
What Are the Experiences of Mental Health Practitioners Involved in a Coroner’s Inquest and Other Inquiry Processes after an Unexpected Death of a Patient? A Systematic Review and Thematic Synthesis of the Literature




Abstract
1. Introduction
2. Methods
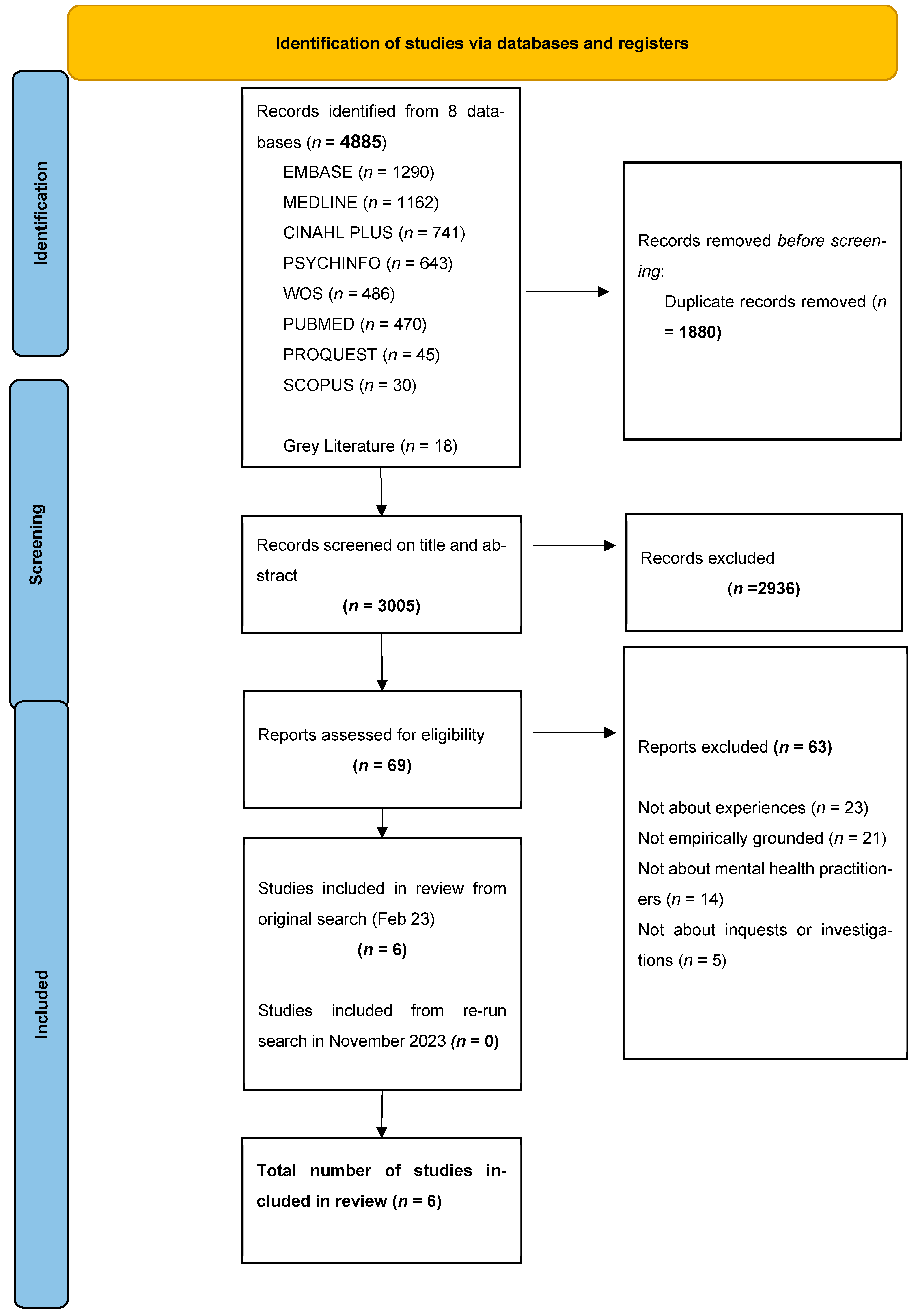
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
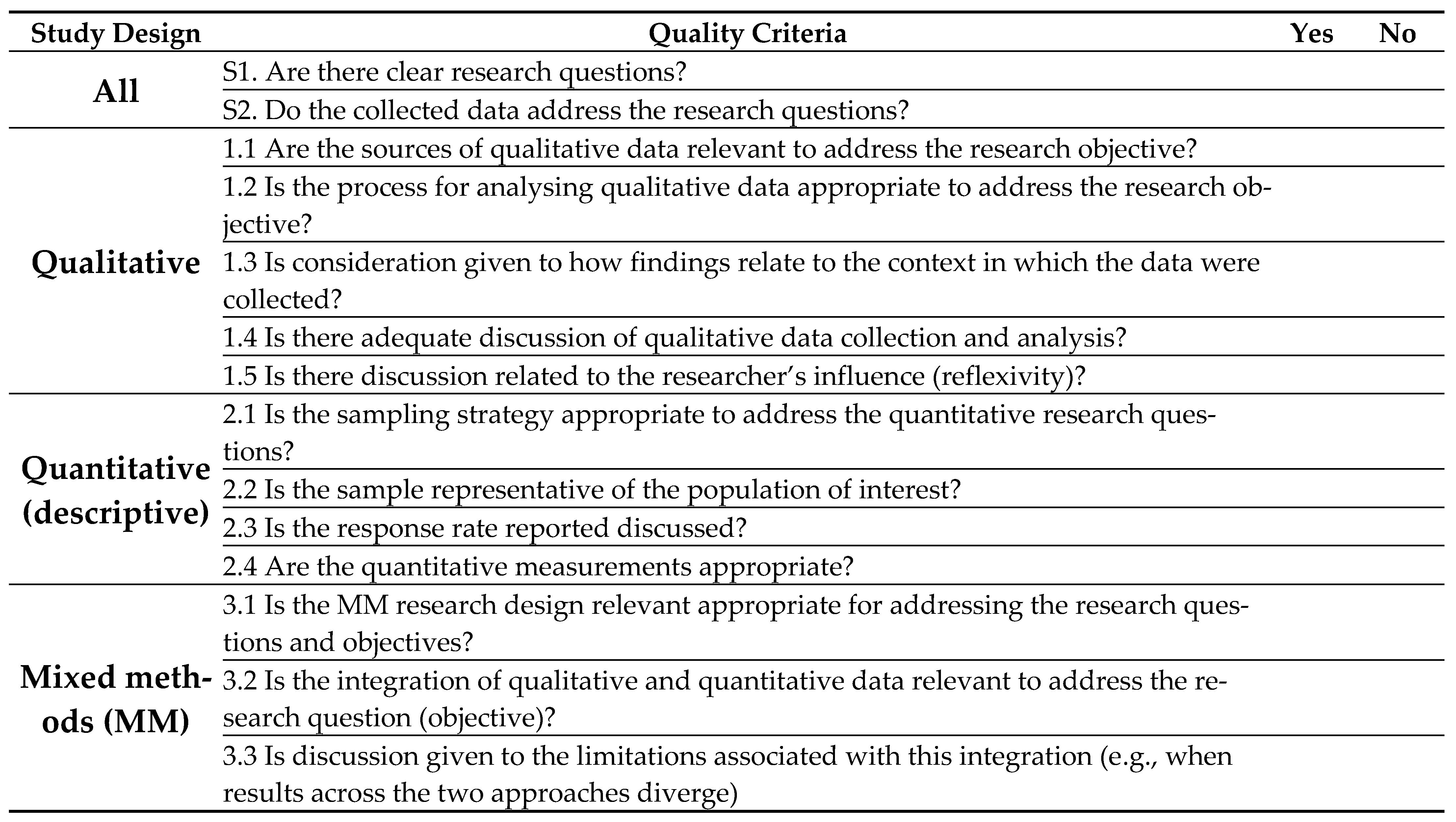
2.3. Data Extraction and Quality Appraisal
2.4. Data Analysis
2.5. Analytic Rigour
3. Results
3.1. Study Characteristics
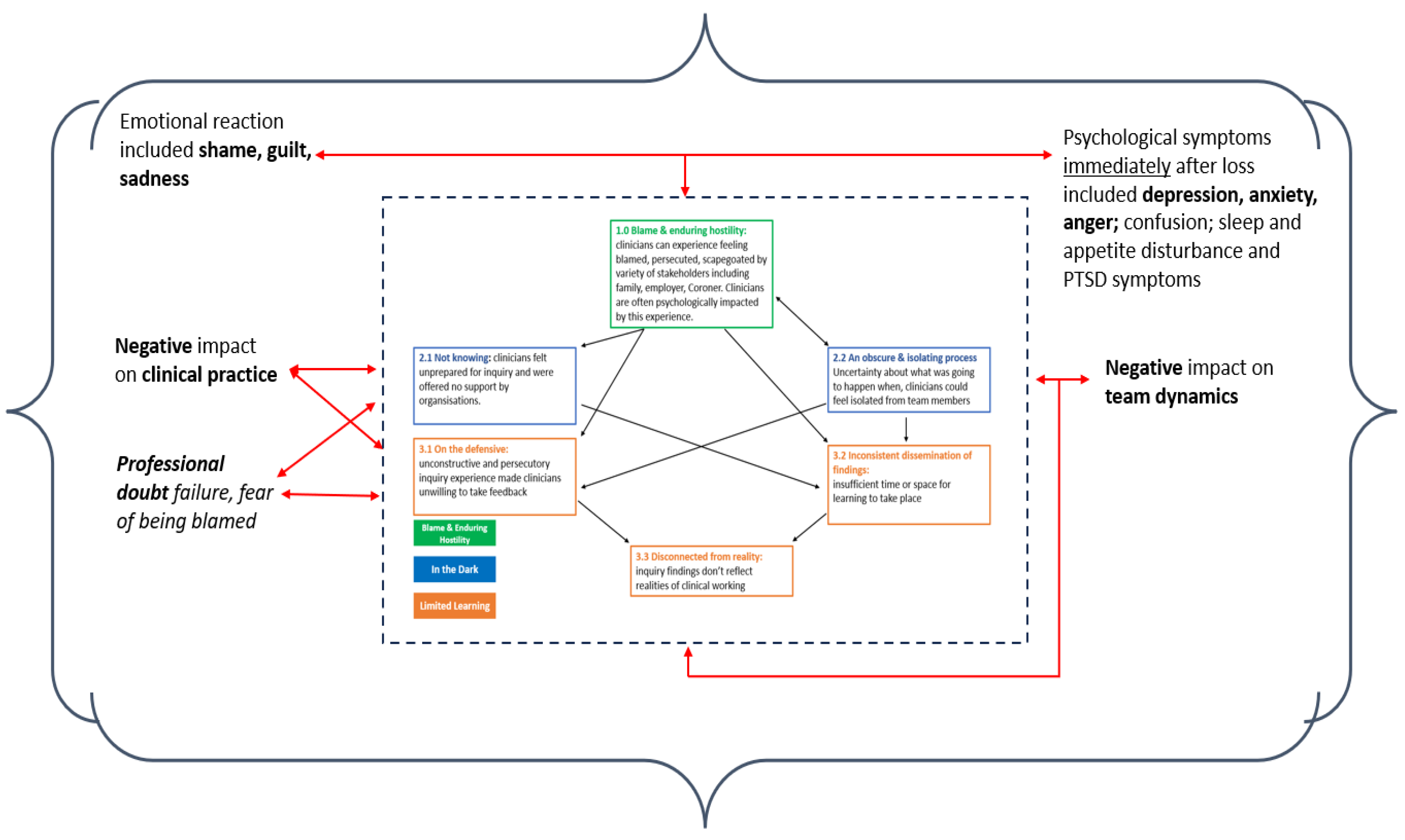
3.2. Thematic Synthesis
3.3. Blame and Enduring Hostility
“People go in with a sense of ‘I’m going to be crucified’. It’s an anxiety-provoking episode”.Psychiatrist/homicide [31]
“The suicide was upsetting, but attending the coroner’s court was traumatic for me. It made me feel like people were out to blame”.Consultant Psychiatrist/suicide [28]
