Migrant Workers and Physical Health: An Umbrella Review

 ,
, 
 ,
, 

Abstract
1. Introduction
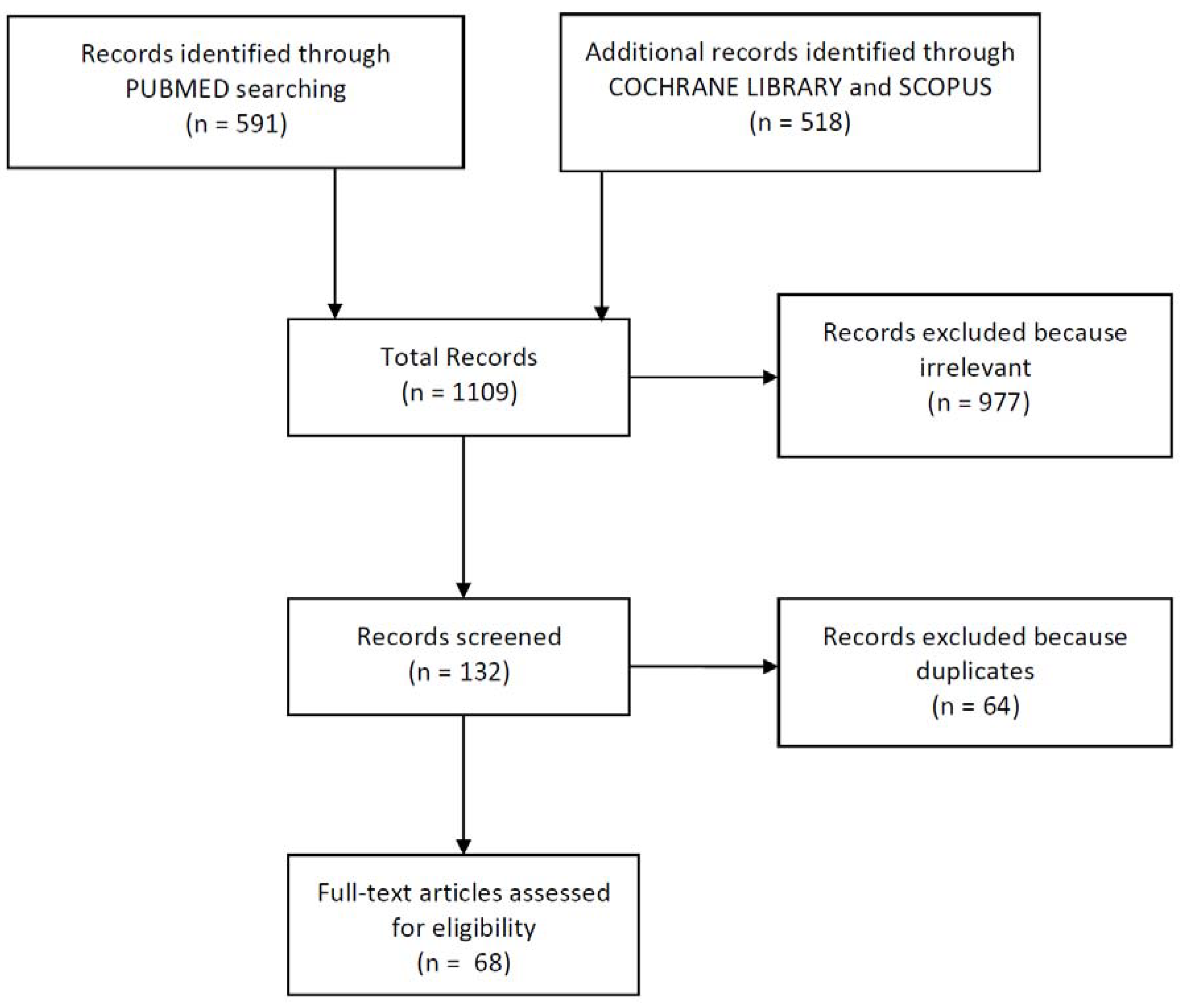
2. Materials and Methods
2.1. Literature Research
2.2. Quality Assessment
2.3. Eligibility and Inclusion Criteria
2.4. Exclusion Criteria
3. Results
3.1. Reviews
3.2. Original Articles
3.2.1. Infectious Diseases
3.2.2. Cardiovascular and Metabolic Diseases
3.2.3. Quality of Life
3.2.4. Various Diseases
3.3. Trial
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Migration Report 2017 (Highlights). Available online: https://www.un.org/development/desa/publications/international-migration-report-2017.html (accessed on 30 October 2018).
- Just Landed. Available online: https://www.justlanded.com/italiano/Common/Footer/Espatriati/Statistiche-e-caratteristiche (accessed on 30 October 2018).
- HSBC Expat Explorer. Available online: https://www.expatexplorer.hsbc.com (accessed on 30 October 2018).
