
Air Pollution and Human Health: Investigating the Moderating Effect of the Built Environment


1
Faculty of Civil Engineering and Mechanics, Jiangsu University, Zhenjiang 212013, China
2
State Key Laboratory of Pollution Control and Resource Reuse, School of the Environment, Nanjing University, Nanjing 210023, China
*
Author to whom correspondence should be addressed.
Remote Sens. 2022, 14(15), 3703; https://doi.org/10.3390/rs14153703
Submission received: 11 June 2022
/
Revised: 14 July 2022
/
Accepted: 29 July 2022
/
Published: 2 August 2022
(This article belongs to the Special Issue Remote Sensing and GIS for Monitoring Urbanization and Urban Health)
Abstract
:Air pollution seriously threatens human health and even causes mortality. It is necessary to explore effective prevention methods to mitigate the adverse effect of air pollution. Shaping a reasonable built environment has the potential to benefit human health. In this context, this study quantified the built environment, air pollution, and mortality at 1 km × 1 km grid cells. The moderating effect model was used to explore how built environment factors affect the impact of air pollution on cause-specific mortality and the heterogeneity in different areas classified by building density and height. Consequently, we found that greenness played an important role in mitigating the effect of ozone (O3) and nitrogen dioxide (NO2) on mortality. Water area and diversity of land cover can reduce the effect of fine particulate matter (PM2.5) and NO2 on mortality. Additionally, gas stations, edge density (ED), perimeter-area fractal dimension (PAFRAC), and patch density (PD) can reduce the effect of NO2 on mortality. There is heterogeneity in the moderating effect of the built environment for different cause-specific mortality and areas classified by building density and height. This study can provide support for urban planners to mitigate the adverse effect of air pollution from the perspective of the built environment.
1. Introduction
Air pollution has become increasingly severe in recent years, which profoundly affects public health and is of concern to health organizations and governments [1,2]. About 90% of the population of the world lives in areas where air quality levels exceed the standard limited by the World Health Organization (WHO) [3]. Mitigating the effect of air pollution on human health has become a key issue to public health. During the last three decades, the effects of air pollution on human health have been documented, especially from particulate matter (PM), O3, and NO2 [4]. The global burden of disease caused by air pollution has barely declined since the 1990s [5]. In particular, an association with cardiovascular and respiratory causes of death has been reported [6,7].
The built environment is defined as human-made physical environment surroundings and conditions [8,9]. Urban spatial conditions can change the wind direction and velocity, which affect the air pollution dispersion [10]. Built environment characteristics can shape our activity patterns, which play a great role in health [11]. However, the health outcomes from physical activity could be offset by adverse exposure to air pollution [12]. Therefore, it is important to understand which built environment factors can alleviate the adverse effects of air pollution on human health. In addition, the definition of some built environment indicators does not adequately reflect local information [13]. Existing research on the built environment tends to select greenness, building density, and road density as major objects [14,15]. The use of multi-source data such as points of interest (POIs) can build a more comprehensive built environment framework [13].
Human health is an important landscape benefit and concern of many landscape users [16]. Although some studies have assessed the effect of the built environment on health, the results are inconsistent. As far as greenness is concerned, the reduction in mortality is associated with the increase in greenness [17]. Greenness was confirmed to link with the mortality of non-accident, cardiovascular, and respiratory diseases [3]. Other studies have pointed out a non-linear correlation between residential greenness and health [18,19]. Nevertheless, some studies point out that greenness is not associated with mortality [20,21]. The effect of the built environment on health is unclear and heterogeneity may exist across different areas. By incorporating building density and height into the framework of the built environment, the moderating mechanism of the built environment can be fully explored from a three-dimensional perspective.
Over the years, the study of the built environment, air pollution, and human health has shown a pairwise relationship, especially the effect of air pollution on health [2,11,22]. A spectrum of the key mechanisms link the built environment to human health, including air pollution and health behaviors [23,24]. The relationship between the built environment and health has been discussed from the perspectives of sleep, resilience, physicochemical environmental factors, movement, relationships, spirituality, and nutrition [25]. However, there is a lack of research linking these three fields.
