Elevated Bathing-Associated Disease Risks Despite Certified Water Quality: A Cohort Study

 ,
, 

Abstract
:Abbreviations
| EU | European Union |
| EPA | US Environmental Protection Agency |
| OR | odds ratio |
| RR | relative risk |
1. Introduction
2. Results
2.1. Demographics

{kind=link}
| Bathers ( n = 3805) | Non-bathers ( n = 572) | ||||
|---|---|---|---|---|---|
| No. | (%) | No. | (%) | ||
| Age (years) | |||||
| 0–4 | 102 | (2.7) | 19 | (3.3) | |
| 5–9 | 147 | (3.9) | 23 | (4.0) | |
| 10–14 | 185 | (4.9) | 26 | (4.5) | |
| 15–19 | 599 | (15.7) | 38 | (6.6) | |
| 20–24 | 742 | (19.5) | 69 | (12.1) | |
| 25–29 | 541 | (14.2) | 33 | (5.8) | |
| 30–34 | 350 | (9.2) | 34 | (5.9) | |
| 35–39 | 295 | (7.8) | 54 | (9.4) | |
| 40–44 | 273 | (7.2) | 50 | (8.7) | |
| 45–49 | 210 | (5.5) | 52 | (9.1) | |
| 50–54 | 129 | (3.4) | 41 | (7.2) | |
| 55–59 | 90 | (2.4) | 33 | (5.8) | |
| 60–64 | 39 | (1.0) | 19 | (3.3) | |
| 65–69 | 31 | (0.8) | 20 | (3.5) | |
| 70+ | 46 | (1.2) | 61 | (10.7) | |
| missing | 26 | (0.6) | 0 | (0.0) | |
| Gender | |||||
| Male | 1837 | (48.3) | 243 | 42.5 | |
| Female | 1947 | (51.2) | 329 | 57.5 | |
| missing | 21 | (0.5) | 0 | (0.0) | |
| Residence | |||||
| Larissa area(Locals) | 2521 | (66.2) | 450 | (78.7) | |
| Thessaly (except of Larissa area) (Visitors) | 726 | (19.1) | 91 | (15.9) | |
| Greece (except of Thessaly area) (Visitors) | 543 | (14.3) | 31 | (5.4) | |
| missing | 15 | (0.4) | 0 | (0.0) | |
| Incidence of illness among locals | |||||
| Gastroenteritis (A) a | 61 | (2.4) | 3 | (0.7) | |
| Gastroenteritis (B) b | 39 | (1.6) | 2 | (0.4) | |
| Respiratory infection (A) a | 149 | (5.9) | 11 | (2.4) | |
| Respiratory infection (B) b | 52 | (2.1) | 6 | (1.3) | |
| Ear infection (A) a | 77 | (3.1) | 1 | (0.2) | |
| Ear infection (B) b | 18 | (0.7) | 0 | (0.0) | |
| Eye infection (A) a | 132 | (5.2) | 8 | (1.8) | |
| Eye infection (B) b | 50 | (2.1) | 3 | (0.7) | |
| Cutaneous infection | 12 | (0.5) | 1 | (0.2) | |
| Medical consultation | 55 | (2.2) | 2 | (0.4) | |
| Medication receiving | 87 | (3.5) | 5 | (1.1) | |
| Hospitalization/home care | 4 | (0.2) | 1 | (0.2) | |
| Incidence of illness among visitors | |||||
| Gastroenteritis (A) a | 53 | (4.2) | 1 | (0.8) | |
| Gastroenteritis (B) b | 35 | (2.8) | 1 | (0.8) | |
