1. Introduction
During the morning rush-hour of 20 March 1995, terrorists released the nerve agent sarin within 5 separate commuter-trains on the Tokyo subway system, exposing 15 stations to the toxic chemical in the minutes that followed [
1]. The attack resulted in 12 fatalities and approximately 5,500 people became ill. Nine months prior to the Tokyo attack the organisation responsible, Aum Shinrikyo, had also attacked a central area of Matsumoto city, Japan, by releasing sarin gas from an over-ground truck [
2]. Approximately 600 people were affected by the noxious cloud, including seven who died. Prior to the Japanese sarin attacks chemical agents were more generally considered as military weapons that had been deployed in a number of twentieth century wars. However, the events of 9/11, 7/7 and other terrorist attacks of the early twenty-first century brought sharply into focus that Western cities might experience other chemical attacks and that further planning for such incidents was a public health priority. Indeed, the threat of exposure to chemical agents is not limited to a deliberate release scenario. On 10 July 1976, there was an accidental chemical release from a manufacturing plant near the town of Seveso, Italy. People who happened to be in the path of the cloud developed headaches and eye-irritation, and a few children were admitted to local hospitals with lesions on exposed skin [
3,
4]. Eight years later a large gas leak from a pesticide plant in Bhopal, India killed at least 3,800 local people in the hours that followed [
5]. More than half a million people were exposed to the toxic chemicals; approximately 120,000 of them continue to suffer from a variety of chronic disorders [
6]. It is clear from the differing magnitudes of these various incidents that public health authorities need to be prepared to mitigate both small and large-scale chemical releases.
In the event of either a deliberate or accidental chemical release contaminated individuals would require rapid decontamination to reduce their probability of illness or death. To prepare for such an incident the emergency services perform field exercises using volunteer “casualty” actors. While these exercises can be extremely useful for testing responses and can help to identify important lessons for the future [
7] they are highly resource intensive to stage. One partial solution to this problem is the use of computer simulation via operational research techniques. Indeed, large-scale exercises in the US have been complemented by mathematical models of antibiotic distribution centres [
8] and mass vaccination clinics [
9] with the aim of optimising staffing levels. In the UK computer simulations of mass decontamination systems have recently been performed by Albores and Shaw [
10], who took a holistic approach that aimed to investigate resource requirements (vehicles, equipment and staff) necessary to decontaminate
x casualties in
y hours. Their model was informed by a number of interviews with key stakeholders who were knowledgeable of the mass decontamination process and/or had exercise experience. In order to build on their study we collected casualty movement data during two field exercises and subsequently modelled some more fundamental aspects of the mass decontamination process, both of which had not been explicitly addressed in earlier work.
2. Background
In the UK mass decontamination of the “walking wounded” (termed
ambulant casualties) would be undertaken by the Fire and Rescue Service (FRS) on behalf of the Ambulance Service as a result of the New Dimension programme [
11]. Ambulant casualties would be required to move away from the area of highest contamination (termed
Hot Zone) to an area ideally up-wind of the incident scene (termed
Warm Zone). If deemed necessary ambulant casualties may undergo either emergency decontamination or interim mass decontamination. The former process involves simply the application of water to ambulant casualties via, for example, building sprinklers or FRS hoses. The latter process is more structured and involves ambulant casualties walking through a makeshift shower utilising FRS hoses suspended from ladders fitted between parallel fire engines. Ambulant casualties would then be directed to a “casualty collection point” from where the FRS would subsequently conduct mass decontamination procedures (as described further below).
Those individuals who are unable to walk (termed
non-ambulant casualties), either because they are symptomatic, seriously injured in any initial explosion/accident or through a pre-existing disability, would be triaged by the Hazardous Area Response Team (HART) of the Ambulance Service [
12]. Non-ambulant casualties would then be conveyed out of the Hot Zone by the FRS and individually decontaminated in the Warm Zone by the Specialist Operational Response Team (SORT) of the Ambulance Service (note that HART does not apply in Scotland with SORT performing both roles). If the release was considered to have been deliberate then the Police Service would seek to maintain an “inner cordon” around the Hot and Warm Zones, in an attempt to apprehend the perpetrators and collect crime-scene evidence. Having passed through the decontamination process all casualties would then move to a “casualty clearing station” located in an area outside of the inner cordon (termed
