
Trends in and Risk Factors for Drug Resistance in Mycobacterium tuberculosis in HIV-Infected Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Methods
2.2.1. Specimen Collection and Culture
2.2.2. Drug Susceptibility Test
2.3. Definition of Drug-Resistant Tuberculosis
- Drug-resistant tuberculosis (DR-TB) refers to tuberculosis that has resistance to at least one anti-tuberculosis drug.
- Mono-resistant tuberculosis (MR-TB) refers to tuberculosis that has resistance to only one anti-tuberculosis drug.
- Isoniazid-resistant tuberculosis (Hr-TB) refers to tuberculosis that has resistance to isoniazid but not concurrent resistance to rifampicin.
- Rifampicin-resistant tuberculosis (RR-TB) refers to tuberculosis that has resistance to rifampicin regardless of its sensitivity or resistance to other anti-tuberculosis drugs.
- Poly-resistant tuberculosis (PR-TB) refers to tuberculosis that has resistance to more than one kind of anti-tuberculosis drug, but not concurrent resistance to isoniazid and rifampicin.
- Multidrug-resistant tuberculosis (MDR-TB) refers to tuberculosis that has simultaneous resistance to isoniazid and rifampicin, regardless of its resistance to other anti-tuberculosis drugs.
- Pre-extensive drug-resistant tuberculosis (Pre-XDR-TB) refers to MDR-TB that has resistance to any quinolone.
- Extensive drug resistant tuberculosis (XDR-TB) refers to MDR-TB that has resistance to any quinolone and at least one of the three injectable drugs including capreomycin, kanamycin, and amikacin [6]. The traditional definition of XDR-TB was still used in this study because linezolid and bedaquiline were unavailable clinically and phenotypic susceptibility testing was not carried out in our hospital.
