
Concept for a Unidirectional Release Mucoadhesive Buccal Tablet for Oral Delivery of Antidiabetic Peptide Drugs Such as Insulin, Glucagon-like Peptide 1 (GLP-1), and their Analogs


Abstract
:1. Introduction
2. Peptides for Treating Diabetes
3. Nanoparticles’ Preparation
3.1. Lipid-Based NPs
3.2. Polymer-Based NPs
4. Drying Procedure to Form Dry Powders

{kind=link}
{kind=link}
{kind=link}
| GLP-1 | Drying Techniques | Drying Parameters | Additives | Ref. |
|---|---|---|---|---|
| Human insulin | Freeze | NA | NA | [88] |
| Linagliptin and empagliflozin | Vacuum | 60 °C and 5 mbar | Pluronic F68, Pluronic F-127, fluorophore umbelliferon and eosine | [113] |
| l-Cysteine | Freeze | −30 °C at 0.01 mbar | NA | [33] |
| D,l-valine | Vacuum | 25 °C and 1000 mbar | Eudragit (ERL) and hydroxypropyl methylcellulose (HPMC) | [102] |
| Human insulin | Freeze | NA | NA | [114] |
| Human insulin | Freeze | −60 °C and 0.09 mbar | 10% w/w fructose, trehalose, or glucose | [107] |
| Human insulin | Spray | 100 °C, feeding flow of 3 L/min, and airflow of 4 L/min | Mannitol (1% w/w) | [18] |
| Human insulin | Freeze | 0 °C at 0.133 mbar | NA | [115] |
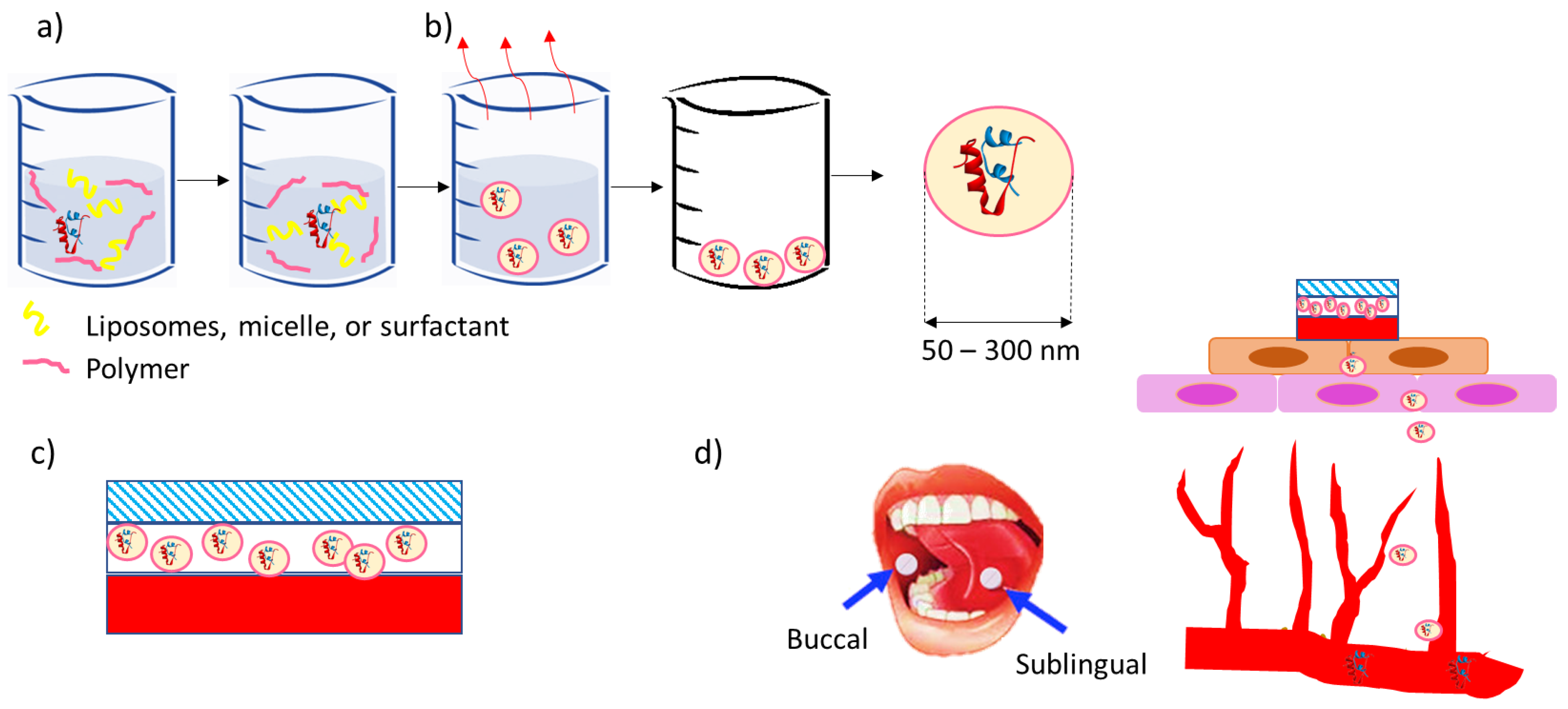
5. Concept for Buccal Tablets for the Buccal Delivery of Nanoparticles Containing Insulin, GLP-1, and their Analogs
- Single-layer devices from which the drug is released multidirectionally;
- Devices including an upper water-resistant layer that reduces the wastage of the drug into the oral cavity and avoids the degradation of drug by salivary enzymes;
- Unidirectional release devices, from which drug loss is low since the drug is released only from one side, facing the buccal mucosa [35].
