Vascular Endothelial Growth Factor Levels in Dobrava/Belgrade Virus Infections


Abstract
:1. Introduction
2. Results and Discussion
2.1. Grouping of HFRS Cases
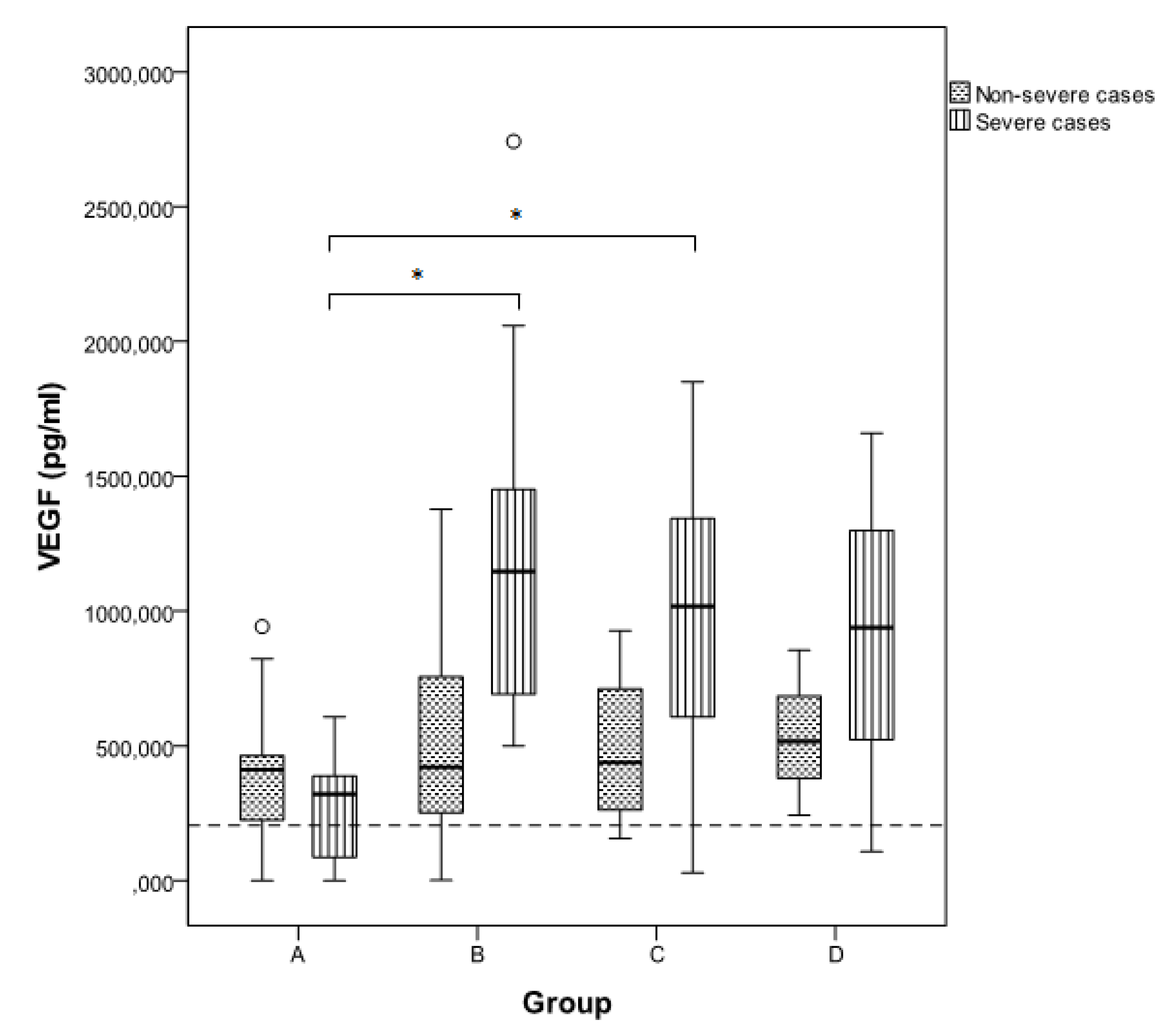
2.2. Estimation of VEGF Levels

{kind=link}
| Group (n) | Severe | Non severe | p-value | ||||
|---|---|---|---|---|---|---|---|
| N | Range | Mean (SD) | N | Range | Mean (SD) | ||
| A (24) | 11 | 0.00–607.23 | 267.16 (201.11) | 13 | 0.00–942.44 | 391.06 (303.67) | 0.338 |
| B (43) | 22 | 499.53–2742.00 | 1159.64 (582.47) | 21 | 1.07–1378.00 | 514.89 (383.59) | <0.001 |
| C (23) | 10 | 28.76–1850.30 | 977.37 (528.65) | 13 | 156.46–927.23 | 508.74 (280.28) | 0.026 |
| D (6) | 3 | 107.20–1660.00 | 901.73 (777.03) | 3 | 242.44–854.00 | 537.48 (306.34) | 0.513 |
| E (6) | 5 | 90.30–1742.00 | 504.07 (694.68) | 1 | 382.00 | 382.00 | 0.380 |
| Total (102) | 51 | 0.00–2742.00 | 851.96 (629.23) | 51 | 0.00–1378.00 | 480.48 (326.75) | 0.003 |

| Patient ID | Age | Sex | ICU/hemorrhagic manifestations/pulmonary involvement/dialysis | Group A (1st week) | Group B (2nd week) | Group C (3rd week) | Group D (4th week) | Group E (>4th week) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Day | VEGF (pg/mL) | Day | VEGF (pg/mL) | Day | VEGF (pg/mL) | Day | VEGF (pg/mL) | Day | VEGF (pg/mL) | ||||
| A. Severe cases | |||||||||||||
| 167/05 | 29 | M | ICU, dialysis | 5 | 0.00 | 17 | 1545.69 | ||||||
| 108/07 | 23 | F | ICU, hemorrhages, pulmonary edema | 7 | 359.53 | 12 | 1678.00 | ||||||
| 53/10 | 51 | F | hemodialysis | 9 | 771.43 | 16 | 1100.00 | 35 70 | 234.29 90.30 | ||||
| 102/04 | 40 | M | pulmonary infiltrations, hematuria, dialysis | 10 | 508.14 | 27 | 107.20 | ||||||
| 184/05 | 44 | M | dialysis, hematuria | 8 11 13 | 2742.00 2058.57 1910.00 | ||||||||
| 188/06 | 38 | M | dialysis, hematuria | 12 | 1050.30 | 17 | 607.23 | ||||||
| 79/02 | 28 | M | petechiae, hemoptysis | 6 | 342.00 | 8 | 634.00 | ||||||
| 43/02 | 27 | M | dialysis | 9 | 534.00 | 15 | 1014.00 | ||||||
| 38/02 | 35 | M | ARDS, sepsis, dialysis, hemorrhages | 22 | 1660.00 | 33 | 1742.00 | ||||||
| 385/01 | 20 | M | hematuria | 10 | 708 | 21 | 262 | ||||||
| 162/98 | 59 | M | hematuria | 7 | 0 | 13 | 1242.44 | ||||||
| 85/97 | 70 | M | sepsis | 7 | 415.77 | 10 | 1029.11 | ||||||
| 100/97 | 38 | M | ICU, fatal | 13 | 1291.33 | 16 | 1020.22 | 22 | 938.00 | ||||
| 62/02 | 36 | M | Pulmonary involvement, dialysis, DIC | 8 9 10 | 1318,00 1289.11 1344.66 | ||||||||
| 177/06 | 31 | M | ARDS | 11 | 1480.22 | 17 | 1342.44 | ||||||
| B. Non-severe cases | |||||||||||||
| 58/10 | 40 | M | 6 | 743.84 | 15 | 491.84 | |||||||