2.4. Statistical Analysis
3. Results
3.1. The Overall Profiles of Drug Resistance
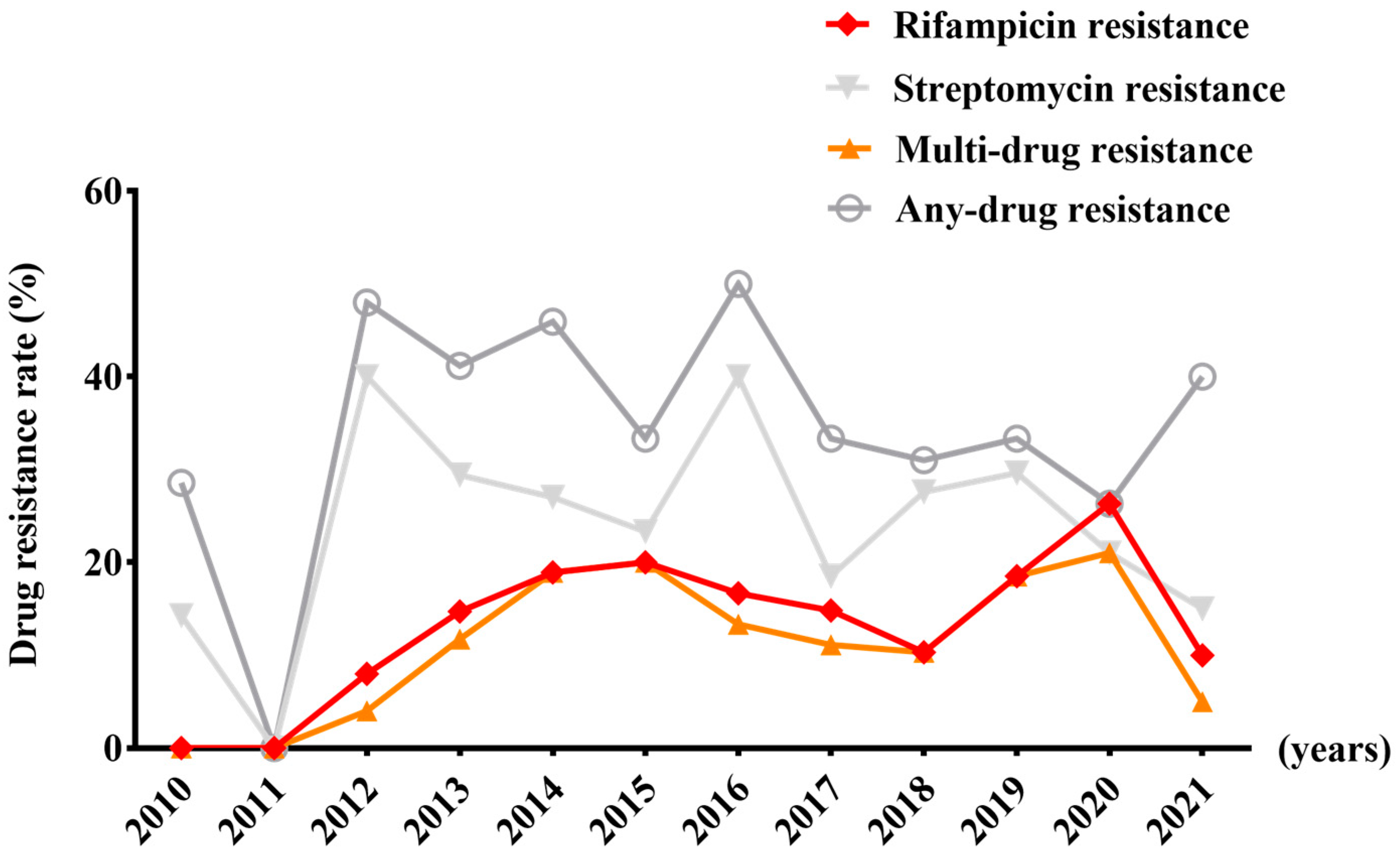
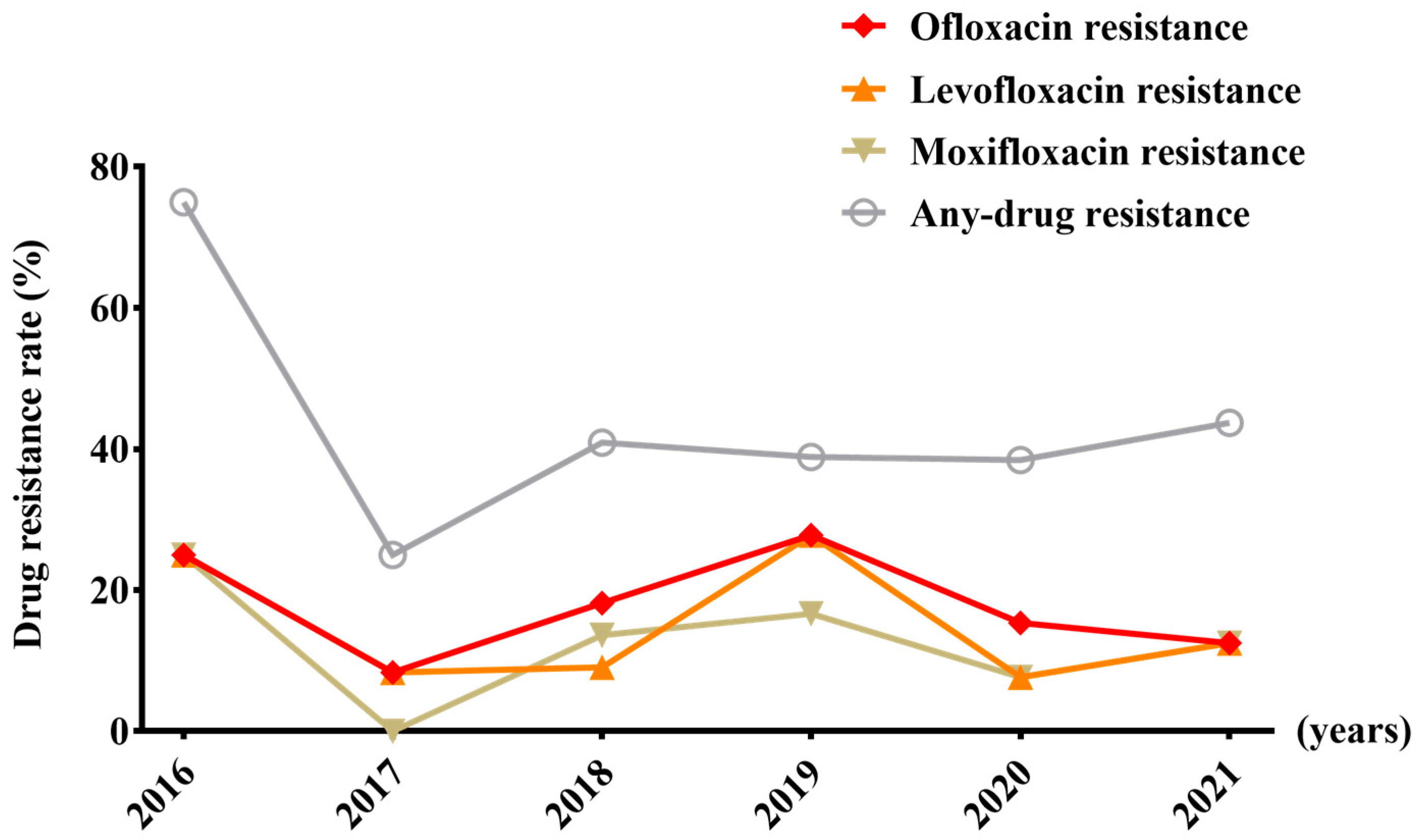
3.2. The Trends in Drug Resistance in M. tuberculosis to the First-Line and Second-Line Anti-Tuberculosis Drugs from 2010 to 2021
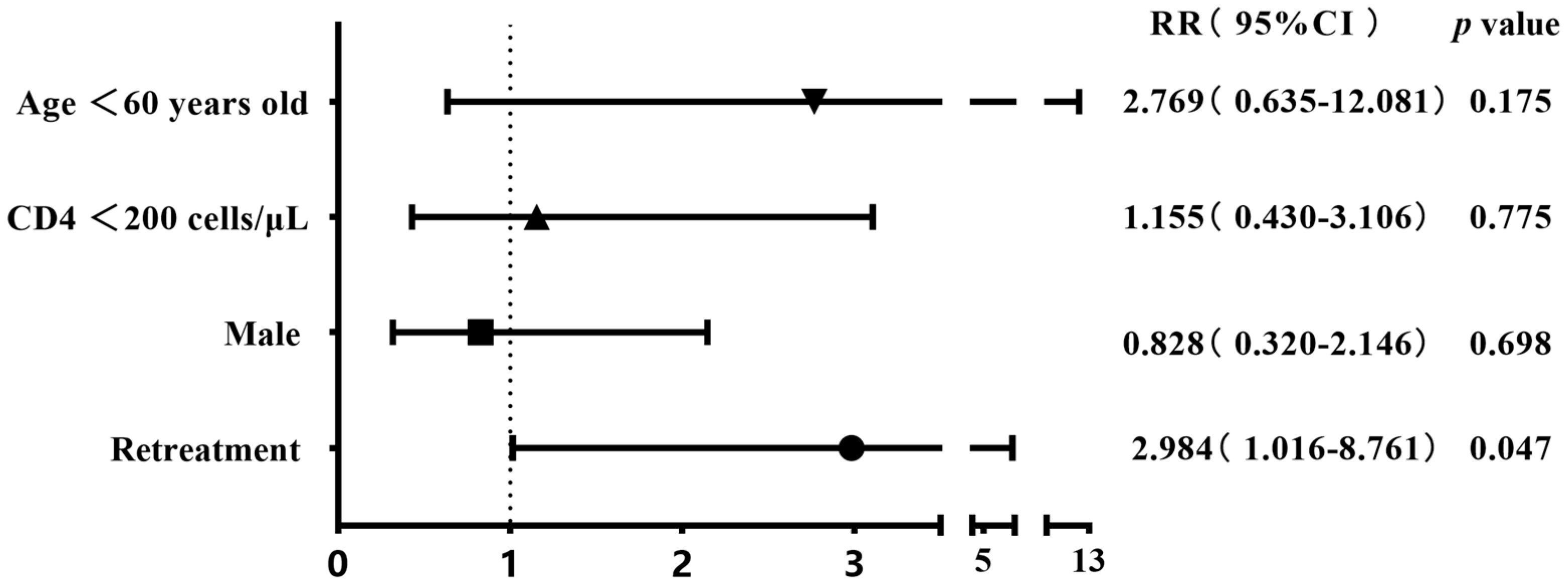
3.3. Comparison of Drug Resistance Rates between Different Groups and Risk Factor Analysis in the Group of 304 Cases
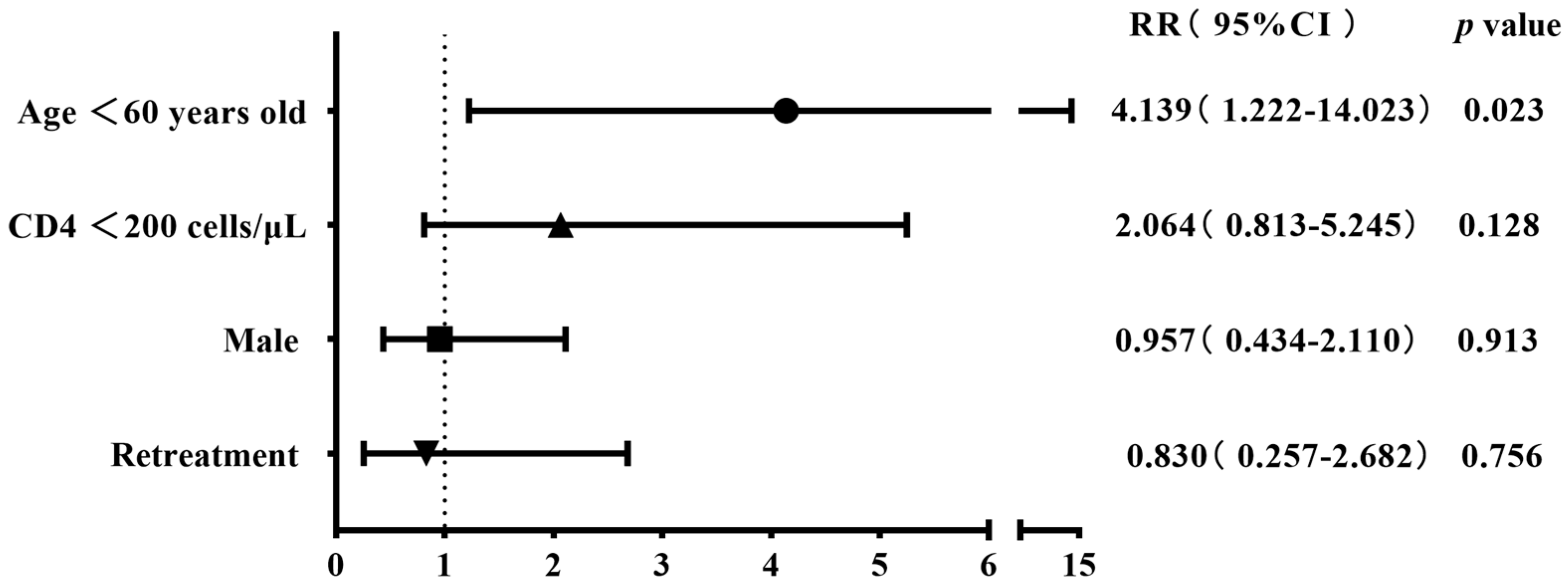
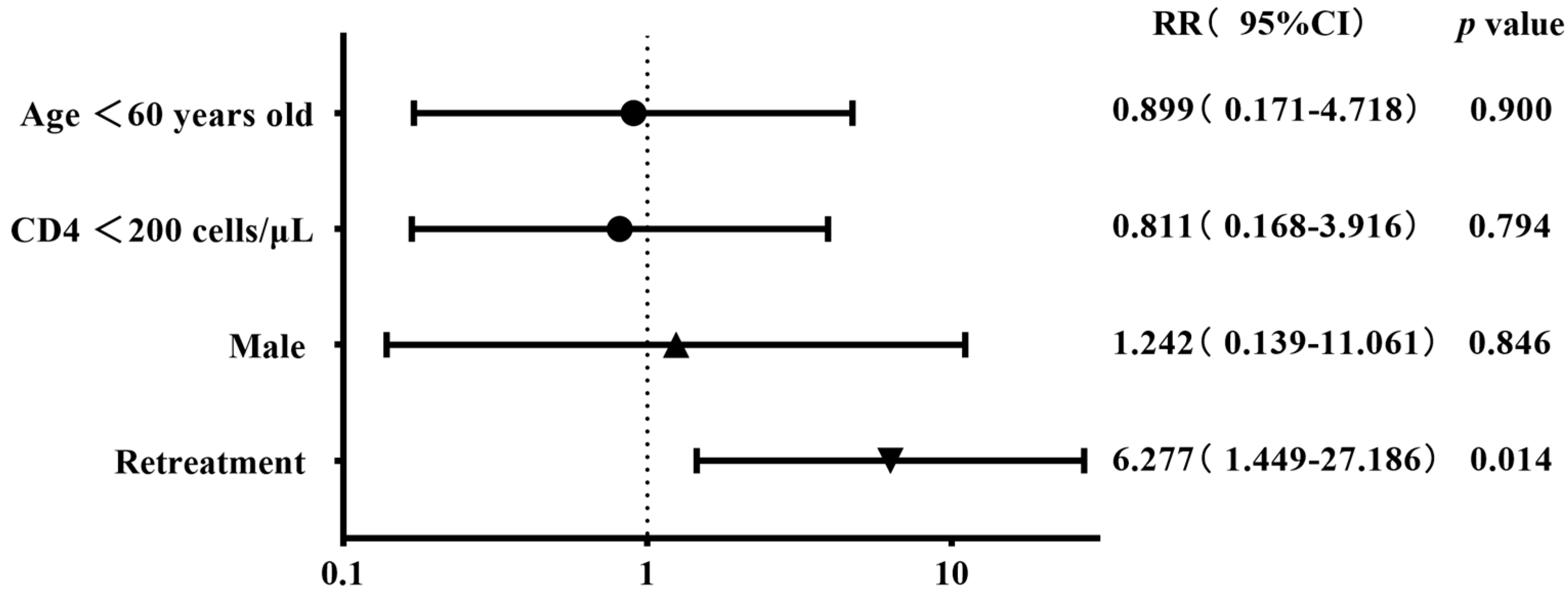
3.4. Comparison of Drug Resistance Rates between Different Groups and Risk Factor Analysis in the Group of 93 Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Professional Committee of HIV Combined with