6. Conclusions and Future Developments
7. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alam, S.; Hasan, K.; Neaz, S.; Hussain, N.; Hossain, F.; Rahman, T. Diabetes Mellitus: Insights from epidemiology, biochemistry, risk factors, diagnosis, complications and comprehensive management. Diabetology 2021, 2, 36–50. [Google Scholar] [CrossRef]
- Riobó Serván, P. Obesidad y diabetes. Nutr. Hosp. 2013, 28, 138–143. [Google Scholar]
- Gurav, A.N. The association of periodontitis and metabolic syndrome. Dent. Res. J. 2014, 11, 1. [Google Scholar]
- Dwivedi, M.; Pandey, A.R. Diabetes mellitus and its treatment: An overview. J. Adv. Pharmacol. 2020, 1, 48–58. [Google Scholar]
- Kaku, K.; Yamamoto, K.; Fukushima, Y.; Lliev, H.; Yasui, A. Safety and effectiveness of empagliflozin in Japanese patients with type 2 diabetes: Final results of a 3-year post-marketing surveillance study. Expert Opin. Drug Saf. 2022, 21, 1315–1328. [Google Scholar] [CrossRef] [PubMed]
- Eizirik, D.L.; Colli, M.L.; Ortis, F. The role of inflammation in insulitis and β-cell loss in type 1 diabetes. Nat. Rev. Endocrinol. 2009, 5, 219–226. [Google Scholar] [CrossRef]
- Thomas, N.J.; Jones, S.E.; Weedon, M.N.; Shields, B.M.; Oram, R.A.; Hattersley, A.T. Frequency and phenotype of type 1 diabetes in the first six decades of life: A cross-sectional, genetically stratified survival analysis from UK Biobank. Lancet Diabetes Endocrinol. 2018, 6, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, A.; Gudbjörnsdottir, S.; Rawshani, A.; Dabelea, D.; Bonifacio, E.; Anderson, B.J.; Jacobsen, L.M.; Schatz, D.A.; Lernmark, Å. Type 1 diabetes mellitus. Nat. Rev. Dis. Primers 2017, 3, 17016. [Google Scholar] [CrossRef]
- Virally, M.; Blicklé, J.-F.; Girard, J.; Halimi, S.; Simon, D.; Guillausseau, P.-J. Type 2 diabetes mellitus: Epidemiology, pathophysiology, unmet needs and therapeutical perspectives. Diabetes Metab. 2007, 33, 231–244. [Google Scholar] [CrossRef]
- Kemp, D.M. Type 2 Diabetes: Disease Overview. New Ther. Strateg. Type 2012, 2, 1–14. [Google Scholar]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.; Kriska, A. Role of physical activity in diabetes management and prevention. J. Am. Diet. Assoc. 2008, 108, S19–S23. [Google Scholar] [CrossRef] [PubMed]
- Chaudhury, A.; Duvoor, C.; Reddy Dendi, V.S.; Kraleti, S.; Chada, A.; Ravilla, R.; Marco, A.; Shekhawat, N.S.; Montales, M.T.; Kuriakose, K. Clinical review of antidiabetic drugs: Implications for type 2 diabetes mellitus management. Front. Endocrinol. 2017, 8, 6. [Google Scholar] [CrossRef]
- McMurray, S.D.; Johnson, G.; Davis, S.; McDougall, K. Diabetes education and care management significantly improve patient outcomes in the dialysis unit. Am. J. Kidney Dis. 2002, 40, 566–575. [Google Scholar] [CrossRef]
- Nelson, K.M.; Reiber, G.; Boyko, E.J. Diet and exercise among adults with type 2 diabetes: Findings from the third national health and nutrition examination survey (NHANES III). Diabetes Care 2002, 25, 1722–1728. [Google Scholar] [CrossRef]
- Krishnamoorthi, R.; Joshi, S.; Almarzouki, H.Z.; Shukla, P.K.; Rizwan, A.; Kalpana, C.; Tiwari, B. A novel diabetes healthcare disease prediction framework using machine learning techniques. J. Healthc. Eng. 2022, 2022, 1684017. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.P.; Guo, Y.; Singh, A.; Xie, W.; Jiang, P. Developments in encapsulation of insulin: Is oral delivery now possible? J. Pharm. Biopharm. Res. 2019, 1, 74–92. [Google Scholar] [CrossRef]
- Guo, Y.; Baldelli, A.; Singh, A.; Fathordoobady, F.; Kitts, D.; Pratap-Singh, A. Production of high loading insulin nanoparticles suitable for oral delivery by spray drying and freeze drying techniques. Sci. Rep. 2022, 12, 9949. [Google Scholar] [CrossRef]
- Bolli, G.B.; Porcellati, F.; Meier, J.J. Switching from insulin bolus treatment to GLP-1 RAs added to continued basal insulin in people with type 2 diabetes on basal-bolus insulin. Diabetes Care 2020, 43, 2333–2335. [Google Scholar] [CrossRef]
- Rosenstock, J.; Reusch, J.; Bush, M.; Yang, F.; Stewart, M.; Group, A.S. Potential of albiglutide, a long-acting GLP-1 receptor agonist, in type 2 diabetes: A randomized controlled trial exploring weekly, biweekly, and monthly dosing. Diabetes Care 2009, 32, 1880–1886. [Google Scholar] [CrossRef]
- Rosenstock, J.; Wysham, C.; Frías, J.P.; Kaneko, S.; Lee, C.J.; Landó, L.F.; Mao, H.; Cui, X.; Karanikas, C.A.; Thieu, V.T. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): A double-blind, randomised, phase 3 trial. Lancet 2021, 398, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.L.; McEntee, N.; Holland, J.; Patel, A. Development and approval of rybelsus (oral semaglutide): Ushering in a new era in peptide delivery. Drug Deliv. Transl. Res. 2022, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kanugo, A.; Misra, A. New and novel approaches for enhancing the oral absorption and bioavailability of protein and peptides therapeutics. Ther. Deliv. 2020, 11, 713–732. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Kang, W.; Li, W.; Chen, S.; Gao, Y. Oral delivery of protein and peptide drugs: From non-specific formulation approaches to intestinal cell targeting strategies. Theranostics 2022, 12, 1419. [Google Scholar] [CrossRef]
- Morales, J.O.; Fathe, K.R.; Brunaugh, A.; Ferrati, S.; Li, S.; Montenegro-Nicolini, M.; Mousavikhamene, Z.; McConville, J.T.; Prausnitz, M.R.; Smyth, H.D. Challenges and future prospects for the delivery of biologics: Oral mucosal, pulmonary, and transdermal routes. AAPS J. 2017, 19, 652–668. [Google Scholar] [CrossRef]
- Bahman, F.; Taurin, S. Inhalation of insulin for diabetes management. Nanotechnol. Diabetes Manag. 2022, 59, 165. [Google Scholar]
- Kumbhar, K.P.; Suryawanshi, S.; Patil, S.V. Novel route of inhaled insulin for diabetes treatment. Asian J. Pharm. Technol. 2022, 12, 25–32. [Google Scholar] [CrossRef]