- Di Fabio, A.; Rosen, M.A. Opening the Black Box of Psychological Processes in the Science of Sustainable Development: A New Frontier. Eur. J. Sustain. Dev. Res. 2018, 2, 47. [Google Scholar] [CrossRef]
- Porru, S.; Arici, C. Gruppi vulnerabili-Migranti. In Trattato di Medicina del Lavoro, 1st ed.; Alessio, L., Franco, G., Tomei, F., Eds.; Piccin-Nuova Libraria: Padova, Italy, 2015; Volume II, pp. 1327–1336. ISBN 978-88-299-2708-1. [Google Scholar]
- Di Carluccio, C. Salute e sicurezza sul lavoro del lavoratore migrante tra conferme e sviluppi. Diritto della Sicurezza sul Lavoro 2017, 1, 45–74. [Google Scholar]
- Di Fabio, A. The Psychology of Sustainability and Sustainable Development for Well-Being in Organizations. Front. Psychol. 2017, 8, 1534. [Google Scholar] [CrossRef] [PubMed]
- Di Fabio, A. Positive Healthy Organizations: Promoting well-being, meaningfulness, and sustainability in organizations. Front. Psychol. 2017, 8, 1938. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Backhaus, I.; Mannocci, A. Rating for narrative reviews: Concept and development of the International Narrative Systematic Assessment tool. Sens. Sci. 2015, 2, 31–35. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connel, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analyses. 2009. Available online: http://wwwohrica/programs/ clinical_epidemiology/oxford (accessed on 30 October 2018).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Fitzgerald, S.; Chen, X.; Qu, H.; Sheff, M.G. Occupational injury among migrant workers in China: A systematic review. Inj. Prev. 2013, 19, 348–354. [Google Scholar] [CrossRef]
- Sabhlok, A.; Cheung, H.; Mishra, Y. Narratives of health and well-being: Migrant road workers in the upper Himalayas. Econ. Polit. Wkly. 2015, 50, 51. [Google Scholar]
- Saradangani, S.P.; Lim, P.L.; Vasoo, S. Infectious diseases and migrant worker health in Singapore: A receiving country’s perspective. J. Travel. Med. 2017, 24. [Google Scholar] [CrossRef]
- Simkhada, P.P.; Regmi, P.R.; Van Teijlingen, E.; Aryal, N. Identifying the gaps in Nepalese migrant workers’ health and well-being: A review of the literature. J. Travel. Med. 2017, 24. [Google Scholar] [CrossRef] [PubMed]
- Arcury, T.A.; Grzywacz, J.G.; Sidebottom, J.; Wiggins, M.F. Overview of immigrant worker occupational health and safety for the agriculture, forestry, and fishing (AgFF) sector in the southeastern United States. Am. J. Ind. Med. 2013, 8, 911–924. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, B. Health inequities faced by Ethiopian migrant domestic workers in Lebanon. Health Place 2018, 50, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Dafalla, A.I.A.; Almuhairi, S.A.S.O.; Al Hosani, M.H.J.; Abuodeh, R.O.; El Bakri, A. Intestinal parasitic infections among expatriate workers in various occupations in Sharjah, United Arab Emirates. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, 82. [Google Scholar] [CrossRef] [PubMed]
- Taha, H.A.; Soliman, M.I.; Banjar, S.A. Intestinal parasitic infections among expatriate workers in Al-Madina Al-Munawarah, Kingdom of Saudi Arabia. Trop. Biomed. 2013, 1, 78–88. [Google Scholar]
- Al Hosani, F.I.; Yahia, G.A. Prevalence of pulmonary tuberculosis among expatriates subjected to medical visa screening in Abu Dhabi, United Arab Emirates. J. Epidemiol. Glob. Health 2013, 1, 23–30. [Google Scholar] [CrossRef]
- Gao, X.F.; Rao, Y. Quality of life of a migrant population with tuberculosis in West China. Int. J. Tuberc. Lung Dis. 2015, 2, 223–230. [Google Scholar] [CrossRef]
- Fonseca, A.G.; Dias, S.S.; Baptista, J.L.; Torgal, J. The burden of imported malaria in Portugal 2003 to 2012. J. Travel. Med. 2014, 2009–2011. [Google Scholar] [CrossRef]
- Fonseca, A.G.; Dias, S.S.; Baptista, J.L.; Torgal, J. Portuguese expatriates’ health in Angola and Mozambique—A cross-sectional study: Increasing awareness and need for more surveillance. J. Travel. Med. 2017, 4. [Google Scholar] [CrossRef]
- Bi, Y.; Wang, L.; Xu, Y.; Jiang, Y.; He, J.; Zhang, M.; Li, Y.; Xu, M.; Lu, J.; Wang, T.; et al. Diabetes-related metabolic risk factors in internal migrant workers in China: A national surveillance study. Lancet Diabetes Endocrinol. 2016, 2, 125–135. [Google Scholar] [CrossRef]
- Varadharajan, K.S.; Thomas, T.; Rajaraman, D.; Kurpad, A.V.; Vaz, M. Overweight and obesity among internal migrants in India. Asia Pac. J. Clin. Nutr. 2013, 3, 416–425. [Google Scholar]