TB, Chinese Association of STD and AIDS Prevention and Control. Expert consensus on diagnosis and treatment of Mycobacterium tuberculosis infection in patients with human immunodeficiency virus infection/acquired immunodeficiency syndrome. Chin. J. Infect. Dis. 2022, 40, 6–19. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2023. Available online: https://www.who.int/publications/i/item/9789240083851 (accessed on 5 April 2024).
- UNAIDS. The Path That Ends AIDS: UNAIDS Global AIDS Update 2023. Available online: https://www.unaids.org/en/resources/documents/2023/global-aids-update-2023 (accessed on 5 April 2024).
- World Health Organization. Tuberculosis Profile: China. Available online: https://worldhealthorg.shinyapps.io/tb_profiles/?_inputs_&entity_type=%22country%22&iso2=%22CN%22&lan=%22EN%22 (accessed on 5 April 2024).
- Acquired Immunodeficiency Syndrome and Hepatitis C Professional Group; Society of Infectious Diseases; Chinese Medical Association; Chinese Center for Disease Control and Prevention. Chinese guidelines for diagnosis and treatment of human immunodeficiency virus/acquired immunodeficiency syndrome (2021 edition). Chin. J. Infect. Dis. 2021, 39, 715–735. [Google Scholar]
- Wang, L.X.; Cheng, S.M.; Zhou, L. Health profession Standards of the People’s Republic of China Classification of tuberculosis: WS 196—2017. Chin. J. Infect. Control 2018, 17, 367–368. [Google Scholar]
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis: Module 4: Treatment—Drug-Resistant Tuberculosis Treatment, 2022 Update. Available online: https://www.who.int/publications/i/item/9789240063129 (accessed on 5 April 2024).