- Fonte, P.; Araújo, F.; Reis, S.; Sarmento, B. Oral insulin delivery: How far are we? J. Diabetes Sci. Technol. 2013, 7, 520–531. [Google Scholar] [CrossRef]
- Misra, A.; Jinturkar, K.; Patel, D.; Lalani, J.; Chougule, M. Recent advances in liposomal dry powder formulations: Preparation and evaluation. Expert Opin. Drug Deliv. 2009, 6, 71–89. [Google Scholar] [CrossRef]
- Ashique, S.; Khatun, T.; Upadhyay, A.; Verma, S.; Tyagi, S.; Iqbal, A.; Kayes, I. Micro-needles as an effective drug delivery system and associated patents in pharmaceutical field: A Review. Biol. Sci. 2021, 1, 53–66. [Google Scholar] [CrossRef]
- Gupta, A.; Pal, P. Micro-electro-mechanical system–based drug delivery devices. In Bioelectronics and Medical Devices; Elsevier: Amsterdam, The Netherlands, 2019; pp. 183–210. [Google Scholar]
- Kumria, R.; Goomber, G. Emerging trends in insulin delivery: Buccal route. J. Diabetol. 2011, 2, 1–9. [Google Scholar]
- Langoth, N.; Kalbe, J.; Bernkop-Schnürch, A. Development of buccal drug delivery systems based on a thiolated polymer. Int. J. Pharm. 2003, 252, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhang, X.; Zhang, Y.; Ye, J.; Wang, H.-L.; Xia, X.; Liu, Y. Mechanisms of deformable nanovesicles based on insulin-phospholipid complex for enhancing buccal delivery of insulin. Int. J. Nanomed. 2018, 13, 7319. [Google Scholar] [CrossRef] [PubMed]
- Şenel, S.; Rathbone, M.J.; Cansız, M.; Pather, I. Recent developments in buccal and sublingual delivery systems. Expert Opin. Drug Deliv. 2012, 9, 615–628. [Google Scholar] [CrossRef] [PubMed]
- Macedo, A.S.; Castro, P.M.; Roque, L.; Thomé, N.G.; Reis, C.P.; Pintado, M.E.; Fonte, P. Novel and revisited approaches in nanoparticle systems for buccal drug delivery. J. Control. Release 2020, 320, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.O.; Vuddanda, P.R.; Velaga, S. Controlled Drug Delivery via the Buccal and Sublingual Routes. In Fundamentals of Drug Delivery; Wiley: Hoboken, NJ, USA, 2021; pp. 433–448. [Google Scholar]
- Baldelli, A.; Liang, D.Y.; Guo, Y.; Pratap-Singh, A. Effect of the formulation on mucoadhesive spray-dried microparticles containing iron for food fortification. Food Hydrocoll. 2023, 134, 107906. [Google Scholar] [CrossRef]
- Advankar, A.; Maheshwari, R.; Tambe, V.; Todke, P.; Raval, N.; Kapoor, D.; Tekade, R.K. Chapter 13 Specialized tablets: Ancient history to modern developments. In Advances in Pharmaceutical Product Development and Research, Drug Delivery Systems; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 615–664. [Google Scholar]
- Suzuki, R.; Brown, G.A.; Christopher, J.A.; Scully, C.C.; Congreve, M. Recent developments in therapeutic peptides for the glucagon-like peptide 1 and 2 receptors. J. Med. Chem. 2019, 63, 905–927. [Google Scholar] [CrossRef]
- Lau, J.L.; Dunn, M.K. Therapeutic peptides: Historical perspectives, current development trends, and future directions. Bioorganic Med. Chem. 2018, 26, 2700–2707. [Google Scholar] [CrossRef]
- Kuo, T.; McQueen, A.; Chen, T.-C.; Wang, J.-C. Regulation of glucose homeostasis by glucocorticoids. In Glucocorticoid Signaling: From Molecules to Mice to Man; Springer: New York, NY, USA, 2015; pp. 99–126. [Google Scholar]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19. [Google Scholar]
- Al-Arouj, M.; Bouguerra, R.; Buse, J.; Hafez, S.; Hassanein, M.; Ibrahim, M.A.; Ismail-Beigi, F.; El-Kebbi, I.; Khatib, O.; Kishawi, S. Recommendations for management of diabetes during Ramadan. Diabetes Care 2005, 28, 2305–2311. [Google Scholar] [CrossRef]
- Peterson, G.E. Intermediate and long-acting insulins: A review of NPH insulin, insulin glargine and insulin detemir. Curr. Med. Res. Opin. 2006, 22, 2613–2619. [Google Scholar] [CrossRef] [PubMed]
- Hölscher, C. Potential role of glucagon-like peptide-1 (GLP-1) in neuroprotection. CNS Drugs 2012, 26, 871–882. [Google Scholar] [CrossRef]
- Cheang, J.Y.; Moyle, P.M. Glucagon-like peptide-1 (GLP-1)-based therapeutics: Current status and future opportunities beyond type 2 diabetes. ChemMedChem 2018, 13, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Anker, C.C.B.; Christiansen, C.B.; Moede, T.; Berggren, P.-O.; Hermansen, K.; Gregersen, S.; Jeppesen, P.B. Pancreatic β Cells Inhibit Glucagon Secretion from α Cells: An In Vitro Demonstration of α–β Cell Interaction. Nutrients 2021, 13, 2281. [Google Scholar] [CrossRef] [PubMed]
- Fineman, M.; Cirincione, B.; Maggs, D.; Diamant, M. GLP-1 based therapies: Differential effects on fasting and postprandial glucose. Diabetes Obes. Metab. 2012, 14, 675–688. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Quast, D.R.; Wefers, J.; Meier, J.J. GLP-1 receptor agonists in the treatment of type 2 diabetes–state-of-the-art. Mol. Metab. 2021, 46, 101102. [Google Scholar] [CrossRef]
- Frandsen, C.S.; Dejgaard, T.F.; Madsbad, S. Non-insulin drugs to treat hyperglycaemia in type 1 diabetes mellitus. Lancet Diabetes Endocrinol. 2016, 4, 766–780. [Google Scholar] [CrossRef]
- Brunton, S. GLP-1 receptor agonists vs. DPP-4 inhibitors for type 2 diabetes: Is one approach more successful or preferable than the other? Int. J. Clin. Pract. 2014, 68, 557–567. [Google Scholar] [CrossRef]
- Iyer, H.; Khedkar, A.; Verma, M. Oral insulin–a review of current status. Diabetes Obes. Metab. 2010, 12, 179–185. [Google Scholar] [CrossRef]
- Vardi, M.; Jacobson, E.; Nini, A.; Bitterman, H. Intermediate acting versus long acting insulin for type 1 diabetes mellitus. Cochrane Database Syst. Rev. 2008, 2008, CD006297. [Google Scholar] [CrossRef]
- Davidson, M.B.; Bate, G.; Kirkpatrick, P. Exenatide. Nat. Rev. Drug Discov. 2005, 4, 713. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J.; Dritselis, A.; Kirkpatrick, P. Liraglutide. Nat. Rev. Drug Discov. 2010, 9, 267–268. [Google Scholar] [CrossRef] [PubMed]