- Yang, H.; He, F.; Wang, T.; Liu, Y.; Shen, Y.; Gong, J.; Dai, W.; Zhou, J.; Gu, J.; Tu, Y.; et al. Health-related lifestyle behaviors among male and female rural-to-urban migrant workers in Shanghai, China. PLoS ONE 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Loney, T.; Sheek-Hussein, M.; El Sadig, M.; Al Dhaheri, S.; El Barazi, I.; Al Marzouqi, L.; Aw, T.C.; Ali, R. Hypertension prevalence, awareness, treatment, and control, in male South Asian immigrants in the United Arab Emirates: A cross-sectional study. BMC Cardiovasc. Disord. 2015, 15, 30. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, S.F.; Rosenbaum, R.P.; Holscher, J.T.; Madanat, H.; Talavera, G.A. Cardiovascular disease risk factors among Latino migrant and seasonal farmworkers. J. Agromed. 2015, 2, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Skokberg, N.; Laatikainen, T.; Jula, A.; Härkänen, T.; Vartiainen, E.; Koponen, P. Contribution of sociodemographic and lifestyle-related factors to the differences in metabolic syndrome among Russian, Somali and Kurdish migrants compared with Finns. Int. J. Cardiol. 2017, 232, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Ali, R.; Loney, T.; Aziz, F.; El Barazi, I.; Al Dhaheri, S.; Farooqi, M.H.; Blair, I. Prevalence of Diabetes among Migrant Women and Duration of Residence in the United Arab Emirates: A Cross Sectional Study. PLoS ONE 2017, 1. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Calabrese, M.; Malandrino, D.; Colella, A.; Galanti, G.; Zhao, D. New findings on type 2 diabetes in first-generation Chinese migrants settled in Italy: Chinese in Prato (CHIP) cross-sectional survey. Diabetes Metab. Res. Rev. 2017, 2. [Google Scholar] [CrossRef]
- Yan, S.; Hong, X.; Yu, H.; Yang, Z.; Liu, S.; Quan, W.; Xu, J.; Zhu, L.; Cheng, W.; Xiao, H.; et al. Prevalence of Diabetes and Health-Related Quality of Life Among Rural-to-Urban Nong Zhuan Fei Migrants in an Urban Area of Northern China, 2013. Public Health Rep. 2016, 1, 167–176. [Google Scholar] [CrossRef]
- Ronda, E.; Briones-Vozmediano, E.; Galon, T.; García, A.M.; Benavides, F.G.; Agudelo-Suárez, A.A. A qualitative exploration of the impact of the economic recession in Spain on working, living and health conditions: Reflections based on immigrant workers’ experiences. Health Expect. 2016, 2, 416–426. [Google Scholar] [CrossRef]
- Anjara, S.G.; Nellums, L.B.; Bonetto, C.; Van Bortel, T. Stress, health and quality of life of female migrant domestic workers in Singapore: A cross-sectional study. BMC Women’s Health 2017, 1, 98. [Google Scholar] [CrossRef]
- Lu, C.H.; Wang, P.X.; Lei, Y.X.; Luo, Z.C. Influence of health-related quality of life on health service utilization in Chinese rural-to-urban female migrant workers. Health Qual. Life Outcome 2014, 12, 121. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Zou, G.; Zeng, Z.; Han, L.; Guo, Y.; Ling, L. Health-Related Quality of Life and Its Correlates among Chinese Migrants in Small- and Medium-Sized Enterprises in Two Cities of Guangdong. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Khongthanachayopit, S.; Laohasiriwong, W. Accessibility to health services among migrant workers in the Northeast of Thailand. F1000 Res. 2017, 6, 972. [Google Scholar] [CrossRef] [PubMed]
- Tam, W.J.; Goh, W.L.; Chua, J.; Legido-Quigley, H. Health is my capital: A qualitative study of access to healthcare by Chinese migrants in Singapore. Int. J. Equity Health 2017, 1, 102. [Google Scholar] [CrossRef] [PubMed]
- Kumparatana, P.; Cournos, F.; Terlikbayeva, A.; Rozental, Y.; Gilbert, L. Factors associated with self-rated health among migrant workers: Results from a population-based cross-sectional study in Almaty, Kazakhstan. Int. J. Public Health 2017, 5, 541–550. [Google Scholar] [CrossRef]
- Yang, H.; Gao, J.; Wang, T.; Yang, L.; Liu, Y.; Shen, Y.; Gong, J.; Dai, W.; Zhou, J.; Gu, J.; et al. Association between adverse mental health and an unhealthy lifestyle in rural-to-urban migrant workers in Shanghai. J. Formos. Med. Assoc. 2017, 2, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, P.; Kim, M. Predictors of the Health-Promoting Behaviors of Nepalese Migrant Workers. J. Nurs. Res. 2016, 3, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Banerejee, M.; Kamath, R.; Tiwari, R.R.; Nair, N.P. Dermatological and respiratory problem in migrant construction workers of Udupi, Karnataka. Indian. J. Occup. Environ. Med. 2015, 3, 125–128. [Google Scholar] [CrossRef]
- Perez-Carceles, M.D.; Medina, M.D.; Perez-Flores, D.; Noguera, J.A.; Pereniguez, J.E.; Madrigal, M.; Luna, A. Screening for hazardous drinking in migrant workers in southeastern Spain. J. Occup. Health 2014, 1, 39–48. [Google Scholar] [CrossRef]
