

Assessing the Quality and Coverage of Maternal Postnatal Care in Bangladesh: A Comparative Analysis of Quality Postnatal Care among Home and Facility Births

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
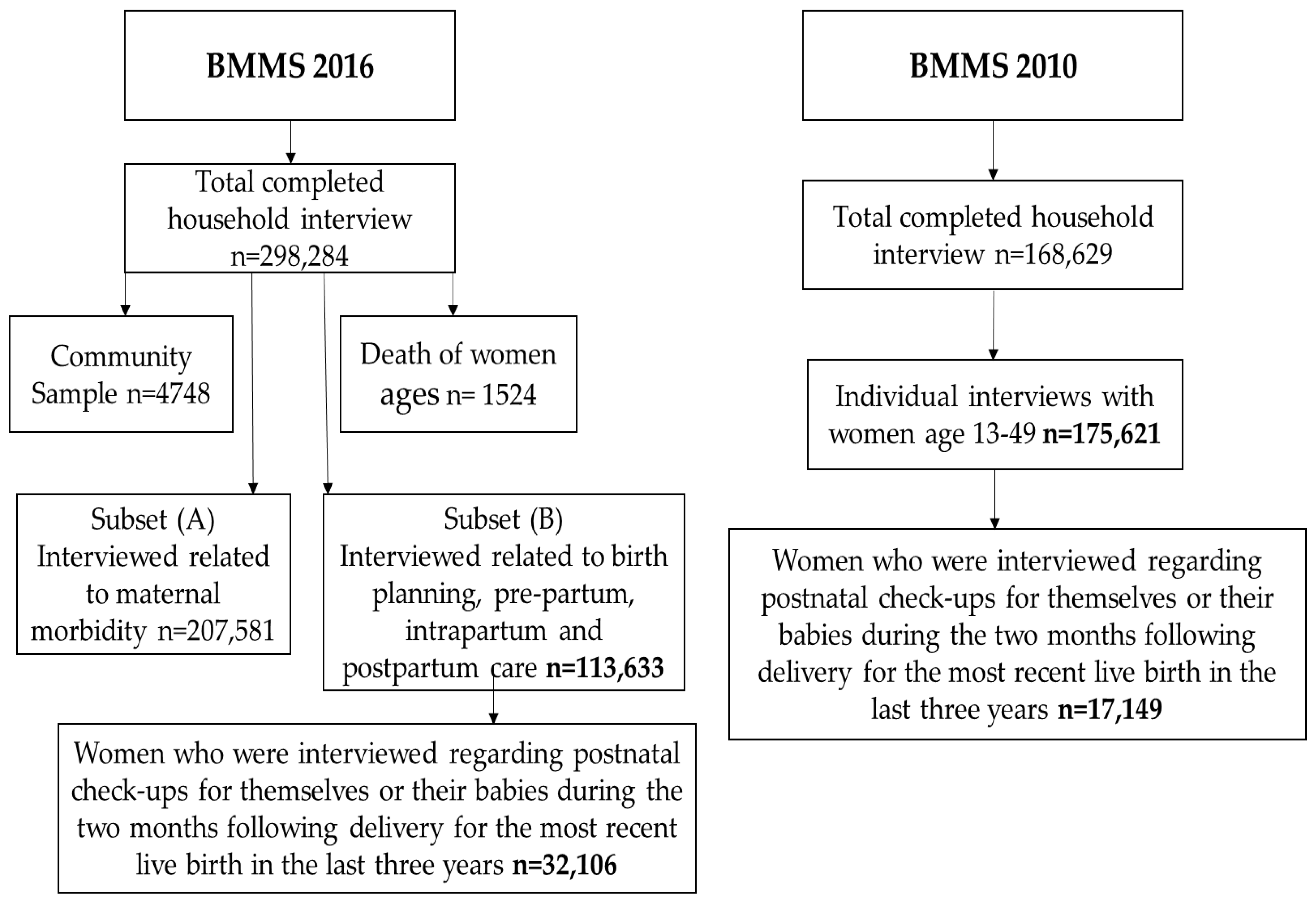
2.1. Study Data
2.2. Study Design and Settings
2.3. Outcome Variable
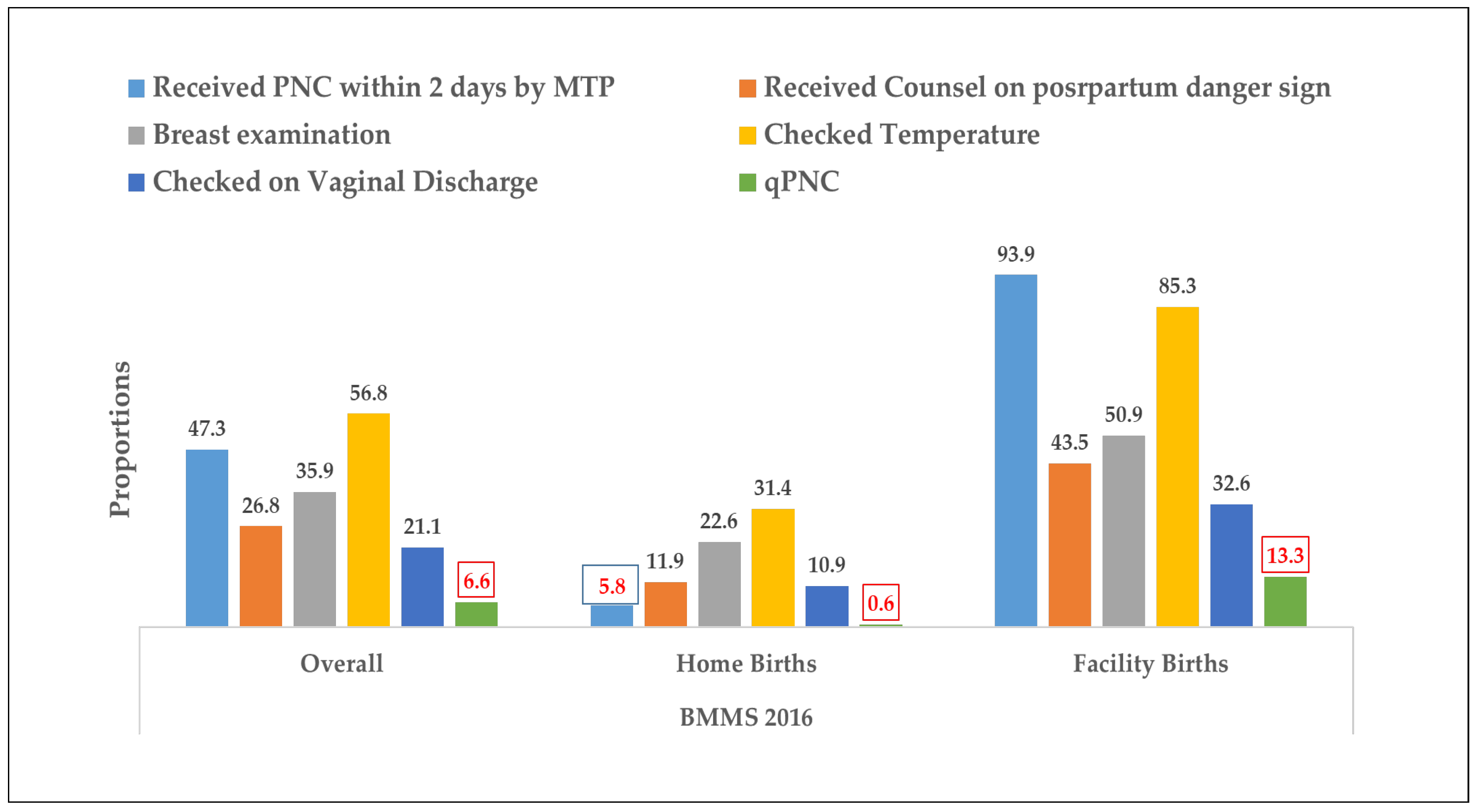
- At least one PNC within 48 h by a medically trained provider (MTP), who could be a doctor, nurse/midwife/paramedic/family welfare visitor (FWV), community skill birth attendant (CSBA), and sub assistant community medical officer (SACMO);
- Breast examination;
- Counseled on postpartum danger signs;
- Temperature check;
- Checked for vaginal discharge (to monitor excessive bleeding and foul-smelling discharge).