Cold Zone) where they would be re-triaged for further hospital treatment if required. Depending on the circumstances of the chemical release and the health status of the casualties, the Police Service may perform brief information gathering interviews at this stage.
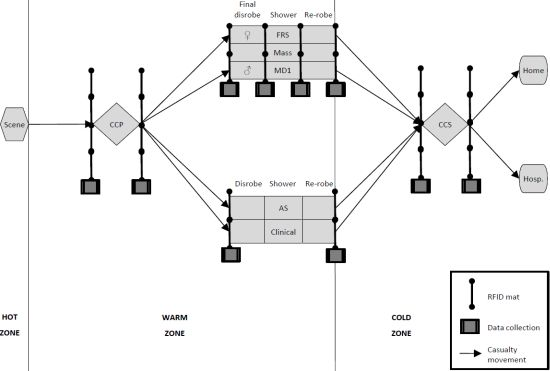
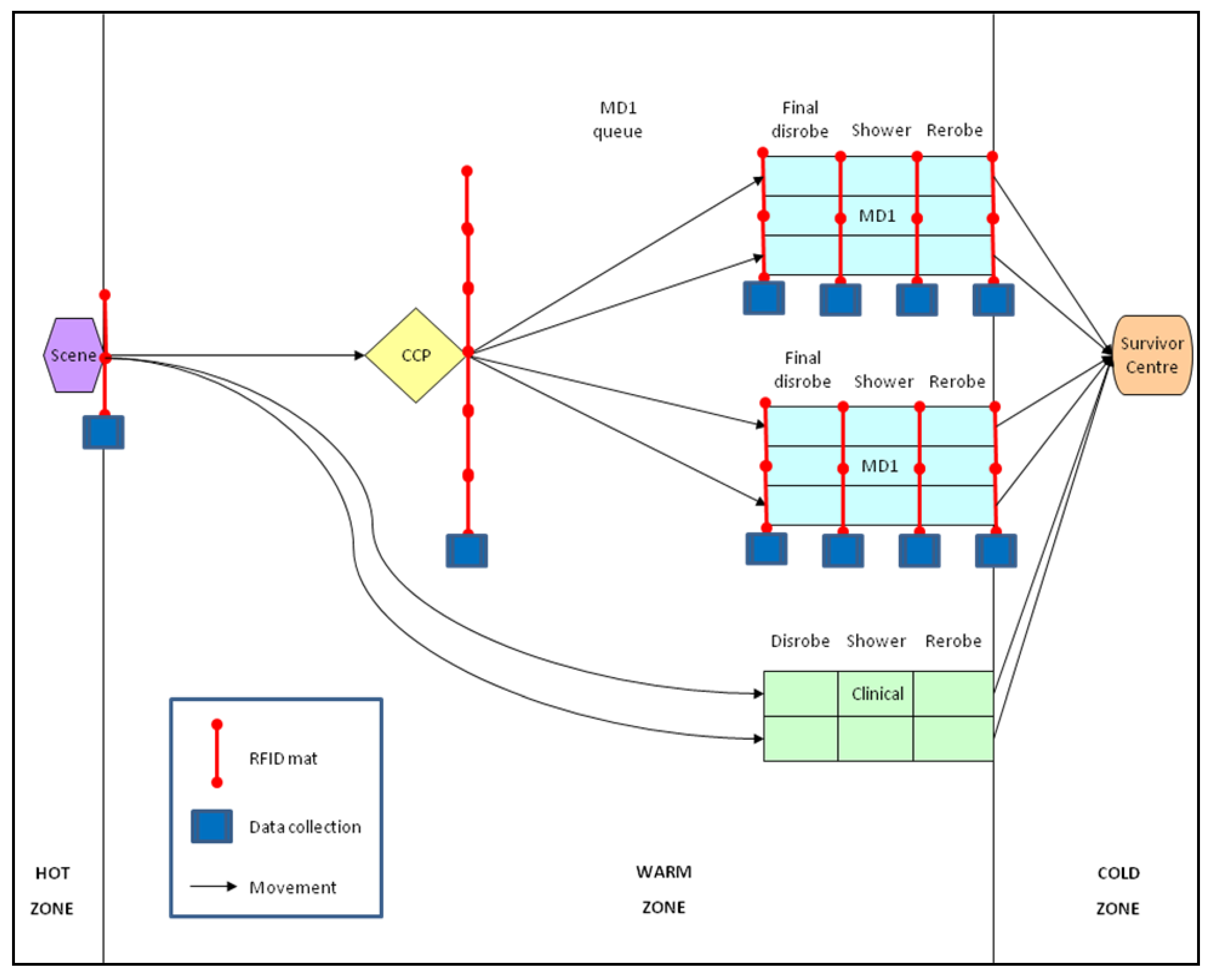
Figure 1 provides a schematic of the casualty movement through an idealised mass decontamination response.
In recent years mass decontamination procedures have developed as a result of training and operational experience, and have also been informed by the work of Albores and Shaw [
10]. In their study ambulant casualties are expected to remove their clothes in the disrobe section of the FRS mass decontamination unit (termed MD1—see
Figure 1) before showering in the middle section and then drying and dressing with fresh clothes in the re-robe section. Although groups of five males and five females are still required to enter two separate lanes of the MD1, the original batch disrobing has been replaced by an initial mass disrobe at the casualty collection point (
i.e., outside of the MD1). Thus, ambulant casualties are now required to remove their potentially contaminated clothing and are provided with temporary clothing from a disrobe pack to maintain warmth and preserve their modesty whilst awaiting MD1 construction. The original disrobe section of the MD1 is now used as a final disrobe section where ambulant casualties remove their disrobe clothing prior to entering the shower section.
The other major change is the introduction of an automated flow control system to the MD1. Lights are located at the entrance to the final disrobe, shower and re-robe sections as well as the exit of the re-robe section.
Figure 1.
Schematic of casualty movement through an idealised mass decontamination response. The Police Service inner cordon runs around the Hot and Warm Zones. Emergency decontamination/interim mass decontamination for ambulant casualties may take place between the Scene and the casualty collection point (CCP). Ambulant casualties progress to the Fire and Rescue Service (FRS) mass decontamination unit (termed MD1) in groups of five males and five females; FRS personnel patrol the middle lane removing disrobe clothing and providing re-robe packs. Non-ambulant casualties progress to the Ambulance Service (AS) clinical decontamination unit; two lanes are available to decontaminate individual casualties. The middle lane of the MD1 can also support clinical decontamination should it be needed but only when specifically configured and not simultaneously with mass decontamination. All casualties finally enter the casualty collection station (CCS) and are assessed for hospital (Hosp.) treatment or otherwise (Home). Radio Frequency Identification (RFID) detection mats were placed at shown locations in Exercise 1. The lights of the MD1 flow control system are located above the four RFID detection mats positioned at the MD1.
Figure 1.
Schematic of casualty movement through an idealised mass decontamination response. The Police Service inner cordon runs around the Hot and Warm Zones. Emergency decontamination/interim mass decontamination for ambulant casualties may take place between the Scene and the casualty collection point (CCP). Ambulant casualties progress to the Fire and Rescue Service (FRS) mass decontamination unit (termed MD1) in groups of five males and five females; FRS personnel patrol the middle lane removing disrobe clothing and providing re-robe packs. Non-ambulant casualties progress to the Ambulance Service (AS) clinical decontamination unit; two lanes are available to decontaminate individual casualties. The middle lane of the MD1 can also support clinical decontamination should it be needed but only when specifically configured and not simultaneously with mass decontamination. All casualties finally enter the casualty collection station (CCS) and are assessed for hospital (Hosp.) treatment or otherwise (Home). Radio Frequency Identification (RFID) detection mats were placed at shown locations in Exercise 1. The lights of the MD1 flow control system are located above the four RFID detection mats positioned at the MD1.
![Ijerph 09 03685 g001]()
For three minutes a red “Wait” pictogram is illuminated during which time the boiler provides two minutes of soapy water for washing in the shower section followed by one minute of water for rinsing. The lights then switch to illuminate a green “Enter” pictogram for fifteen seconds allowing casualties to move through to the next section (or enter/leave the MD1). An audible prompt also accompanies this stage following which the green “Enter” pictogram then flashes for a further five seconds to indicate that the cycle is about to revert back to the red “Wait” pictogram. Having entered the MD1 the ideal situation is for two groups of five (fe)male ambulant casualties to pass through the entire structure in 10 minutes, having spent three minutes in each section with 20 second transitions between each section and exiting the MD1.