Therefore, taking Nanjing city of Jiangsu Province in China as the study area, the main objectives of this study were (i) to determine which built environment can mitigate the adverse health effect of air pollution, (ii) to compare the moderating effect of the built environment on the relationship between air pollution (O3, PM2.5, and NO2) and cause-specific mortality, and (iii) to analyze the heterogeneity of the built environment moderating effect in different areas classified by building density and height. This study quantified annual O3, PM2.5, NO2, non-accident deaths, cardiovascular disease deaths, and respiratory disease deaths at a 1 km × 1 km grid scale from 2007 to 2015. Built environment factors were assumed to remain unchanged in this study, and we calculated them for 2015 as moderating variables. First, we investigated the moderating effect of the built environment on the relationship between air pollution and mortality. Then, we further explored the heterogeneity in different areas classified by building height and density.
Addressing these issues will be beneficial to reveal the mechanism of the built environment on mortality, and the findings can provide support for urban planning to reduce the adverse effect from air pollution.
2. Materials and Methods
2.1. Study Area
China has suffered severe air pollution for the last decade because of fast urbanization and industrialization, particularly in the economically developed eastern regions such as the Yangtze River Delta (YRD) region [26]. This study was conducted in Nanjing (Figure 1), one of the cities in the YRD region, the capital of Jiangsu province in China. Jiangsu Province is one of the most developed provinces in China. Nanjing (31°14′N–32°37′N, 118°22′E–119°14′E) had experienced a rapid urbanization process with a population of 8.4 million by the end of 2018. At the same time, because Nanjing is surrounded by mountains on three sides, which is not conducive to the diffusion of pollutants, the concentrations of air pollutants in Nanjing is higher than the national average. Nanjing has a subtropical monsoon climate.
2.2. Data Collection
The data used in this study include road data, building information, normalized difference vegetation index (NDVI), land use and land cover data, point of interest (POI), air pollution (NO2, PM2.5, and O3), population density, and mortality data. Road data from OpenStreetMap were used to calculate the road length and road crossing at a grid scale. The building dataset was acquired from BIGEMAP, which contained detailed information on building space coordinates, footprints, and the number of floors in a building. Point of interest (POI) data from BIGEMAP were adopted to measure the diversity of the POI and the number in the grid. NDVI was used to measure surface greenness in this study. The study calculated the proportion of construction land, forestland, and water area within the grid based on the land cover data from Resource and Environment Science and Date Center. This study considered three air pollutants i.e., O3, PM2.5, and NO2. This study took into account population density as a covariate in the relationship between air pollution and mortality. Based on the address information, this study calculated the deaths in the grid scale. The sources of the data are shown in Table 1. The overall framework of this paper is shown in Figure 2.
2.3. Measurement of Built Environment
In this study, 24 features were calculated to interpret the built environment. We operationalized the measurements of the built environment at the grid scale according to the framework in Table 2. All 24 features were divided into five categories including design, destination, land use, landscape, and diversity. The factors of design, destination, and land cover were calculated using the ArcGIS Desktop platform (version 10.8). The landscape indexes and SHDI of each grid were calculated by the Fragstats 4.2. The diversity of the built environment was calculated by the entropy method [31] based on the diversity of the design and diversity of POI and SHDI. This study used standardized indexes to calculate the diversity of design. The diversity of design and diversity of POI were calculated using the following Hill numbers equation [32]:
where is diversity, indicates the number of the types, is proportion of the category occupied by type , and = 2 (according to the Gini–Simpson concentration index).
2.4. Air Pollution and Mortality from 2007 to 2015
High resolution exposure data are helpful to accurately assess the effect of air pollution on human health. Based on the high-resolution spatiotemporal model and data of previous studies [27,28], we calculated the annual O3, PM2.5, and NO2 concentration from 2007 to 2015 at 1 km × 1 km grid scale in Nanjing.