2.4. Key Independent Variables
2.4.1. Background Characteristics
2.4.2. Maternal Health Services
- ANC from MTP: no ANC, ANC from qualified (which includes doctors, Nurses/midwives/paramedics/FWV, CSBA, MA/SACMO), and unqualified providers
- Number of ANC: no ANC, 1–3 ANC, and 4 or more ANC;
- Place of delivery: home and facility births
- Type of birth attendant: skilled and unskilled (skilled providers include qualified doctors, nurses/midwives/paramedics/FWV, CSBA, and MA/SACMO);
- Mode of delivery: normal or c-section;
- Complications during pregnancy: yes or no;
- Complications during delivery: yes or no;
- Complications during the postnatal period: yes or no;
- Savings available for delivery care: yes or no;
- Mobile phone ownership: yes or no.
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Background Characteristics of Study Population
3.2. Components of PNC
3.3. Utilization and Factors Associated with qPNC in Bangladesh
3.4. Determinants of qPNC in Bangladesh
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Maternal Mortality. Fact Sheets 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed on 17 February 2020).
- WHO. Newborns: Reducing Mortality. Fact Sheets 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality (accessed on 17 February 2020).
- Darmstadt, G.L.; Choi, Y.; Arifeen, S.E.; Bari, S.; Rahman, S.M.; Mannan, I.; Seraji, H.R.; Winch, P.J.; Saha, S.K.; Ahmed, A.S.M.N.U.; et al. Evaluation of a cluster-randomized controlled trial of a package of community-based maternal and newborn interventions in Mirzapur, Bangladesh. PLoS ONE 2010, 5, e9696. [Google Scholar] [CrossRef] [PubMed]
- Martines, J.; Paul, V.K.; Bhutta, Z.A.; Koblinsky, M.; Soucat, A.; Walker, N.; Bahl, R.; Fogstad, H.; Costello, A. Neonatal survival: A call for action. Lancet 2005, 365, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Sines, E.; Syed, U.; Wall, S.; Worley, H. Postnatal care: A critical opportunity to save mothers and newborns. Policy Perspect. Newborn Health 2007, 1, 1–7. [Google Scholar]
- Maswime, S.; Buchmann, E. Causes and avoidable factors in maternal death due to cesarean-related hemorrhage in South Africa. Int. J. Gynecol. Obstet. 2016, 134, 320–323. [Google Scholar] [CrossRef]
- Barnett, S.; Nair, N.; Tripathy, P.; Borghi, J.; Rath, S.; Costello, A. A prospective key informant surveillance system to measure maternal mortality–findings from indigenous populations in Jharkhand and Orissa, India. BMC Pregnancy Childbirth 2008, 8, 6. [Google Scholar] [CrossRef] [PubMed]
- Carvajal–Aguirre, L.; Amouzou, A.; Mehra, V.; Ziqi, M.; Zaka, N.; Newby, H. Gap between contact and content in maternal and newborn care: An analysis of data from 20 countries in sub–Saharan Africa. J. Glob. Health 2017, 7, 020501. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Bahl, R.; Lawn, J.E.; Salam, R.A.; Paul, V.K.; Sankar, M.J.; Blencowe, H.; Rizvi, A.; Chou, V.B.; et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 2014, 384, 347–370. [Google Scholar] [CrossRef]
- WHO. WHO Recommendations on Postnatal Care of the Mother and Newborn; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. Standards for Improving Quality of Maternal and Newborn Care in Health Facilities; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- National Institute of Population Research and Training (NIPORT). Bangladesh Maternal Mortality and Health Care Survey 2010. Dhaka, Bangladesh: NIPORT, MEASURE Evaluation, and icddr,b., Bangladesh Maternal Mortality and Health Care Survey 2010. 2012. Available online: https://www.measureevaluation.org/resources/publications/tr-12-87.html (accessed on 10 December 2023).