| Respiratory infection (A) a | 87 | (6.9) | 4 | (3.4) | |
| Respiratory infection (B) b | 31 | (2.6) | 1 | (0.8) | |
| Ear infection (A) a | 52 | (4.1) | 0 | (0.0) | |
| Ear infection (B) b | 9 | (0.7) | 0 | (0.0) | |
| Eye infection (A) a | 73 | (5.8) | 3 | (2.5) | |
| Eye infection (B) b | 26 | (2.1) | 0 | (0.0) | |
| Cutaneous infection | 9 | (0.7) | 0 | (0.0) | |
| Medical consultation | 40 | (3.2) | 2 | (1.6) | |
| Medication receiving | 52 | (4.1) | 1 | (0.8) | |
| Hospitalization/home care | 1 | (0.1) | 0 | (0.0) | |
2.2. Microbiological Water Quality
| Beach | (cfu/100 mL) | ECOL * | FCOL * | TCOL * | Enterococci |
|---|---|---|---|---|---|
| A | 95-Percentile | 14.9 | 33.1 | 58.8 | 64.6 |
| Geometric mean (range) | 2.2 | 2.9 | 4.5 | 5.6 (0–1380) | |
| N | 67 | 67 | 67 | 67 | |
| B | 95-percintile | 10.8 | 11.2 | 26.5 | 16.3 |
| Geometric mean (range) | 1.9 | 2.0 | 3.1 | 2.8 (0–74) | |
| N | 61 | 61 | 61 | 61 | |
| C | 95-percintile | 4.7 | 5.4 | 17.4 | 10.6 |
| Geometric mean (range) | 1.6 | 1.7 | 3.0 | 2.5 (0–15) | |
| N | 21 | 21 | 21 | 21 |
2.3. Symptoms Related to Infectious Diseases
| Symptom | Bathers with symptom/total (%) | Non bathers with symptom/total (%) | Relative Risk | p-value |
|---|---|---|---|---|
| Nausea or vomiting | 40/3796 (1.1) | 0/571 (0.0) | 12.20 a | 0.022 |
| Abdominal pain | 74/3796 (1.9) | 3/571 (0.5) | 3.71 | 0.016 |
| Diarrhea more than two times | 39/3796 (1.0) | 4/571 (0.7) | 1.47 | 0.461 |
| Fever | 11/3796 (0.3) | 1/571 (0.2) | 1.66 | 0.626 |
| Gastroenteritis (A) | 114/3796 (3.0) | 4/571 (0.7) | 4.29 | 0.002 |
| Gastroenteritis (B) | 74/3778 (2.0) | 3/570 (0.5) | 3.72 | 0.016 |
| Sore throat | 100/3796 (2.6) | 3/571 (0.5) | 5.01 | 0.002 |
| Dysphagia (odynophagia) | 41/3796 (1.1) | 2/571 (0.4) | 3.08 | 0.101 |
| Rheum (runny nose) | 72/3796 (1.9) | 7/571 (1.2) | 1.55 | 0.433 |
| Cough | 84/3796 (2.2) | 8/571 (1.4) | 1.58 | 0.330 |
| Hoarseness | 79/3796 (2.1) | 10/571 (1.8) | 1.19 | 0.673 |
| Respiratory infection (A) | 236/3796 (6.2) | 15/571 (2.6) | 2.37 | 0.005 |
| Respiratory illness (B) | 83/3643 (2.3) | 7/563 (1.2) | 1.83 | 0.236 |
| Ear pain | 93/3796 (2.4) | 1/571 (0.2) | 13.99 | <0.001 |
| Fullness in the ear | 35/3796 (0.9) | 0/571 (0.0) | 10.70 a | 0.035 |
| Otorrhea | 21/3796 (0.6) | 0/571 (0.0) | 6.48 a | 0.100 |