| 116/07 | 33 | F | 7 | 27.23 | 15 | 278.00 | |||||||
| 159/07 | 21 | M | 7 | 0.00 | 15 | 824.66 | |||||||
| 196/07 | 35 | M | 7 | 262.86 | 12 | 490.00 | |||||||
| 236/05 | 22 | M | 8 11 | 1236.46 376.46 | |||||||||
| 62/10 | 29 | M | 7 | 413.38 | 11 | 242.44 | 26 | 1.07 | |||||
| 240/04 | 32 | M | 8 11 | 962.61 1062.61 | |||||||||
| 66/03 | 49 | M | 10 | 48.00 | 16 | 156.46 | |||||||
| 252/04 | 38 | F | 16 18 | 927.23 913.55 | |||||||||
| 18/02 | 19 | M | 17 | 626.00 | 25 | 516.00 | |||||||
| 34/09 | 38 | M | 14 | 755.77 | 19 | 211.33 | |||||||
| 243/95 | 35 | F | 5 | 822.44 | 16 | 664.66 | |||||||
| 218/95 | 42 | M | 6 | 411.33 | 13 | 182,44 | |||||||
| 258/95 | 40 | M | 6 | 426.88 | 10 | 251.33 | |||||||
| 254/96 | 24 | M | 5 | 344.66 | 13 | 355,77 | |||||||
| 28/96 | M | 10 | 835.77 | 17 | 711.33 | ||||||||
| 278/00 | 21 | M | 16 | 438.00 | 22 | 854.00 | 30 | 382.00 | |||||
3. Experimental Section
3.1. ELISA
3.2. Statistical Analysis
4. Conclusions
Acknowledgments
Conflicts of Interest
References
- Papa, A. Crimean-Congo Hemorrhagic Fever and Hantavirus Infections. In Tropical and Emerging Infectious Diseases; Maltezou, H., Gikas, A., Eds.; Research Signpost: Kerala, India, 2010; pp. 49–73. [Google Scholar]
- Avsic-Zupanc, T.; Petrovec, M.; Furlan, P.; Kaps, R.; Elgh, F.; Lundkvist, A. Hemorrhagic fever with renal syndrome in the Dolenjska region of Slovenia -a 10-year survey. Clin. Infect. Dis. 1999, 28, 860–865. [Google Scholar]
- Papa, A.; Antoniadis, A. Hantavirus infections in Greece--an update. Eur. J. Epidemiol. 2001, 17, 189–194. [Google Scholar] [CrossRef]
- Antoniadis, A.; Stylianakis, A.; Papa, A.; Alexiou-Daniel, S.; Lampropoulos, A.; Nichol, S.T.; Peters, C.J.; Spiropoulou, C.F. Direct genetic detection of Dobrava virus in Greek and Albanian patients with hemorrhagic fever with renal syndrome. J. Infect. Dis. 1996, 174, 407–410. [Google Scholar] [CrossRef]
- Papa, A.; Johnson, A.M.; Stockton, P.C.; Bowen, M.D.; Spiropoulou, C.F.; Alexiou-Daniel, S.; Ksiazek, T.G.; Nichol, S.T.; Antoniadis, A. Retrospective serological and genetic study of the distribution of hantaviruses in Greece. J. Med. Virol. 1998, 55, 321–327. [Google Scholar] [CrossRef]
- Krautkramer, E.; Zeier, M.; Plyusnin, A. Hantavirus infection: An emerging infectious disease causing acute renal failure. Kidney Int. 2013, 83, 23–27. [Google Scholar] [CrossRef]
- Papa, A. Dobrava-Belgrade virus: Phylogeny, epidemiology, disease. Antivir. Res. 2012, 95, 104–117. [Google Scholar] [CrossRef]
