Scheduling Optimization of Home Health Care Service Considering Patients’ Priorities and Time Windows


Abstract
:1. Introduction
2. Literature Review
3. The Scheduling Optimization Model
3.1. Problem Definition
3.2. Mathematical Programming Model
- (1)
- Only one type of service is required by each patient per time;
- (2)
- The time that it takes the doctors to reach any two patients respectively is the same;
- (3)
- Service will be started immediately after the medical staff arrive at the patients’ homes;
- (4)
- Medical staff are enough to meet all demands.
- i represents the previous service-required place (departure place);
- j represents the next service-required place (destination) (i, j ∈ P = {0, 1, …, n};
- 0 represents the service center;
- h represents the medical staff (h = 1, …, H);
- k represents the type of service (k = 1, …, K);
- c1ij represents the travel cost from place i to place j to provide service to patients;
- c2hk represents the cost for medical staff h to provide the k-th service;
- tij represents the travel time from service center i to service-required place j;
- τj represents the execution time of the service required by the j-th patient;
- wi represents the required waiting time of the service personnel arriving at service nodes early;
- ei represents that patient i can accept the earliest starting time;
- li represents that the patient can accept the latest starting time, which constitutes the time window requirements of the provision of each patient service;
- Si represents the time that the medical staff take to reach service-required place i, and S1 = e1;
- Di represents the time that the medical staff take to leave service-required place i; , in which ei represents the earliest starting time accepted by the i-th patient; li represents the latest starting time accepted by the i-th patient;
- yjhk represents whether the service k can be provided by the medical staff h for the service-required place j (0: no, 1: yes), and yjhk is the input parameter;
- rij represents whether the service-required place j has priority over the service-required place i (0: yes, 1: no), and rij is the input parameter that can be determined in advance;
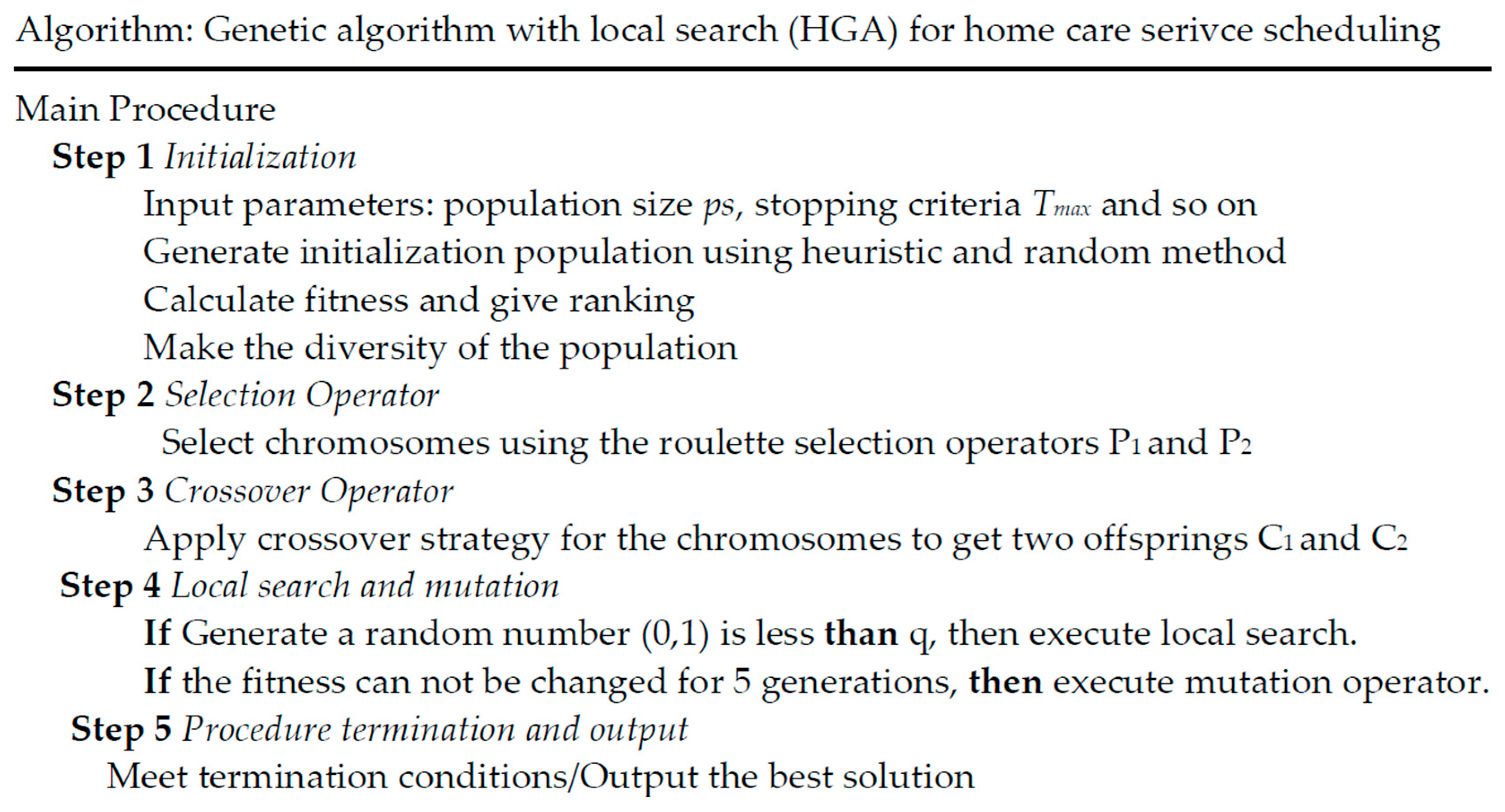
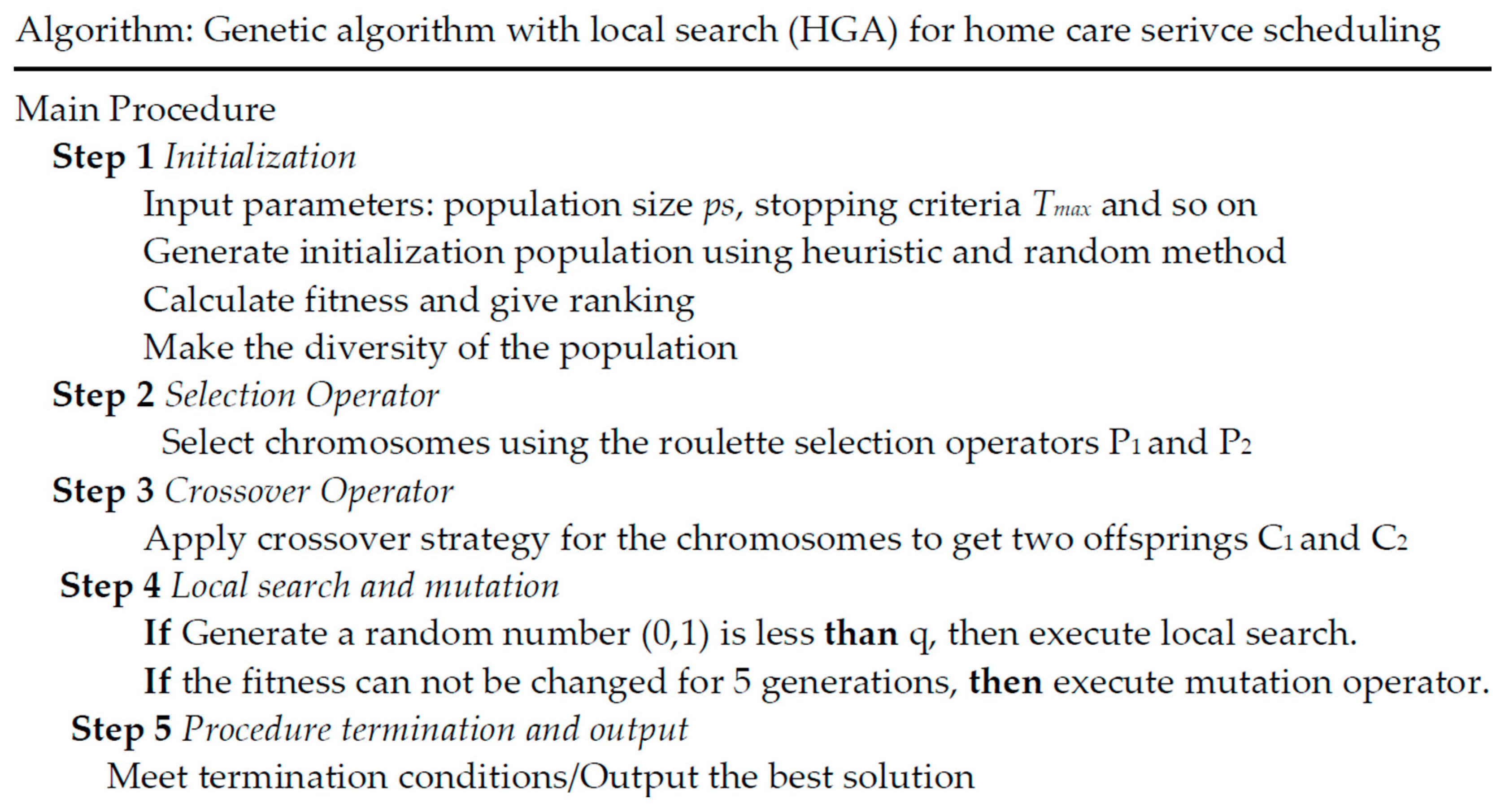
4. The Genetic Algorithm with Local Search
- Before crossing:Parent Generation A: 872,139 | 546Parent Generation B: 983 | 567,142
- After crossing:Filial Generation A: 721,546 | 983Filial Generation B: 546 | 983,712
- (1)
- It has reached the predefined evolution generations, namely 3000 generations.