- Pichardo-Geisinger, R.; Muñoz-Ali, D.; Arcury, T.A.; Feldman, S.R.; Quandt, S.A. Dermatologist-diagnosed skin diseases among immigrant Latino poultry processors and other manual workers in North Carolina, USA. Int. J. Dermatol. 2013, 11, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Dodd, V.J.; Schenck, D.P.; Chaney, E.H.; Padhya, T. Assessing Oral Cancer Awareness among Rural Latino Migrant Workers. J. Immigr. Minor. Health 2016, 3, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Brumitt, J.; Garside, L.I.; Reisch, R.; Marshall, T.; Gilpin, H.E.; Kinsey, J.; Imondi, K.; Robinson, H.J. Exercise habits and tobacco use among male Latino farmworkers. Agromedicine 2013, 12, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, J.B.; Calzavara, L.; Light, L.; Burchell, A.N. Design and implementation of a sexual health intervention for migrant construction workers situated in Shanghai, China. Emerg. Themes Epidemiol. 2015, 1. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, J.; De La Rosa, M.; Serna, C.A. Project Salud: Efficacy of a community-based HIV prevention intervention for Hispanic migrant workers in south Florida. AIDS Educ. Prev. 2013, 5, 363. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Li, T.; Zou, G.; Li, X.; Shi, L.; Feng, S.; Shi, J.; Zhou, F.; Han, S.; Ling, L. Study protocol: A cluster randomized controlled trial to assess the effectiveness of a multi-pronged behavioral intervention to improve use of personal protective equipment among migrant workers exposed to organic solvents in small and medium-sized enterprises. BMC Public Health 2016, 16, 580. [Google Scholar] [CrossRef]
- Lee, H.; Cho, S.; Wilbur, J.; Kim, J.; Park, C.G.; Lee, Y.M.; Lee, H. Effects of culturally adaptive walking intervention on cardiovascular disease risks for middle-aged Korean-Chinese female migrant workers. Arch. Environ. Occup. Health 2017, 6, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Han, L.Q.; Guo, Y.J.; Sun, J. Using WeChat official accounts to improve malaria health literacy among Chinese expatriates in Niger: An intervention study. Malaria J. 2016, 1, 567. [Google Scholar] [CrossRef]
- Vernier, M.; Rossi-Tamisier, M.; Richet, H.; Colson, P.; Gautret, P. Anti-hepatitis E virus antibody prevalence in French expatriate workers. IJID 2013, 11. [Google Scholar] [CrossRef]
- Sharif, F.; Daryani, A.; Kia, E.; Rezaei, F.; Nasiri, M.; Nasrolahei, M. Prevalence of intestinal parasites among food handlers of Sari, Northern Iran. Rev. Inst. Med. Trop. Sao Paulo 2015, 2, 139–144. [Google Scholar] [CrossRef]
- Kheirandish, F.; Tarahi, M.; Ezatpour, B. Prevalence of intestinal parasites among food handlers in West Iran. Rev. Inst. Med. Trop. Sao Paulo 2014, 2, 111–114. [Google Scholar] [CrossRef]
- Wangroogsarb, P.; Hwang, J.; Thwing, J.; Karuchit, S.; Kumpetch, S.; Rand, A.; Drakeley, C.; MacArthur, J.R.; Kachur, S.P.; Satimai, W.; et al. Using Respondent Driven Sampling to Identify Malaria Risks and Occupational Networks among Migrant Workers in Ranong, Thailand. PLoS ONE 2016, 12. [Google Scholar] [CrossRef]
- Global Tuberculosis Report 2018. Available online: https://www.who.int/tb/publications/global_report/en/ (accessed on 30 October 2018).
- Li, Y.; Huang, X.M.; Zhao, D.M.; Liu, Y.Z.; He, K.W.; Liu, Y.X.; Chen, C.H.; Long, L.P.; Xu, Y.; Xie, X.X.; et al. Detection of Avian H7N9 Influenza a Viruses in the Yangtze Delta Region of China during Early H7N9 Outbreaks. Avian Dis. 2016, 1, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Li, Y.; Wangen, K.R.; Nicholas, S.; Maitland, E.; Wang, J. Hepatitis B discrimination in everyday life by rural migrant workers in Beijing. Hum. Vaccines Immunother. 2016, 5, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Salyer, S.J.C.; Bron, C.; Juin, S.; Hemme, R.R.; Hunsperger, E.; Jentes, E.S.; Magloire, R.; Tomashek, K.M.; Desormeaux, A.M.; Muñoz-Jordán, J.L.; et al. Dengue virus infections among Haitian and expatriate non-governmental organization workers—Léogane and Port-au-Prince, Haiti, 2012. PLoS Negl. Trop. Dis. 2014, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Tang, G.; Huang, Y.; Bai, T.; Shu, Y. A returning migrant worker with avian influenza A (H7N9) virus infection in Guizhou, China: A case report. J. Med. Case Rep. 2015, 9, 109. [Google Scholar] [CrossRef] [PubMed]
- Ning, C.; Jiang, J.; Ye, L.; Yang, X.; Wei, B.; Deng, W.; Wei, S.; Huang, J.; Qin, B.; Upur, H.; et al. Comparison of Three Intervention Models for Promoting Circumcision among Migrant Workers in Western China to Reduce Local Sexual Transmission of HIV. PLoS ONE 2013, 9. [Google Scholar] [CrossRef]
- Al Rifai, R.; Nakamura, K.; Seino, K.; Kizuki, M.; Morita, A. Unsafe sexual behaviour in domestic and foreign migrant male workers in multinational workplaces in Jordan: Occupational-based and behavioural assessment survey. BMJ Open 2015, 6. [Google Scholar] [CrossRef]
- Norris, A.H.; Decker, M.R.; Weisband, Y.L.; Hindin, M.J. Reciprocal physical intimate partner violence is associated with prevalent STI/HIV among male Tanzanian migrant workers: A cross-sectional study. Sex Transm. Infect. 2017, 4, 253–258. [Google Scholar] [CrossRef]
- Urmi, A.Z.; Leung, D.T.; Wilkinson, V.; Miah, M.A.A.; Rahman, M.; Azim, T. Profile of an HIV testing and counseling unit in Bangladesh: Majority of new diagnoses among returning migrant workers and spouses. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Goldenberg, S.M.; Rocha Jiménez, T.; Brouwer, K.C.; Morales Miranda, S.; Silverman, J.G. Influence of indoor work environments on health, safety, and human rights among migrant sex workers at the Guatemala-Mexico Border: A call for occupational health and safety interventions. BMC Int. Health Hum. Rights 2018, 1, 9. [Google Scholar] [CrossRef]