“The whole experience was negative, humiliating, criticising”.Forensic Psychiatrist(s)/homicide [30]
“I was devastated by the incident and subsequent inquiry. I considered leaving medicine early”.Consultant Psychiatrist/homicide [32]
“The family were very angry and felt their loved one’s death was preventable; they were angry with me personally”.Social Worker/suicide [27]
“The patient’s family were very thoughtful and supportive towards my team even in the midst of their grief”.Consultant Psychiatrist/suicide [28]
4. In the Dark
4.1. Not Knowing
“It would help to know what to expect, what about GMC [General Medical Council] referral, what do I do to prepare?”.Forensic Psychiatrist/homicide [30]
“There’s all sorts of other things circulating…that becomes a bit like rumours and gossip because there isn’t a clear process for that [information] to get to those staff”.Psychiatrist/homicide [31]
“Very good. Interviewed for 3 h […] by trust lawyer the next day, who drafted my statement that I needed for the next 2+ years […] really wise and helpful”.Consultant Psychiatrist/homicide [32]
“My team, manager, clinical director and CEO [chief executive officer] were utterly amazing. CEO called me to check in. Team looked after me. Manager called ahead to a meeting I was chairing to make sure they looked after me”.Consultant Psychiatrist/homicide [32]
4.2. An Obscure and Isolating Process
“The internal inquiry blamed everyone and was poorly managed. The interview was traumatic, a panel of 8 people, arguing with each other”.Forensic Psychiatrist/homicide [30]
“There was a time when the team did not even talk to each other, it impacted team cohesiveness”.Psychiatrist/homicide [31]
“It made me feel unable to trust colleagues who tried to shift blame from themselves”.