- Klempa, B.; Avsic-Zupanc, T.; Clement, J.; Dzagurova, T.K.; Henttonen, H.; Heyman, P.; Jakab, F.; Kruger, D.H.; Maes, P.; Papa, A.; et al. Complex evolution and epidemiology of Dobrava-Belgrade hantavirus: Definition of genotypes and their characteristics. Arch. Virol. 2012, 158, 521–529. [Google Scholar]
- Fukasawa, H.; Bornheimer, S.; Kudlicka, K.; Farquhar, M.G. Slit diaphragms contain tight junction proteins. J. Am. Soc. Nephrol. 2009, 20, 1491–1503. [Google Scholar] [CrossRef]
- Reiser, J.; Kriz, W.; Kretzler, M.; Mundel, P. The glomerular slit diaphragm is a modified adherens junction. J. Am. Soc. Nephrol. 2000, 11, 1–8. [Google Scholar]
- Schonrich, G.; Rang, A.; Lutteke, N.; Raftery, M.J.; Charbonnel, N.; Ulrich, R.G. Hantavirus-induced immunity in rodent reservoirs and humans. Immunol. Rev. 2008, 225, 163–189. [Google Scholar] [CrossRef]
- Bates, D.O. Vascular endothelial growth factors and vascular permeability. Cardiovasc. Res. 2010, 87, 262–271. [Google Scholar] [CrossRef]
- Gavrilovskaya, I.N.; Brown, E.J.; Ginsberg, M.H.; Mackow, E.R. Cellular entry of hantaviruses which cause hemorrhagic fever with renal syndrome is mediated by beta3 integrins. J. Virol. 1999, 73, 3951–3959. [Google Scholar]
- Raymond, T.; Gorbunova, E.; Gavrilovskaya, I.N.; Mackow, E.R. Pathogenic hantaviruses bind plexin-semaphorin-integrin domains present at the apex of inactive, bent alphavbeta3 integrin conformers. Proc. Natl. Acad. Sci. USA 2005, 102, 1163–1168. [Google Scholar] [CrossRef]
- Krautkramer, E.; Grouls, S.; Stein, N.; Reiser, J.; Zeier, M. Pathogenic old world hantaviruses infect renal glomerular and tubular cells and induce disassembling of cell-to-cell contacts. J. Virol. 2011, 85, 9811–9823. [Google Scholar] [CrossRef]
- Gavrilovskaya, I.N.; Gorbunova, E.E.; Mackow, N.A.; Mackow, E.R. Hantaviruses direct endothelial cell permeability by sensitizing cells to the vascular permeability factor VEGF, while angiopoietin 1 and sphingosine 1-phosphate inhibit hantavirus-directed permeability. J. Virol. 2008, 82, 5797–5806. [Google Scholar] [CrossRef]
- Gorbunova, E.E.; Gavrilovskaya, I.N.; Pepini, T.; Mackow, E.R. VEGFR2 and Src kinase inhibitors suppress Andes virus-induced endothelial cell permeability. J. Virol. 2011, 85, 2296–2303. [Google Scholar] [CrossRef]
- Tseng, C.S.; Lo, H.W.; Teng, H.C.; Lo, W.C.; Ker, C.G. Elevated levels of plasma VEGF in patients with dengue hemorrhagic fever. FEMS Immunol. Med. Microbiol. 2005, 43, 99–102. [Google Scholar] [CrossRef]
- Taylor, S.L.; Wahl-Jensen, V.; Copeland, A.M.; Jahrling, P.B.; Schmaljohn, C.S. Endothelial cell permeability during hantavirus infection involves factor XII-dependent increased activation of the kallikrein-kinin system. PLoS Pathog. 2013, 9, e1003470. [Google Scholar] [CrossRef]