- Christou, G.A.; Katsiki, N.; Blundell, J.; Fruhbeck, G.; Kiortsis, D.N. Semaglutide as a promising antiobesity drug. Obes. Rev. 2019, 20, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Maurya, A.; Singh, A.K.; Mishra, G.; Kumari, K.; Rai, A.; Sharma, B.; Kulkarni, G.T.; Awasthi, R. Strategic use of nanotechnology in drug targeting and its consequences on human health: A focused review. Interv. Med. Appl. Sci. 2019, 11, 38–54. [Google Scholar] [CrossRef]
- Banerjee, A.; Qi, J.; Gogoi, R.; Wong, J.; Mitragotri, S. Role of nanoparticle size, shape and surface chemistry in oral drug delivery. J. Control. Release 2016, 238, 176–185. [Google Scholar] [CrossRef]
- Mailander, V.; Landfester, K. Interaction of nanoparticles with cells. Biomacromolecules 2009, 10, 2379–2400. [Google Scholar] [CrossRef]
- Adair, J.H.; Parette, M.P.; Altınoglu, E.I.; Kester, M. Nanoparticulate alternatives for drug delivery. ACS Nano 2010, 4, 4967–4970. [Google Scholar] [CrossRef]
- Wong, T.; John, P. Advances in spray drying technology for nanoparticle formation. In Handb Nanoparticles [Internet]; Springer International Publishing: Cham, Switzerland, 2016; pp. 329–346. [Google Scholar]
- Cheung, L.K.; Sanders, A.D.; Pratap-Singh, A.; Dee, D.R.; Dupuis, J.H.; Baldelli, A.; Yada, R.Y. Effects of high pressure on protein stability, structure, and function—Theory and applications. In Effect of High-Pressure Technologies on Enzymes; Elsevier: Amsterdam, The Netherlands, 2023; pp. 19–48. [Google Scholar]
- Lopes, M.A.; Abrahim-Vieira, B.; Oliveira, C.; Fonte, P.; Souza, A.M.; Lira, T.; Sequeira, J.A.; Rodrigues, C.R.; Cabral, L.M.; Sarmento, B. Probing insulin bioactivity in oral nanoparticles produced by ultrasonication-assisted emulsification/internal gelation. Int. J. Nanomed. 2015, 10, 5865. [Google Scholar]
- Pedroso-Santana, S.; Fleitas-Salazar, N. Ionotropic gelation method in the synthesis of nanoparticles/microparticles for biomedical purposes. Polym. Int. 2020, 69, 443–447. [Google Scholar] [CrossRef]
- Gao, S.; McClements, D.J. Formation and stability of solid lipid nanoparticles fabricated using phase inversion temperature method. Colloids Surf. A Physicochem. Eng. Asp. 2016, 499, 79–87. [Google Scholar] [CrossRef]
- Battaglia, L.; Gallarate, M.; Cavalli, R.; Trotta, M. Solid lipid nanoparticles produced through a coacervation method. J. Microencapsul. 2010, 27, 78–85. [Google Scholar] [CrossRef]
- Reverchon, E.; Adami, R. Nanomaterials and supercritical fluids. J. Supercrit. Fluids 2006, 37, 1–22. [Google Scholar] [CrossRef]
- Aditya, N.; Patankar, S.; Madhusudhan, B.; Murthy, R.; Souto, E. Arthemeter-loaded lipid nanoparticles produced by modified thin-film hydration: Pharmacokinetics, toxicological and in vivo anti-malarial activity. Eur. J. Pharm. Sci. 2010, 40, 448–455. [Google Scholar] [CrossRef]
- Schubert, M.; Müller-Goymann, C. Solvent injection as a new approach for manufacturing lipid nanoparticles–evaluation of the method and process parameters. Eur. J. Pharm. Biopharm. 2003, 55, 125–131. [Google Scholar] [CrossRef]
- Chopde, S.; Datir, R.; Deshmukh, G.; Dhotre, A.; Patil, M. Nanoparticle formation by nanospray drying & its application in nanoencapsulation of food bioactive ingredients. J. Agric. Food Res. 2020, 2, 100085. [Google Scholar]
- Xu, L.; Wang, X.; Liu, Y.; Yang, G.; Falconer, R.J.; Zhao, C.-X. Lipid nanoparticles for drug delivery. Adv. NanoBiomed Res. 2022, 2, 2100109. [Google Scholar] [CrossRef]
- Çağdaş, M.; Sezer, A.D.; Bucak, S. Liposomes as potential drug carrier systems for drug delivery. Appl. Nanotechnol. Drug Deliv. 2014, 1, 1–50. [Google Scholar]
- He, H.; Lu, Y.; Qi, J.; Zhu, Q.; Chen, Z.; Wu, W. Adapting liposomes for oral drug delivery. Acta Pharm. Sin. B 2019, 9, 36–48. [Google Scholar] [CrossRef]
- Yu, J.; Zhang, Y.; Wang, J.; Wen, D.; Kahkoska, A.R.; Buse, J.B.; Gu, Z. Glucose-responsive oral insulin delivery for postprandial glycemic regulation. Nano Res. 2019, 12, 1539–1545. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, Y.; Li, X.; Nie, D.; Liu, C.; Gan, Y. Ligand-modified nanocarriers for oral drug delivery: Challenges, rational design, and applications. J. Control. Release 2022, 352, 813–832. [Google Scholar] [CrossRef]
- Ding, R.; Zhao, Z.; He, J.; Tao, Y.; Zhang, H.; Yuan, R.; Sun, K.; Shi, Y. Preparation, Drug Distribution, and In Vivo Evaluation of the Safety of Protein Corona Liposomes for Liraglutide Delivery. Nanomaterials 2023, 13, 540. [Google Scholar] [CrossRef]
- Sawant, R.R.; Torchilin, V.P. Polymeric micelles: Polyethylene glycol-phosphatidylethanolamine (PEG-PE)-based micelles as an example. Cancer Nanotechnol. Methods Protoc. 2010, 624, 131–149. [Google Scholar]
- Suzuki, K.; Kim, K.S.; Bae, Y.H. Long-term oral administration of Exendin-4 to control type 2 diabetes in a rat model. J. Control. Release 2019, 294, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; He, Y.; Zhang, H.; Zhang, Y.; Gao, T.; Wang, J.-H.; Wang, S. Zwitterion-functionalized mesoporous silica nanoparticles for enhancing oral delivery of protein drugs by overcoming multiple gastrointestinal barriers. J. Colloid Interface Sci. 2021, 582, 364–375. [Google Scholar] [CrossRef]
- Zhang, Z.-H.; Zhang, Y.-L.; Zhou, J.-P.; Lv, H.-X. Solid lipid nanoparticles modified with stearic acid–octaarginine for oral administration of insulin. Int. J. Nanomed. 2012, 7, 3333–3339. [Google Scholar]
- Wang, T.; Shen, L.; Zhang, Y.; Li, H.; Wang, Y.; Quan, D. “Oil-soluble” reversed lipid nanoparticles for oral insulin delivery. J. Nanobiotechnol. 2020, 18, 98. [Google Scholar] [CrossRef]
- Alsulays, B.B.; Anwer, M.K.; Soliman, G.A.; Alshehri, S.M.; Khafagy, E.-S. Impact of penetratin stereochemistry on the oral bioavailability of insulin-loaded solid lipid nanoparticles. Int. J. Nanomed. 2019, 14, 9127–9138. [Google Scholar] [CrossRef] [PubMed]