“‘It was like a big dysfunctional family… a bird’s nest of bad relationships… where the abused children turn on each other”.Forensic Psychiatrist(s)/homicide [30]
“I learned the meaning of the term Kafka-esque … being prosecuted for something but you don’t know what, and … things around you keep changing in an inexplicable way”.Forensic Psychiatrist/homicide [30]
“harrowing, terrifying, sobering, felt like I was going on trial, but the coroner was clear and made it easier”.Nurse/suicide [27]
5. Limited Learning
5.1. Inconsistent Dissemination of Findings
“Maybe there needs to be a greater dialogue between the people doing the inquiry and the service unit in question, to see how things could be framed in a way that was relevant, meaningful [and] achievable”.(Psychiatrist)/homicide [31]
5.2. Disconnected from Reality
“Too many of them [recommendations] were so poorly worded or generic they didn’t actually make sense as a statement, let alone make sense to the clinical team”.Psychiatrist/homicide [31]
“I saw them as biased and unfair”.Forensic psychiatrist/homicide [30]
“…the medical member’s punitive approach and the rush to judgment. I also thought that there was some sadistic pleasure in shafting another colleague”.Forensic Psychiatrist/homicide [30]
5.3. On the Defensive
“There is no point after an incident, people coming in and saying we don’t want to blame anyone, we just want to learn. Nobody’s going to buy that. Unless there’s a cultural shift that happens repeatedly with each incident… I don’t think there’ll be much buy-in from the clinical frontline”.Psychiatrist/homicide [31]
“I felt I had to be defensive”.Nurse/suicide [27]
“It confirmed my existing beliefs about the importance of accurate record keeping, including formalising leave cover. It was the hardest thing I have ever dealt with but taught me a lot early on”.Practitioner/suicide [27]
“It’s made me more assertive. When I know my patient needs something, I advocate. If I know they need some sort of support I’d really push for it”.Nurse/homicide [31]
6. Discussion
6.1. Main Findings of This Review
6.2. Wider Research
6.3. Blame
6.4. Not Knowing
6.5. Limited Learning
6.6. Strengths and Limitations of This Paper
6.7. Strengths and Limitations of the Included Literature
6.8. Areas for Future Research
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gregory, M.J. Managing the Homicide-Suicide Inquest the Practices of Coroners in One Region of England and Wales. Int. J. Law Crime Justice 2014, 42, 237–250. [Google Scholar] [CrossRef]
- Biddle, L. Public Hazards or Private Tragedies? An Exploratory Study of the Effect of Coroners’ Procedures on Those Bereaved by Suicide. Soc. Sci. Med. 2003, 56, 1033–1045. [Google Scholar] [CrossRef]
- Tamworth, M.; Killaspy, H.; Billings, J.; Gibbons, R. Psychiatrists’ Experience of a Peer Support Group for Reflecting on Patient Suicide and Homicide: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 14507. [Google Scholar] [CrossRef]
- Chapple, A.; Ziebland, S.; Hawton, K. A Proper, Fitting Explanation?: Suicide Bereavement and Perceptions of the Coroner’s Verdict. Crisis 2012, 33, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Freckelton, I. Minimising the Counter-Therapeutic Effects of Coronial Investigations: In Search of Balance. QUT Law Rev. 2016, 16, 4–29. [Google Scholar] [CrossRef]