- National Institute of Population Research and Training (NIPORT). Bangladesh Maternal Mortality and Health Care Survey 2016: Final Report. Dhaka, Bangladesh, and Chapel Hill, NC, USA: NIPORT, icddr,b, and MEASURE Evaluation., Bangladesh Maternal Mortality and Health Care Survey (BMMS) 2016: Final Report. 2019. Available online: https://www.measureevaluation.org/resources/publications/tr-18-297.html (accessed on 10 December 2023).
- National Institute of Population Research and Training, Bangladesh Maternal Mortality and Health Care Survey BMMS, in Preliminary Report. 2016. Available online: https://www.measureevaluation.org/resources/publications/tr-17-218.html (accessed on 10 December 2023).
- National Institute of Population Research and Training (NIPORT) and ICF, Bangladesh Demographic and Health Survey, in Key Indicators. 2017–18. 2019: Dhaka, Bangladesh, and Rockville, Maryland, USA. Available online: http://archive.dgfp.gov.bd//handle/123456789/180 (accessed on 10 December 2023).
- Ministry of Health & Family Welfare of Government of the People’s Republic of Bangladesh, Maternal Health Standard Operating Procedures (SOP). Vol. 1. 2019. Available online: http://hospitaldghs.gov.bd/wp-content/uploads/2023/05/MNH-Service-Accreditation-Manual_Clean_Cor-14-4-23.pdf (accessed on 10 December 2023).
- Ministry of Health and Family Welfare. National Strategy for Maternal Health 2015–2030. 2015, Ministry of Health and Family Welfare Bangladesh. Available online: http://archive.dgfp.gov.bd//handle/123456789/268 (accessed on 10 December 2023).
- Baqui, A.H.; Ahmed, S.; El Arifeen, S.; Darmstadt, G.L.; Rosecrans, A.M.; Mannan, I.; Rahman, S.M.; Begum, N.; Mahmud, A.B.A.; Seraji, H.R.; et al. Effect of timing of first postnatal care home visit on neonatal mortality in Bangladesh: A observational cohort study. BMJ 2009, 339, b2826. [Google Scholar] [CrossRef]
- Chou, V.B.; Walker, N.; Kanyangarara, M. Estimating the global impact of poor quality of care on maternal and neonatal outcomes in 81 low-and middle-income countries: A modeling study. PLoS Med. 2019, 16, e1002990. [Google Scholar] [CrossRef]
- Billah, S.M.; Chowdhury, M.A.K.; Khan, A.N.S.; Karim, F.; Hassan, A.; Zaka, N.; El Arifeen, S.; Manu, A. Quality of care during childbirth at public health facilities in Bangladesh: A cross-sectional study using WHO/UNICEF ‘Every Mother Every Newborn (EMEN)’standards. BMJ Open Qual. 2019, 8, e000596. [Google Scholar] [CrossRef]
- Chakraborty, N.; Islam, M.A.; Chowdhury, R.I.; Bari, W. Utilisation of postnatal care in Bangladesh: Evidence from a longitudinal study. Health Soc. Care Community 2002, 10, 492–502. [Google Scholar] [CrossRef]
- Syed, U.; Asiruddin, S.; Helal, S.; Mannan, I.I.; Murray, J. Immediate and early postnatal care for mothers and newborns in rural Bangladesh. J. Health Popul. Nutr. 2006, 24, 508. [Google Scholar]
- Rahman, M.; Haque, S.E.; Zahan, S. Factors affecting the utilisation of postpartum care among young mothers in Bangladesh. Health Soc. Care Community 2011, 19, 138–147. [Google Scholar] [PubMed]