- Lee, W.S. Height, Weight and Well-Being for Rural, Urban and Migrant Workers in China. Soc. Indic. Res. 2017, 132, 117–136. [Google Scholar] [CrossRef]
- Shah, S.M.; Loney, T.; Dhaheri, S.A.; Vatanparast, H.; Elbarazi, I.; Agarwal, M.; Blair, I.; Ali, R. Association between acculturation, obesity and cardiovascular risk factors among male South Asian migrants in the United Arab Emirates—A cross-sectional study. BMC Public Health 2015, 28, 204. [Google Scholar] [CrossRef]
- Eastwood, S.V.; Tillin, T.; Dehbi, H.M.; Wright, A.; Forouhi, N.G.; Godsland, I. Ethnic differences in associations between fat deposition and incident diabetes and underlying mechanisms: The SABRE study. Obesity 2015, 3, 699–706. [Google Scholar] [CrossRef]
- Gele, A.A.; Mbalilaki, A.J. Overweight and obesity among African immigrants in Oslo. BMC Res. Notes 2013, 6, 119. [Google Scholar] [CrossRef]
- Martin, M.Y.; Francis, L.A. U.S. Migrant Networks and Adult Cardiometabolic Health in El Salvador. J. Immigr. Minor. Health 2016, 6, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Mannocci, A.; Pignalosa, S.; Nicosia, V.; Saulle, R.; Sernia, S.; La Torre, G. Cardiovascular Diseases Risk Factors in oil and gas workers: A ten years observational retrospective cohort. Annali di Igiene 2016, 2, 122–132. [Google Scholar] [CrossRef]
- Norredam, M.; Agyemang, C.; Hoejbjerg Hansen, O.K.; Petersen, J.H.; Byberg, S.; Krasnik, A. Duration of residence and disease occurrence among refugees and family reunited immigrants: Test of the ‘healthy migrant effect’ hypothesis. Trop. Med. Int. Health 2014, 8, 958–967. [Google Scholar] [CrossRef]
- Le-Scherban, F.; Albrecht, S.S.; Bertoni, A.; Kandula, N.; Mehta, N.; Diez Roux, A.V. Immigrant status and cardiovascular risk over time: Results from the Multi-Ethnic Study of Atherosclerosis. Ann. Epidemiol. 2016, 6, 429–435. [Google Scholar] [CrossRef]
- Commodore-Mensah, N.; Ukonu, O.; Obisesan, J.K.; Aboagye, C.; Agyemang, C.M. Length of residence in the United States is associated with a higher prevalence of cardiometabolic risk factors in immigrants: A contemporary analysis of the National Health Interview Survey. J. Am. Heart. Assoc. 2016, 11. [Google Scholar] [CrossRef]
- Adsul, B.B.; Laad, P.S.; Howal, P.V.; Chaturvedi, R.M. Health problems among migrant construction workers: A unique public-private partnership project. Indian. J. Occup. Environ. Med. 2011, 15, 29–32. [Google Scholar] [CrossRef]
- Maldonado Molina, M.M.; Reingle, J.M.; Jennings, W.G.; Prado, G. Drinking and driving among immigrant and US-born Hispanic young adults: Results from a longitudinal and nationally representative study. Addict. Behav. 2011, 36, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Relazione Annuale INAIL 2017. Available online: www.inail.it/cs/internet/comunicazione/pubblicazioni/rapporti-e-relazioni-inail/relazione-annuale-anno-2017.html (accessed on 30 October 2018).
- Biering, K.; Lander, F.; Rasmussen, K. Work injuries among migrant workers in Denmark. Occup. Environ. Med. 2017, 4, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Mariammal, T.; Jaisheeba, A.A.; Sornaraj, R. Work related respiratory symptoms and pulmonary function tests observed among construction and sanitary workers of Thoothukudi. Int. J. Pharm. Tech. Res. 2012, 4, 1266–1273. [Google Scholar]
- Habib, R.R.; Mikati, D.; Hojeij, S.; Chaaya, M.; Zurayk, R. Associations between poor living conditions and multi-morbidity among Syrian migrant agricultural workers in Lebanon. Eur. J. Public Health 2016, 6, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Earle-Richardson, G.; Wyckoff, L.; Carrasquillo, M.; Scribani, M.; Jenkins, P.; May, J. Evaluation of a community-based participatory farmworker eye health intervention in the “black dirt” region of New York State. Am. J. Ind. Med. 2014, 9, 1053. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Apostolopoulos, Y.; Sönmez, S. Work Conditions and Health and Well-Being of Latina Hotel Housekeepers. J. Immigr. Minor. Health 2016, 3, 568–581. [Google Scholar] [CrossRef]
- Jensen, M.T.; Rundmo, T. Associations between work family conflict, emotional exhaustion, musculoskeletal pain, and gastrointestinal problems in a sample of business travelers. Scand. J. Psychol. 2015, 1, 105–113. [Google Scholar] [CrossRef]
- Thomas, B.E.; Charles, N.; Watson, B.; Chandrasekaran, V.; Senthil Kumar, R.; Dhanalakshmi, A.; Wares, F.; Swaminathan, S. Prevalence of chest symptoms amongst brick kiln migrant workers and care seeking behaviour: A study from South India. J. Public Health 2015, 4, 590–596. [Google Scholar] [CrossRef]
- Zeng, Z.; Lu, L.; Rao, Z.; Han, L.; Shi, J.; Ling, L. Analysis of use of personal protective equipment among rural-to-urban migrant workers in small and medium enterprises in Zhongshan and Shenzhen, China. Chin. J. Ind. Hyg. Occup. Dis. 2014, 4, 274–276. [Google Scholar]