- Spillane, A.; Matvienko-Sikar, K.; Larkin, C.; Corcoran, P.; Arensman, E. How Suicide-Bereaved Family Members Experience the Inquest Process: A Qualitative Study Using Thematic Analysis. Int. J. Qual. Stud. Health Well-Being 2019, 14, 1563430. [Google Scholar] [CrossRef] [PubMed]
- Freckelton, I. Death Investigation, the Coroner and Therapeutic Jurisprudence. J. Law Med. 2007, 15, 242–253. [Google Scholar]
- Doka, K.J. Living with Grief after Sudden Loss: Suicide, Homicide, Accident, Heart Attack, Stroke; Doka, K.J., Ed.; Taylor & Francis: Philadelphia, PA, USA, 1996. [Google Scholar]
- Pitman, A.L.; Osborn, D.P.; Rantell, K.; King, M.B. The Stigma Perceived by People Bereaved by Suicide and Other Sudden Deaths: A Cross-Sectional Uk Study of 3432 Bereaved Adults. J. Psychosom. Res. 2016, 87, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Pitman, A.L.; Stevenson, F.; Osborn, D.P.J.; King, M.B. The Stigma Associated with Bereavement by Suicide and Other Sudden Deaths: A Qualitative Interview Study. Soc. Sci. Med. 2018, 198, 121–129. [Google Scholar] [CrossRef]
- Seys, D.; Wu, A.W.; Van Gerven, E.; Vleugels, A.; Euwema, M.; Panella, M.; Scott, S.D.; Conway, J.; Sermeus, W.; Vanhaecht, K. Health Care Professionals as Second Victims after Adverse Events: A Systematic Review. Eval. Health Prof. 2013, 36, 135–162. [Google Scholar] [CrossRef]
- Chemtob, C.M.; Bauer, G.B.; Hamada, R.S.; Pelowski, S.R.; Muraoka, M.Y. Patient Suicide: Occupational Hazard for Psychologists and Psychiatrists. Prof. Psychol. Res. Pract. 1989, 20, 294–300. [Google Scholar] [CrossRef]
- Herbert, H.; Lipschitz, A.; Maltsberger, J.T.; Haas, A.P.; Wynecoop, S. Therapists’ Reactions to Patients’ Suicides. Am. J. Psychiatry 2000, 157, 2022–2027. [Google Scholar]
- House, A. Suicide and the Psychiatrist: Commentary on… Effects of Patient Suicide on Psychiatrists. BJPsych Bull. 2019, 43, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Gunn, S.; Robertson, N. The Impact of Patient Suicide on Doctors and Nurses: A Critical Interpretive Meta-Synthesis. Arch. Suicide Res. 2022, 26, 1266–1285. [Google Scholar] [CrossRef]
- Sandford, D.M.; Kirtley, O.J.; Thwaites, R.; O’Connor, R.C. The Impact on Mental Health Practitioners of the Death of a Patient by Suicide: A Systematic Review. Clin. Psychol. Psychother. 2020, 28, 261–294. [Google Scholar] [CrossRef]
- Wurst, F.M.; Kunz, I.; Skipper, G.; Wolfersdorf, M.; Beine, K.H.; Thon, N. The Therapist’s Reaction to a Patient’s Suicide: Results of a Survey and Implications for Health Care Professionals’ well-Being. Crisis 2011, 32, 99–105. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The Prisma Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Protogerou, C.; Hagger, M.S. A Case for a Study Quality Appraisal in Survey Studies in Psychology. Front. Psychol. 2018, 9, 2788. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Gagnon, M.-P.; Griffiths, F.; Johnson-Lafleur, J. A Scoring System for Appraising Mixed Methods Research, and Concomitantly Appraising Qualitative, Quantitative and Mixed Methods Primary Studies in Mixed Studies Reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M.; Cavers, D.; Agarwal, S.; Annandale, E.; Arthur, A.; Harvey, J.; Hsu, R.; Katbamna, S.; Olsen, R.; Smith, L.; et al. Conducting a Critical Interpretive Synthesis of the Literature on Access to Healthcare by Vulnerable Groups. BMC Med. Res. Methodol. 2006, 6, 35. [Google Scholar]