- Gopi, S.; Amalraj, A.; Sukumaran, N.P.; Haponiuk, J.T.; Thomas, S. Biopolymers and their composites for drug delivery: A brief review. In Macromolecular Symposia; Wiley: Hoboken, NJ, USA, 2018; p. 1800114. [Google Scholar]
- Ali, A.; Ahmed, S. A review on chitosan and its nanocomposites in drug delivery. Int. J. Biol. Macromol. 2018, 109, 273–286. [Google Scholar] [CrossRef]
- Hsu, L.-W.; Ho, Y.-C.; Chuang, E.-Y.; Chen, C.-T.; Juang, J.-H.; Su, F.-Y.; Hwang, S.-M.; Sung, H.-W. Effects of pH on molecular mechanisms of chitosan–integrin interactions and resulting tight-junction disruptions. Biomaterials 2013, 34, 784–793. [Google Scholar] [CrossRef]
- Şenel, S. Chitosan-based particulate systems for non-invasive vaccine delivery. In Chitosan Biomaterials I; Springer: Berlin/Heidelberg, Germany, 2011; pp. 111–137. [Google Scholar]
- Barzoki, Z.M.; Emam-Djomeh, Z.; Mortazavian, E.; Rafiee-Tehrani, N.; Behmadi, H.; Rafiee-Tehrani, M.; Moosavi-Movahedi, A.A. Determination of diffusion coefficient for released nanoparticles from developed gelatin/chitosan bilayered buccal films. Int. J. Biol. Macromol. 2018, 112, 1005–1013. [Google Scholar] [CrossRef]
- Chen, X.; Ren, Y.; Feng, Y.; Xu, X.; Tan, H.; Li, J. Cp1-11 peptide/insulin complex loaded pH-responsive nanoparticles with enhanced oral bioactivity. Int. J. Pharm. 2019, 562, 23–30. [Google Scholar] [CrossRef]
- Chenthamara, D.; Subramaniam, S.; Ramakrishnan, S.G.; Krishnaswamy, S.; Essa, M.M.; Lin, F.-H.; Qoronfleh, M.W. Therapeutic efficacy of nanoparticles and routes of administration. Biomater. Res. 2019, 23, 1–29. [Google Scholar] [CrossRef]
- Azevedo, C.; Nilsen, J.; Grevys, A.; Nunes, R.; Andersen, J.T.; Sarmento, B. Engineered albumin-functionalized nanoparticles for improved FcRn binding enhance oral delivery of insulin. J. Control. Release 2020, 327, 161–173. [Google Scholar] [CrossRef]
- Araujo, F.; Shrestha, N.; Gomes, M.J.; Herranz-Blanco, B.; Liu, D.; Hirvonen, J.J.; Granja, P.L.; Santos, H.A.; Sarmento, B. In vivo dual-delivery of glucagon like peptide-1 (GLP-1) and dipeptidyl peptidase-4 (DPP4) inhibitor through composites prepared by microfluidics for diabetes therapy. Nanoscale 2016, 8, 10706–10713. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, J.; Zhu, X.; Shan, W.; Li, L.; Zhong, J.; Zhang, Z.; Huang, Y. Efficient mucus permeation and tight junction opening by dissociable “mucus-inert” agent coated trimethyl chitosan nanoparticles for oral insulin delivery. J. Control. Release 2016, 222, 67–77. [Google Scholar] [CrossRef]
- Lee, J.S.; Han, P.; Chaudhury, R.; Khan, S.; Bickerton, S.; McHugh, M.D.; Park, H.B.; Siefert, A.L.; Rea, G.; Carballido, J.M. Metabolic and immunomodulatory control of type 1 diabetes via orally delivered bile-acid-polymer nanocarriers of insulin or rapamycin. Nat. Biomed. Eng. 2021, 5, 983–997. [Google Scholar] [CrossRef]
- He, Z.; Hu, Y.; Gui, Z.; Zhou, Y.; Nie, T.; Zhu, J.; Liu, Z.; Chen, K.; Liu, L.; Leong, K.W. Sustained release of exendin-4 from tannic acid/Fe (III) nanoparticles prolongs blood glycemic control in a mouse model of type II diabetes. J. Control. Release 2019, 301, 119–128. [Google Scholar] [CrossRef]
- Uhl, P.; Grundmann, C.; Sauter, M.; Storck, P.; Tursch, A.; Özbek, S.; Leotta, K.; Roth, R.; Witzigmann, D.; Kulkarni, J. Coating of PLA-nanoparticles with cyclic, arginine-rich cell penetrating peptides enables oral delivery of liraglutide. Nanomed. Nanotechnol. Biol. Med. 2020, 24, 102132. [Google Scholar] [CrossRef]
- Zhang, X.; Sun, M.; Zheng, A.; Cao, D.; Bi, Y.; Sun, J. Preparation and characterization of insulin-loaded bioadhesive PLGA nanoparticles for oral administration. Eur. J. Pharm. Sci. 2012, 45, 632–638. [Google Scholar] [CrossRef]
- Andreani, T.; de Souza, A.L.R.; Kiill, C.P.; Lorenzón, E.N.; Fangueiro, J.F.; Calpena, A.C.; Chaud, M.V.; Garcia, M.L.; Gremião, M.P.D.; Silva, A.M. Preparation and characterization of PEG-coated silica nanoparticles for oral insulin delivery. Int. J. Pharm. 2014, 473, 627–635. [Google Scholar] [CrossRef]
- Tan, X.; Yin, N.; Liu, Z.; Sun, R.; Gou, J.; Yin, T.; Zhang, Y.; He, H.; Tang, X. Hydrophilic and electroneutral nanoparticles to overcome mucus trapping and enhance oral delivery of insulin. Mol. Pharm. 2020, 17, 3177–3191. [Google Scholar] [CrossRef]
- He, Z.; Nie, T.; Hu, Y.; Zhou, Y.; Zhu, J.; Liu, Z.; Liu, L.; Leong, K.W.; Chen, Y.; Mao, H.-Q. A polyphenol-metal nanoparticle platform for tunable release of liraglutide to improve blood glycemic control and reduce cardiovascular complications in a mouse model of type II diabetes. J. Control. Release 2020, 318, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Yin, M.; Song, Y.; Wang, T.; Guo, S.; Zhang, X.; Sun, K.; Li, Y. Oral delivery of liraglutide-loaded poly-N-(2-hydroxypropyl) methacrylamide/chitosan nanoparticles: Preparation, characterization, and pharmacokinetics. J. Biomater. Appl. 2021, 35, 754–761. [Google Scholar] [CrossRef]
- Morales, J.O.; Huang, S.; Williams III, R.O.; McConville, J.T. Films loaded with insulin-coated nanoparticles (ICNP) as potential platforms for peptide buccal delivery. Colloids Surf. B Biointerfaces 2014, 122, 38–45. [Google Scholar] [CrossRef]
- Okamoto, H.; Nakamori, T.; Arakawa, Y.; Iida, K.; Danjo, K. Development of polymer film dosage forms of lidocaine for buccal administration: II. Comparison of preparation methods. J. Pharm. Sci. 2002, 91, 2424–2432. [Google Scholar] [CrossRef]
- Anwar, S.H.; Kunz, B. The influence of drying methods on the stabilization of fish oil microcapsules: Comparison of spray granulation, spray drying, and freeze drying. J. Food Eng. 2011, 105, 367–378. [Google Scholar] [CrossRef]
- Baldelli, A.; Ren, M.; Liang, D.Y.; Lai, S.; Hartono, B.; Sum, K.; Pratap-Singh, A. Sprayed microcapsules of minerals for fortified food. J. Funct. Foods 2023, 101, 105401. [Google Scholar] [CrossRef]