- Halder, A.K.; Saha, U.; Kabir, M. Inequalities in reproductive healthcare utilization: Evidence from Bangladesh Demographic and Health Survey 2004. World Health Popul. 2007, 9, 48–63. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience; WHO: Geneve, Switzerland, 2018. [Google Scholar]
- Okawa, S.; Win, H.H.; Leslie, H.H.; Nanishi, K.; Shibanuma, A.; Aye, P.P.; Jimba, M. Quality gap in maternal and newborn healthcare: A cross-sectional study in Myanmar. BMJ Glob. Health 2019, 4, e001078. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Tarafder, T.; Mostofa, G. Modes of delivery assistance in Bangladesh. Tanzan. J. Health Res. 2008, 10, 246–252. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mohan, D.; Gupta, S.; LeFevre, A.; Bazant, E.; Killewo, J.; Baqui, A.H. Determinants of postnatal care use at health facilities in rural Tanzania: Multilevel analysis of a household survey. BMC Pregnancy Childbirth 2015, 15, 282. [Google Scholar] [CrossRef] [PubMed]
- Fosu, G.B. Childhood morbidity and health services utilization: Cross-national comparisons of user-related factors from DHS data. Soc. Sci. Med. 1994, 38, 1209–1220. [Google Scholar] [CrossRef]
- Kikuchi, K.; Ansah, E.K.; Okawa, S.; Enuameh, Y.; Yasuoka, J.; Nanishi, K.; Shibanuma, A.; Gyapong, M.; Owusu-Agyei, S.; Oduro, A.R.; et al. Effective linkages of continuum of care for improving neonatal, perinatal, and maternal mortality: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0139288. [Google Scholar] [CrossRef]
- Joshi, C.; Torvaldsen, S.; Hodgson, R.; Hayen, A. Factors associated with the use and quality of antenatal care in Nepal: A population-based study using the demographic and health survey data. BMC Pregnancy Childbirth 2014, 14, 94. [Google Scholar] [CrossRef] [PubMed]
- Ononokpono, D.N.; Odimegwu, C.O.; Imasiku, E.N.S.; Adedini, S.A. Does it really matter where women live? A multilevel analysis of the determinants of postnatal care in Nigeria. Matern. Child Health J. 2014, 18, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Hong, R. Levels and determinants of continuum of care for maternal and newborn health in Cambodia-evidence from a population-based survey. BMC Pregnancy Childbirth 2015, 15, 62. [Google Scholar] [CrossRef]
- Lahariya, C. Cash incentives for institutional delivery: Linking with antenatal and post natal care may ensure ‘continuum of care’in India. Indian J. Community Med. 2009, 34, 15. [Google Scholar] [CrossRef]
- Yunus, A.; Iqbal, S.; Munawar, R.; Zakar, R.; Mushtaq, S.K.; Sadaf, F.; Usman, A. Determinants of postnatal care services utilization in Pakistan-insights from Pakistan demographic and health survey (PDHS) 2006–2007. Middle-East J. Sci. Res. 2013, 18, 1440–1447. [Google Scholar]
- Chungu, C.; Makasa, M.; Chola, M.; Jacobs, C.N. Place of delivery associated with postnatal care utilization among childbearing women in Zambia. Front. Public Health 2018, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- Dhaher, E.; Mikolajczyk, R.T.; Maxwell, A.E.; Krämer, A. Factors associated with lack of postnatal care among Palestinian women: A cross-sectional study of three clinics in the West Bank. BMC Pregnancy Childbirth 2008, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Borders, N. After the afterbirth: A critical review of postpartum health relative to method of delivery. J. Midwifery Women’s Health 2006, 51, 242–248. [Google Scholar] [CrossRef]