3. Field Exercise Data
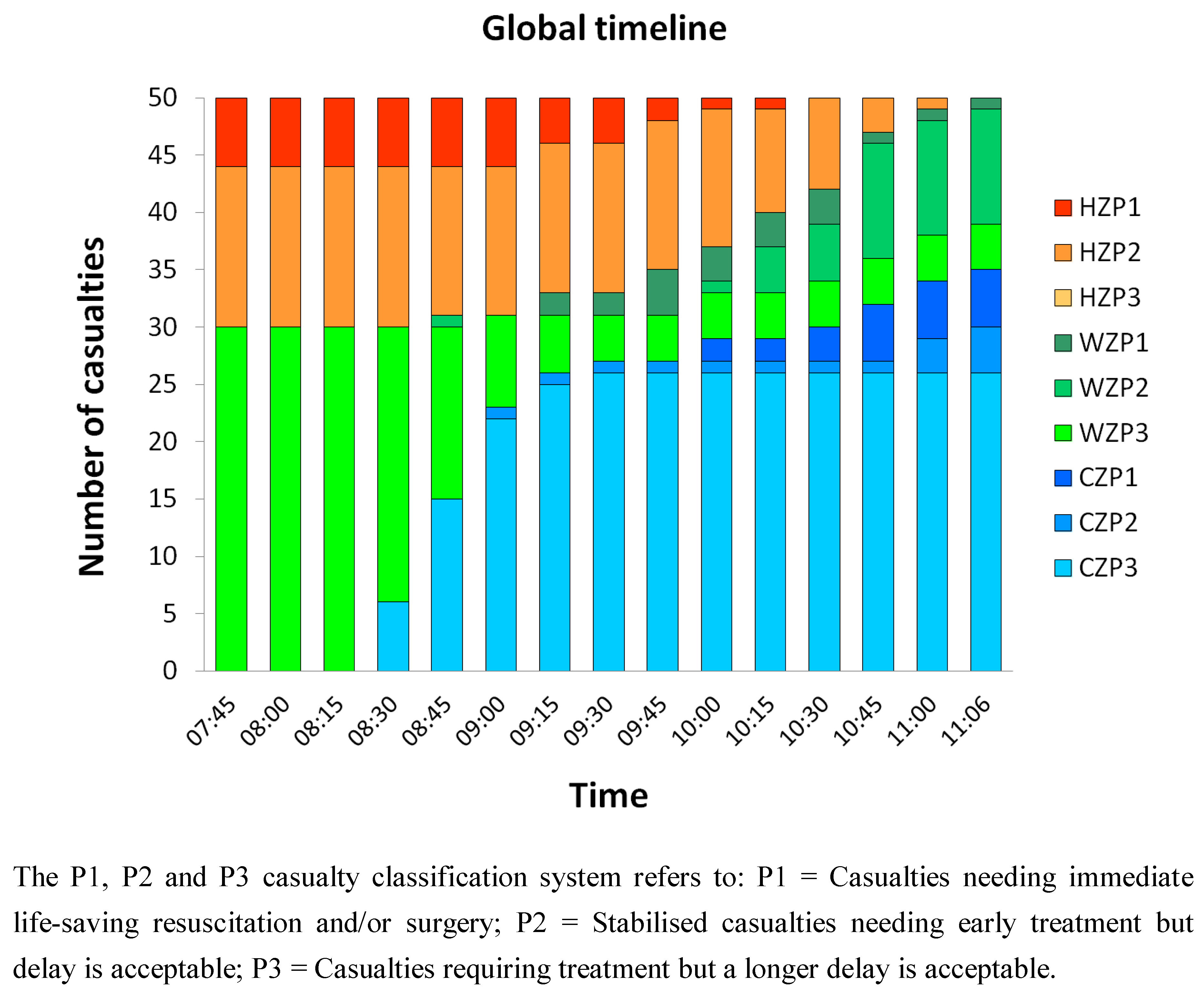
To evaluate the current procedures outlined above we collected casualty movement data from two UK mass decontamination field exercises. Exercise 1 assumed an accidental release of a hazardous material and therefore involved the local FRS and Ambulance Service. There were 50 casualties in total comprising both able-bodied and disabled volunteers who were recruited mainly from a university local to the exercise location and a number of disability organisations. The casualties had a median age of 24 (range 16 to 67) and a standard deviation of 13.4 years. Exercise 2 assumed a deliberate release and therefore also involved the Police Service. A total of 130 volunteer casualties comprised only the able-bodied who were recruited mainly from two further-education colleges local to the exercise location. The