- Baldelli, A.; Boraey, M.A.; Oguzlu, H.; Cidem, A.; Rodriguez, A.P.; Ong, H.X.; Jiang, F.; Bacca, M.; Thamboo, A.; Traini, D. Engineered nasal dry powder for the encapsulation of bioactive compounds. Drug Discov. Today 2022, 27, 2300–2308. [Google Scholar] [CrossRef]
- Fonte, P.; Soares, S.; Costa, A.; Andrade, J.C.; Seabra, V.; Reis, S.; Sarmento, B. Effect of cryoprotectants on the porosity and stability of insulin-loaded PLGA nanoparticles after freeze-drying. Biomatter 2012, 2, 329–339. [Google Scholar] [CrossRef]
- Damgé, C.; Reis, C.P.; Maincent, P. Nanoparticle strategies for the oral delivery of insulin. Expert Opin. Drug Deliv. 2008, 5, 45–68. [Google Scholar] [CrossRef]
- Soares, S.; Fonte, P.; Costa, A.; Andrade, J.; Seabra, V.; Ferreira, D.; Reis, S.; Sarmento, B. Effect of freeze-drying, cryoprotectants and storage conditions on the stability of secondary structure of insulin-loaded solid lipid nanoparticles. Int. J. Pharm. 2013, 456, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Baldelli, A.; Vehring, R. Control of the radial distribution of chemical components in spray-dried crystalline microparticles. Aerosol Sci. Technol. 2016, 50, 1130–1142. [Google Scholar] [CrossRef]
- Baldelli, A.; Power, R.M.; Miles, R.E.; Reid, J.P.; Vehring, R. Effect of crystallization kinetics on the properties of spray dried microparticles. Aerosol Sci. Technol. 2016, 50, 693–704. [Google Scholar] [CrossRef]
- Baldelli, A.; Boraey, M.A.; Nobes, D.S.; Vehring, R. Analysis of the particle formation process of structured microparticles. Mol. Pharm. 2015, 12, 2562–2573. [Google Scholar] [CrossRef] [PubMed]
- Hammad, R.W.; Sanad, R.A.-B.; Abdelmalak, N.S.; Latif, R. Architecting novel multilayer nanosponges for co-administration of two drugs managing high-risk type II diabetes mellitus patients suffering from cardiovascular diseases. Int. J. Biol. Macromol. 2022, 220, 1429–1443. [Google Scholar] [CrossRef]
- Tomar, L.; Tyagi, C.; Kumar, M.; Kumar, P.; Singh, H.; Choonara, Y.E.; Pillay, V. In vivo evaluation of a conjugated poly (lactide-ethylene glycol) nanoparticle depot formulation for prolonged insulin delivery in the diabetic rabbit model. Int. J. Nanomed. 2013, 8, 505–520. [Google Scholar]
- Patil, N.H.; Devarajan, P.V. Insulin-loaded alginic acid nanoparticles for sublingual delivery. Drug Deliv. 2016, 23, 429–436. [Google Scholar] [CrossRef]
- Erzengin, S.; Guler, E.; Eser, E.; Polat, E.B.; Gunduz, O.; Cam, M.E. In vitro and in vivo evaluation of 3D printed sodium alginate/polyethylene glycol scaffolds for sublingual delivery of insulin: Preparation, characterization, and pharmacokinetics. Int. J. Biol. Macromol. 2022, 204, 429–440. [Google Scholar] [CrossRef]
- Dinsmore, W.W.; Wyllie, M.G. The long-term efficacy and safety of a testosterone mucoadhesive buccal tablet in testosterone-deficient men. BJU Int. 2012, 110, 162–169. [Google Scholar] [CrossRef]
- Paris, A.-L.; Caridade, S.; Colomb, E.; Bellina, M.; Boucard, E.; Verrier, B.; Monge, C. Sublingual protein delivery by a mucoadhesive patch made of natural polymers. Acta Biomater. 2021, 128, 222–235. [Google Scholar] [CrossRef]
- Boateng, J.S.; Mitchell, J.C.; Pawar, H.; Ayensu, I. Functional characterisation and permeation studies of lyophilised thiolated chitosan xerogels for buccal delivery of insulin. Protein Pept. Lett. 2014, 21, 1163–1175. [Google Scholar] [CrossRef]
- Nagai, T.; Konishi, R. Buccal/gingival drug delivery systems. J. Control. Release 1987, 6, 353–360. [Google Scholar] [CrossRef]
- Duggan, S.; Cummins, W.; Donovan, O.O.; Hughes, H.; Owens, E. Thiolated polymers as mucoadhesive drug delivery systems. Eur. J. Pharm. Sci. 2017, 100, 64–78. [Google Scholar] [CrossRef] [PubMed]
- Bakhrushina, E.; Anurova, M.; Demina, N.; Kashperko, A.; Rastopchina, O.; Bardakov, A.; Krasnyuk, I. Comparative study of the mucoadhesive properties of polymers for pharmaceutical use. Open Access Maced. J. Med. Sci. 2020, 8, 639–645. [Google Scholar] [CrossRef]
- Böhme, N.; Anders, M.; Reichelt, T.; Schuhmann, K.; Bridarolli, A.; Chevalier, A. New treatments for canvas consolidation and conservation. Herit. Sci. 2020, 8, 16. [Google Scholar] [CrossRef]
- Wasilewska, K.; Winnicka, K. Ethylcellulose–a pharmaceutical excipient with multidirectional application in drug dosage forms development. Materials 2019, 12, 3386. [Google Scholar] [CrossRef]
- Alsarra, I.A.; Hamed, A.Y.; Mahrous, G.M.; El Maghraby, G.M.; Al-Robayan, A.A.; Alanazi, F.K. Mucoadhesive polymeric hydrogels for nasal delivery of acyclovir. Drug Dev. Ind. Pharm. 2009, 35, 352–362. [Google Scholar] [CrossRef]
- Kaczmarek, B. Improving sodium alginate films properties by phenolic acid addition. Materials 2020, 13, 2895. [Google Scholar] [CrossRef]
- Shirsand, S.; Wadageri, G.; Raju, S.; Kolli, G.; Reddy, V. Design and evaluation of mucoadhesive bilayer buccal tablets of nebivolol. RGUHS J. Pharm. Sci. 2013, 3, 40–47. [Google Scholar]
- Singh, T.P.; Singh, R.K.; Shah, J.N.; Mehta, T.A. Mucoadhesive bilayer buccal patches of Verapamil hydrochloride: Formulation development and characterization. Int. J. Pharm. Pharm. Sci. 2014, 6, 234–241. [Google Scholar]
- Shivakumara, L.R.; Demappa, T.; Singh, V. Mechanical and barrier properties of hydroxy propyl methyl cellulose edible polymer films with plasticizer combinations. J. Food Process. Preserv. 2017, 41, e13020. [Google Scholar]
- Gadomska, M.; Musiał, K.; Bełdowski, P.; Sionkowska, A. New Materials Based on Molecular Interaction between Hyaluronic Acid and Bovine Albumin. Molecules 2022, 27, 4956. [Google Scholar] [CrossRef]
- de Souza, A.B.; Chaud, M.V.; Alves, T.F.; de Souza, J.F.; Santana, M.H.A. Hyaluronic acid in the intestinal tract: Influence of structure, rheology, and mucoadhesion on the intestinal uptake in rats. Biomolecules 2020, 10, 1422. [Google Scholar] [CrossRef]