| Ear itching | 16/3796 (0.4) | 0/571 (0.0) | 4.97 a | 0.174 |
| Ear infection (A) | 129/3796 (3.4) | 1/571 (0.2) | 19.40 | <0.001 |
| Ear infection (B) | 27/3694 (0.7) | 0/570 (0.0) | 8.50 a | 0.067 |
| Eye redness | 145/3796 (3.8) | 3/571 (0.5) | 7.27 | <0.001 |
| Eye pain or burn | 91/3796 (2.4) | 4/571 (0.7) | 3.42 | 0.010 |
| Tear secretion (eyes discharge) | 43/3796 (1.0) | 7/571 (1.2) | 0.92 | 0.861 |
| Mucopurulent exudates (eye) | 25/3796 (0.7) | 0/571 (0.0) | 7.68 a | 0.081 |
| Eye infection (A) | 205/3796 (5.4) | 11/571 (1.9) | 2.80 | 0.001 |
| Eye infection (B) | 76/3667 (2.1) | 3/563 (0.5) | 3.89 | 0.012 |
| Cutaneous infection | 21/3796 (0.6) | 1/571 (0.2) | 3.16 | 0.233 |
| Urinary tract infection b | 6/1944 (0.3) | 0/328 (0.0) | 2.20 a | 0.320 |
| Vaginitis b | 24/1944 (1.2) | 1/328 (0.3) | 4.05 | 0.135 |
| Medical consultation | 94/3796 (2.5) | 4/571 (0.7) | 3.54 | 0.008 |
| Medication receiving | 139/3796 (3.7) | 6/571 (1.1) | 3.49 | 0.001 |
| Hospitalization/home care | 5/3796 (0.1) | 1/571 (0.2) | 0.75 | 0.794 |
| Symptom | Odds Ratio | 95% CI | p-value | AUC b |
|---|---|---|---|---|
| Abdominal pain | 3.16 | 0.95–10.51 | 0.061 | 0.638 |
| Diarrhea more than two times | 1.06 | 0.35–3.21 | 0.911 | 0.658 |
| Gastroenteritis (A) | 3.60 a | 1.28–10.13 | 0.015 | 0.632 |
| Gastroenteritis (B) | 3.16 | 0.95–10.52 | 0.060 | 0.639 |
| Sore throat | 4.28 a | 1.35–13.51 | 0.013 | 0.653 |
| Dysphagia (odynophagia) | 2.45 | 0.60–10.02 | 0.213 | 0.643 |
| Rheum (runny nose) | 1.17 | 0.38–3.66 | 0.783 | 0.647 |
| Cough | 1.27 | 0.49–3.26 | 0.627 | 0.643 |
| Hoarseness | 0.93 | 0.41–2.14 | 0.872 | 0.618 |
| Respiratory infection (A) | 1.92 a | 1.00–3.67 | 0.049 | 0.648 |
| Respiratory infection (B) | 1.50 | 0.53–4.21 | 0.444 | 0.672 |
| Ear pain | 12.02 a | 1.69–85.58 | 0.013 | 0.685 |
| Ear infection (A) | 17.21 a | 2.42–122.34 | 0.004 | 0.659 |
| Eye redness | 6.15 a | 2.00–18.91 | 0.002 | 0.651 |
| Eye pain or burn | 3.10 a | 1.19–8.06 | 0.021 | 0.671 |
| Tear secretion | 0.82 | 0.35–1.91 | 0.641 | 0.577 |
| Eye infection (A) | 2.43 a | 1.27–4.63 | 0.007 | 0.631 |
| Eye infection (B) | 3.48 a | 1.16–10.42 | 0.026 | 0.654 |
| Cutaneous infection | 2.92 | 0.38–22.62 | 0.306 | 0.635 |
| Medical consultation | 3.07 a | 1.15–8.23 | 0.026 | 0.632 |