casualties had a median age of 17 (range 9 to 53) and a standard deviation of 6.6 years. For both exercises the characteristics of the casualties (e.g., age, gender, disability) and their total number were largely determined in advance by the exercise organisers and were outside of the authors’ control. Casualties were tracked by providing each of them with a passive Radio Frequency Identification (RFID) tag supplied by FR Systems (Stoke on Trent, UK). Mats that could detect the presence of the RFID tags were placed at pre-defined locations (see
Figure 1) allowing a calculation of the time that each casualty had spent at each stage of the decontamination process. For the purposes of this study we restricted our analysis to the processing times of ambulant casualties within the three sections of the MD1. Interested readers can find further details describing the casualty movement analysis in the Supplementary Material.
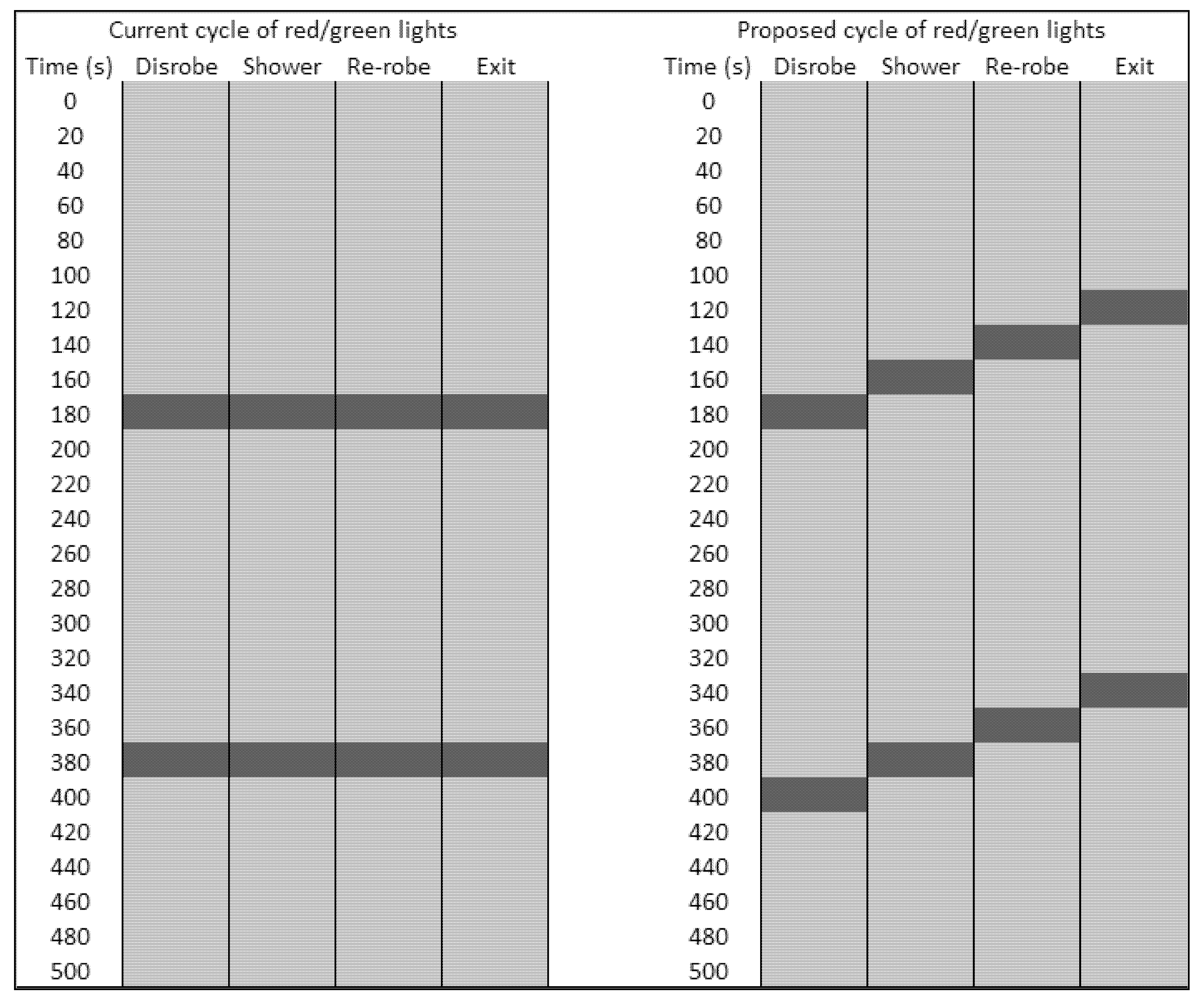
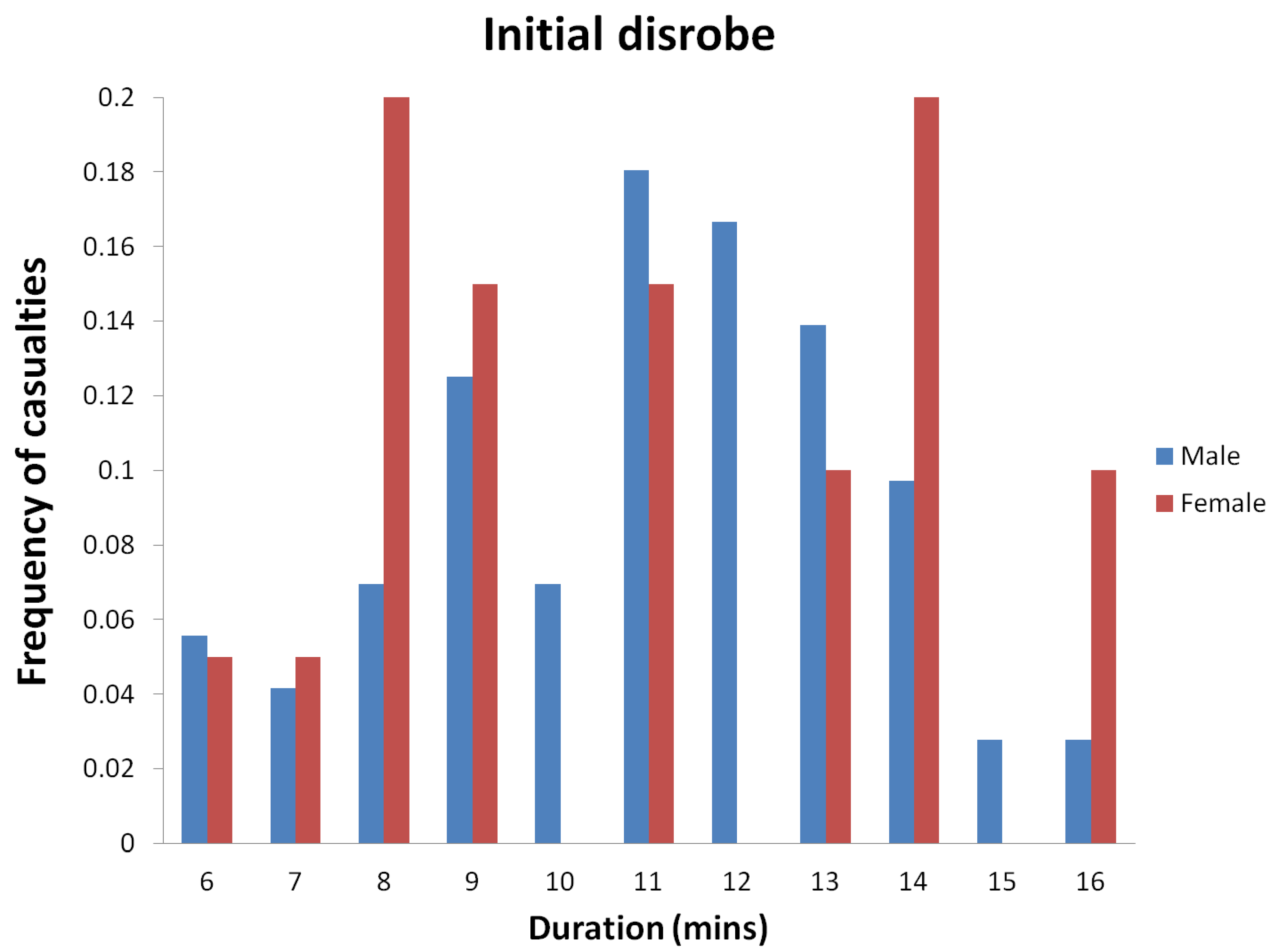
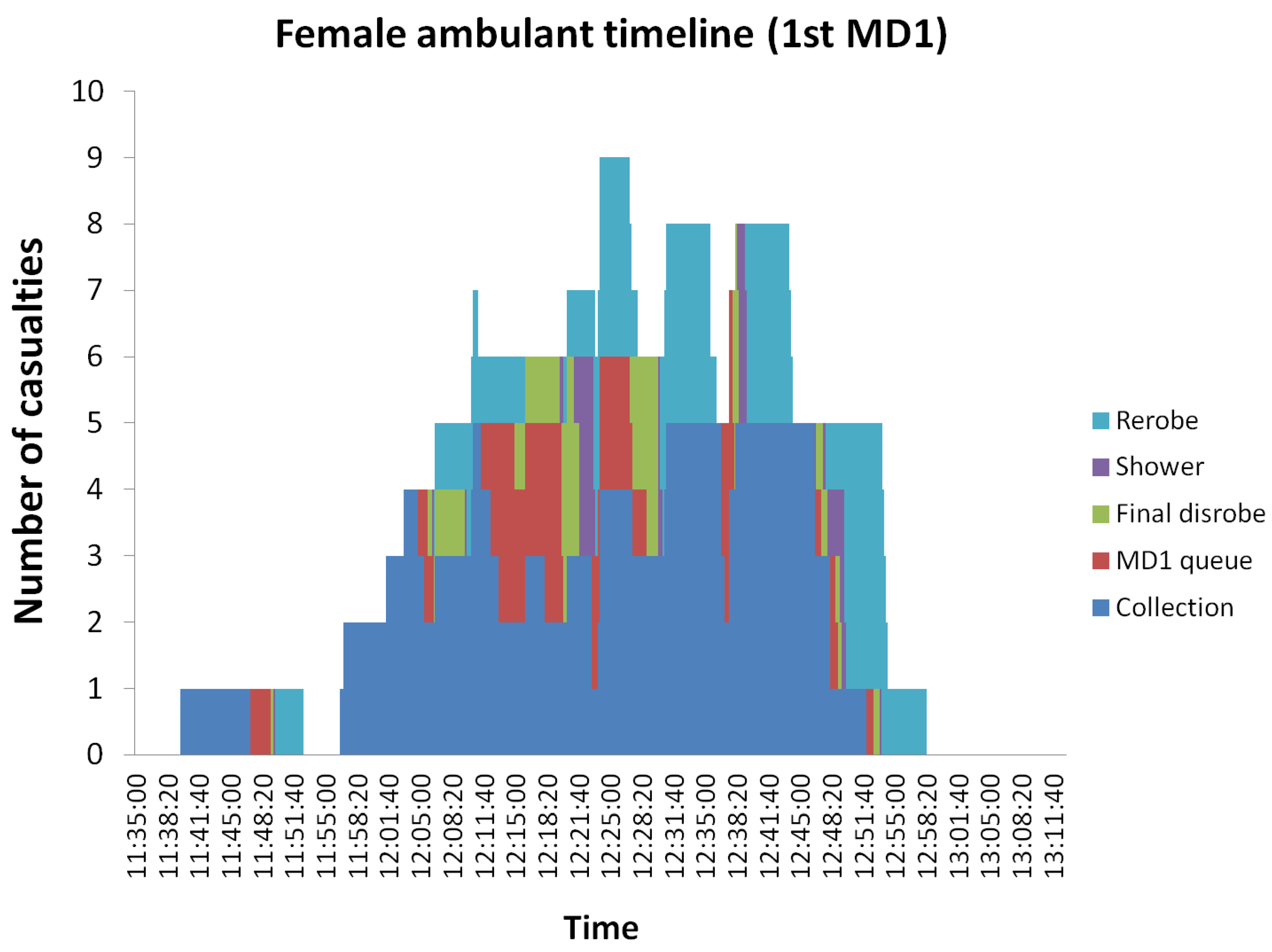
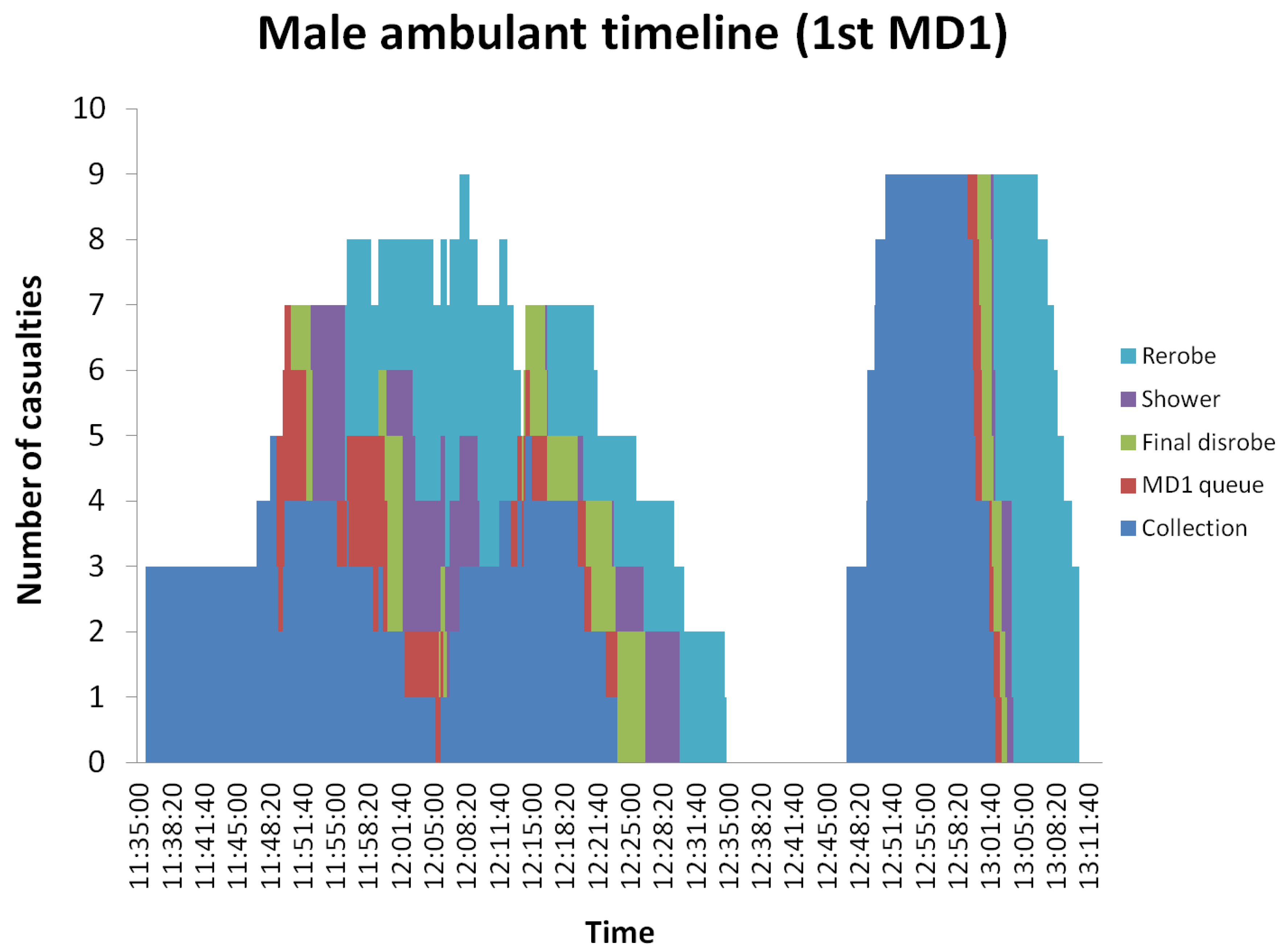
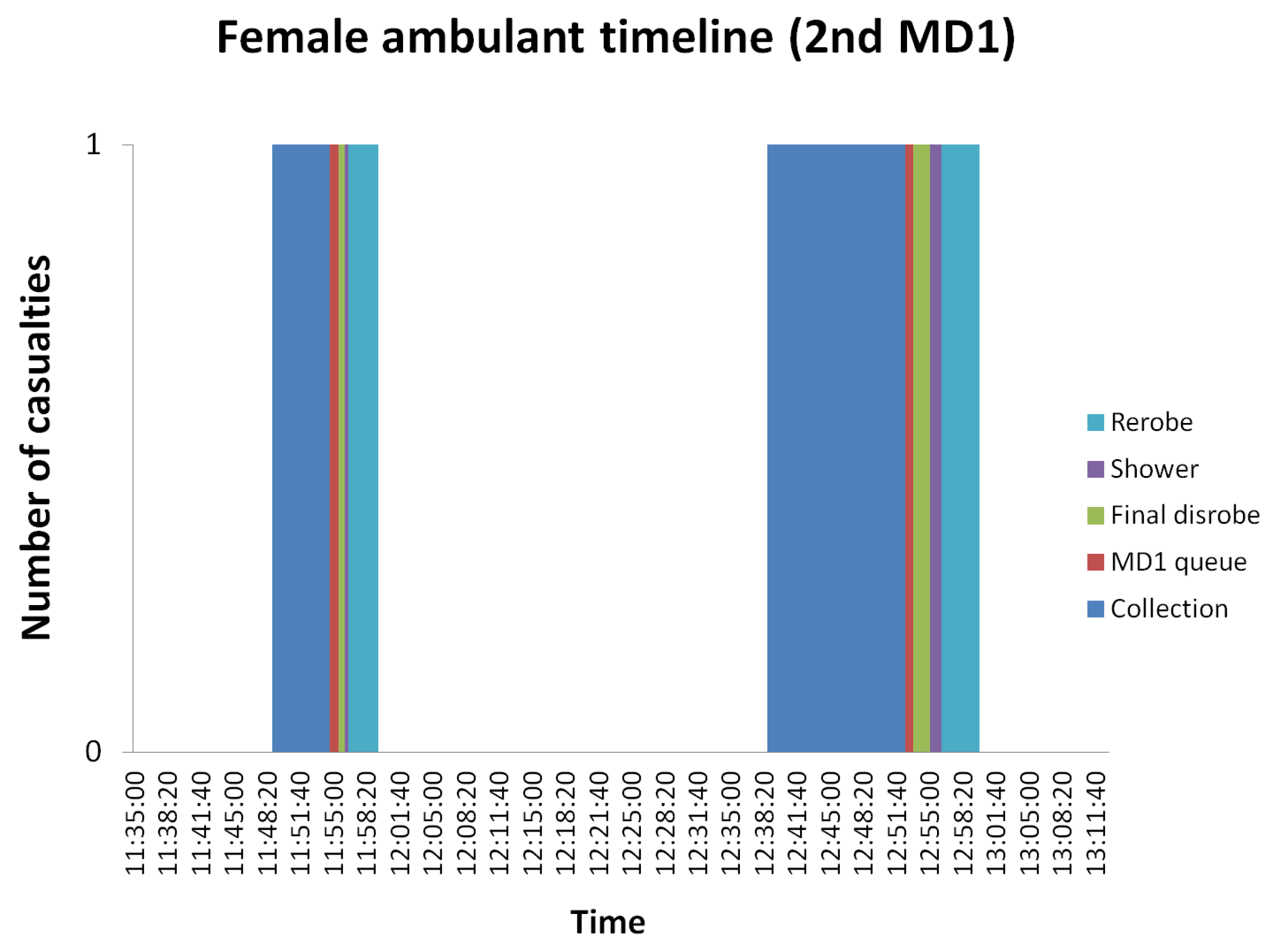
Figure 2 shows a range of times spent in each section of the MD1 suggesting that the flow control system was often ignored or misunderstood by casualties during both exercises. Notably, casualties in both exercises walked through the shower section into the re-robe section without stopping. This behaviour has also been anecdotally observed at other field exercises but the data provided in
Figure 2 importantly provides quantitative evidence. One possible explanation for this occurrence is that because all of the flow control system lights turn green at the same time, casualties simply pass by each light in