- (2)
- The best individual of the population cannot obtain more improvements in 200 consecutive generations.
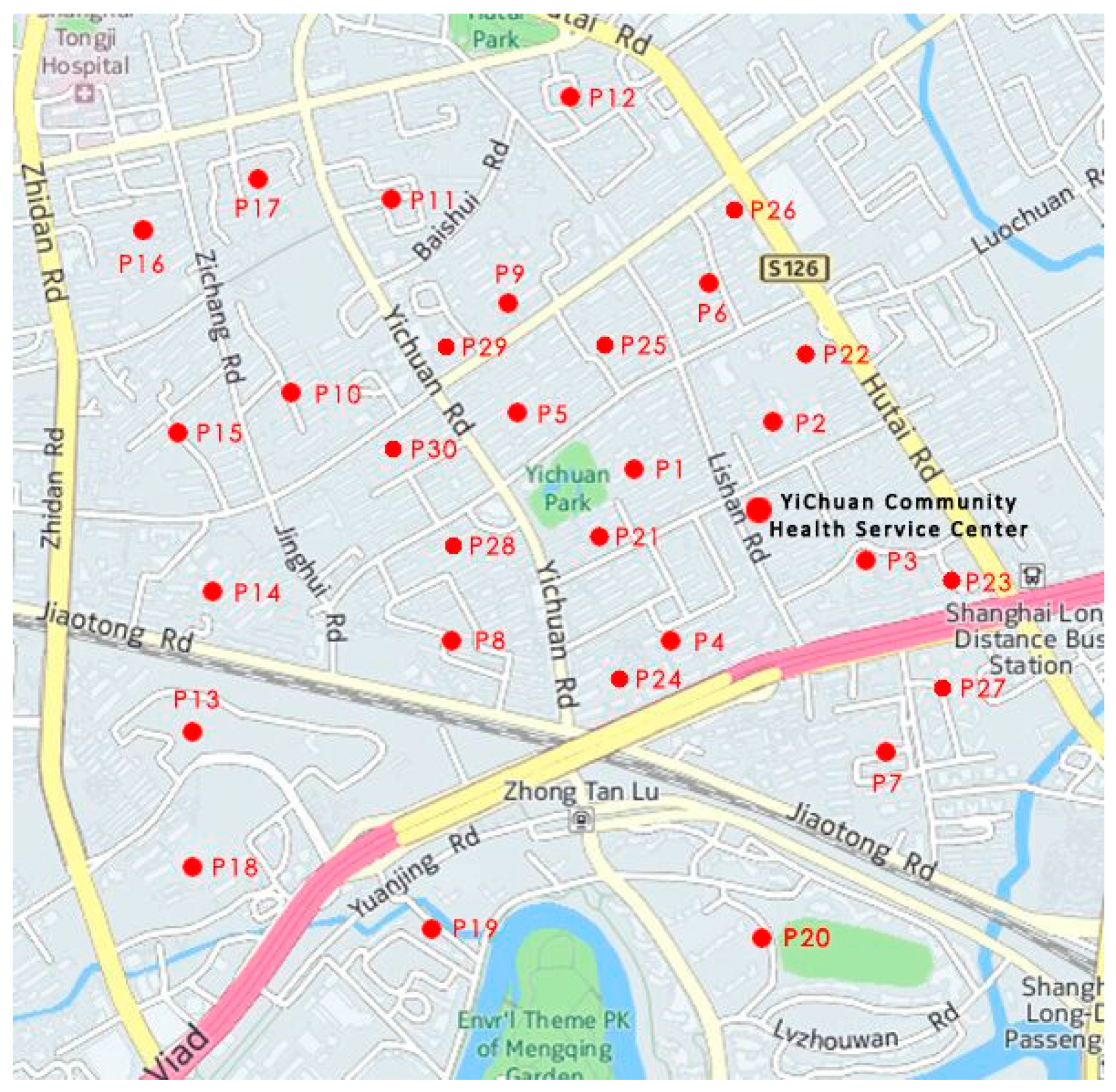
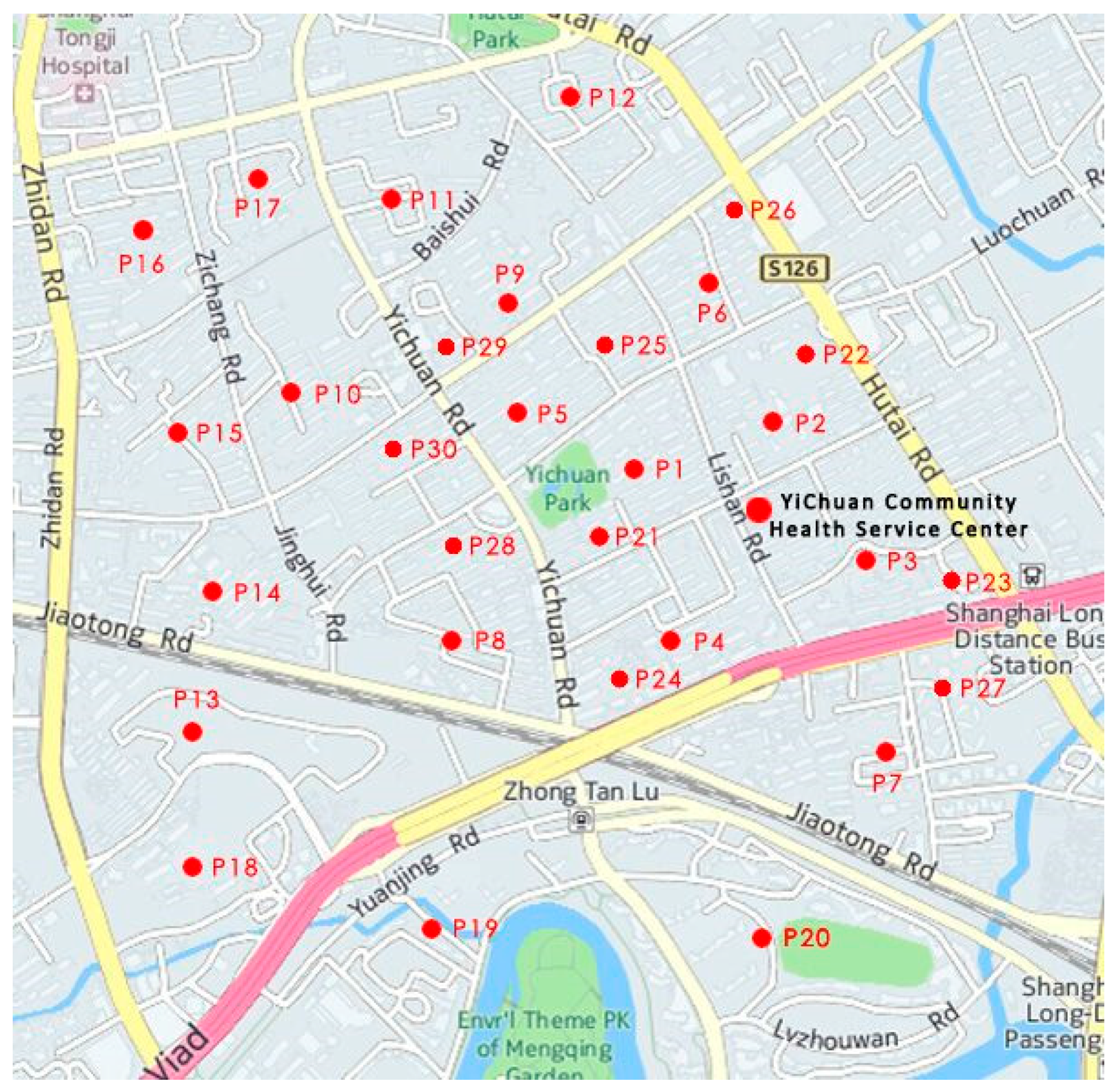
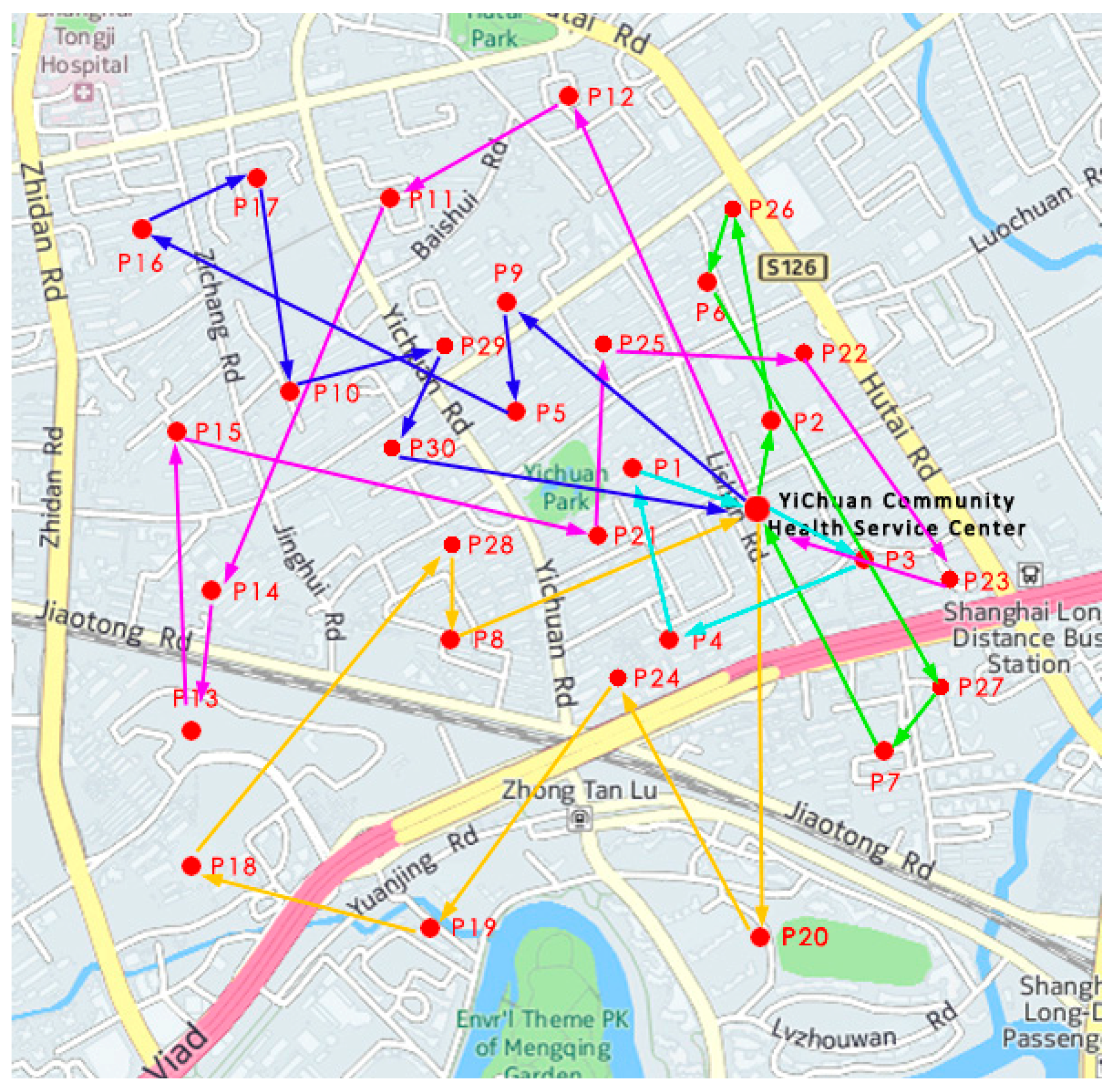
5. Empirical Analysis
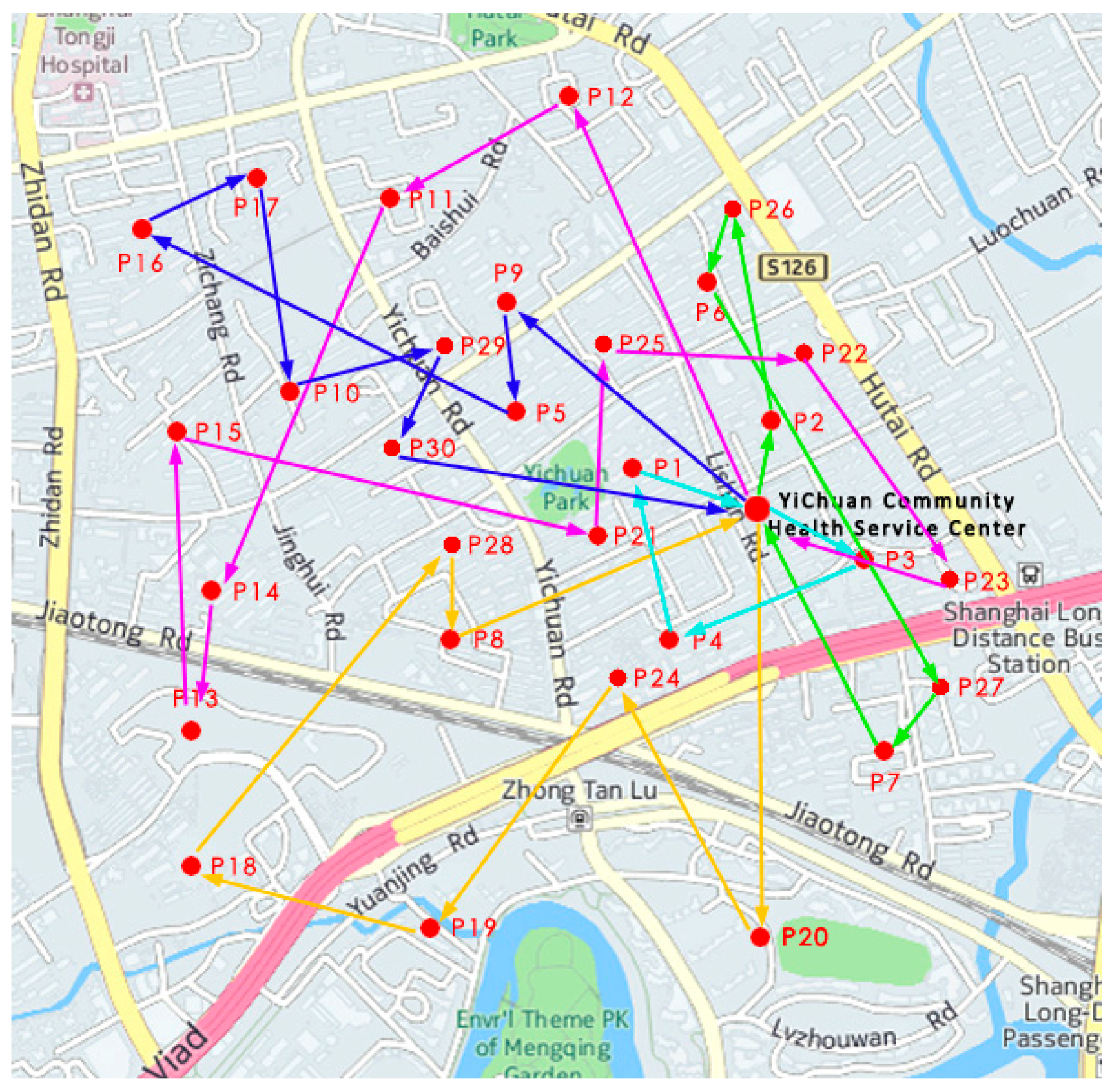
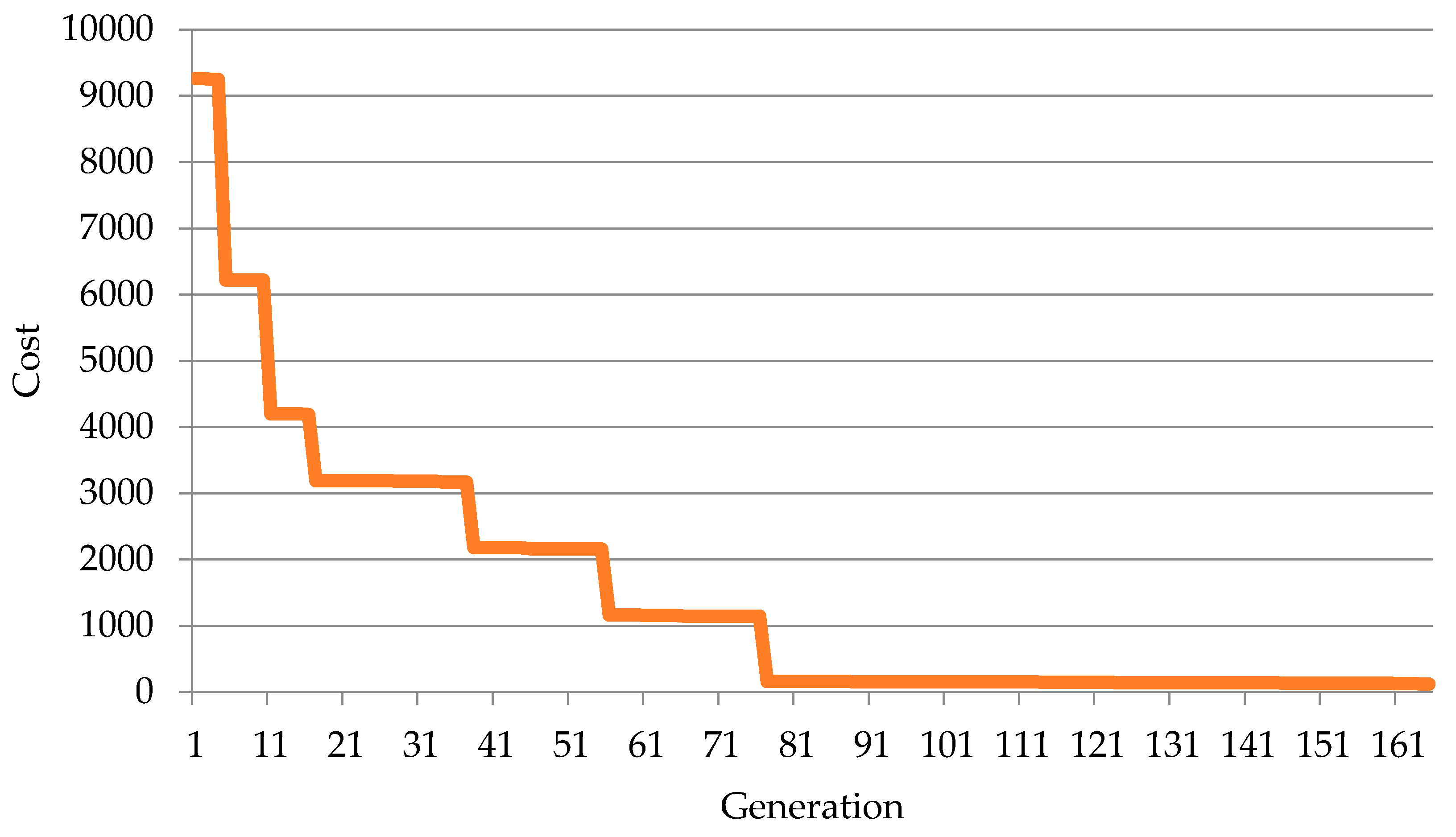
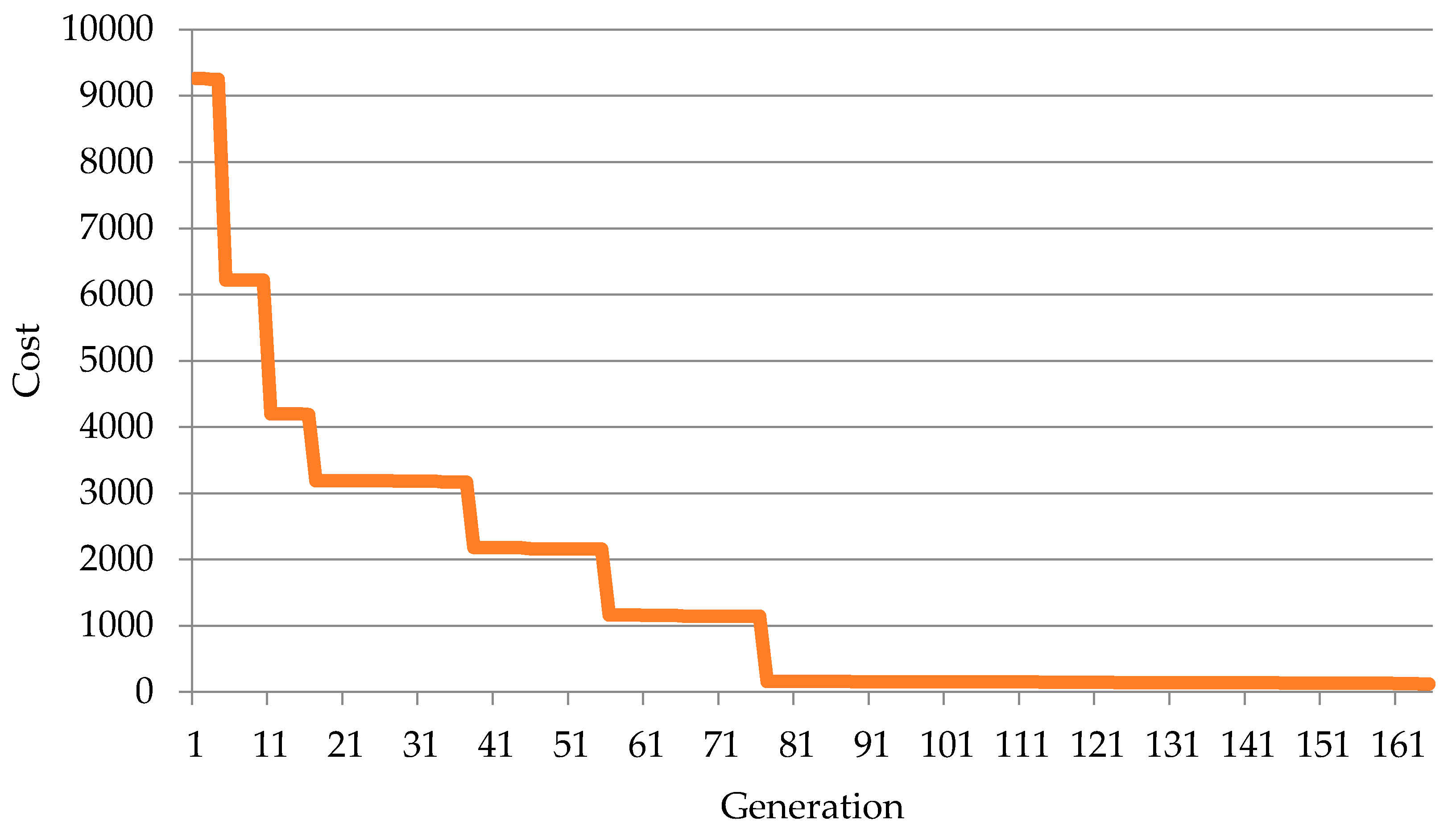
5.1. The Analysis of the Calculation Results
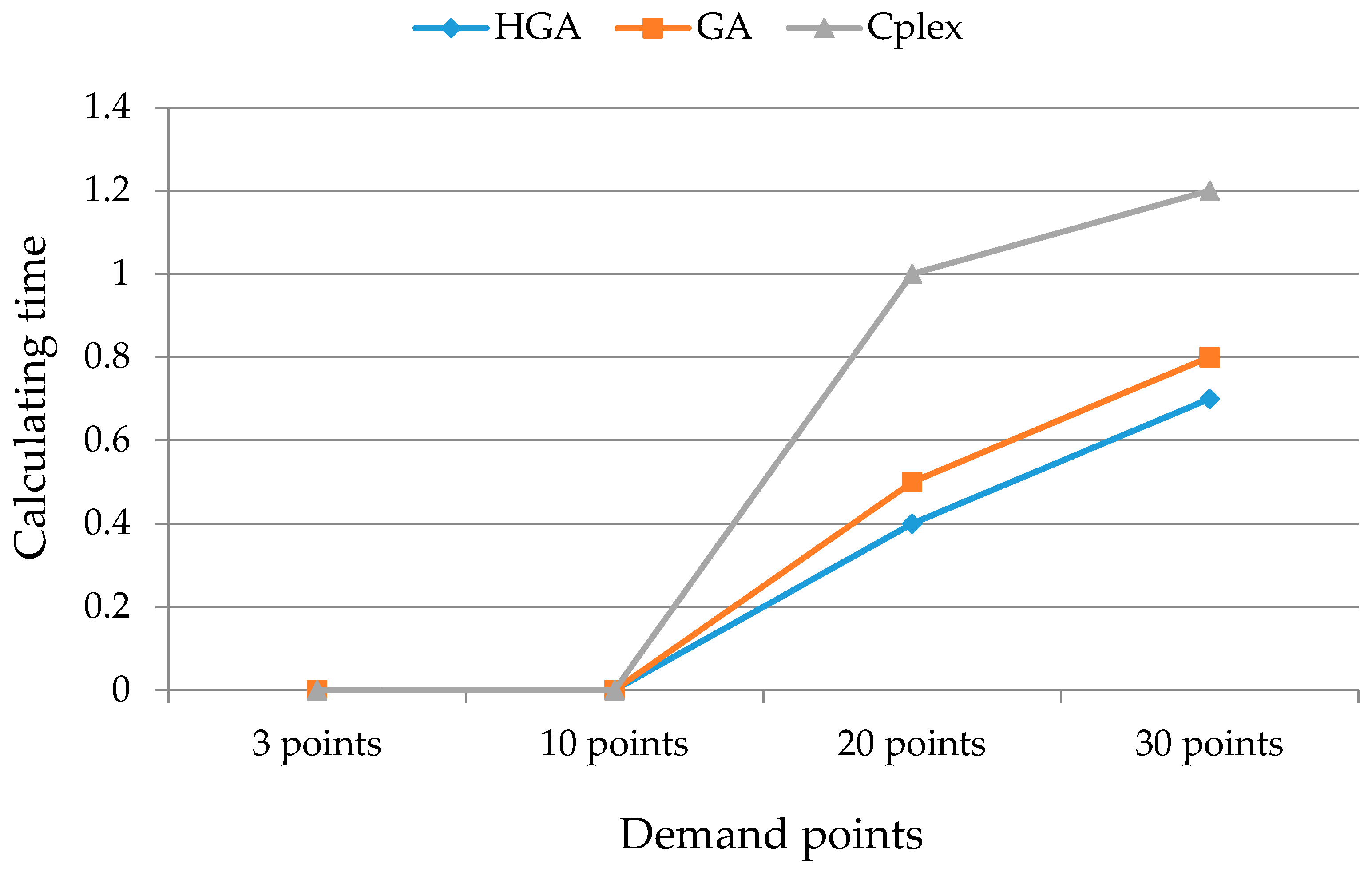
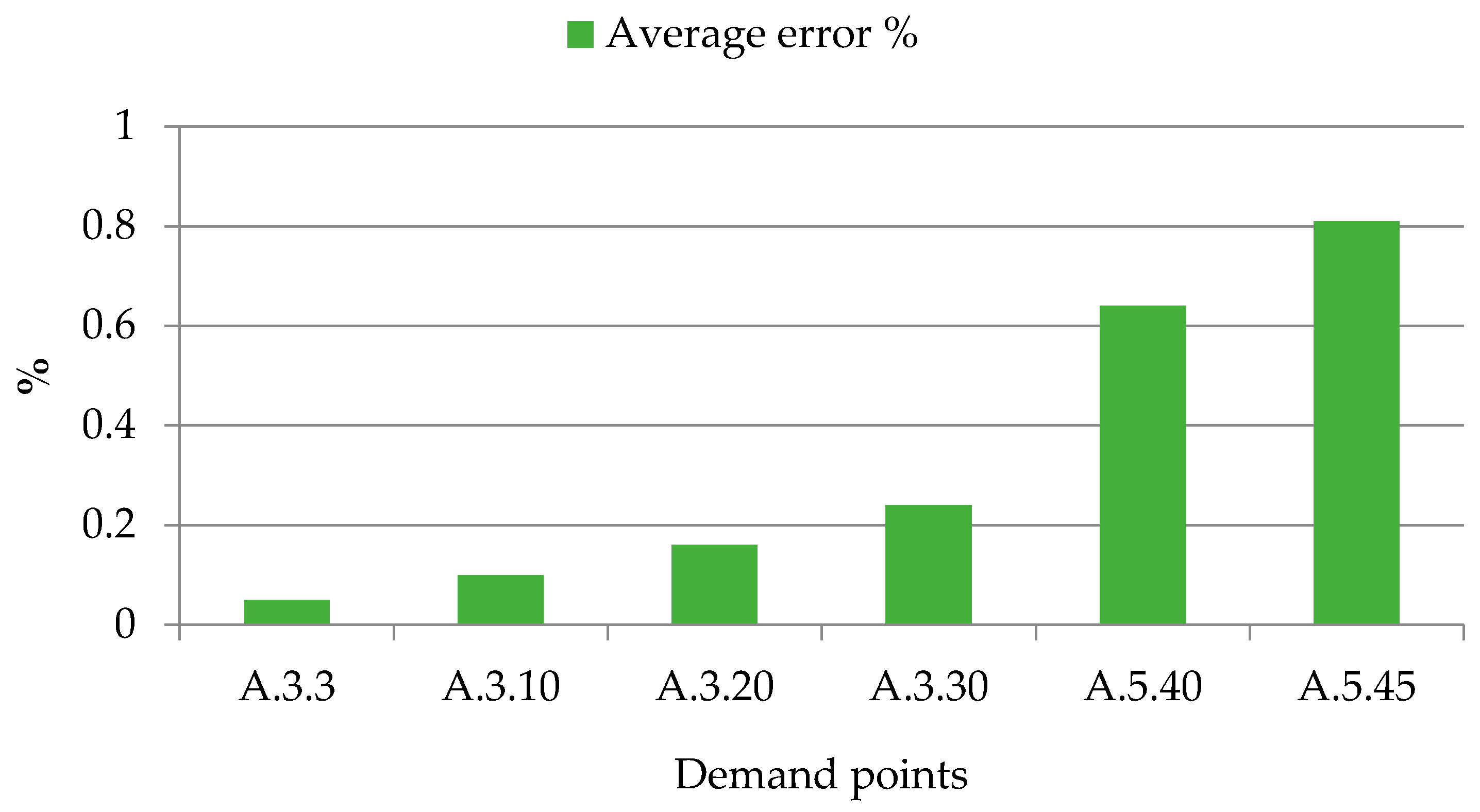
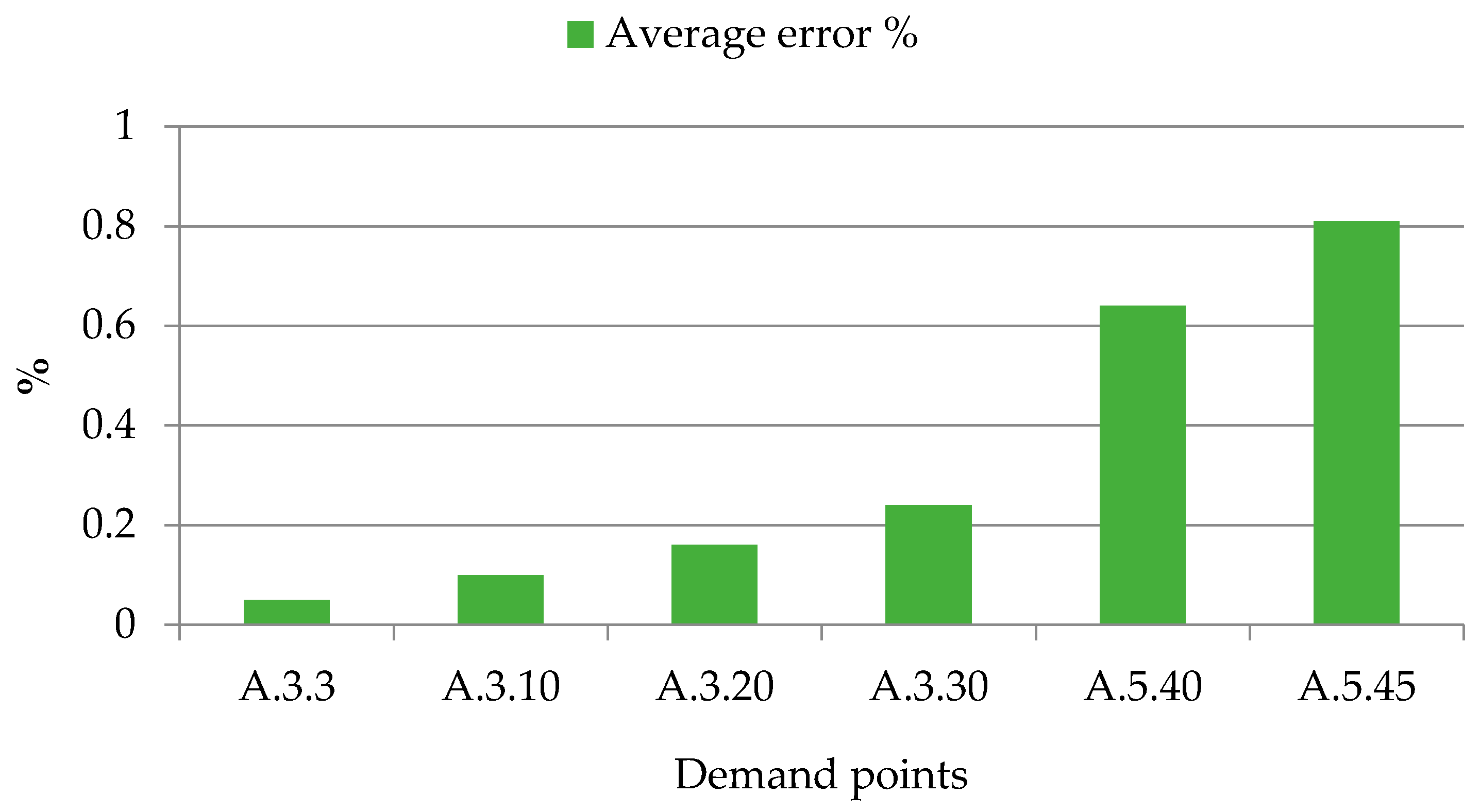
5.2. Comparisons of Schedules’ Quality
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chahed, S.; Matta, A.; Sahin, E.; Dallery, Y. Operations Management Related Activities for Home Health Care Providers. Available online: http://www.sciencedirect.com/science/article/pii/S1474667015360456 (accessed on 10 February 2017).
- Eveborn, P.; Flisberg, P.; Ronnqvist, M. LAPS CARE-an operational system for staff planning of home care. Eur. J. Oper. Res. 2006, 171, 962–976. [Google Scholar] [CrossRef]
- Eveborn, P.; Ronnqvist, M.; Einarsdottir, H.; Eklund, M.; Liden, K.; Almroth, M. Operations research improves quality and efficiency in home care. Interfaces 2009, 39, 18–34. [Google Scholar] [CrossRef]
- Bertels, S.; Fahle, T. A hybrid setup for a hybrid scenario: Combining heuristics for the home health care problem. Comput. Oper. Res. 2006, 33, 2866–2890. [Google Scholar] [CrossRef]