- Mays, N.; Pope, C. Synthesising Qualitative Research. In Qualitative Research in Health Care; Wiley: Hoboken, NJ, USA, 2020; pp. 151–168. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the Thematic Synthesis of Qualitative Research in Systematic Reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing Transparency in Reporting the Synthesis of Qualitative Research: Entreq. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Morse, J.M. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual. Health Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef]
- Croft, A.; Lascelles, K.; Brand, F.; Carbonnier, A.; Gibbons, R.; Wolfart, G.; Hawton, K. Effects of Patient Deaths by Suicide on Clinicians Working in Mental Health: A Survey. Int. J. Ment. Health Nurs. 2022, 32, 245–276. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.; Brand, F.; Carbonnier, A.; Croft, A.; Lascelles, K.; Wolfart, G.; Hawton, K. Effects of Patient Suicide on Psychiatrists: Survey of Experiences and Support Required. BJPsych Bull. 2019, 43, 236–241. [Google Scholar] [CrossRef]
- Alexander, D.A. Suicide by Patients: Questionnaire Study of Its Effect on Consultant Psychiatrists. BMJ 2000, 320, 1571–1574. [Google Scholar] [CrossRef] [PubMed]
- Mezey, G.; Rowe, R.; Adshead, G. Impact of Homicide by a Psychiatric Patient on Forensic Psychiatrists: National Survey. BJPsych Bull. 2021, 45, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Ng, L.; Merry, A.F.; Paterson, R.; Merry, S.N. Clinicians’ Experiences of Inquiries Following Mental Health Related Homicide: A Qualitative Study. Australas. Psychiatry 2021, 30, 185–189. [Google Scholar] [CrossRef]
- Hussain, Q.; Killaspy, H.; McPherson, P.; Gibbons, R. Experiences and Support Needs of Consultant Psychiatrists Following a Patient-Perpetrated Homicide. BJPsych Bull. 2023, 48, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R. Eight ‘Truths’ about Suicide. BJPsych Bull. 2023, 1–5. [Google Scholar] [CrossRef]
- Stolorow, R.D. A Phenomenological-Contextual, Existential, and Ethical Perspective on Emotional Trauma. Psychoanal. Rev. 2015, 102, 123–138. [Google Scholar] [CrossRef] [PubMed]
- Darden, A.J.; Rutter, P.A. Psychologists’ Experiences of Grief after Client Suicide: A Qualitative Study. OMEGA J. Death Dying 2011, 63, 317–342. [Google Scholar]
- Foley, S.R.; Kelly, B.D. When a Patient Dies by Suicide: Incidence, Implications and Coping Strategies. Adv. Psychiatr. Treat. 2007, 13, 134–138. [Google Scholar] [CrossRef]
- Campbell, D.; Hale, R. Working in the Dark: Understanding the Pre-Suicide State of Mind; Routledge: London, UK, 2017. [Google Scholar]
- Stanley, N.; Manthorpe, J. The Inquiry as Janus. In The Age of the Inquiry—Learning and Blaming in Health and Social Care; Routledge: London, UK, 2004; pp. 1–17. [Google Scholar]
- Committee, House of Commons Justice. “The Coroner Service.” London. 2021. Available online: https://committees.parliament.uk/publications/6079/documents/75085/default/ (accessed on 3 February 2024).