the same way as they would in a vehicle travelling through multiple sets of traffic lights. Observational data collected during each of the two exercises (not reported here) suggests that this issue may occur particularly when the number of casualties in each section of the MD1 is fewer than the maximum capacity, and if verbal instructions from emergency services personnel to casualties are not heard or fully understood [
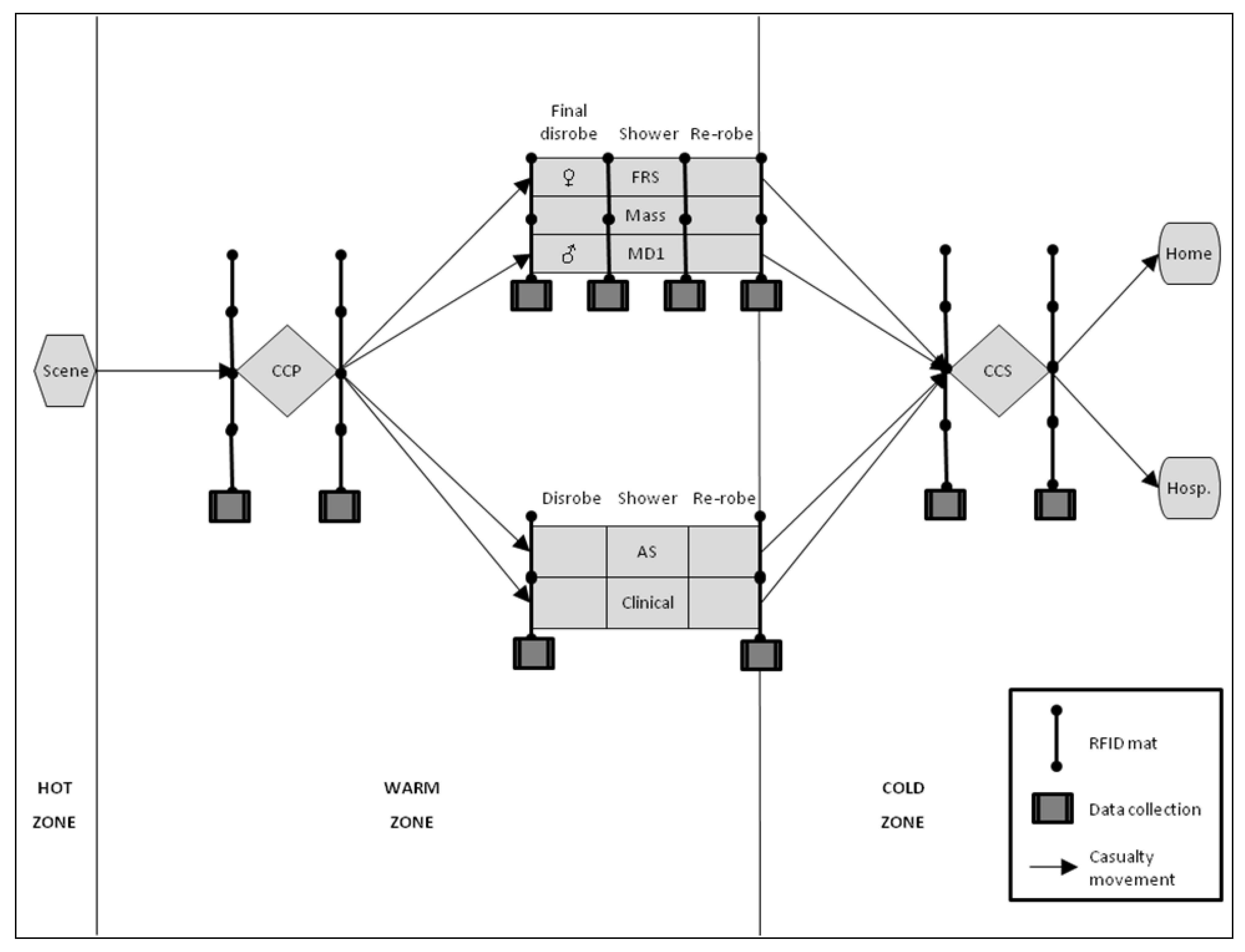
13]. A technical solution to this problem might be to stagger the traffic lights so that having entered one section on a green light, the light to the next section would have already changed to red, thus instructing casualties to wait before proceeding (see
Figure 3). Better communication between emergency services personnel and casualties might also help to improve the flow of casualties through the MD1.