- Thomsen, K. Optimization on Home Care. Thesis in Informatics and Mathematical Modeling; Technical University of Denmark Copenhagen: Lyngby, Denmark, 2006. [Google Scholar]
- Bennett, A.; Erera, A. Dynamic periodic fixed appointment scheduling for home health. IIE Trans. Healthc. Syst. Eng. 2011, 1, 6–19. [Google Scholar] [CrossRef]
- Bard, J.F.; Purnomo, H.W. Preference scheduling for nurses using column generation. Eur. J. Oper. Res. 2005, 164, 510–534. [Google Scholar] [CrossRef]
- Bard, J.F.; Purnomo, H.W. Cyclic preference scheduling of nurses using a Lagrangian-based heuristic. J. Sched. 2007, 10, 5–23. [Google Scholar] [CrossRef]
- Beliën, J.; Demeulemeester, E. A branch-and-price approach for integrating nurse and surgery scheduling. Eur. J. Oper. Res. 2008, 189, 652–668. [Google Scholar] [CrossRef]
- Punnakitikashem, P.; Rosenberger, J.; Behan, D. Stochastic programming for nurse assignment. Comput. Opt. Appl. 2008, 40, 321–349. [Google Scholar] [CrossRef]
- Hertz, A.; Lahrichi, N. A patient assignment algorithm for home care services. J. Oper. Res. Soc. 2009, 60, 481–495. [Google Scholar] [CrossRef]
- Brunner, J.O.; Bard, J.F.; Kolisch, R. Flexible shift scheduling of physicians. Health Care Manag. Sci. 2009, 12, 285–305. [Google Scholar] [CrossRef]