- Bener, A. Health status and working condition of migrant workers: Major public health problems. Int. J. Prev. Med. 2017, 8, 68. [Google Scholar] [CrossRef]
- Dodd, W.; Humphries, S.; Patel, K.; Majowicz, S.; Little, M.; Dewey, C. Determinants of internal migrant health and the healthy migrant effect in South India: A mixed methods study. BMC Int. Health Hum. Rights 2017, 1, 23. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Luo, Z.; Wang, J.; Zhong, J.; Wang, P. Health-Related Quality of Life and Health Service Utilization in Chinese Rural-to-Urban Migrant Workers. Int. J. Environ. Res. Public Health 2015, 12, 2205–2214. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Qian, Y. Native-immigrant occupational segregation and worker health in the United States, 2004–2014. Soc. Sci. Med. 2017, 183, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Yu, W.; Chen, S.; Zhang, D.; Tan, R. Influence of Social Support on Health-Related Quality of Life in New-Generation Migrant Workers in Eastern China. Iran J. Public Health 2013, 8, 806–812. [Google Scholar]
- Chen, H.; Zhu, Z.; Sun, D.; Wang, X. The Physical and Psychological Health of Migrants in Guangzhou, China: How Does Neighborhood Matter? Inquiry 2016, 53. [Google Scholar] [CrossRef] [PubMed]
- Di Fabio, A.; Bucci, O. Green positive guidance and green positive life counseling for decent work and decent lives: Some empirical results. Front. Psychol. 2016, 7, 261. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year of Publication | Country of Publication | Type of Study | Score |
|---|---|---|---|---|
| Al Hosani F. et al. | 2013 | Arab Emirates | Cross sectional | N.6 |
| Al Rifai R. et al. | 2015 | Japan | Cross sectional | N.8 |
| Anjara S. G. et al. | 2017 | Malesia | Cross sectional | N.7 |
| Arcury T. et al. | 2013 | America | Review | I.4 |
| Banerjee M. et al. | 2015 | India | Cross sectional | N.6 |
| Bener A. | 2017 | Arab Emirates | Cross sectional | N.6 |
| Bhandari P. et al. | 2016 | Korea | Cross sectional | N.7 |
| Bi Y. et al. | 2016 | China | Cross sectional | N.7 |
| Biering K. et al. | 2016 | Denmark | Cross sectional | N.6 |
| Brumitt J. et al. | 2013 | America | Cross sectional | N.6 |
| Castaneda S. et al. | 2015 | America | Cross sectional | N.7 |
| Chen H. et al. | 2016 | China | Cross sectional | N.5 |
| Chen W. et al. | 2016 | China | Trial | J.4 |
| Dafalla A. et al. | 2017 | Arab Emirates | Cross sectional | N.7 |
| Dodd V. et al. | 2016 | America | Cross sectional | N.5 |
| Dodd W. et al. | 2017 | South India | Cross sectional | N.6 |
| Earle-Richardson G. et al. | 2014 | America | Case control | N.6 |
| Fan W. et al. | 2017 | America | Cross sectional | N.7 |
| Fernandez B. | 2018 | Australia | Review | I.5 |
| Fitzgerald S. et al. | 2017 | China | Review | A.7 |
| Fonseca A. et al. | 2017 | Portugal | Cross sectional | N.5 |
| Gao X. F. et al. | 2015 | China | Cross sectional | N.6 |
| Goldenberg S. M. et al. | 2018 | America | Cross sectional | N.5 |
| Habib R. R. et al. | 2016 | Lebanon | Cross sectional | N.6 |
| Hsieh Y. C. et al. | 2016 | America | Cross sectional | N.7 |
| Jensen M. T. et al. | 2015 | Norway | Cross sectional | N.6 |
| Khongthanachayopit S. et al. | 2017 | Thailand | Cross sectional | N.7 |
| Kumparatana P. et al. | 2017 | America | Cross sectional | N.7 |
| Lee W. S. et al. | 2017 | China | Cross sectional | N.7 |
| Lee H. et al. | 2017 | Korea | Trial | J.3 |
| Leng A. et al. | 2016 | China | Cross sectional | N.5 |
| Li W. et al. | 2016 | China | Trial | J.3 |
| Li Y. et al. | 2013 | China | Case report | |
| Lu C. et al. | 2015 | China | Cross sectional | N.7 |
| Lu C. et al. | 2014 | China | Cross sectional | N.7 |
| Lu L. et al. | 2014 | China | Cross sectional | N.7 |
| Mannocci A. et al. | 2016 | Italy | Cohort study | N.7 |
| Martin M. et al. | 2016 | America | Cross sectional | N.7 |
| Mendelsohn J. et al. | 2015 | China | Trial | J.3 |
| Modesti P. et al. | 2017 | Italy | Cross sectional | N.6 |
| Ning C. et al. | 2013 | China | Cohort study | N.8 |
| Norris A. et al. | 2017 | America | Cross sectional | N.7 |
| Perez-Carceles M. D. et al. | 2014 | Spain | Cross sectional | N.7 |
| Pichardo-Geisinger R. et al. | 2013 | America | Cross sectional | N.7 |
| Rodriguez G. et al. | 2016 | America | Cross sectional | N.5 |
| Ronda E. et al. | 2015 | Spain | Cross sectional | N.3 |
| Sabhlok A. et al. | 2015 | India | Review | I.4 |
| Sanchez J. et al. | 2013 | America | Trial | J.3 |
| Sadarangani S. et al. | 2017 | Malesia | Review | A.4 |
| Salyer S. J. et al. | 2014 | America | Cross sectional | N.6 |
| Shah S. et al. | 2017 | Arab Emirates | Cross sectional | N.7 |
| Shah S. et al. | 2015 | Arab Emirates | Cross sectional | N.7 |
| Shah S. et al. | 2015 | Arab Emirates | Cross sectional | N.7 |