Mortality data were classified into non-accidental causes (A00-R99), cardiovascular diseases (I00-I99), and respiratory diseases (J00-J99) based on the International Statistical Classification of Diseases and Related Health Problems 10th Revision (https://icd.who.int/browse10/2010/en#/IX (accessed on 14 June 2021)). Based on the addressed information, we calculated the gridded death counts of non-accidental, cardiovascular diseases, and respiratory diseases. The high death toll may be related to the high population base. Meanwhile, higher population density is related to higher mortality [33,34]. Hence, we selected population density as a control variable to eliminate the effect of population on mortality in this study.
2.5. Statistical Analysis
This study derived the air pollution and mortality in Nanjing for each year from 2007 to 2015. Then, correlation analysis was used to explore the relationships between the air pollution and mortality. In the correlation analysis, this study deleted the sample with zero death. Based on the correlation test, the study further used regression models to control the effect of population on deaths. Pearson’s correlation coefficient can measure the correlation between two variables, and [14].
Because of the availability of data, the built environment indexes were calculated for 2015. This study assumed that the built environment remains unchanged. Then, we explored the spatial correlation between air pollution and the built environment and mortality and the built environment, respectively. Local indicators of spatial association (LISA) can describe the spatial correlation between the spatial distribution of different variables [35]. The study used GeoDa 1.14 to explore the bivariate spatial correlation. Local indicators of spatial association were calculated as follows [36]:
where is the local Moran index of grid ; is the spatial weight between grid and ; is the number of spatial grids adjacent to grid ; and are the values of grid and , respectively; is the variable average; and indicates the variance.
Hierarchical regression was used to explore the moderating effect of the built environment in the relationship between air pollution and mortality. Within the model, air pollution was the independent variable () and mortality was the dependent variable (), with population density as the covariate. The built environment was defined as the moderator (). The study further conducted subgroup analyses by building density and height [37]. The moderating effect was confirmed by a significant interaction between the independent variable and the moderator. Before modeling, we normalized the variables and centered to zero. The moderation analysis was conducted in PROCESS, a plug-in for SPSS 25.0. All of the analyses were accepted with significance at α = 0.05.
3. Results
3.1. Spatial Patterns of the Built Environment
The spatial patterns of the built environment are shown in Figure 3. It was observed that built environment indexes have a high level of agglomeration. The diversity of the built environment is higher in the middle part of Nanjing. Close to the city center, the urbanization level and development intensity were higher. High-intensity development usually means higher building density, building height, and road density, while greenness is relatively low.
3.2. Pairwise Correlation between Air Pollution, Mortality, and the Built Environment
The results of the correlation analysis of air pollution and mortality are shown in Figure 4, and the detailed results of the regression analysis are shown in the Table 3. Statistically positive associations were found between air pollution and mortality. NO2 shows the strongest positive association with mortality, especially for respiratory death. The direct correlations between air pollution and mortality have an indicative character. However, there are some other factors that can also contribute to mortality, such as built environment factors.
The spatial correlation between air pollution and the built environment and mortality and the built environment is shown in Figure S1. It is clear that the built environment has agglomeration relationships with air pollution and mortality. High–high (H–H) areas indicate high air pollution or high mortality with a high built environment level. High–low (H–L) areas indicate high air pollution or high mortality with a low built environment level. Low–high (L–H) areas indicate low air pollution or low mortality with high built environment level. Low–low (L–L) areas indicate low air pollution or low mortality with a low built environment level.
3.3. The Moderation Analysis
The coefficient of the interaction item “built environment × air pollution” was used as an indicator to judge the moderating effect. The moderating effects of 24 built environment indexes on the relationship between air pollution (O3, PM2.5, and NO2) and cause-specific mortality are shown in Figure 5. The results shown in Figure S2 reveal the moderating effect in six classes, which include high-rise with high-density, high-rise with low-density, mid-rise with high density, mid-rise with low density, low-rise with high density, and low-rise with high density. Respective moderating effects of the built environment on the relationship between air pollution (O3, PM2.5, and NO2) and cause-specific mortality are illustrated below.