- Campbell, O.M.R.; Cegolon, L.; Macleod, D.; Benova, L. Length of stay after childbirth in 92 countries and associated factors in 30 low-and middle-income countries: Compilation of reported data and a cross-sectional analysis from nationally representative surveys. PLoS Med. 2016, 13, e1001972. [Google Scholar] [CrossRef]
- Ndugga, P.; Namiyonga, N.K.; Sebuwufu, D. Determinants of early postnatal care attendance: Analysis of the 2016 Uganda demographic and health survey. BMC Pregnancy Childbirth 2020, 20, 163. [Google Scholar] [CrossRef]
- Titaley, C.R.; Dibley, M.J.; Roberts, C.L. Utilization of village midwives and other trained delivery attendants for home deliveries in Indonesia: Results of Indonesia Demographic and Health Survey 2002/2003 and 2007. Matern. Child Health J. 2011, 15, 1400–1415. [Google Scholar] [CrossRef] [PubMed]
- Ith, P.; Dawson, A.; Homer, C.S.; Whelan, A.K. Practices of skilled birth attendants during labour, birth and the immediate postpartum period in Cambodia. Midwifery 2013, 29, 300–307. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | n | % |
|---|---|---|
| Mother’s age at birth | ||
| <20 | 5094 | 15.9 |
| 20–34 | 24,894 | 77.5 |
| 35–49 | 2118 | 6.6 |
| Mobile phone | ||
| Yes | 29,239 | 91.1 |
| No | 2867 | 8.9 |
| Mother’s education | ||
| No education | 3145 | 9.8 |
| Primary | 9487 | 29.6 |
| Secondary+ | 19,474 | 60.7 |
| Religion | ||
| Muslim | 29,517 | 91.9 |
| Others | 2589 | 8.1 |
| Wealth index | ||
| Poor | 13,344 | 41.6 |
| Middle class | 6287 | 19.6 |
| Rich | 12,475 | 38.9 |
| Birth Order | ||
| 1 | 13,358 | 41.6 |
| 2 | 11,067 | 34.5 |
| 3+ | 7681 | 23.9 |
| Number of ANC | ||
| No ANC | 5602 | 17.5 |
| 1–3 | 14,292 | 44.5 |
| 4+ | 12,212 | 38.0 |
| ANC from MTP | ||
| No ANC | 5608 | 17.5 |
| Qualified Provider | 23,581 | 73.5 |
| Unqualified Provider | 2917 | 9.1 |
| Type of facility of delivery | ||
| Private facility | 10,341 | 67.7 |
| Public facility | 4936 | 32.3 |
| Type of birth attendant | ||
| Skilled | 16,176 | 50.4 |
| Unskilled | 15,930 | 49.6 |
| Complications during pregnancy | ||
| Yes | 20,379 | 63.5 |
| No | 11,727 | 36.5 |
| Complications during delivery | ||
| Yes | 24,179 | 75.3 |
| No | 7927 | 24.7 |
| Complications during Postnatal Period | ||
| Yes | 25,684 | 80.0 |
| No | 6422 | 20.0 |
| Savings available for delivery care | ||
| Yes | 14,894 | 46.4 |
| No | 17,212 | 53.6 |
| 2010 | 2016 | |||||
|---|---|---|---|---|---|---|
| Indicators | Home Births | Facility Births | Total | Home Births | Facility Births | Total |
| % | ||||||
| Received postnatal visit within 42 days | - | - | 41.0 | 44.6 | 95.9 | 69.0 |
| Received postnatal visit within 48 h | 16.6 | 80.1 | 32.0 | 39.7 | 94.9 | 66.0 |
| Postnatal visit by a qualified provider within 2 days | 4.6 | 78.8 | 23.0 | 5.8 | 93.9 | 47.0 |
| qPNC | - | - | 0.6 | 13.3 | 6.6 | |
| Covariates | qPNC among Facility Births (n = 15,277) | qPNC among Home Births (n = 16,829) | ||||
|---|---|---|---|---|---|---|
| n | % | p-Value | n | % | p-Value | |