| Simkhada P. P. et al. | 2017 | UK | Review | I.7 |
| Skogberg N. et al. | 2017 | Finland | Cross sectional | N.7 |
| Taha H. A. et al. | 2013 | Arab Emirates | Cross sectional | N.6 |
| Tam W. et al. | 2017 | Malesia | Cross sectional | N.4 |
| Thomas B. et al. | 2014 | South India | Cross sectional | N.7 |
| Urmi A. Z. et al. | 2015 | Bangladesh | Cross sectional | N.7 |
| Varadharajan K. et al. | 2013 | India | Cross sectional | N.7 |
| Vernier M. et al. | 2013 | France | Cohort study | N.5 |
| Wang D et al. | 2015 | China | Case report | |
| Wang P. et al. | 2015 | China | Cross sectional | N.7 |
| Wangroongsarb P. et al. | 2016 | Thailand | Cross sectional | N.7 |
| Xing H. et al. | 2013 | China | Case control | N.6 |
| Yan S. et al. | 2016 | China | Cross sectional | N.6 |
| Yang H. et al. | 2015 | China | Cross sectional | N.7 |
| Yang H. et al. | 2017 | China | Cross sectional | N.7 |
| Authors | Year | Type of Study | Diseases | Workers’ Categories | Score |
|---|---|---|---|---|---|
| Arcury T. et al. | 2013 | Review | Injury, illnesses, pesticides | Agriculture, forestry and fishing sector workers | I.4 |
| Fernandez B. | 2018 | Review | Pregnancy, injuries, illnesses | Domestic workers | I.5 |
| Fitzgerald S. et al. | 2017 | Review | Work injuries | Construction and manual labor workers; employees | A.7 |
| Sabhlok A et al. | 2015 | Review | Respiratory diseases, injuries | Road workers | I.4 |
| Sadarangani S. et al. | 2017 | Review | Infectious diseases | Employees and domestic workers | A.4 |
| Simkhada P. P. et al. | 2017 | Review | Sexual risks, injuries, alcohol, drugs | Employees and agricultural workers | I.7 |
| Chen W. et al. | 2016 | Trial | Organic solvent exposure | Employees | J.4 |
| Lee H. et al. | 2017 | Trial | Cardiovascular risk | Employees | J.3 |
| Li W. et al. | 2016 | Trial | Malaria | Staff members of company | J.3 |
| Mendelsohn J. et al. | 2015 | Trial | Sexual infections | Construction workers | J.3 |
| Sanchez J. et al. | 2013 | Trial | Sexual infections | Agricultural workers | J.3 |
| Xing H. et al. | 2013 | Case control | Quality of life | Shoe factory, textile, domestic, construction, and transport workers | N.6 |
| Earle-Richardson G. et al. | 2014 | Case control | Eye irritations | Farm workers | N.6 |
| Li Y. et al. | 2013 | Case report | Malaria | Not specified | Not applicable |
| Wang D. et al. | 2015 | Case report | Infectious diseases | Not specified | Not applicable |
| Vernier M. et al. | 2013 | Cohort study | Hepatitis | Employees | N.5 |
| Ning C. et al. | 2013 | Cohort study | Sexual infections | Construction and mining workers | N.8 |
| Mannocci A. et al. | 2016 | Cohort study | Cardiometabolic diseases | Oil and gas workers | N.7 |
| Authors | Year | Type of Study | Diseases | Job Categories | Score |
|---|---|---|---|---|---|
| Al Hosani F. et al. | 2013 | Cross sectional | Tuberculosis | Office workers, drivers, domestic workers, food handlers, etc. | N.6 |
| Al Rifai R. et al. | 2015 | Cross sectional | Sexual infections | Domestic multinational workers | N.8 |
| Anjara S. G. et al. | 2017 | Cross sectional | Lower quality of life | Domestic workers | N.7 |
| Banerjee M. et al. | 2015 | Cross sectional | Dermatologic and respiratory problems | Construction workers | N.6 |
| Bener A. | 2017 | Cross sectional | BMI, smoke, pain, cardiovascular, and gastrointestinal diseases | Construction and agricultural workers; drivers | N.6 |
| Bhandari P. et al. | 2016 | Cross sectional | Perceived health, physical activity | Manual laborers; domestic, construction, and office workers; others | N.7 |
| Bi Y. et al. | 2016 | Cross sectional | Diabetes | Manufacturing, construction, services, and accommodation workers | N.7 |
| Biering K. et al. | 2016 | Cross sectional | Work injuries | Employees | N.6 |
| Brumitt J. et al. | 2013 | Cross sectional | Tobacco smoke/physical activity | Seasonal farm workers | N.6 |
| Castaneda S. et al. | 2015 | Cross sectional | Cardiovascular diseases | Seasonal farm workers | N.7 |
| Chen H. et al. | 2016 | Cross sectional | Quality of life | Government and private enterprise workers; employees | N.5 |
| Dafalla A. et al. | 2017 | Cross sectional | Infectious diseases | Food handlers, babysitters, housemaids, drivers | N.7 |
| Dodd V. et al. | 2016 | Cross sectional | Oral cancer | Farm workers | N.5 |
| Dodd W. et al. | 2017 | Cross sectional | Musculoskeletal disorders, infective diseases, skin problems | Construction, textile sector, and manufacturing workers | N.6 |
| Fan W. Et al. | 2017 | Cross sectional | Lower quality of life | Agricultural, textile, and construction workers | N.7 |
| Fonseca A. et al. | 2017 | Cross sectional | Malaria and endocrine, metabolic, cardiovascular, and respiratory diseases | Directors, managers, and specialists in scientific activities | N.5 |
| Gao X. F. et al. | 2015 | Cross sectional | Tuberculosis | Employees | N.6 |