- Albudaiwi, D. Surveys, Advantages and Disadvantages of. In The SAGE Encyclopedia of Communication Research Methods; SAGE Publications: Thousand Oaks, CA, USA, 2017; pp. 1735–1736. [Google Scholar] [CrossRef]
- Garcia, J.; Evans, J.; Reshaw, M. Is There Anything Else You Would Like to Tell Us—Methodological Issues in the Use of Free-Text Comments from Postal Surveys. Qual. Quant. 2004, 38, 113–125. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author and Publication Year | Country | Topic | Study Design | N | Male (%) | Profession | Yrs Experience | # Events * |
|---|---|---|---|---|---|---|---|---|
| Croft, A. 2022 [27] | U.K. | Suicide | Cross sectional survey (including free text responses) | 134 | 19% | 53% psychologists and therapists; 33% nurses; 10.5% social workers; 7% support workers; 4% occupational therapists | >10 (68%) 7–10 (10.5%) 4–5 (14%) 1–3 (7%) | 1–5 (90%) 10+ (3%) |
| Gibbons, R. 2019 [28] | U.K. | Suicide | Cross sectional survey (including free text responses) | 140 | 52% | consultant psychiatrists | Not stated | 1+ (72%) 6+ (15%) 10+ (3%) |
| Alexander, D. A. 2000 [29] | U.K. | Suicide | Cross sectional survey (including free text responses) | 159 | 63% | consultant psychiatrists | 17.5 mean (SD 17.2) | 1 (23%) 2–6 (66%) 7–15 (13%) |
| Mezey, G. 2021 [30] | U.K. | Homicide | Cross sectional survey (including free text responses) + interviews | 26 | 74% | forensic psychiatrists | >15 (50%) 2–15 (42%) <2 (8%) | 1 (70%) 2 (16%) 3+ (12%) |
| Ng, L. 2021 [31] | New Zealand | Homicide | Semi-structured interviews | 10 | 70% | 40% psychiatrists; 40% nursing; 10% social workers; 10% community support workers | 2–30 (range) | 1 (100%) |
| Hussain, Q. 2023 [32] | U.K. | Homicide | Cross sectional survey (including free text responses) | 165 | 52% | consultant psychiatrists | 21 mean (SD 9) | 1 (60%) 2 (16%) Unspecified (39%) |
| Author (Year), Country | Research Objective | Key Findings |
|---|---|---|
| Croft, A. 2022 [27] | To investigate the experiences of mental health practitioners, excluding doctors, following death by suicide and their requirements for support in aftermath | (1) Most reported feeling unprepared for the formal processes that followed the death but felt more knowledgeable having been through it. Prospect of inquest could be frightening but could be mitigated by experiencing a fair and transparent process. (2) Many felt afraid of writing a report for coroner and did not know what to include. (3) Internal inquiry could be insensitively handled with overzealous investigators, inference of blame and poor delivery of feedback. Some did experience good guidance on formal processes and a well-conducted investigation. (4) 72% (82/114) received advice or support for the formal process (55% (63) from their organisation, the rest had informal forms of support). 46% (102) wanted more support for formal processes after a patient suicide. |
| Gibbons, R. 2019 [28] | To examine how patient suicide affects the emotional well-being and clinical practice of psychiatrists; and the resources that psychiatrists would find helpful before and after the suicide of a patient | (1) Experience of inquest described as ‘very traumatic’, and made some respondents feel upset, sad, angry and that they were being blamed. (2) 19% (15) of respondents commented that the serious incident process was insensitive and/or persecutory. 11% (9) cited coroner’s court as unhelpful with negative factors including the stress of giving evidence; delays; fear of attending and punitive attitude of coroner. (3) 70% (97) of survey respondents asked for support for formal processes following a patient’s suicide. (4) Respondents said the overall experience could be shaped by the attitude adopted by the Trust, the family of the deceased and the coroner. |
| Alexander, D. A. 2000 [29] | To identify the effect of patients’ suicide on consultant psychiatrists | (1) Fatal Accident Inquiry (n = 31) described as unhelpful or very unhelpful by 49%; disciplinary proceedings (n = 11) described as unhelpful or very unhelpful by 45%; legal proceedings (n = 17) described as unhelpful or very unhelpful by 82%. Conversely, the critical incident review (n = 83) described as helpful or very helpful by 78%. 21 of 159 consultants were moderately distressed at prospect of litigation and 12 were extremely distressed. (2) Open text comments suggested clinicians could feel scapegoated, blamed and part of a witch hunt. (3) Formal inquiries could create a climate of blame and impeded a constructive analysis of events. Suggestions for investigation handling: should be clinically led with legal consequences kept separate from critical incident analysis. |