- Brunner, J.O.; Bard, J.F.; Kolisch, R. Midterm scheduling of physicians with flexible shifts using branch and price. IIE Trans. 2010, 43, 84–109. [Google Scholar] [CrossRef]
- Taylor, G.; McClean, S. Geriatric-patient flowrate modeling. IMA J. Math. Appl. Med. Biol. 1996, 13, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.; McClean, S.I.; Millard, P.H. Continuous-time Markov models for geriatric patient behaviour. Appl. Stoch. Models Data Anal. 1997, 13, 315–323. [Google Scholar] [CrossRef]
- Taylor, G.J.; McClean, S.I.; Millard, P.H. Stochastic models of geriatric patient bedoccupancy behavior. J. R. Stat. Soc. Ser. A 2000, 163, 39–48. [Google Scholar] [CrossRef]
- McClean, S.I.; McAlea, B.; Millard, P.H. Using a Markov reward model to estimate spend-down costs for a geriatric department. J. Oper. Res. Soc. 1998, 49, 1021–1025. [Google Scholar] [CrossRef]
- McClean, S.I.; Millard, P.H. A three compartment model of the patient flows in a geriatric department: A decision support approach. Health Care Manag. Sci. 1998, 1, 159–163. [Google Scholar] [CrossRef] [PubMed]
- McClean, S.I.; Millard, P.H. Where to treat the older patient? Can Markov models help us better understand the relationship between hospital and community care? J. Oper. Res. Soc. 2007, 58, 255–261. [Google Scholar] [CrossRef]
- Congdon, P. The development of Gravity models for hospital patient flows under system change: A Bayesian modelling approach. Health Care Manag. Sci. 2001, 4, 289–304. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.H.; Mcclean, S.I.; Shapcott, C.M.; Millard, P.H. Modelling patient duration of stay to facilitate resource management of geriatric hospitals. Health Care Manag. Sci. 2002, 5, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.H.; McClean, S.I. Using coxian phase-type distributions to identify patient characteristics for duration of stay in hospital. Health Care Manag. Sci. 2004, 7, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.; Vasilakis, C.; El-Darzi, E. Length of stay-based patient flow models: Recent developments and future directions. Health Care Manag. Sci. 2005, 8, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Krahn, M. Estimating the prognosis of hepatitis C patients infected by transfusion in Canada between 1986 and 1990. Med. Decis. Mak. 2004, 24, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, N.; Kuno, E.; Smith, T.E. Modelling patient flows using a queuing network with blocking. Health Care Manag. Sci. 2005, 8, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Borsani, V.; Matta, A.; Beschi, G.; Sommaruga, F. A Home Care Scheduling Model for Human Resources. Available online: http://ieeexplore.ieee.org/abstract/document/4114475/ (accessed on 5 February 2017).