| Medication receiving | 2.98 a | 1.30–6.82 | 0.010 | 0.615 |
2.4. Symptoms Related to GI and RI
2.5. Symptoms Related to Ear Eye and Cutaneous Infections
| Food consumption | Swimming time a | Head immersion | Enterococci density b | Bather density c | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptom | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Abdominal pain | 1.11 | (0.67–1.83) | 0.689 | 1.96 | (1.17–3.30) | 0.011 | 1.35 | (0,64–2,86) | 0.434 | 0.53 | (0.13–2.23) | 0.385 | 2.01 | (1.00–4.03) | 0.049 |
| Diarrhea more than 2 times | 0.95 | (0.51–1.79) | 0.881 | 1.74 | (0.84–3.59) | 0.136 | 0.98 | (037–259) | 0.960 | NA | NA | NA | 4.10 | (1.42–11.80) | 0.009 |
| Gastroenteritis (A) | 1.01 | (0.67–1.53) | 0.968 | 1.22 | (0.75–1.99) | 0.424 | 0.99 | (0.57–1.71) | 0.968 | 0.68 | (0.27–1.76) | 0.428 | 1.34 | (0.81–2.21) | 0.250 |
| Gastroenteritis (B) | 1.10 | (0.67–1.82) | 0.704 | 1.94 | (1.15–3.27) | 0.013 | 1.35 | (0.64–2.86) | 0.433 | 0.53 | (0.12–2.22) | 0.382 | 2.02 | (1.01–4.06) | 0.048 |
| Sore throat | 0.57 | (0.36–0.89) | 0.013 | 1.69 | (1.02–2.82) | 0.043 | 0.89 | (0.49–1.62) | 0.699 | 0.62 | (0.19–2.00) | 0.420 | 1.71 | (1.01–2.87) | 0.044 |
| Dysphagia (odynophagia) | 0.45 | (0.22–0.92) | 0.029 | 2.34 | (1.08–5.05) | 0.030 | 1.15 | (0.42–3.11) | 0.786 | 1.26 | (0.31–5.15) | 0.749 | 2.46 | (1.05–5.76) | 0.038 |
| Rheum (runny nose) | 0.68 | (0.40–1.14) | 0.144 | 0.76 | (0.37–1.56) | 0.454 | 1.13 | (0.52–2.46) | 0.754 | NA | NA | NA | 1.74 | (0.93–3.25) | 0.084 |
| Cough | 0.60 | (0.38–0.97) | 0.037 | 1.68 | (0.95–2.97) | 0.075 | 1.61 | (0.66–3.92) | 0.292 | 1.41 | (0.53–3.79) | 0.495 | 2.20 | (1.18–4.12) | 0.014 |
| Hoarseness | 0.47 | (0.28–0.80) | 0.005 | 1.49 | (0.79–2.84) | 0.219 | 1.10 | (0.53–2.28) | 0.802 | 0.25 | (0.03–1.84) | 0.174 | 1.64 | (0.88–3.07) | 0.123 |
| Respiratory infection (A) | 0.56 | (0.41–0.76) | <0.001 | 1.23 | (0.85–1.79) | 0.270 | 1.18 | (0.74–1.87) | 0.483 | 0.58 | (0.26–1.29) | 0.180 | 1.77 | (1.22–2.55) | 0.003 |
| Respiratory infection (B) | 0.54 | (0.33–0.88) | 0.014 | 1.62 | (0.91–2.87) | 0.102 | 0.88 | (0.46–1.67) | 0.684 | 0.89 | (0.28–2.89) | 0.847 | 2.79 | (1.49–5.22) | 0.001 |
| Ear pain | 0.77 | (0.49–1.21) | 0.258 | 1.34 | (0.79–2.26) | 0.276 | 0.89 | (0.47–1.65) | 0.700 | 0.61 | (0.18–2.00) | 0.413 | 1.59 | (0.91–2.76) | 0.101 |