| Mezey, G. 2021 [30] | To examine the impact on the treating forensic psychiatrist of a patient committing a homicide | (1) Inquiry and legal action ‘one of the most difficult aspects of the overall experience of patient suicide, described as frightening, confusing, punitive and humiliating. (2) Identified issues were length of inquiries, complexity, obscure rules of engagement, highly adversarial and lack of impartiality. These features were present in both internal and external inquiries. (3) No positive aspects of inquiry in terms of learning for clinicians; answers for victim families; righting wrongs or driving improvements. |
| Ng, L. 2021 [31] | To explore the experiences of clinicians involved with inquiries into the mental health care of patients who were perpetrators of homicide | (1) Inquiry process: most struggled with inquiry interview panel and pointed to disconnect between reality of clinical working and the panel perspective. (2) Varied experiences of dissemination of findings; all wanted more time to reflect on inquiry findings and recommendations. (3) Emotional burden of inquiry included shock at their patient having killed someone; stress at prospect of being sanctioned. (4) Found support through peers, lack of formal support. (5) Detrimental effect on team dynamics made worse by poor communication. (5) Perception of enquiry experience differed across employing Trusts. |
| Hussain, Q. 2023 [32] | To investigate the experiences and support needs of consultant psychiatrists from all disciplines following a homicide by a patient under their care | (1) 84% (101/121) were involved in an internal inquiry and 2% (4/165) in external disciplinary proceedings. No referrals to GMC. 31% (32/104) provided a report for court and 18% (19) gave evidence. (2) 14% (23/165) felt the formal processes were psychologically damaging, most commonly feeling they were blamed; 5% (9/165) found formal processes constructive and gained valuable experience. (3) 67% (40/60) received no support from their employing organisation and 50% (28/60) said they relied on friends and family. Those who did have support from their employer found it helpful. |
| Q1 | Q2 | 1.1 | 1.2 | 1.3 | 1.4 | 1.5 | 2.1 | 2.2 | 2.3 | 3.1 | 3.2 | 3.3 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Study Design | Rating | Screening | Qualitative | Quantitative | Mixed Methods | MMR Rating | |||||||||
| Croft, A. 2022 [27] | survey with free text section | 64% | Y | Y | Y | Y | Y | N | N | Y | N | Y | Y | Y | N | *** |
| Gibbons, R. 2019 [28] | survey with free text section | 57% | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | Y | N | *** |
| Alexander, D. A. 2000 [29] | survey with free text section | 64% | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | N | *** |
| Mezey, G. 2021 [30] | survey + follow up interview | 50% | Y | Y | Y | Y | N | N | N | Y | N | N | Y | Y | N | ** |
| Ng, L. 2021 [31] | semi-structured interview | 63% | Y | Y | Y | Y | N | Y | N | - | - | - | - | - | - | *** |
| Hussain, Q. 2023 [32] | survey with free text section | 64% | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | Y | N | *** |
| 1.0 Blame and enduring hostility | |
| 2.0 In the dark | 2.1 Not knowing |
| 2.2 An obscure and isolating process | |
| 3.0 Limited learning | 3.1 On the defensive |
| 3.2 Inconsistent dissemination of findings | |
| 3.3 Disconnected from reality |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamworth, M.; Tekin, S.; Billings, J.; Killaspy, H. What Are the Experiences of Mental Health Practitioners Involved in a Coroner’s Inquest and Other Inquiry Processes after an Unexpected Death of a Patient? A Systematic Review and Thematic Synthesis of the Literature. Int. J. Environ. Res. Public Health 2024, 21, 357. https://doi.org/10.3390/ijerph21030357
Tamworth M, Tekin S, Billings J, Killaspy H. What Are the Experiences of Mental Health Practitioners Involved in a Coroner’s Inquest and Other Inquiry Processes after an Unexpected Death of a Patient? A Systematic Review and Thematic Synthesis of the Literature. International Journal of Environmental Research and Public Health. 2024; 21(3):357. https://doi.org/10.3390/ijerph21030357
Chicago/Turabian StyleTamworth, Millie, Sahra Tekin, Jo Billings, and Helen Killaspy. 2024. "What Are the Experiences of Mental Health Practitioners Involved in a Coroner’s Inquest and Other Inquiry Processes after an Unexpected Death of a Patient? A Systematic Review and Thematic Synthesis of the Literature" International Journal of Environmental Research and Public Health 21, no. 3: 357. https://doi.org/10.3390/ijerph21030357
APA StyleTamworth, M., Tekin, S., Billings, J., & Killaspy, H. (2024). What Are the Experiences of Mental Health Practitioners Involved in a Coroner’s Inquest and Other Inquiry Processes after an Unexpected Death of a Patient? A Systematic Review and Thematic Synthesis of the Literature. International Journal of Environmental Research and Public Health, 21(3), 357. https://doi.org/10.3390/ijerph21030357