| Mother’s age at birth | ||||||
| <20 | 270 | 11.2 | 0.002 | 13 | 0.5 | 0.259 |
| 20–34 | 1652 | 13.8 | 81 | 0.6 | ||
| 35–49 | 133 | 14.1 | 11 | 0.9 | ||
| Mobile phone | 0.847 | 0.320 | ||||
| Yes | 1883 | 13.4 | 92 | 0.6 | ||
| No | 172 | 13.6 | 13 | 0.8 | ||
| Mother’s education | ||||||
| No education | 87 | 11.2 | <0.001 | 9 | 0.4 | 0.017 |
| Primary | 341 | 11.3 | 32 | 0.5 | ||
| secondary+ | 1627 | 14.2 | 64 | 0.8 | ||
| Religion | 0.809 | 0.252 | ||||
| Muslim | 1838 | 13.4 | 96 | 0.6 | ||
| Others | 217 | 13.6 | 9 | 0.9 | ||
| Wealth index | ||||||
| Poor | 480 | 12.3 | <0.001 | 32 | 0.3 | <0.001 |
| Middle class | 351 | 11.8 | 21 | 0.6 | ||
| Rich | 1224 | 14.6 | 52 | 1.3 | ||
| Birth Order | ||||||
| 1 | 1041 | 13.6 | 0.345 | 40 | 0.7 | 0.640 |
| 2 | 709 | 13.7 | 35 | 0.6 | ||
| 3+ | 305 | 12.5 | 30 | 0.6 | ||
| Number of ANC | ||||||
| No ANC | 77 | 10.6 | <0.001 | 12 | 0.2 | <0.001 |
| 1–3 | 762 | 11.9 | 50 | 0.6 | ||
| 4+ | 1216 | 15 | 43 | 1.1 | ||
| ANC from MTP | ||||||
| No ANC | 75 | 10.3 | 0.001 | 12 | 0.2 | <0.001 |
| Qualified Provider | 1913 | 13.8 | 86 | 0.9 | ||
| Unqualified Provider | 67 | 10 | 7 | 0.3 | ||
| Type of facility of delivery | ||||||
| Private facility | 1495 | 14.5 | <0.001 | |||
| Public facility | 560 | 11.3 | ||||
| Type of birth attendant | ||||||
| Skilled | 2053 | 13.6 | <0.001 | 67 | 6.3 | <0.001 |
| Unskilled | 2 | 1.2 | 38 | 0.2 | ||
| Complications during pregnancy | ||||||
| Yes | 1104 | 12.7 | 0.003 | 62 | 0.5 | 0.019 |
| No | 951 | 14.4 | 43 | 0.8 | ||
| Complications during delivery | ||||||
| Yes | 1357 | 12.7 | <0.001 | 65 | 0.5 | <0.001 |
| No | 698 | 15.3 | 40 | 1.2 | ||
| Complications during Postnatal Period | ||||||
| Yes | 1520 | 12.8 | <0.001 | 63 | 0.5 | <0.001 |
| No | 535 | 15.5 | 42 | 1.4 | ||
| Savings available for delivery care | ||||||
| Yes | 635 | 11.4 | <0.001 | 43 | 0.5 | 0.003 |
| No | 1420 | 14.6 | 62 | 0.8 | ||
| Covariates | qPNC among Home Births | qPNC among Facility Births | ||||||
|---|---|---|---|---|---|---|---|---|
| uRR (95% CI) | aRR (95% CI) | uRR (95% CI) | aRR (95% CI) | |||||
| Mother’s age at birth | ||||||||
| <20 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 20–34 | 1.29 (0.72–2.32) | 1.22 (0.69–2.18) | 1.23 (1.09–1.39) | ** | 1.17 (1.04–1.32) | * | ||
| 35–49 | 1.93 (0.87–4.31) | 2.02 (0.9–4.54) | 1.25 (1.04–1.53) | * | 1.19 (0.98–1.44) | |||
| Mother’s education | ||||||||
| No education | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Primary | 1.30 (0.62–2.72) | 1.19 (0.58–2.45) | 1.01 (0.81–1.26) | 0.98 (0.79–1.23) | ||||
| secondary+ | 2.11 (1.05–4.24) | * | 0.98 (0.48–2) | 1.26 (1.03–1.54) | * | 1.08 (0.88–1.33) | ||
| Wealth index | ||||||||
| Poor | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Middle | 1.86 (1.08–3.23) | * | 1.34 (0.77–2.33) | 0.96 (0.85–1.1) | 0.88 (0.77–1.00) | |||
| Rich | 3.77 (2.43–5.85) | *** | 1.95 (1.22–3.11) | ** | 1.18 (1.07–1.31) | ** | 0.97 (0.87–1.08) | |
| Number of ANC | ||||||||
| No ANC | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 1–3 | 2.58 (1.38–4.84) | ** | 0.59 (0–1.33) | 1.12 (0.9–1.4) | 0.4 (0.15–1.04) | |||