| Ear infection (A) | 0.68 | (0.45–1.00) | 0.052 | 1.32 | (0.82–2.13) | 0.261 | 0.85 | (0.51–1.43) | 0.547 | 0.85 | (0.36–2.02) | 0.717 | 1.60 | (1.01–2.52) | 0.044 |
| Eye redness | 0.71 | (0.48–1.06) | 0.096 | 1.55 | (0.96–2.50) | 0.072 | 1.31 | (0.69–2.49) | 0.407 | 1.32 | (0.56–3.14) | 0.526 | 0.94 | (0.63–1.42) | 0.782 |
| Eye pain or burn | 0.55 | (0.34–0.88) | 0.013 | 2.05 | (1.19–3.51) | 0.009 | 1.63 | (0.77–3.48) | 0.205 | 0.56 | (0.17–1.86) | 0.341 | 1.14 | (0.66–1.95) | 0.644 |
| Tear secretion | 0.62 | (0.29–1.34) | 0.223 | 0.98 | (0.38–2.54) | 0.973 | 1.10 | (0.41–2.95) | 0.847 | 0.30 | (0.04–2.19) | 0.233 | 0.77 | (0.35–1.70) | 0.522 |
| Eye infection (A) | 0.63 | (0.45–0.89) | 0.008 | 1.52 | (1.01-2.30) | 0.047 | 1.33 | (0.79–2.25) | 0.286 | 0.94 | (0.42–2.13) | 0.887 | 0.94 | (0.65–1.36) | 0.741 |
| Eye infection (B) | 0.80 | (0.47–1.36) | 0.415 | 1.84 | (1.06–3.22) | 0.032 | 1.68 | (0.69–4.11) | 0.254 | 0.62 | (0.18–2.12) | 0.446 | 0.86 | (0.48–1.53) | 0.605 |
| Cutaneous infection | 0.38 | (0.12–1.25) | 0.112 | 0.98 | (0.20–4.80) | 0.984 | 0.31 | (0.11–0.88) | 0.027 | 1.57 | (0.35–6.94) | 0.555 | 1.15 | (0.39–3.37) | 0.805 |
| Medical consultation | 0.92 | (0.58–1.45) | 0.712 | 1.33 | (0.75–2.35) | 0.328 | 0.32 | (0.19–0.53) | <0.001 | 0.98 | (0.33–2.92) | 0.974 | 2.51 | (1.40–4.50) | 0.002 |
| Medication receiving | 0.80 | (0.54–1.18) | 0.259 | 1.00 | (0.61–1.65) | 0.993 | 0.76 | (0.46–1.27) | 0.301 | 0.81 | (0.32–2.00) | 0.641 | 2.10 | (1.28–3.44) | 0.003 |
2.6. Need for Medical Consultation or Use of Medication
3. Discussion
4. Experiment Section
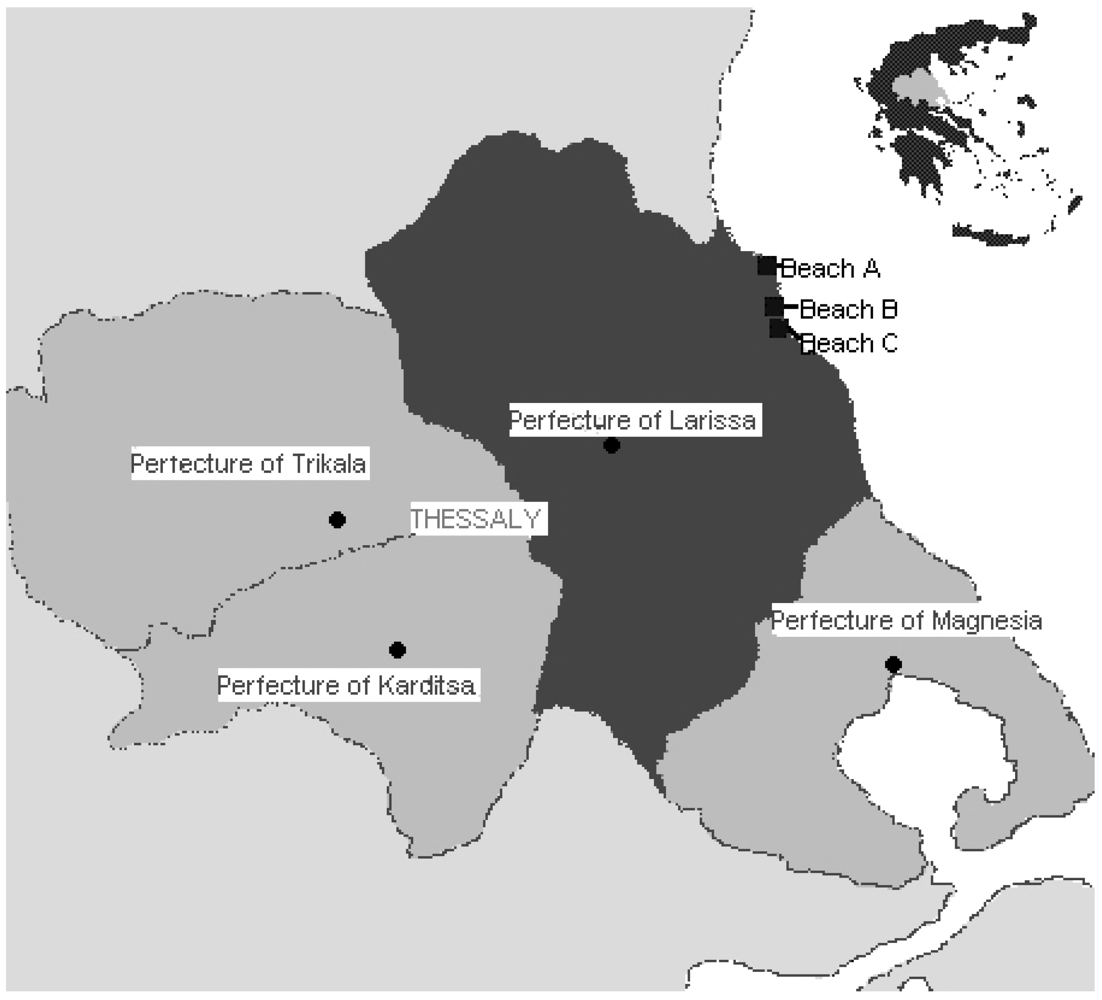
4.1. Study Beaches and Study Population

4.2. Questionnaire and Data Collection
4.3. Self-Reported Symptoms and Disease Definitions
- Gastrointestinal infection (GI): nausea/vomiting, abdominal pain, diarrhea (defined as two or more loose or watery stools in a 24-hour period), fever.
- RI: sore throat, dysphagia (odynophagia, pain during deglutition), rheum, cough, hoarseness. Respiratory illness in our study included infection of the upper or lower respiratory organs.
- Ear infection: ear pain, sense of fullness in the ear, otorrhea, ear itching.