| Goldenberg S. M. et al. | 2018 | Cross sectional | Infectious diseases, alcohol abuse | Migrant sex workers | N.5 |
| Habib R. R. et al. | 2016 | Cross sectional | Respiratory, digestive, and musculoskeletal disorders | Farm workers | N.6 |
| Hsieh Y. C. et al. | 2016 | Cross sectional | Dermatologic and musculoskeletal problems | Housekeepers | N.7 |
| Jensen M. T. et al. | 2015 | Cross sectional | Muscle pain, gastric discomfort | Business travelers | N.6 |
| Khongthanachayopit S. et al. | 2017 | Cross sectional | Musculoskeletal disorders, diabetes, hypertension, allergies | Agriculture sector workers, employees in restaurant/factory | N.7 |
| Kumparatana P. et al. | 2017 | Cross sectional | Lower health, alcohol | Employees | N.7 |
| Lee W. S. et al. | 2017 | Cross sectional | BMI | Agricultural workers | N.7 |
| Leng A. et al. | 2016 | Cross sectional | Hepatitis B | Rural workers | N.5 |
| Lu C. et al. | 2015 | Cross sectional | Chronic diseases | Factory employees | N.7 |
| Lu C. et al. | 2014 | Cross sectional | BMI | Textile factory employees | N.7 |
| Lu L. et al. | 2014 | Cross sectional | Quality of life | Factory employees | N.7 |
| Martin M. et al. | 2016 | Cross sectional | Cardio-metabolic diseases | Sales, agricultural, forestry, and manufacturing workers; administrators | N.7 |
| Modesti P. et al. | 2017 | Cross sectional | Type 2 diabetes | Textile employees, managers, students, housekeepers | N.6 |
| Norris A. et al. | 2017 | Cross sectional | HIV | Employees | N.7 |
| Perez-Carceles M. D. et al. | 2014 | Cross sectional | Hazardous drinking | Construction industry and agricultural workers | N.7 |
| Pichardo-Geisinger R. et al. | 2013 | Cross sectional | Dermatologic problems | Manual and poultry workers | N.7 |
| Rodriguez G. et al. | 2016 | Cross sectional | Pain, stress, blood pressure | Employees in service, production and office support | N.5 |
| Ronda E. et al. | 2015 | Cross sectional | Muscle pain, headaches, gastric discomfort | Employees and domestic and construction workers | N.3 |
| Salyer S. J. et al. | 2014 | Cross sectional | Infectious diseases | Non-governmental organization workers | N.6 |
| Shah S. et al. | 2017 | Cross sectional | Diabetes | Employees | N.7 |
| Shah S. et al. | 2015 | Cross sectional | Obesity and cardiovascular risk | Employees | N.7 |
| Shah S. et al. | 2015 | Cross sectional | Hypertension | Drivers, construction and agriculture workers, salesmen, office workers, tailors, cooks | N.7 |
| Skogberg N. et al. | 2017 | Cross sectional | Metabolic syndrome | Employees | N.7 |
| Taha H. A. et al. | 2013 | Cross sectional | Infectious diseases | Farmers, food handlers, shepherds, drivers, housemaids | N.6 |
| Tam W. et al. | 2017 | Cross sectional | Influenza, gastritis, cancer, accidents | Manual workers | N.4 |
| Thomas B. et al. | 2014 | Cross sectional | Chest symptoms | Brick kiln workers | N.7 |
| Urmi A. Z. et al. | 2015 | Cross sectional | Sexual infections | Employees | N.7 |
| Varadharajan K. et al. | 2013 | Cross sectional | Obesity | Professional, technical, managerial, sales, services, and manual labor workers | N.7 |
| Wang P. et al. | 2015 | Cross sectional | Lifestyle behaviors | Service sector and construction workers; managers | N.7 |
| Wangroongsarb P. et al. | 2016 | Cross sectional | Malaria | Agricultural, domestic, factory, and fisheries workers | N.7 |
| Yan S. et al. | 2016 | Cross sectional | Diabetes | Not specified | N.6 |
| Yang H. et al. | 2015 | Cross sectional | BMI | Manufacturing, construction, hospitality, domestic, small business, and recreation workers | N.7 |
| Yang H. et al. | 2017 | Cross sectional | Lifestyle behaviors | Manufacturing, construction, hospitality, domestic, small business, and recreation workers | N.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mucci, N.; Traversini, V.; Giorgi, G.; Garzaro, G.; Fiz-Perez, J.; Campagna, M.; Rapisarda, V.; Tommasi, E.; Montalti, M.; Arcangeli, G. Migrant Workers and Physical Health: An Umbrella Review. Sustainability 2019, 11, 232. https://doi.org/10.3390/su11010232
Mucci N, Traversini V, Giorgi G, Garzaro G, Fiz-Perez J, Campagna M, Rapisarda V, Tommasi E, Montalti M, Arcangeli G. Migrant Workers and Physical Health: An Umbrella Review. Sustainability. 2019; 11(1):232. https://doi.org/10.3390/su11010232
Chicago/Turabian StyleMucci, Nicola, Veronica Traversini, Gabriele Giorgi, Giacomo Garzaro, Javier Fiz-Perez, Marcello Campagna, Venerando Rapisarda, Eleonora Tommasi, Manfredi Montalti, and Giulio Arcangeli. 2019. "Migrant Workers and Physical Health: An Umbrella Review" Sustainability 11, no. 1: 232. https://doi.org/10.3390/su11010232
APA StyleMucci, N., Traversini, V., Giorgi, G., Garzaro, G., Fiz-Perez, J., Campagna, M., Rapisarda, V., Tommasi, E., Montalti, M., & Arcangeli, G. (2019). Migrant Workers and Physical Health: An Umbrella Review. Sustainability, 11(1), 232. https://doi.org/10.3390/su11010232