- Kurakula, M.; Rao, G.K. Pharmaceutical assessment of polyvinylpyrrolidone (PVP): As excipient from conventional to controlled delivery systems with a spotlight on COVID-19 inhibition. J. Drug Deliv. Sci. Technol. 2020, 60, 102046. [Google Scholar] [CrossRef]
- Shahzadi, I.; Fürst, A.; Akkus-Dagdeviren, Z.B.; Arshad, S.; Kurpiers, M.; Matuszczak, B.; Bernkop-Schnürch, A. Less reactive thiol ligands: Key towards highly mucoadhesive drug delivery systems. Polymers 2020, 12, 1259. [Google Scholar] [CrossRef]
- Ball, J.P.; Springer, M.J.; Ni, Y.; Finger-Baker, I.; Martinez, J.; Hahn, J.; Suber, J.F.; DiMarco, A.V.; Talton, J.D.; Cobb, R.R. Intranasal delivery of a bivalent norovirus vaccine formulated in an in situ gelling dry powder. PLoS ONE 2017, 12, e0177310. [Google Scholar] [CrossRef] [PubMed]
- Malucelli, L.C.; Lomonaco, D.; Marco Filho, A.; Magalhães, W.L. Cellulose triacetate from different sources: Modification assessment through thermal and chemical characterization. Holzforschung 2020, 74, 505–512. [Google Scholar] [CrossRef]
- Khater, E.-S.; Bahnasawy, A.; Gabal, B.A.; Abbas, W.; Morsy, O. Effect of adding nano-materials on the properties of hydroxypropyl methylcellulose (HPMC) edible films. Sci. Rep. 2023, 13, 5063. [Google Scholar] [CrossRef]
- Wong, W.S.; Hauer, L.; Naga, A.; Kaltbeitzel, A.; Baumli, P.; Berger, R.d.; D ‘Acunzi, M.; Vollmer, D.; Butt, H.-J.r. Adaptive wetting of polydimethylsiloxane. Langmuir 2020, 36, 7236–7245. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, M.; Ullah, S.; Ullah, A.; Saito, Y.; Haider, M.K.; Bie, X.; Wada, K.; Kim, I.S. Carboxymethyl cellulose (CMC) based electrospun composite nanofiber mats for food packaging. Polymers 2021, 13, 302. [Google Scholar] [CrossRef]
- Zhou, Z.-X.; Chen, Y.-R.; Zhang, J.-Y.; Jiang, D.; Yuan, F.-Z.; Mao, Z.-M.; Yang, F.; Jiang, W.-B.; Wang, X.; Yu, J.-K. Facile strategy on hydrophilic modification of poly (ε-caprolactone) scaffolds for assisting tissue-engineered meniscus constructs in vitro. Front. Pharmacol. 2020, 11, 471. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Rubio, L.; Alonso, M.L.; Pérez-Álvarez, L.; Alonso, R.M.; Vilas, J.L.; Khutoryanskiy, V.V. Formulation of Carbopol®/Poly (2-ethyl-2-oxazoline) s mucoadhesive tablets for buccal delivery of hydrocortisone. Polymers 2018, 10, 175. [Google Scholar] [CrossRef]
- Qi, X.; Chen, H.; Rui, Y.; Yang, F.; Ma, N.; Wu, Z. Floating tablets for controlled release of ofloxacin via compression coating of hydroxypropyl cellulose combined with effervescent agent. Int. J. Pharm. 2015, 489, 210–217. [Google Scholar] [CrossRef]
- Abo-shady, A.Z.; Elkammar, H.; Elwazzan, V.S.; Nasr, M. Formulation and clinical evaluation of mucoadhesive buccal films containing hyaluronic acid for treatment of aphthous ulcer. J. Drug Deliv. Sci. Technol. 2020, 55, 101442. [Google Scholar] [CrossRef]
- Hejazi, R.; Amiji, M. Chitosan-based gastrointestinal delivery systems. J. Control. Release 2003, 89, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Nafee, N.A.; Ismail, F.A.; Boraie, N.A.; Mortada, L.M. Mucoadhesive delivery systems. I. Evaluation of mucoadhesive polymers for buccal tablet formulation. Drug Dev. Ind. Pharm. 2004, 30, 985–993. [Google Scholar] [CrossRef]
- Zaman, M.; Qureshi, J.; Ejaz, H.; Sarfraz, R.M.; Khan, H.; Sajid, F.; Rehman, M. Oral controlled release drug delivery system and characterization of oral tablets: A review. Pak. J. Pharm. Res. 2016, 2, 67–76. [Google Scholar] [CrossRef]
- Brandl, M.; Bauer-Brandl, A. Oromucosal drug delivery: Trends in in-vitro biopharmaceutical assessment of new chemical entities and formulations. Eur. J. Pharm. Sci. 2019, 128, 112–117. [Google Scholar] [CrossRef]
- Chun, M.-K.; Kwak, B.-T.; Choi, H.-K. Preparation of buccal patch composed of carbopol, poloxamer and hydroxypropyl methylcellulose. Arch. Pharmacal Res. 2003, 26, 973–978. [Google Scholar] [CrossRef]
- Dutta, T.; Chowdhury, S.K.; Ghosh, N.N.; Chattopadhyay, A.P.; Das, M.; Mandal, V. Green synthesis of antimicrobial silver nanoparticles using fruit extract of Glycosmis pentaphylla and its theoretical explanations. J. Mol. Struct. 2022, 1247, 131361. [Google Scholar] [CrossRef]
- Khamhan, S.; Baimark, Y. Morphology and Thermal Stability of Chitosan and Methoxy Poly (ethylene glycol)-b-Poly (e-caprolactone)/Poly (D, L-lactide) Nanocomposite Films. J. Appl. Sci. 2009, 9, 1147–1152. [Google Scholar] [CrossRef]
- Javanbakht, S.; Shaabani, A. Carboxymethyl cellulose-based oral delivery systems. Int. J. Biol. Macromol. 2019, 133, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y. Nanoencapsulation and Buccal Delivery System to Augment Bioavailability of Insulin. Ph.D. Thesis, University of British Columbia, Vancouver, BC, Canada, 2023. [Google Scholar]



| Peptide | Chemical Structure | Detailed Type | Molecular Weight (kDa) | Water Solubility (mg/mL) | Ref. |
|---|---|---|---|---|---|
| Short-acting insulin | C257H383N65O77S6 | Humulin R U-100 Novolin R FlexPen ReliOn | 5.8 | Insoluble | [53] |
| Rapid-acting insulin | C257H383N65O77S6 | inhaled insulin insulin aspart insulin glulisine insulin lispro | 5.8 | Insoluble | [53] |
| Intermediate-acting insulin | C257H383N65O77S6 | insulin isophane | 5.8 | Insoluble | [54] |
| Long-acting insulin | C274H411N65O81S6 | insulin degludec | 5.8 | 104 | [54] |
| C267H402O76N64S6 | insulin detemir | 5.9 | 14.2 | ||
| C267H404N72O78S6 | insulin glargine | 6.1 | 3.6 | ||
| Exenatide | C184H282N50O60S | GLP-1 stimulates glucose | 4.2 | 3 | [55] |
| Liraglutide | C172H265N43O51 | GLP-1 stimulates glucose | 3.7 | 270 | [56] |
| Semaglutide | C187H291N45O59 | GLP-1 stimulates glucose | 4.1 | 1 | [57] |
| Preparation Method | Advantages | Disadvantages |
|---|---|---|
| High-pressure homogenization (HPP) |
|
|
| Ultrasonication |
|
|
| Ion gelation |
|
|
| Phase inversion temperature (PIT) |
|
|
| Coacervation |
|
|
| Supercritical fluid method |
|
|
| Solvent emulsification/evaporation |
|
|
| Film hydration |
|
|