For the relationship between O3 and cause-specific mortality, indexes like diversity of the built environment, diversity of design, diversity of POI, building density, building height, SDBH, and construction land have significant positive associations with three cause-specific mortalities, while NDVI has a negative moderating effect. Road length has a significant positive association with non-accidental and cardiovascular mortality. The moderating effect is significant in high-rise with high density areas. We found that a hygiene facility can inhibit the effect of O3 on cause-specific mortality in mid-rise with high density areas. The moderating effects detected in respiratory and cardiovascular mortality are higher than in non-accidental mortality.
The effects of PM2.5 on non-accidental and cardiovascular mortality are moderated by the diversity of POI, SHDI, and catering facility, where SHDI shows a negative moderating effect. The moderating effects of SHDI and the catering facility are higher in cardiovascular than in non-accidental mortality. The water area has a significant negative moderating effect in the relationship between PM2.5 and non-accidental mortality. In high-rise with high density and mid-rise with high density areas, the moderating effects of all built environment indexes are insignificant. The moderating effects of building density, road length, road crossing, hygiene facility, government agency, residential community, traffic facility, catering facility, AI, ED, PAFRAC, and PD are highest for respiratory mortality in low-rise with high density areas. We found that a higher building height can inhibit the effect of PM2.5 on cause-specific mortality in high-rise with low density areas. Water area, government agency, and residential community have a negative effect on the relationship between PM2.5 and mortality.
On the whole, the moderating effects in the relationship between NO2 and mortality are higher than O3 and PM2.5. Diversity of POI, building density, road crossing, construction land, hygiene facility, government agency, residential community, catering facility, and AI have a positive moderating effect on the relationship between NO2 and three cause-specific mortality, while SHDI, building height, NDVI, gas station, ED, PAFRAC, and PD have a negative effect. The effect of NO2 on mortality is most significantly moderated by building density. The coefficient of the interaction of “building density × NO2” is 0.125 (95%CI: 0.104–0.146) for non-accidental mortality, 0.106 (95%CI: 0.081–0.130) for cardiovascular mortality, and 0.146 (95%CI: 0.112–0.180) for respiratory mortality, with all p-values < 0.0001. Although the moderating effect of construction land is positive and not significant for forestland, SHDI indicates that the diversity of land cover has a negative moderating effect on the relationship between NO2 and cause-specific mortality. Positive moderating effects for non-accidental and respiratory mortality were detected on the diversity of the built environment, diversity of design, road length, and traffic facility. The effects were higher for respiratory mortality. In mid-rise with high-density areas, building density, hygiene facility, government agency, residential community, and catering facility have a negative moderating effect on mortality. The building height and SDBH show a negative moderating effect for three cause-specific mortality in low-rise with high-density areas. The residential community can inhibit the effect of NO2 on mortality on high-rise with low-density and mid-rise with low-density areas. The relationship between NO2 and mortality can be inhibited by the diversity of the built environment, diversity of POI, and SHDI in the low-rise with low-density areas.
4. Discussion
In this study, we first assessed the associations among the built environment, air pollution, and mortality from different causes such as non-accident, cardiovascular disease and respiratory disease. Then, we analyzed how the built environment affected the relationship between air pollution and mortality. The results show that the built environment has a significant moderating effect on the relationship between air pollution and mortality. The moderating effect is stronger in NO2 than PM2.5 and O3. We found some heterogeneity across different areas classified by building height and density.
4.1. Which Built Environment Can Moderate the Effect of Air Pollution on Mortality?
As the first step, the study analyzed the relationship between air pollution and mortality by correlation analysis and linear regression. This study confirmed that air pollutants have an adverse effect on human health. The results were consistent with most existing air pollution and health studies [22,38,39]. We have found a statistically significant association between air pollution and mortality, especially in NO2. Then, we explored the spatial agglomeration between air pollution and the built environment and mortality and the built environment. According to the spatial correlation (Figure S1), a high built environment may lead to high or low air pollution and mortality; the pairwise relationship between built environment, air pollution, and mortality is not absolute. Then, we took the built environment as the moderating variable to explore how the built environment affects the impact of air pollution on mortality.