- Eye infection: Red eye (redness of the conjunctiva), eye pain/burning, eye secretion, mucopurulent exudate.
- Symptoms possibly related to cutaneous infection (e.g., self-reported symptoms as rash).
4.4. Microbiological Water Quality Assessment
4.5. Statistical Analysis
5. Conclusions
Acknowledgements
Conflict of Interest
References
- Stevenson, A.H. Studies of bathing water quality and health. Am. J. Public Health Nations Health 1953, 43, 529–538. [Google Scholar]
- Ferley, J.P.; Zmirou, D.; Balducci, F.; Baleux, B.; Fera, P.; Larbaigt, G.; Jacq, E.; Moissonnier, B.; Blineau, A.; Boudot, J. Epidemiological significance of microbiological pollution criteria for river recreational waters. Int J. Epidemiol. 1989, 18, 198–205. [Google Scholar]
- Fleisher, J.M.; Kay, D.; Salmon, R.L.; Jones, F.; Wyer, M.D.; Godfree, A.F. Marine waters contaminated with domestic sewage: Nonenteric illnesses associated with bather exposure in the United Kingdom. Am. J. Public Health 1996, 86, 1228–1234. [Google Scholar]
- Kay, D.; Fleisher, J.M.; Salmon, R.L.; Jones, F.; Wyer, M.D.; Godfree, A.F.; Zelenauch-Jacquotte, Z.; Shore, R. Predicting likelihood of gastroenteritis from sea bathing; results from randomized exposure. Lancet 1994, 344, 905–909. [Google Scholar]
- Marino, F.J.; Morinigo, M.A.; Martinez-Manzanares, E.; Borrego, J.J. Microbiological-epidemiological study of selected marine beaches in Malaga (Spain). Water Sci. Technol. 1995, 31, 5–9. [Google Scholar]
- Corbett, S.J.; Rubin, G.L.; Curry, G.K.; Kleinbaum, D.G. The health effects of swimming at Sydney beaches. The Sydney Beach Users Advisory Group. Am. J. Public Health 1993, 83, 1701–1706. [Google Scholar] [CrossRef]
- Pruss, A. A review of epidemiological studies from exposure to recreational water. Int. J. Epidemiol. 1998, 27, 1–9. [Google Scholar]
- Wade, T.J.; Pai, N.; Eisenberg, J.N.S.; Colford, J.M.J. Do U.S. environmental protection agency water quality guidelines for recreational waters prevent gastrointestinal illness? A systematic review and meta-analysis. Environ. Health Perspect. 2003, 111, 1102–1109. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency (USEPA), Ambient Water Quality Criteria for Bacteria-1986. Tech Rep EPA-440/5-84-002. Office of Water Regulations and Standards, Criteria and Standards Division: Washington, DC, USA, 1986.