| 4+ | 4.27 (2.25–8.08) | *** | 0.74 (0–1.68) | 1.42 (1.14–1.76) | ** | 0.47 (0.18–1.22) | ||
| ANC from MTP | ||||||||
| No ANC | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Qualified Provider | 3.6 (1.97–6.58) | *** | 2.32 (0–5.23) | 1.34 (1.08–1.67) | ** | 2.51 (0.95–6.65) | ||
| Unqualified Provider | 1.27 (0.50–3.22) | 1.77 (0–4.03) | 0.97 (0.71–1.32) | 2.22 (0.82–6.01) | ||||
| Type of facility of delivery | ||||||||
| Private facility | - | - | 1.00 | 1.00 | ||||
| Public facility | - | - | 0.78 (0.72–0.86) | *** | 0.98 (0.89–1.08) | |||
| Type of birth attendant | ||||||||
| Unskilled | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Skilled | 25.92 (17.49–38.40) | *** | 19.8 (13.04–30.05) | *** | 11.76 (2.96–46.66) | *** | 7.9 (1.98–31.41) | ** |
| Mode of delivery | ||||||||
| Normal | - | - | 1.00 | 1.00 | ||||
| C-section | - | - | 1.72 (1.56–1.89) | *** | 1.58 (1.42–1.76) | *** | ||
| Complications during delivery | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Yes | 2.46 (1.66–3.63) | *** | 1.39 (0.9–2.16) | 1.21 (1.11–1.32) | *** | 1.21 (1.1–1.33) | *** | |
| Complications during postnatal period | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Yes | 3.11 (2.11–4.58) | *** | 2.48 (1.6–3.84) | *** | 1.21 (1.1–1.32) | *** | 1.08 (0.98–1.19) | |
| Savings available for delivery care | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Yes | 1.8 (1.22–2.66) | ** | 1.29 (0.87–1.9) | 1.27 (1.17–1.39) | *** | 1.20 (1.1–1.31) | *** | |
| Mobile Phone | ||||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||
| Yes | 0.75 (0.42–1.33) | 0.83 (0.47–1.47) | 0.99 (0.85–1.14) | *** | 1.00 (0.87–1.16) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priyanka, S.S.; Dasgupta, D.P.; Abdullah, A.Y.M.; Ali, N.B.; Khatun, H.; Billah, S.M. Assessing the Quality and Coverage of Maternal Postnatal Care in Bangladesh: A Comparative Analysis of Quality Postnatal Care among Home and Facility Births. Int. J. Environ. Res. Public Health 2024, 21, 359. https://doi.org/10.3390/ijerph21030359
Priyanka SS, Dasgupta DP, Abdullah AYM, Ali NB, Khatun H, Billah SM. Assessing the Quality and Coverage of Maternal Postnatal Care in Bangladesh: A Comparative Analysis of Quality Postnatal Care among Home and Facility Births. International Journal of Environmental Research and Public Health. 2024; 21(3):359. https://doi.org/10.3390/ijerph21030359
Chicago/Turabian StylePriyanka, Sabrina Sharmin, Dibbya Pravas Dasgupta, Abu Yousuf Md Abdullah, Nazia Binte Ali, Hafeza Khatun, and Sk Masum Billah. 2024. "Assessing the Quality and Coverage of Maternal Postnatal Care in Bangladesh: A Comparative Analysis of Quality Postnatal Care among Home and Facility Births" International Journal of Environmental Research and Public Health 21, no. 3: 359. https://doi.org/10.3390/ijerph21030359
APA StylePriyanka, S. S., Dasgupta, D. P., Abdullah, A. Y. M., Ali, N. B., Khatun, H., & Billah, S. M. (2024). Assessing the Quality and Coverage of Maternal Postnatal Care in Bangladesh: A Comparative Analysis of Quality Postnatal Care among Home and Facility Births. International Journal of Environmental Research and Public Health, 21(3), 359. https://doi.org/10.3390/ijerph21030359