level of satisfaction | Before surgery, in the hospital, after physical therapy and at 4 months. | 16 interventions of 45 to 60 min every 2 weeks, for 8 weeks/8 weeks | HCSQ, WOMAC, KOOS, 6MWD, | Similar level of satisfaction between IG and CG. The greater the improvements in WOMAC and KOOS, the higher the level of satisfaction. The use of TR improves access to rehabilitation services. |
| Pastora-Bernal JM. 2018 [24] | Web and videoconferencing-based system | Both groups strengthening and joint amplitude exercises, web-based TR and regular face-to-face physiotherapy CG | Functionality | At baseline, 4, 8 and 12 weeks | 5 days per week/12 weeks | Constant-Murley Test | Evidence of efficacy of TR, physical and functional improvements in both groups. Non-significant trend of greater improvements in TR. |
| Maddison R. 2019 [25] | REMOTE-CR telerehabilitation system | TR individualized exercise using customized platform and traditional cardiac CG RHB | Functionality, Quality of life, Adherence to treatment, Cost-utility analysis | Start-up, 12 weeks and 24 weeks | 12 weeks | VO2 max, EQ-5D, Exercise adherence was calculated as the completion of prescribed exercise sessions prescribed. QALY | Efficient and cost-effective alternative, individualized intervention and overcoming accessibility barriers, implementation costs of the REMOTE-CR program were substantially lower than those of CBexCR. |
| Nelson M. 2020 [26] | Apple iPad technology and Wellpepper clinic internet application and eHAB (real time videoconferencing) | CG strengthening and gait re-education exercises. TR same exercise content as GC via internet application. | Quality of life, Functionality, Level of satisfaction | Onset (before surgery), at discharge from hospital, 6 weeks and 6 months after operation | 3 times per week/6 weeks | QOLS, HOOS, TUG, SF-12, EQ-5D-5L, satisfaction survey, SUS | Easy access for the population, high levels of satisfaction, physical and functional results not inferior to those obtained with traditional physical therapy. Program compliance rate in favor of TR |
| Prvu Bettger J. 2020 [27] | VERA (virtual exercise rehabilitation assistant) | Prescribed exercises varied by therapist and patient in both groups. Sports and recreational exercises (squatting, running, jumping, twisting/pivoting, kneeling) were included. | Functionality, cost | At baseline, 6 weeks, 12 weeks | Frequency and duration NOT restricted/12 weeks | KOOS, PROMIS, Cost analysis. | Lower costs in TR, fewer rehospitalizations than in GC, no inferiority in terms of knee flexion–extension and gait speed. |
| Tarakci E. 2021 [28] | Video calls | Functionality, quality of life, health profile, fatigue | Functionality, quality of life, health profile, fatigue | At baseline and end (12 weeks) | 3 sessions per week/12 weeks | FIM, NHP-I, FSS, QOLS | Telerehabilitation can help improve quality of life and activities of daily living although supervised exercise without TR may be more beneficial for fatigue and health profile. |
| Özden F. 2022 [29] | Exercise videos Fizyoweb system | Both groups: lumbar and lower back stretching exercises, abdominal strengthening, spinal column mobility. | Functionality, Quality of life, Adherence to treatment, Pain | At baseline and 8 weeks | once daily for 8 weeks | TUG, FTST, ODI, TSK, SF-36, EARS, VAS | The TR protocol has a positive effect on all clinical parameters (pain, functionality, quality of life, kinesiophobia, motivation, satisfaction) compared to conventional RHB. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Tomás, M.T.; Burillo-Lafuente, M.; Vicente-Parra, A.; Sanz-Rubio, M.C.; Suarez-Serrano, C.; Marcén-Román, Y.; Franco-Sierra, M.Á. Telerehabilitation as a Therapeutic Exercise Tool versus Face-to-Face Physiotherapy: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4358. https://doi.org/10.3390/ijerph20054358
Muñoz-Tomás MT, Burillo-Lafuente M, Vicente-Parra A, Sanz-Rubio MC, Suarez-Serrano C, Marcén-Román Y, Franco-Sierra MÁ. Telerehabilitation as a Therapeutic Exercise Tool versus Face-to-Face Physiotherapy: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(5):4358. https://doi.org/10.3390/ijerph20054358
Chicago/Turabian StyleMuñoz-Tomás, Mª Teresa, Mario Burillo-Lafuente, Araceli Vicente-Parra, Mª Concepción Sanz-Rubio, Carmen Suarez-Serrano, Yolanda Marcén-Román, and Mª Ángeles Franco-Sierra. 2023. "Telerehabilitation as a Therapeutic Exercise Tool versus Face-to-Face Physiotherapy: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 5: 4358. https://doi.org/10.3390/ijerph20054358