| Solvent injection |
|
|
| Nano spray drying |
|
|
| Drug | Encapsulation Method | In Vivo Method/Dose | Delivery Mechanism | Ref. |
|---|---|---|---|---|
| Insulin | Fc-receptor (FcRn)-targeted liposomes with glucose-sensitive hyaluronic acid (HA) shell | Chemically induced type 1 diabetic mice/10U/kg | The detachment of HA occurs when glucose binds with phenylboronic acid during high postprandial glucose levels. Fc facilitates the absorption of liposomes in the intestines. | [75] |
| Exendin-4 | Chondroitin sulfate-g-glycocholic acid (GCA)-coated liposomes (EL-CSG) | High-fat diet STZ-induced T2DM rats/300 μg/kg | GCA promoted the transportation of liposomes through the layer of intestinal epithelial cells. | [79] |
| Insulin | Solid lipid nanoparticles (SLNs) modified with stearic acid–octaarginine (SA-R8) | Fasted diabetic rats/25 U/kg | Insulin was partially protected from gastrointestinal enzymes by incorporation into SLNs and SA-R8. | [81] |
| Insulin | “Oil-soluble” reversed lipid nanoparticles (ORLN) coated with phospholipid (PC) shell | Fasted diabetic rats/60 μg/kg | The decrease in enzymatic degradation of insulin in the intestinal tract, as well as the increase in drug transcytosis across the intestinal epithelia. | [82] |
| Insulin | Cell-penetrating peptides (CPPs)—incorporated insulin-loaded solid lipid nanoparticles | Fasted diabetic rats/10 U/kg | Intermolecular interactions between INS and L- and/or D-penetration. | [83] |
| Drug | Encapsulation Method | In Vivo Method/Dose | Delivery Mechanism | Ref. |
|---|---|---|---|---|
| Exendin-4 | Tannic acid/exendin-4/Fe3+ ternary nanoparticle system | T2D mice/6 mg/kg | The ternary NPs release exendin-4 in a sustained manner because of pH-induced dissociation after intraperitoneal administration | [95] |
| Insulin | Hydroxypropyl methylcellulose phthalate (HP55)-coated capsule containing PLGA/RS NPs | Fasted diabetic rats/50 U/kg | Selectively released insulin from NPs in the intestinal tract, instead of stomach, enhances the penetration of insulin across the mucosal surface in the intestine. | [95] |
| liraglutide | PLA NPs modified with a cyclic, polyarginine-rich, cell-penetrating peptide (cyclic R9-CPP) | Fasted diabetic rats/0.5 MBq | These NPs facilitated the intestinal retention and mucosal penetration of peptide therapeutics. | [96] |
| Insulin | Positively charged chitosan-coated PLGA NP (CS-PLGA NP) | Fasted diabetic rats/15 U/kg | CS-PLGA NPs show positive charge, mucosal adhesion, and absorption promotion, and thus, a long residence of insulin | [97] |
| Insulin | PEG-coated silica nanoparticles (SiNP–PEG) | Fasted diabetic rats/15 U/kg | SiNP shows high porosity allowing efficient drug loading | [98] |
| Insulin | Mesoporous silica NPs (MSNs) modified with a hydrophilic block polymer PLA–PEG | Fasted diabetic rats/80 U/kg | MSNs can decrease hydrophobic forces and achieve mucus-inert or penetrating characteristics. | [99] |
| liraglutide | Liraglutide/tannic acid (TA)/Al3+ NP system based on hydrogen bond formation between liraglutide and TA and stabilized by complex coordination interaction between TA and Al3+ | Fasted diabetic mice/2 mg/kg | Under physiological conditions (Ph 7.4), the partial ionization of phenol groups weaken the hydrogen bonding, and thus trigger decomplexation and release of liraglutide. | [100] |
| liraglutide | NPs composed of chitosan and poly-N-(2-hydroxypropyl) methacrylamide (Phpma) | Fasted diabetic mice/5 mg/kg | Chitosan can open the connection of epithelial cells while the water solubility of Phpma helps to penetrate the mucus layer | [101] |
| Bioadhesive Layer | |||||
| Polymer | Mucoadhesivity (N) | Water Solubility (mg/mL) | Tensile Strength (MPa) | Viscosity (Pa s) | Ref. |
| Carbopol (940) | 6–7 | 100 | 0.1–114 | 3–5 | [140] |
| Sodium alginate | 6–9 | 0.4 | 30–70 | 0.25–0.60 | [116] |
| Hydroxyethyl cellulose | 25–35 | 9 | 1.3 ± 0.7 | 0.1–8.5 | [141] |
| Hydroxypropyl methylcellulose | 1.5–9 | 10 | 10–38 | 0.1–10 | [102] |
| Hyaluronic acid | 0.4–5 | 5 | 5–50 | <10−4 | [142] |
| Chitosan | 9–11 | 8 | 100–130 | 0.1–1 | [143] |
| Polyvinyl pyrrolidone | 4–9 | 100 | 0.5–1.4 | 1.2–1.7 | [113] |
| Polyacrylic acid | 0.1–0.5 | 2–10 | 0.1–5 | 0.1–2 | [144] |
| Water-Repellent Layer | |||||
| Polymer | Hydrophobicity (°) | Water Solubility (mg/mL) | Tensile Strength (MPa) | Viscosity (Pa s) | Ref. |
| Polyvinylchloride | 73–81 | 10 | 40–50 | 0.01–0.05 | [145] |
| Polydimethylsiloxane | 88–95 | Insoluble | 3.1–5.5 | 4–10 | [146] |
| Hydroxypropyl methylcellulose | 57–84 | 1–500 | 40–160 | 4–10 | [147] |
| Hemicellulose | 80–90 | Insoluble | 30–40 | 0.4–0.45 | [148] |
| Ethylcellulose | 73–75 | Poor | 170–240 | 0.18–1.10 | [145] |
| Poly(e-caprolactone) (PCL) | 40–80 | 1–3 | 100–150 | 800–1300 | [149] |
| Carboxymethyl cellulose | 85–120 | 10 | 42–47 | 800–1200 | [150] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pratap-Singh, A.; Guo, Y.; Baldelli, A.; Singh, A. Concept for a Unidirectional Release Mucoadhesive Buccal Tablet for Oral Delivery of Antidiabetic Peptide Drugs Such as Insulin, Glucagon-like Peptide 1 (GLP-1), and their Analogs. Pharmaceutics 2023, 15, 2265. https://doi.org/10.3390/pharmaceutics15092265
Pratap-Singh A, Guo Y, Baldelli A, Singh A. Concept for a Unidirectional Release Mucoadhesive Buccal Tablet for Oral Delivery of Antidiabetic Peptide Drugs Such as Insulin, Glucagon-like Peptide 1 (GLP-1), and their Analogs. Pharmaceutics. 2023; 15(9):2265. https://doi.org/10.3390/pharmaceutics15092265
Chicago/Turabian StylePratap-Singh, Anubhav, Yigong Guo, Alberto Baldelli, and Anika Singh. 2023. "Concept for a Unidirectional Release Mucoadhesive Buccal Tablet for Oral Delivery of Antidiabetic Peptide Drugs Such as Insulin, Glucagon-like Peptide 1 (GLP-1), and their Analogs" Pharmaceutics 15, no. 9: 2265. https://doi.org/10.3390/pharmaceutics15092265