- European Union. Directive 2006/7/EC of the European Parliament and of the Council of 15 February 2006 concerning the management of bathing water quality and repealing Directive 76/160/EEC. Off. J. Eur. Union 2006, L64, 37–51.
- European Union. Council directive 76/160/EEC of 8 December 1975 concerning the quality of bathing water. Off. J. Eur. Communities 1976, L31, 1–7.
- Ministerial decision oik 46399/1352/86. Available online: http://www.elinyae.gr/el/lib_file_upload/438-86.1112683462745.pdf (accessed on 22 February 2011).
- Common Ministerial decision HΠ8600/416/Ε103. Available online: http://www.ypeka.gr/LinkClick.aspx?fileticket=CGZnB%2B5RXjk%3D&tabid=253&llanguag=el-GR (accessed on 4 February 2011).
- Papastergiou, P.; Mouchtouri, V.; Karanika, M.; Kostara, E.; Kolokythopoulou, F.; Mpitsolas, N.; Papaioannou, A.; Hadjichristodoulou, C. Analysis of seawater microbiological quality data in Greece from 1997 to 2006: association of risk factors with bacterial indicators. J. Water Health 2009, 7, 514–526. [Google Scholar]
- World Health Organization (WHO), Guidelines for Safe Recreational Waters. Volume 1. Coastal and Fresh Waters; WHO: Geneva, Switzerland, 2003.
- Borrego, J.; Romero, P.; Marino, F. Epidemiological Studies Related to Environmental Quality Criteria for Bathing Waters, Shellfish Growing Waters and Edible Marine organisms. Final Report on Epidemiological Study on Bathers from Selected Beaches in Malaga, Spain 1988-89. MAP Technical Reports Series; United Nations Environment Programme: Athens, Greece, 1999; Volume 53. [Google Scholar]
- Cabelli, V.J.; Dufour, A.P.; McCabe, L.J.; Levin, M.A. Swimming-associated gastroenteritis and water quality. Am. J. Epidemiol. 1982, 115, 606–616. [Google Scholar]
- Cheung, W.H.; Chang, K.C.; Hung, R.P.; Kleevens, J.W. Health effects of beach water pollution in Hong Kong. Epidemiol. Infect. 1990, 105, 139–162. [Google Scholar]
- Prieto, M.D.; Lopez, B.; Juanes, J.A.; Revilla, J.A.; Delgardo-Rodrigues Llorca, J. Receation in coastal waters: Health risks associated with bathing in sea water. J. Epidemiol. Community Health 2001, 55, 442–447. [Google Scholar]
- Given, S.; Pendleton, L.H.; Boehm, A.B. Regional public health cost estimates of contaminated coastal waters: A case study of gastroenteritis at southern California beaches. Environ. Sci. Technol. 2006, 40, 4851–4588. [Google Scholar]
- Brinks, M.V.; Dwight, R.H.; Osgood, N.D.; Sharavanakumar, G.; Turbow, D.J.; El-Gohary, M.; Caplan, J.S.; Semenza, J.C. Health risk of bathing in Southern California coastal waters. Arch. Environ. Occup. Healt. 2008, 63, 123–135. [Google Scholar]
- Corbett, S.J.; Rubin, G.L.; Curry, G.K.; Kleinbaum, D.G. The health effects of swimming at Sydney beaches. The Sydney Beach Users Study Advisory Group. Am. J. Public Health 1993, 83, 1701–1706. [Google Scholar] [CrossRef]
- Van Asperen, I.A.; Medema, G.; Borgdorff, M.W.; Sprenger, M.J.; Havelaar, A.H. Risk of gastroenteritis among triathletes in relation to faecal pollution of fresh waters. Int. J. Epidemiol. 1998, 27, 309–315. [Google Scholar]
- Marion, J.W.; Lee, J.; Lemeshow, S.; Buckley, T.J. Association of gastrointestinal illness and recreational water exposure at an inland U.S. beach. Water Res. 2010, 44, 4796–4804. [Google Scholar] [CrossRef]