Figure 2.
Histograms of the final disrobe and shower durations for both exercises.
Figure 2.
Histograms of the final disrobe and shower durations for both exercises.
Figure 3.
Current (left) and proposed (right) flow control system. The light and dark grey sections represent the time when the lights are illuminated red and green, respectively. “Disrobe” refers to the final disrobe section as described in the main text.
Figure 3.
Current (left) and proposed (right) flow control system. The light and dark grey sections represent the time when the lights are illuminated red and green, respectively. “Disrobe” refers to the final disrobe section as described in the main text.
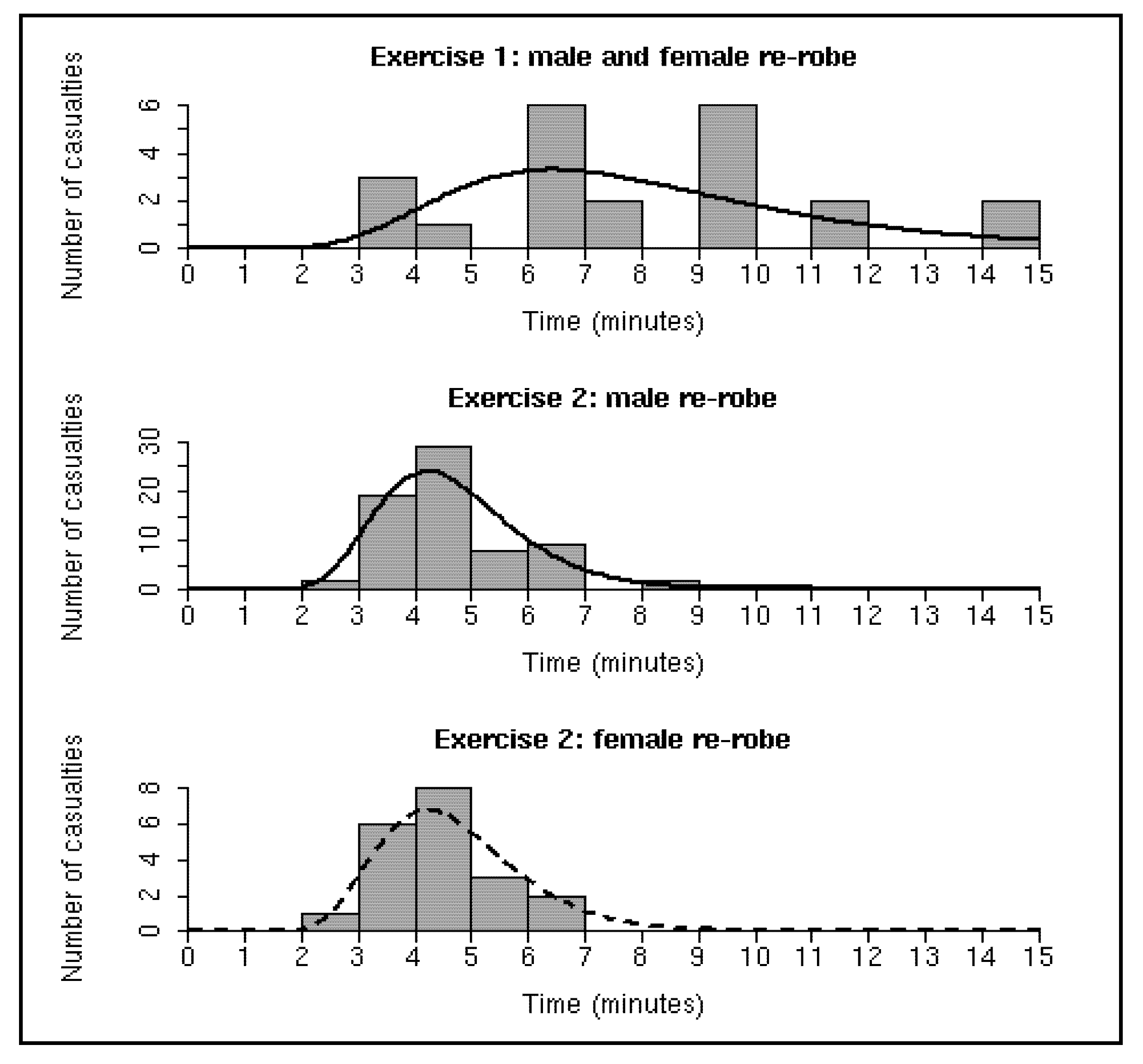
Let us assume that the enhancements outlined above are made to the flow control system and/or that all casualties correctly understand how to proceed through the MD1. In this situation the final disrobe section would essentially become a waiting area because the process of removing the disrobe clothing would likely take significantly less time than the allocated three minutes. Similarly the process of showering could be considered complete when the lights change from red to green after three minutes. However, re-robing is particularly dependent on the individual casualty,
i.e., the re-robe data shown in
Figure 4 are less likely to be an artefact of the flow control system but more likely to reflect the actual time that it takes to dry and dress. Therefore, given that many casualties require more than the allotted three minutes to re-robe (see
Figure 4), it is immediately clear that the re-robe section is a potential bottleneck in the MD1. According to system improvement philosophies the best way to increase throughput is to increase the capacity and/or decrease process time at bottlenecks [
9]. Although it may be possible to speed up re-robing times by making alterations to the clothing within the re-robe pack, in this study we investigate varying the capacity of the re-robe section via computer (discrete event) simulation. In addition, controlled volunteer trials (rather than field exercises) have previously shown that a doubling of the showering duration has demonstrated no significant improvement to the efficacy of decontamination [
14]. Therefore, it is conceivable that there may be scope for decreasing the shower duration without reducing its effectiveness which could help to increase the rate at which casualties flow through the system.