- Kergosien, Y.; Lenté, C.; Billaut, J.-C. Home health care problem an extended multiple Traveling Salesman Problem. In Proceedings of the Multidisciplinary International Conference on Scheduling: Theory and Applications (MISTA 2009), Dublin, Ireland, 10–12 August 2009; pp. 85–92.
- Bachouch, R.B.; Guinet, A.; Hajri-Gabouj, S. An Optimization Model for Task Assignment in Home Health Care. Available online: http://ieeexplore.ieee.org/abstract/document/5441277/ (accessed on 5 February 2017).
- Lanzarone, E.; Matta, A.; Scaccabarozzi, G. A patient stochastic model to support human resource planning in home care. Prod. Plan. Control 2010, 21, 3–25. [Google Scholar] [CrossRef]
- Triki, N.; Garaix, T.; Xie, X. A two-phase approach for periodic home health care planning. In Proceedings of the 2014 IEEE International Conference on Automation Science and Engineering (CASE), Taipei, Taiwan, 18–22 August 2014; pp. 518–523.
- Liu, R.; Xie, X.; Augusto, V.; Rodriguez, C. Heuristic algorithms for a vehicle routing problem with simultaneous delivery and pickup and time windows in home health care. Eur. J. Oper. Res. 2013, 230, 475–486. [Google Scholar] [CrossRef]
- Liu, R.; Xie, X.; Garaix, T. Weekly Home Health Care Logistics. Available online: http://ieeexplore.ieee.org/abstract/document/6548751/ (accessed on 5 February 2017).
- Cappanera, P.; Scutella, M.G. Joint assignment, scheduling and routing models to Home Care optimization: A pattern based Approach. Transp. Sci. 2014, 49. [Google Scholar] [CrossRef]
- Koeleman, P.M.; Bhulai, S.; van Meersbergen, M. Optimal patient and personnel scheduling policies for care-at-home service facilities. Eur. J. Oper. Res. 2012, 219, 557–563. [Google Scholar] [CrossRef]
- Hiermann, G.; Prandtstetter, M.; Rendl, A.; Puchinger, J.; Raidl, G.R. Metaheuristics for Solving a Multimodal Home-Healthcare Scheduling Problem. Cent. Eur. J. Oper. Res. 2015, 23, 89–113. [Google Scholar] [CrossRef]
- Liu, R.; Xie, X.; Garaix, T. Hybridization of tabu search with feasible and infeasible local searches for periodic home health care logistics. Omega 2014, 47, 17–32. [Google Scholar] [CrossRef]
- Rasmussen, M.S.; Justesen, T.; Dohn, A.; Larsen, J. The home care crew scheduling problem: Preference-based visit clustering and temporal dependencies. Eur. J. Oper. Res. 2012, 219, 598–610. [Google Scholar] [CrossRef]
- Cappanera, P.; Scutella, M.G. Home Care optimization: Impact of pattern generation policies on scheduling and routing decisions. Electron. Notes Discret. Math. 2013, 41, 53–60. [Google Scholar] [CrossRef]
- Matta, A.; Chahed, S.; Sahin, E.; Dallery, Y. Modelling home care organisations from an operations management perspective. Flex. Serv. Manuf. J. 2014, 26, 295–319. [Google Scholar] [CrossRef]
- Yalcindag, S.; Matta, A.; Sahin, E. Operator assignment and routing problems in home health care services. In Proceedings of the 2012 IEEE International Conference on Automation Science and Engineering (CASE), Seoul, South Korea, 20–24 August 2012; pp. 329–334.
- Nickel, S.; Schröder, M.; Steeg, J. Mid-term and short-term planning support for home health care services. Eur. J. Oper. Res. 2012, 219, 574–587. [Google Scholar] [CrossRef]
- Lanzarone, E.; Matta, A.; Sahin, E. Operations Management Applied to Home Care Services: The Problem of Assigning Human Resources to Patients. IEEE Trans. Syst. Man Cybern. Part A 2012, 42, 1346–1363. [Google Scholar] [CrossRef]
- Yuan, B.; Liu, R.; Jiang, Z. Home Health Care Crew Scheduling and Routing Problem with Stochastic Service Times. In Proceedings of the 2014 IEEE International Conference on Automation Science and Engineering (CASE), Taipei, Taiwan, 18–22 August 2014; pp. 564–569.
- Akjiratikarl, C.; Yenradee, P.; Drake, P.R. PSO-based algorithm for home care worker scheduling in the UK. Comput. Ind. Eng. 2007, 53, 559–583. [Google Scholar] [CrossRef]
- Duque, P.A.M.; Castro, M.; Sörensen, K.; Goos, P. Home care service planning. The case of Landelijke Thuiszorg. Eur. J. Oper. Res. 2015, 243, 292–301. [Google Scholar] [CrossRef]
- Braekers, K.; Hartl, R.F.; Parragh, S.N.; Tricoire, F. A bi-objective home care scheduling problem: Analyzing the trade-off between costs and client inconvenience. Eur. J. Oper. Res. 2016, 248, 428–443. [Google Scholar] [CrossRef]
- Rest, K.D.; Hirsch, P. Daily scheduling of home health care services using time-dependent public transport. Flex. Serv. Manuf. J. 2016, 28, 1–31. [Google Scholar] [CrossRef]
- Redjem, R.; Marcon, E. Operations management in the home care services: A heuristic for the caregivers’ routing problem. Flex. Serv. Manuf. J. 2016, 28, 280–303. [Google Scholar] [CrossRef]
- Yalçındağ, S.; Matta, A.; Şahin, E.; Shanthikumar, J.G. The patient assignment problem in home health care: Using a data-driven method to estimate the travel times of care givers. Flex. Serv. Manuf. J. 2016, 28, 304–335. [Google Scholar] [CrossRef]
- Mankowska, D.S.; Meisel, F.; Bierwirth, C. The home health care routing and scheduling problem with interdependent services. Health Care Manag. Sci. 2014, 17, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Trautsamwieser, A.; Hirsch, P. Optimization of daily scheduling for home health care services. J. Appl. Oper. Res. 2011, 3, 124–136. [Google Scholar]
- Nguyen, T.V.L.; Montemanni, R. Mathematical programming models for home health care service optimisation. Int. J. Oper. Res. 2016, 25, 449–463. [Google Scholar] [CrossRef]
- Addis, B.; Carello, G.; Grosso, A.; Lanzarone, E.; Mattia, S. Handling uncertainty in health care management using the cardinality-constrained approach: Advantages and remarks. Oper. Res. Health Care 2015, 4, 1–4. [Google Scholar] [CrossRef]
- Bektas, T. The multiple traveling salesman problem: An overview of formulations and solution procedures. Omega 2006, 34, 209–219. [Google Scholar] [CrossRef]
- Gendreau, M.; Hertz, A.; Laporte, G.; Stan, M. A generalized insertion heuristic for the traveling salesman problem with time windows. Oper. Res. 1998, 46, 330–335. [Google Scholar] [CrossRef]
- Savelsbergh, M.W.P. Local search in routing problems with time windows. Ann. Oper. Res. 1985, 4, 285–305. [Google Scholar] [CrossRef]
- Ascheuer, N.; Fischetti, M.; Grötschel, M. Solving the asymmetric travelling salesman problem with time windows by branch-and-cut. Math. Program. 2001, 90, 475–506. [Google Scholar] [CrossRef]
- Goldberg, D.E.; Deb, K. A comparative analysis of selection schemes used in genetic algorithms. Found. Genet. Algorithms 1991, 1, 69–93. [Google Scholar]
- Jayalakshmi, G.A.; Sathiamoorthy, S.; Rajaram, R. A hybrid genetic algorithm—A new approach to solve traveling salesman problem. Int. J. Comput. Eng. Sci. 2001, 2, 339–355. [Google Scholar] [CrossRef]
- Lin, B.; Sun, X.; Salous, S. Solving travelling salesman problem with an improved hybrid genetic algorithm. J. Comput. Commun. 2016, 4, 98. [Google Scholar] [CrossRef]
- Snyder, L.V.; Daskin, M.S. A random-key genetic algorithm for the generalized traveling salesman problem. Eur. J. Oper. Res. 2006, 174, 38–53. [Google Scholar] [CrossRef]
- Larranaga, P.; Kuijpers, C.M.H.; Murga, R.H.; Dizdarevic, I.S. Genetic algorithms for the travelling salesman problem: A review of representations and operators. Artif. Intell. Rev. 1999, 13, 129–170. [Google Scholar] [CrossRef]
- Shahvari, O.; Salmasi, N.; Logendran, R.; Abbasi, B. An efficient tabu search algorithm for flexible flow shop sequence-dependent group scheduling problems. Int. J. Prod. Res. 2012, 50, 4237–4254. [Google Scholar] [CrossRef]
- Shahvari, O.; Logendran, R. Bi-Criteria Batch Scheduling on Unrelated-Parallel Machines. Available online: http://search.proquest.com/openview/885118ef4fbd523f3eb8b1ac18a674e7/1?pq-origsite=gscholar&cbl=51908 (accessed on 5 February 2017).