- Yau, V.; Wade, T.J.; deWilde, C.K.; Colford, J.M., Jr. Skin-related symptoms following exposure to recreational water: a systematic review and meta-analysis. Water Qual. Expo. Health 2009, 1, 79–103. [Google Scholar]
- Andersson, Y.; Ekdahl, K. Wound infections due to Vibrio cholerae in Sweden after swimming in the Baltic Sea. Summer 2006. Eurosurveillamce 2006, 11, E060803–2. [Google Scholar]
- Schets, F.M.; van den Berg, H.H.; Demeulmeester, A.A.; van Dijk, E.; Rutjes, S.A.; van Hooijdonk, H.J.; de Roda Husman, A.M. Vibrio alginolyticus infections in the Netherlands after swimming in the North Sea. Eurosurveillance 2006, 11, E061109–3. [Google Scholar]
- Papastergiou, P.; Mouchtouri, V.; Rachiotis, G.; Pinaka, O.; Katsiaflaka, A.; Hadjichristodoulou, C. Bather density as a predominant factor for health effects related to recreational bathing: Results from the Greek bathers cohort study. Mar. Pollut. Bull. 2010. [Google Scholar]
- Ashbolt, N.J.; Schoen, M.E.; Soller, J.A.; Roser, D.J. Predicting pathogen risks to aid beach management: the real value of quantitative microbial risk assessment (QMRA). Water Res. 2010, 44, 4692–4703. [Google Scholar]
- Fleisher, J.M.; Fleming, L.E.; Solo-Gabriele, H.M.; Kish, J.K.; Sinigalliano, C.D.; Plano, L.; Elmir, S.M.; Wang, J.D.; Withum, K.; Shibata, T.; et al. The BEACHES study: Health effects and exposures from non-point source microbial contaminants in subtropical recreational marine waters. Int. J. Epidemiol. 2010, 39, 1291–1298. [Google Scholar] [CrossRef]
- Hellenic Centre for Diseases Control and Prevention. Available online: http://www.keelpno.gr (accessed on 11 January 2011).
- Agresti, A. Categorical Data Analysis, 2nd ed; John Wiley and Sons Inc.: Hoboken, NJ, USA, 2002. [Google Scholar]
- Field, A.P. Discovering Statistics Using SPSS (and Sex, Drugs and Rock “n” Roll), 2nd ed; Sage: London, UK, 2005. [Google Scholar]
- Kleinbaum, D.G.; Kupper, L.L.; Morgenstern, H. Epidemiologic Research: Principles and Quantitative Methods; Van Nostrand Reinhold: New York, NY, USA, 1982. [Google Scholar]
- Haldane, J.B. The estimation and significance of the logarithm of a ratio of frequencies. Ann. Intern. Med. 1956, 20, 309–311. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Papastergiou, P.; Mouchtouri, V.; Pinaka, O.; Katsiaflaka, A.; Rachiotis, G.; Hadjichristodoulou, C. Elevated Bathing-Associated Disease Risks Despite Certified Water Quality: A Cohort Study. Int. J. Environ. Res. Public Health 2012, 9, 1548-1565. https://doi.org/10.3390/ijerph9051548
Papastergiou P, Mouchtouri V, Pinaka O, Katsiaflaka A, Rachiotis G, Hadjichristodoulou C. Elevated Bathing-Associated Disease Risks Despite Certified Water Quality: A Cohort Study. International Journal of Environmental Research and Public Health. 2012; 9(5):1548-1565. https://doi.org/10.3390/ijerph9051548
Chicago/Turabian StylePapastergiou, Panagiotis, Varvara Mouchtouri, Ourania Pinaka, Anna Katsiaflaka, George Rachiotis, and Christos Hadjichristodoulou. 2012. "Elevated Bathing-Associated Disease Risks Despite Certified Water Quality: A Cohort Study" International Journal of Environmental Research and Public Health 9, no. 5: 1548-1565. https://doi.org/10.3390/ijerph9051548