- Zhao, Y.L.; Pang, Y. Tuberculosis Diagnostic Laboratory Test Procedures; China Education and Culture Press: Beijing, China, 2006; pp. 30–96. [Google Scholar]
- Dalielihan, G.; Song, Y.X.; Li, H.; Zhong, Y.X.; Wushouer, Q. Analysis of drug resistance of Mycobacterium tuberculosis in AIDS patients with tuberculosis. Infect. Dis. Info. 2022, 35, 245–247+258. [Google Scholar]
- Huang, A.C.; Lu, X.C.; Zhou, Z.J.; He, H.W.; Zhu, Q.D.; Zhou, M.; Lu, H.Z. Clinical features of AIDS-tuberculosis co-infection patients with positive Mycobacterium tuberculosis culture. Guangxi Med. J. 2018, 40, 1129–1131. [Google Scholar]
- Xu, Y.H.; Li, Q.F.; Zhu, M.; Wang, D.M.; Luo, J.; Li, Y.J.; Zhong, J. Characteristics and drug resistance analysis of Mycobacterium infection in HIV infection patients in Sichuan area. Chin. J. Nosocomiol. 2019, 29, 1624–1628. [Google Scholar]
- Chen, Y.Y.; Liu, X.H.; Wang, Y.L.; Hou, M.J.; Wang, Z.Y.; Yuan, H.Z.; Xin, N.B.; Zhao, Q.X. Initial drug resistance of mycobacterium tuberculosis in HIV patients with tuberculosis in Henan. Chin. J. AIDS STD 2021, 27, 14–16. [Google Scholar]
- Zhao, Y.; Xu, S.; Wang, L.; Chin, D.P.; Wang, S.; Jiang, G.; Xia, H.; Zhou, Y.; Li, Q.; Ou, X.; et al. National survey of drug-resistant tuberculosis in China. N. Engl. J. Med. 2012, 366, 2161–2170. [Google Scholar] [CrossRef] [PubMed]
- Sultana, Z.Z.; Hoque, F.U.; Beyene, J.; Akhlak-Ul-Islam, M.; Khan, M.H.R.; Ahmed, S.; Hawlader, D.H.; Hossain, A. HIV infection and multidrug resistant tuberculosis: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 51. [Google Scholar]
- Mesfin, Y.M.; Hailemariam, D.; Biadgilign, S.; Kibret, K.T. Association between HIV/AIDS and multi-drug resistance tuberculosis: A systematic review and meta-analysis. PLoS ONE 2014, 9, e82235. [Google Scholar] [CrossRef] [PubMed]
- Khan, P.Y.; Yates, T.A.; Osman, M.; Warren, R.M.; van der Heijden, Y.; Padayatchi, N.; Nardell, E.A.; Moore, D.; Mathema, B.; Gandhi, N.; et al. Transmission of drug-resistant tuberculosis in HIV-endemic settings. Lancet Infect. Dis. 2019, 19, e77–e88. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Prasad, R.; Balasubramanian, V.; Gupta, N. Drug-Resistant Tuberculosis and HIV Infection: Current Perspectives. HIV AIDS 2020, 12, 9–31. [Google Scholar] [CrossRef] [PubMed]
- van Rie, A.; Victor, T.C.; Richardson, M.; Johnson, R.; van der Spuy, G.D.; Murray, E.J.; Beyers, N.; Gey van Pittius, N.C.; van Helden, P.D.; Warren, R.M. Reinfection and mixed infection cause changing Mycobacterium tuberculosis drug-resistance patterns. Am. J. Respir. Crit. Care Med. 2005, 172, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Pizzol, D.; Cebola, B.; Stubbs, B.; Monno, L.; Saracino, A.; Luchini, C.; Solmi, M.; Segafredo, G.; Putoto, G.; et al. Social determinants of therapy failure and multi drug resistance among people with tuberculosis: A review. Tuberculosis 2017, 103, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Deutschendorf, C.; Goldani, L.Z.; Santos, R.P. Previous use of quinolones: A surrogate marker for first line anti-tuberculosis drugs resistance in HIV-infected patients? Braz. J. Infect. Dis. 2012, 16, 142–145. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with First-Line Drug Susceptibility Results (n = 304) | Patients with First-Line and Second-Line Drug Susceptibility Results (n = 93) | |