- Shahvari, O.; Logendran, R. Hybrid flow shop batching and scheduling with a bicriteria objective. Int. J. Prod. Econ. 2016, 179, 239–258. [Google Scholar] [CrossRef]
- Shahvari, O.; Logendran, R. An enhanced tabu search algorithm to minimize a bicriteria objective in batching and scheduling problems on unrelated-parallel machines with desired lower bounds on batch sizes. Comput. Oper. Res. 2017, 77, 154–176. [Google Scholar] [CrossRef]
- Du, G.; Jiang, Z.; Yao, Y.; Diao, X. Clinical pathways scheduling using hybrid genetic algorithm. J. Med. Syst. 2013, 37, 9945. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M. An Introduction to Genetic Algorithms; MIT Press: Cambridge, MA, USA, 1998. [Google Scholar]
- Deb, K.; Pratap, A.; Agarwal, S.; Meyarivan, T. A fast and elitist multiobjective genetic algorithm: NSGA-II. IEEE Trans. Evol. Comput. 2002, 6, 182–197. [Google Scholar] [CrossRef]
- Oliver, I.M.; Smith, D.J.; Holland, J.R.C. Study of Permutation Crossover Operators on the Traveling Salesman Problem. Available online: http://agris.fao.org/agris-search/search.do?recordID=US201301782179 (accessed on 5 February 2017).
- Goldberg, D.E.; Lingle, R. Alleles, Loci, and the Traveling Salesman Problem. Available online: https://books.google.com/books?hl=en&lr=&id=lI17AgAAQBAJ&oi=fnd&pg=PA154&dq=Alleles,+loci,+and+the+traveling+salesman+problem&ots=0Kr0ecO21s&sig=aoHK4wu5P6i6JV_pIq7ZquZbbDM#v=onepage&q=Alleles%2C%20loci%2C%20and%20the%20traveling%20salesman%20problem&f=false (accessed on 5 February 2017).
- Syswerda, G. Uniform Crossover in Genetic Algorithms; Morgan Kaufmann Publishers, Inc.: San Francisco, CA, USA, 1989; pp. 2–9. [Google Scholar]
- Mühlenbein, H. Parallel Genetic Algorithms, Population Genetics and Combinatorial Optimization. Available online: http://link.springer.com/chapter/10.1007/3-540-55027-5_23#page-1 (accessed on 5 February 2017).
- Braun, H. On solving travelling salesman problems by genetic algorithms. In Parallel Problem Solving from Nature; Springer: Berlin/Heidelberg, Germany, 1990; pp. 129–133. [Google Scholar]
- Ulder, N.L.J.; Aarts, E.H.L.; Bandelt, H.J.; van Laarhoven, P.J.M.; Pesch, E. Genetic local search algorithms for the traveling salesman problem. In Parallel Problem Solving from Nature; Springer: Berlin/Heidelberg, Germany, 1990; pp. 109–116. [Google Scholar]
- Potvin, J.Y. Genetic algorithms for the traveling salesman problem. Ann. Oper. Res. 1996, 63, 337–370. [Google Scholar] [CrossRef]
- Croes, G.A. A method for solving traveling-salesman problems. Oper. Res. 1958, 6, 791–812. [Google Scholar] [CrossRef]
- Lin, S.; Kernighan, B.W. An effective heuristic algorithm for the traveling-salesman problem. Oper. Res. 1973, 21, 498–516. [Google Scholar] [CrossRef]
- Tarantilis, C.D.; Kiranoudis, C.T. Distribution of fresh meat. J. Food Eng. 2002, 51, 85–91. [Google Scholar] [CrossRef]
- Prins, C. Two memetic algorithms for heterogeneous fleet vehicle routing problems. Eng. Appl. Artif. Intell. 2009, 22, 916–928. [Google Scholar] [CrossRef]
- Johnson, L.A.; Montgomery, D.C. Operations Research in Production Planning, Scheduling, and Inventory Control; Wiley: New York, NY, USA, 1974. [Google Scholar]
- Batchelor, C.; Owens, D.; Read, M.; Bloor, M. Patient satisfaction studies: Methodology, management and consumer evaluation. Int. J. Health Care Qual. Assur. 1994, 7, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Tam, J. Linking quality improvement with patient satisfaction: A study of a health service centre. Mark. Intell. Plan. 2007, 25, 732–745. [Google Scholar] [CrossRef]
- Mourad, S.; Nelen, W.; Akkermans, R.; Vollebergh, J.H.A.; Grol, R.P.T.M.; Hermens, R.P.M.G.; Kremer, J.A.M. Determinants of patients’ experiences and satisfaction with fertility care. Fertil. Steril. 2010, 94, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Du, G.; Sun, C. Location planning problem of service centers for sustainable home health care: Evidence from the empirical analysis of Shanghai. Sustainability 2015, 7, 15812–15832. [Google Scholar] [CrossRef]
- Benbassat, J.; Taragin, M. Hospital readmissions as a measure of quality of health care: Advantages and limitations. Arch. Intern. Med. 2000, 160, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B.; Shi, L. The medical home, access to care, and insurance: A review of evidence. Pediatrics 2004, 113, 1493–1498. [Google Scholar] [PubMed]
- Bruce, M.L.; McAvay, G.J.; Raue, P.J.; Brown, E.L.; Meyers, B.S.; Keohane, D.J.; Jagoda, D.R.; Weber, C. Major depression in elderly home health care patients. Am. J. Psychiatr. 2002, 159, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Du, G.; Jiang, Z.; Diao, X.; Yao, Y. Knowledge extraction algorithm for variances handling of CP using integrated hybrid genetic double multi-group cooperative PSO and DPSO. J. Med. Syst. 2012, 36, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Du, G.; Jiang, Z.; Diao, X.; Ye, Y.; Yao, Y. Variances handling method of clinical pathways based on ts fuzzy neural networks with novel hybrid learning algorithm. J. Med. Syst. 2012, 36, 1283–1300. [Google Scholar] [CrossRef] [PubMed]
- Du, G.; Jiang, Z.; Diao, X.; Ye, Y.; Yao, Y. Modelling, Variation Monitoring, Analyzing, Reasoning for Intelligently Reconfigurable Clinical Pathway. Available online: http://ieeexplore.ieee.org/abstract/document/5203909/ (accessed on 5 February 2017).