Figure 4.
Histograms of the re-robe durations for both exercises. The solid black lines show the baseline (middle) and worst-case (top) re-robe distribution fits to the data. The dashed black line overlays the baseline fit on the female data in order to highlight their similarity. The worst-case fit is based on a combination of male and female data from Exercise 1 whereas the baseline fit is based only on the male data from Exercise 2.
Figure 4.
Histograms of the re-robe durations for both exercises. The solid black lines show the baseline (middle) and worst-case (top) re-robe distribution fits to the data. The dashed black line overlays the baseline fit on the female data in order to highlight their similarity. The worst-case fit is based on a combination of male and female data from Exercise 1 whereas the baseline fit is based only on the male data from Exercise 2.
4. Methods
Although analytical techniques could have been investigated we were concerned that model formulation and development might quickly become intractable. Therefore, we took a more flexible approach and built a simple model describing the MD1 using the SIMUL8
® software. The final disrobe, shower and re-robe sections were modelled as work-stations with work items representing casualties. In addition to the “drag and drop” functionality used to construct the basic model, we wrote Visual Logic code to capture the flow control system. Casualties could only enter/exit the system and transition between sections when the lights were green and when there was available capacity to do so. In order to capture the behaviour of the system we simulated an unlimited number of casualties queuing at the entrance to the MD1. We also set a conservative warm-up period of 100 minutes to allow the initial simulated casualties to filter through the three MD1 sections before collecting 5,000 additional minutes of simulation output. Note that the computer run-time was not meant to reflect an actual response scenario but rather to allow for a robust statistical analysis of the results. Processing times for the final disrobe and shower sections were set at 3 minutes, equal to the duration of the red light. Any lower values would have produced the same results because the lights are the controlling factor here. Re-robing times were modelled on the raw data collected during the two exercises. Two-parameter gamma, log-normal, and Weibull probability density functions (PDFs) were fitted to the data using the “mle” function in the R stats4 package [
15]. As a sensitivity analysis we varied the simulated shower duration between one and four minutes in one minute intervals by varying the duration of the red lights by the same values. The duration of the green lights remained unchanged at 20 seconds to allow the transition between sections as before. We assumed that the final disrobe could still be completed within one minute (equivalent to the shortest considered shower duration) and so this section effectively remained as a waiting area.
6. Discussion
Personal communications between the authors and FRS personnel suggests that the issues with the re-robe section highlighted in this study are well known. On three separate occasions un-related to the field exercises evaluated in this study, re-robing has been described as often taking longer than the allotted three minutes and that casualties are sometimes stopped from entering the MD1 to allow the bottleneck in the re-robe section to ease. Although this solution is relatively simple to implement it does not exploit the potential of the system and falls short of decontaminating the theoretical maximum of 180 casualties per hour per MD1. Our proposal of increasing the re-robe capacity has also been mentioned by FRS personnel during previous discussions; however, the results in this study provide a scientific platform on which to base decisions regarding the most appropriate capacity. Given that a per lane re-robe capacity of 10 effectively minimises the average time in the system with the baseline re-robe distribution (reflecting a population consisting mainly of able-bodied casualties) perhaps the most practical solution would be to provide a second re-robe section making the MD1 four sections in total. With the worst-case re-robe distribution (reflecting a population consisting mainly of disabled casualties) or if the shower duration was decreased without a detrimental effect on the efficacy of decontamination then consideration might have to be given to a larger or additional re-robe section/s. For example, the process of re-robing might be split in two, analogous to the initial/final disrobe areas; the drying process could potentially be performed in the “initial re-robe” section, with the dressing occurring in the “final re-robe” section. Such proposals, if deemed practical, would have to be tested in future exercises with further data collection of the dry/dress timings allowing informed extensions to the model described in this study.
Immediately after the Tokyo sarin attack there was no field decontamination of casualties on site; instead the local fire department established an emergency rescue quarter at the affected stations containing extra-large ambulances equipped with eight beds and large tents expandable with compressed air. Triage tags were available but were not used because the vast majority of casualties went to local hospitals on foot or via taxis [
1]. In the aftermath of the Bhopal disaster there was no mass casualty emergency response system in place and local hospitals were soon overwhelmed with casualties [
5]. Even with the UK’s current capability of implementing mass decontamination procedures at a safe distance from the Hot Zone it is still likely that many casualties will quickly leave the scene and self-present at hospitals largely in the following six hours [
16]. This brings into question our assumption that ambulant casualties having performed their initial disrobe (averaging approximately 10 minutes, see
Figure A8 in the Supplementary Material) will be queuing for the MD1 prior to its construction. Indeed, we have observed a trickle of casualties into the MD1 (and even then a subsequent overloading of the re-robe section—see
Figure A4 in the Supplementary Material) during the two field exercises reported here. However, our assumption that casualties will be ready to enter the final disrobe section in groups of five (fe)males per lane provides a rigorous test of the system as it is designed. In addition, previous studies have highlighted the uncertainty in arrival times following mass casualty incidents [
8,
9], making it difficult to quantify and justify different numbers of casualties entering simultaneously.
Although we collected additional casualty movement data relating to the varying stages of the emergency response outside of the MD1 during both field exercises (see
Figure 1 and the Supplementary Material), it is difficult to gauge how such information might help to inform the modelling of a more complete system. For example, as casualties left the re-robe section in Exercise 1 they quickly entered a casualty clearing station with a capacity of 12 whereas in Exercise 2 the casualties were transported in a mini-bus to a survivor centre with an essentially unlimited capacity. During such field exercises the experiences of casualties can be captured via questionnaires and interviews providing useful feedback for emergency response organisations. However, from a modelling perspective the data might be considered exercise dependent and not generally applicable—Albores and Shaw summarise the predicament as follows: “…one limitation is the availability of accurate input data—a result of rare, unexpected incidents being heavily effected by uncontrollable variables. Evaluations of real incidents, and large-scale simulation [field] exercises, may provide this data although such simulations tend to lack the chaos and confusion of unprepared members of the public (and some staff) which permeate real disasters and which compromises the quality of the data” [
10]. Nevertheless, the MD1 is one component of the entire process that has been distributed nationally and where data collection and modelling can provide useful insights.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}