- Ma, Y.; Liu, B.; Yuan, B.; Wang, J.; Yu, H.; Zhang, Y.; Xu, Z.; Yi, J.; Zhang, C.; Zhou, X.; et al. Sustained high level of serum VEGF at convalescent stage contributes to the renal recovery after HTNV Infection in patients with hemorrhagic fever with renal syndrome. Clin. Dev. Immunol. 2012, 2012, 812386. [Google Scholar]
- Li, Y.; Wang, W.; Wang, J.P.; Pan, L.; Zhang, Y.; Yu, H.T.; Jiang, W.; Wang, P.Z.; Bai, X.F. Elevated vascular endothelial growth factor levels induce hyperpermeability of endothelial cells in hantavirus infection. J. Int. Med. Res. 2012, 40, 1812–1821. [Google Scholar] [CrossRef]
- Gavrilovskaya, I.; Gorbunova, E.; Koster, F.; Mackow, E. Elevated VEGF levels in pulmonary edema fluid and PBMCs from patients with acute hantavirus pulmonary syndrome. Adv. Virol. 2012, 2012, 674360. [Google Scholar]
- Gorbunova, E.; Gavrilovskaya, I.N.; Mackow, E.R. Pathogenic hantaviruses Andes virus and Hantaan virus induce adherens junction disassembly by directing vascular endothelial cadherin internalization in human endothelial cells. J. Virol. 2010, 84, 7405–7411. [Google Scholar] [CrossRef]
- Shrivastava-Ranjan, P.; Rollin, P.E.; Spiropoulou, C.F. Andes virus disrupts the endothelial cell barrier by induction of vascular endothelial growth factor and downregulation of VE-cadherin. J. Virol. 2010, 84, 11227–11234. [Google Scholar] [CrossRef]
- Safronetz, D.; Zivcec, M.; Lacasse, R.; Feldmann, F.; Rosenke, R.; Long, D.; Haddock, E.; Brining, D.; Gardner, D.; Feldmann, H.; et al. Pathogenesis and host response in Syrian hamsters following intranasal infection with Andes virus. PLoS Pathog. 2011, 7, e1002426. [Google Scholar] [CrossRef]
- Spengler, J.R.; Haddock, E.; Gardner, D.; Hjelle, B.; Feldmann, H.; Prescott, J. Experimental Andes virus infection in deer mice: Characteristics of infection and clearance in a heterologous rodent host. PLoS One 2013, 8, e55310. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tsergouli, K.; Papa, A. Vascular Endothelial Growth Factor Levels in Dobrava/Belgrade Virus Infections. Viruses 2013, 5, 3109-3118. https://doi.org/10.3390/v5123109
Tsergouli K, Papa A. Vascular Endothelial Growth Factor Levels in Dobrava/Belgrade Virus Infections. Viruses. 2013; 5(12):3109-3118. https://doi.org/10.3390/v5123109
Chicago/Turabian StyleTsergouli, Katerina, and Anna Papa. 2013. "Vascular Endothelial Growth Factor Levels in Dobrava/Belgrade Virus Infections" Viruses 5, no. 12: 3109-3118. https://doi.org/10.3390/v5123109