- Ye, Y.; Diao, X.; Jiang, Z.; Du, G. A Knowledge-Based Variance Management System for Supporting the Implementation of Clinical Pathways. Available online: http://ieeexplore.ieee.org/abstract/document/5305190/ (accessed on 5 February 2017).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Decision Type | Objective | Factors Considered | Model | Solution Technique |
|---|---|---|---|---|---|
| Lanzarone et al. [29] | Human resource planning in home care | Optimize service quality of human resources | Some variables and unpredictable event | Stochastic model | Markov chain |
| Triki et al. [30] | Periodic home health care planning | Minimize the total cost of transportation during each time period | The adherence to the care plan while optimizing the routes | One two-stage mathematical formulation | The tabu search and a Mixed-Integer Programming (MIP)-based neighborhood search method |
| Liu et al. [31] | Vehicle routing problem with delivery and pickup and time windows in home health care | Improve the quality and health service at their homes | Medical logistics vehicle scheduling problem in home care | Two mixed-integer programming model | Heuristic algorithms, a genetic algorithm (GA) and a tabu search (TS) method |
| Liu et al. [32] | Weekly home health care logistics optimization problem | Minimize the maximal routing costs of the week | Time window constraints of patients and precedence constraints | Periodic vehicle routing problem (PVRP) model | Tabu search and different local search schemes |
| Cappanera and Scutellà [33] | Scheduling and routing optimization to home care for a weekly planning horizon | Balance the operator utilization | The assignment and the scheduling in the planning horizon | Integer linear programming (ILP) model | Cplex 12.4 |
| Koeleman et al. [34] | Optimal patient and personnel scheduling policies for home care | Optimal control policy | Family medical human resource configuration, staff scheduling, family health service facilities | Markov decision process | Successive over-relaxation (SOR) algorithm |
| Hiermann et al. [35] | Multimodal home health care scheduling problem | Determine efficient multimodal tours | Staff and customer satisfaction | Mathematical modeling | Meta heuristics, simulated annealing hyper-heuristic |
| Service Staff | Mastered skills |
|---|---|
| h1 | Home Treatment |
| h2 | Home Treatment, Health Record |
| h3 | Hospital Bed at Home |
| h4 | Hospital Bed at Home |
| h5 | Hospital Bed at Home, Health Record |
| Parameter | Value |
|---|---|
| The service hours for hospital bed at home (k1) (hour) | 0.5 |
| The service hours for health record (k2) (hour) | 0.3 |
| travelling speed (km/h) | 8 |
| Unit travel costs (RMB/km) | 2 |
| The penalty coefficient for early arrival | 1 |
| The penalty coefficient Late arrival | 2 |
| Parameter | Value |
|---|---|
| The size of population | 500 |
| The probability of crossover | 0.5 |
| The probability of mutation | 0.5 |
| Termination generation | 3000 |
| Route | Node i | Node j | Service Personnel | Service Type |
|---|---|---|---|---|
| P0→P20(K1)→P24(K1)→P19(K1)→P18(K1)→P28(K1)→P8(K1)→P0 | 0 | 20 | h1 | k1 |
| 20 | 24 | h1 | k1 | |
| 24 | 19 | h1 | k1 | |
| 19 | 18 | h1 | k1 | |
| 18 | 28 | h1 | k1 | |
| 28 | 8 | h1 | k1 | |
| 8 | 0 | h1 | k1 | |
| P0→P2(K1)→P26(K1)→P6(K1)→P27(K1)→P7(K1)→P0 | 0 | 2 | h2 | k1 |
| 2 | 26 | h2 | k1 | |
| 26 | 6 | h2 | k1 | |
| 6 | 27 | h2 | k1 | |
| 27 | 7 | h2 | k1 | |
| 7 | 0 | h2 | k1 | |
| P0→P3(K1)→P4(K1)→P1(K1)→P0 | 0 | 3 | h3 | k1 |
| 3 | 4 | h3 | k1 | |
| 4 | 1 | h3 | k1 | |
| 1 | 0 | h3 | k1 | |
| P0→P12(K2)→P11(K2)→P14(K2)→P13(K2)→P15(K2)→P21(K2)→P25(K2)→P22(K2)→→P23(K2)→P0 | 0 | 12 | h4 | k2 |
| 12 | 11 | h4 | k2 | |
| 11 | 14 | h4 | k2 | |
| 14 | 13 | h4 | k2 | |
| 13 | 15 | h4 | k2 | |
| 15 | 21 | h4 | k2 | |
| 21 | 25 | h4 | k2 | |
| 25 | 22 | h4 | k2 | |
| 22 | 23 | h4 | k2 | |
| 23 | 0 | h4 | k2 | |
| P0→P9(K1)→P5(K1)→P16(K1)→P17(K1)→P10(K1)→P29(K1)→P30(K1)→P0 | 0 | 9 | h5 | k1 |
| 9 | 5 | h5 | k1 | |
| 5 | 16 | h5 | k1 | |
| 16 | 17 | h5 | k1 | |
| 17 | 10 | h5 | k1 | |
| 10 | 29 | h5 | k1 | |
| 29 | 30 | h5 | k1 | |
| 30 | 0 | h5 | k1 |
| The Target | Results |
|---|---|
| Final generation | 2904 |
| Minimum cost | 48.0 |
| Route 1 | P0→P22(K1)→P1(K1)→P21(K1)→P15(K1)→P16(K1)→P36(K1)→P34(K1)→P43(K1) →P8(K1)→P49(K1)→P17(K1)→P35(K1)→P37(K1)→P10(K1)→P30(K1)→P26(K1) →P6(K1)→P32(K1)→P5(K1)→P28(K1)→P13(K1)→P38(K1)→P0 |
| Route 2 | P0→P18(K1)→P45(K1)→P33(K1)→P44(K1)→P14(K1)→P48(K1) →P19(K1)→P4(K1)→P42(K1)→P11(K1)→P31(K1)→P12(K1)→P2(K1)→P3(K1)→P0 |
| Route 3 | P0→P9(K1)→P25(K1)→P23(K1)→P47(K1)→P46(K1)→P24(K1)→P41(K1)→P50(K1)→P27(K1)→P7(K1)→P40(K1)→P20(K1)→P39(K1)→P29(K1)→P0 |
| Route | Node | Earliest Starting Time | Latest Starting Time | Service Personnel | Service Type |
|---|---|---|---|---|---|
| Route 1 | P22 | 8 | 11 | h1 | k1 |
| P1 | 8 | 11 | h1 | k1 | |
| P21 | 8 | 12 | h1 | k1 | |
| P15 | 8 | 11 | h1 | k1 | |
| P16 | 9 | 12 | h1 | k1 | |
| P36 | 8 | 12 | h1 | k1 | |
| P34 | 10 | 16 | h1 | k1 | |
| P43 | 8 | 12 | h1 | k1 | |
| P8 | 9 | 12 | h1 | k1 | |
| P49 | 12 | 15 | h1 | k1 | |
| P17 | 10 | 13 | h1 | k1 | |
| P35 | 13 | 17 | h1 | k1 | |
| P37 | 13 | 16 | h1 | k1 | |
| P10 | 10 | 14 | h1 | k1 | |
| P30 | 13 | 16 | h1 | k1 | |
| P26 | 12 | 15 | h1 | k1 | |
| P6 | 9 | 15 | h1 | k1 | |
| P32 | 15 | 18 | h1 | k1 | |
| P5 | 10 | 16 | h1 | k1 | |
| P28 | 14 | 17 | h1 | k1 | |
| P13 | 13 | 17 | h1 | k1 | |
| P38 | 14 | 17 | h1 | k1 | |
| Route 2 | P18 | 10 | 14 | h2 | k1 |
| P45 | 8 | 11 | h2 | k1 | |
| P33 | 9 | 15 | h2 | k1 | |
| P44 | 9 | 15 | h2 | k1 | |
| P14 | 8 | 12 | h2 | k1 | |
| P48 | 10 | 14 | h2 | k1 | |
| P19 | 12 | 15 | h2 | k1 | |
| P4 | 9 | 15 | h2 | k1 | |
| P42 | 13 | 17 | h2 | k1 | |
| P11 | 12 | 15 | h2 | k1 | |
| P31 | 14 | 17 | h2 | k1 | |
| P12 | 13 | 16 | h2 | k1 | |
| P2 | 14 | 17 | h2 | k1 | |
| P3 | 15 | 18 | h2 | k1 | |
| Route 3 | P9 | 10 | 13 | h3 | k2 |
| P25 | 10 | 14 | h3 | k2 | |
| P23 | 9 | 12 | h3 | k2 | |
| P47 | 10 | 13 | h3 | k2 | |
| P46 | 9 | 12 | h3 | k2 | |
| P24 | 10 | 13 | h3 | k2 | |
| P41 | 10 | 16 | h3 | k2 | |
| P50 | 10 | 16 | h3 | k2 | |
| P27 | 13 | 16 | h3 | k2 | |
| P7 | 10 | 16 | h3 | k2 | |
| P40 | 9 | 15 | h3 | k2 | |
| P20 | 13 | 17 | h3 | k2 | |
| P39 | 15 | 18 | h3 | k2 | |
| P29 | 15 | 18 | h3 | k2 |
| Instance | Cplex | GA | HGA |
|---|---|---|---|
| B.3.50 | - | 50 ± 0.61 | 48 ± 0.23 |
| B.5.60 | - | 69 ± 0.45 | 66 ± 0.18 |
| B.6.70 | - | 76 ± 0.39 | 71 ± 0.22 |
| B.8.80 | - | 96 ± 0.27 | 88 ± 0.14 |
| C.9.90 | - | 123 ± 0.28 | 102 ± 0.23 |
| C.10.100 | - | 165 ± 0.51 | 122 ± 0.45 |
| C.12.120 | - | 188 ± 0.42 | 141 ± 0.29 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, G.; Liang, X.; Sun, C. Scheduling Optimization of Home Health Care Service Considering Patients’ Priorities and Time Windows. Sustainability 2017, 9, 253. https://doi.org/10.3390/su9020253
Du G, Liang X, Sun C. Scheduling Optimization of Home Health Care Service Considering Patients’ Priorities and Time Windows. Sustainability. 2017; 9(2):253. https://doi.org/10.3390/su9020253
Chicago/Turabian StyleDu, Gang, Xi Liang, and Chuanwang Sun. 2017. "Scheduling Optimization of Home Health Care Service Considering Patients’ Priorities and Time Windows" Sustainability 9, no. 2: 253. https://doi.org/10.3390/su9020253
APA StyleDu, G., Liang, X., & Sun, C. (2017). Scheduling Optimization of Home Health Care Service Considering Patients’ Priorities and Time Windows. Sustainability, 9(2), 253. https://doi.org/10.3390/su9020253