|---|---|---|
| Age ≥ 60 years old, n (%) | 33 (10.9) | 14 (15.1) |
| Male, n (%) | 267 (87.8) | 84 (90.3) |
| CD4 T cell counts ≥ 200 cells/μL, n (%) | 38 (12.5) | 12 (12.9) |
| Initial treatment, n (%) | 286 (94.1) | 83 (89.2) |
| Isoniazid resistance, n (%) | 35 (11.5) | 9 (9.7) |
| Rifampicin resistance, n (%) | 46 (15.1) | 20 (21.5) |
| Ethambutol resistance, n (%) | 38 (12.5) | 10 (10.8) |
| Streptomycin resistance, n (%) | 81 (26.6) | 27 (29) |
| Kanamycin resistance, n (%) | / | 4 (4.3) |
| Capreomycin resistance, n (%) | / | 5 (5.4) |
| Para-aminosalicylic acid resistance, n (%) | / | 7 (7.5) |
| Protionamide resistance, n (%) | / | 6 (6.5) |
| Amikacin resistance, n (%) | / | 4 (4.3) |
| Ofloxacin resistance, n (%) | / | 19 (20.4) |
| Levofloxacin resistance, n (%) | / | 16 (17.2) |
| Moxifloxacin resistance, n (%) | / | 14 (15.1) |
| XDR-TB, n (%) | / | 5 (5.4) |
| Pre-XDR-TB, n (%) | / | 14 (15.1) |
| MDR-TB, n (%) | 40 (13.2) | 17 (18.3) |
| PR-TB, n (%) | 20 (6.6) | 11 (11.8) |
| MR-TB, n (%) | 54 (17.8) | 12 (12.9) |
| DR-TB, n (%) | 114 (37.5) | 40 (43.0) |
| Gender | Age | CD4 T Cell Count (Cells/μL) | Treatment History | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | χ2 | p Value | ≥60 years old | <60 years old | χ2 | p-Value | ≥200 | <200 | χ2 | p-Value | Initial Treatment | Retreatment | χ2 | p-Value | |
| (n = 267) | (n = 37) | (n = 33) | (n = 271) | (n = 38) | (n = 266) | (n = 286) | (n = 18) | |||||||||
| Isoniazid resistance rate | 12.40% | 5.40% | 0.94 | 0.333 | 9.10% | 11.80% | 0.03 | 0.863 | 13.20% | 11.30% | 0.005 | 0.946 | 11.90% | 5.60% | 0.2 | 0.663 |
| Rifampicin resistance rate | 15.00% | 16.20% | 0.04 | 0.844 | 6.10% | 16.20% | 1.646 | 0.2 | 15.80% | 15.00% | 0.015 | 0.904 | 14.00% | 33.30% | 3.5 | 0.06 |
| Streptomycin resistance rate | 26.60% | 27.00% | 0 | 0.955 | 9.10% | 28.80% | 5.836 | 0.016 | 15.80% | 28.20% | 2.618 | 0.106 | 26.90% | 22.20% | 0 | 0.871 |
| Ethambutol resistance rate | 11.60% | 18.90% | 0.99 | 0.32 | 9.10% | 12.90% | 0.121 | 0.728 | 13.20% | 12.40% | 0 | 1 | 12.60% | 11.10% | 0 | 1 |
| Prevalence of MDR-TB | 12.70% | 16.20% | 0.11 | 0.743 | 6.10% | 14.00% | 1.009 | 0.315 | 10.50% | 13.50% | 0.263 | 0.608 | 12.60% | 22.20% | 0.7 | 0.416 |
| Prevalence of PR-TB | 7.10% | 2.70% | 0.44 | 0.509 | 6.10% | 6.60% | 0 | 1 | 7.90% | 6.40% | 0 | 1 | 7.00% | 0.00% | 0.5 | 0.502 |
| Prevalence of MR-TB | 18.40% | 13.50% | 0.52 | 0.47 | 3.00% | 19.60% | 5.501 | 0.019 | 13.20% | 18.40% | 0.631 | 0.427 | 17.80% | 16.70% | 0 | 1 |
| Prevalence of DR-TB | 38.20% | 32.40% | 0.46 | 0.497 | 15.20% | 40.20% | 7.889 | 0.005 | 31.60% | 38.30% | 0.65 | 0.42 | 37.40% | 38.90% | 0.2 | 0.9 |
| Gender | Age | CD4 T Cell Count (Cells/μL) | Condition of Treatment | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 84) | Female (n = 9) | χ2 | p-Value | ≥60 Years Old (n = 14) | <60 Years Old (n = 79) | χ2 | p-Value | ≥200 (n = 12) | <200 (n = 81) | χ2 | p-Value | Initial treatment (n = 83) | Retreatment (n = 10) | χ2 | p-Value | |
| Isoniazid resistance rate | 9.5% | 11.1% | - | 1 | 7.1% | 10.1% | 0 | 1 | 8.3% | 9.9% | 0 | 1 | 9.6% | 10% | - | 1 |
| Rifampicin resistance rate | 22.6% | 11.1% | 0.138 | 0.71 | 7.1% | 24.1% | 1.137 | 0.286 | 25.0% | 21.0% | 0 | 1 | 18.1% | 50% | 3.66 | 0.056 |
| Streptomycin resistance rate | 10.7% | 11.1% | - | 1 | 7.1% | 11.4% | 0 | 0.996 | 16.7% | 9.9% | 0.044 | 0.834 | 27.7% | 40% | 0.21 | 0.646 |
| Ethambutol resistance rate | 29.8% | 22.2% | 0.008 | 0.93 | 7.1% | 32.9% | 2.684 | 0.101 | 25.0% | 29.6% | 0 | 1 | 27.7% | 40% | 0.19 | 0.66 |
| Kanamycin resistance rate | 4.8% | 0.0% | - | 1 | 0.0% | 15.1% | - | 1 | 8.3% | 3.7% | - | 0.43 | 1.2% | 30% | - | 0.003 |
| Capreomycin resistance rate | 4.8% | 11.1% | - | 0.406 | 0.0% | 6.3% | - | 1 | 8.3% | 4.9% | - | 0.507 | 4.8% | 10% | - | 0.441 |
| Para-aminosalicylic acid resistance rate | 6.0% | 22.2% | - | 0.136 | 7.1% | 7.6% | 0 | 1 | 8.3% | 7.4% | - | 1 | 6.0% | 20% | - | 0.163 |
| Protionamide resistance rate | 7.1% | 0.0% | - | 1 | 0.0% | 7.6% | - | 0.586 | 16.7% | 4.9% | - | 0.171 | 3.6% | 30% | - | 0.015 |
| Amikacin resistance rate | 4.8% | 0.0% | - | 1 | 0.0% | 5.1% | - | 1 | 8.3% | 3.7% | - | 0.43 | 2.4% | 20% | - | 0.056 |
| Ofloxacin resistance rate | 21.4% | 11.1% | 0.087 | 0.768 | 14.3% | 21.5% | 0.067 | 0.796 | 25.0% | 19.8% | 0.001 | 0.97 | 16.9% | 50% | 4.16 | 0.041 |
| Levofloxacin resistance rate | 17.9% | 11.1% | 0.002 | 0.964 | 14.3% | 17.7% | 0 | 1 | 25.0% | 16.0% | 0.127 | 0.721 | 13.3% | 50% | 6.08 | 0.014 |
| Moxifloxacin resistance rate | 16.7% | 0.0% | 0.703 | 0.402 | 7.1% | 16.5% | 0.243 | 0.622 | 16.7% | 14.8% | 0 | 1 | 13.3% | 30% | 0.87 | 0.352 |
| Prevalence of MDR-TB | 19.0% | 11.1% | 0.017 | 0.895 | 7.1% | 20.3% | 0.631 | 0.427 | 16.7% | 18.5% | 0 | 1 | 15.7% | 40% | 2.1 | 0.148 |
| Prevalence of PR-TB | 11.9% | 11.1% | - | 0.944 | 7.1% | 12.7% | - | 1 | 16.7% | 11.1% | - | 0.63 | 10.8% | 20% | - | 0.336 |
| Prevalence of MR-TB | 13.1% | 11.1% | 0 | 1 | 7.1% | 13.9% | 0.07 | 0.791 | 0.0% | 14.8% | 0.936 | 0.333 | 14.5% | 0% | - | 0.35 |
| Prevalence of DR-TB | 44.0% | 33.3% | - | 0.727 | 21.4% | 46.8% | 3.132 | 0.077 | 33.3% | 44.4% | 0.526 | 0.468 | 41.0% | 60% | - | 0.318 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, X.; Qian, X.; Liu, L.; Sun, J.; Song, W.; Qi, T.; Wang, Z.; Tang, Y.; Xu, S.; Yang, J.; et al. Trends in and Risk Factors for Drug Resistance in Mycobacterium tuberculosis in HIV-Infected Patients. Viruses 2024, 16, 627. https://doi.org/10.3390/v16040627
Le X, Qian X, Liu L, Sun J, Song W, Qi T, Wang Z, Tang Y, Xu S, Yang J, et al. Trends in and Risk Factors for Drug Resistance in Mycobacterium tuberculosis in HIV-Infected Patients. Viruses. 2024; 16(4):627. https://doi.org/10.3390/v16040627
Chicago/Turabian StyleLe, Xiaoqin, Xueqin Qian, Li Liu, Jianjun Sun, Wei Song, Tangkai Qi, Zhenyan Wang, Yang Tang, Shuibao Xu, Junyang Yang, and et al. 2024. "Trends in and Risk Factors for Drug Resistance in Mycobacterium tuberculosis in HIV-Infected Patients" Viruses 16, no. 4: 627. https://doi.org/10.3390/v16040627