The results showed that the built environment played a moderating role in the relationship between air pollution and non-accident mortality (Figure 5). NDVI can reduce the effect of O3 on all-cause mortality, which means the effect of O3 on all-cause mortality is lower for people living in areas with higher greenness. Many studies have indicated the benefit of greenness. For example, a cohort study of Hong Kong found that elders living in low greenness areas had a higher health risk than those living in higher greenness areas [3,17]. SHDI and water area can reduce the effect of PM2.5 on all-cause mortality. SHDI, NDVI, water area, building height, gas station, ED, PAFRAC, and PD can reduce the effect of NO2 on all-cause mortality. Landscape patterns can change the travel mode industrial layout and climate conditions, further influencing human health [40]. Higher greenness and a larger water area can mitigate the adverse effects of the environment on human health [41,42]. Building height might mitigate the effect of NO2 on all-cause mortality by providing shade to influence human comfort [43].
4.2. Heterogeneity of the Moderating Effect in Different Areas and Cause-Specific Mortality
We further discussed the moderating effect of the built environment for cause-specific mortality and different areas. The moderating effects of all built environment indexes on the relationship between three air pollutants and cause-specific mortality are shown in Figure 5 and Figure S2. The moderating effect of the diversity of the built environment, design, and NDVI in the relationship between O3 and mortality is the strongest for respiratory disease, while building height is the strongest for cardiovascular disease. The moderating effect of the built environment was not significant in the relationship of PM2.5 and respiratory disease mortality. Generally, the moderating effect of the built environment in the relationship between NO2 and mortality is the strongest for respiratory disease.
In high-rise with high-density areas, the moderating effect of the built environment is the strongest. SHDI, building height, water area, ED, PAFRAC, and PD can mitigate the effect of O3 and NO2 on non-accident, cardiovascular disease and respiratory disease mortality. We found that the moderating effect of NDVI and forestland in high-rise with high-density areas was not significant. The construction land can intensify the effect of O3 and NO2 on mortality. However, SHDI, which indicates the diversity of land cover, has a significant negative effect on the relationship between O3 and NO2 on mortality. The results show that the adverse effect of air pollution can be mitigated with the reasonable allocation of landscape and improvement in the diversity of land cover in high-rise with high-density areas. In mid-rise with high-density areas, the hygiene facility plays a vital role in mitigating the effect of O3 and NO2 on mortality. Government agency, residential community, and catering facility can also mitigate the effect of NO2 on mortality in mid-rise with high-density areas. High accessibility to amenities and greater residential density mean more transport via walking, which can reduce the risk of all-cause mortality [11,44]. In low-rise with high-density areas, this study found that building height and SDBH can mitigate the effect of NO2 on mortality. Building height and difference is associated with the wind environment and a high building height will form a strong angular flow area [2]. It is known that wind speed and air flow affect human comfort [45]. They can provide comfortability and health for pedestrians, as well as maintain a fresh air flow [46].
In high-rise with low-density areas, the diversity of design can mitigate the effect of PM2.5 on non-accident mortality. Building density can mitigate the effect of PM2.5 on three cause-specific mortality, and it is strongest for cardiovascular disease mortality. Hygiene facility, residential community, and traffic facilities can mitigate the effect of PM2.5 on respiratory disease mortality. For NO2, the moderating effect of the built environment is the strongest for respiratory disease mortality. In mid-rise with low-density areas, SHDI, NDVI, gas station, ED, PAFRAC, and PD have a negative effect on the relationship between NO2 and mortality in mid-rise with low-density areas. The moderating effect of the built environment exited heterogeneity across different air pollutants. SHDI can mitigate the effect of NO2 on mortality while intensifying the effect of O3 on mortality. This heterogeneity is due to the correlation between pollutants. For instance, NO2 and O3 may be negatively correlated in urban areas [47]. In low-rise with low-density areas, we found that the diversity of POI can mitigate the effect of NO2 on mortality, while it had a positive moderating effect in other areas. A higher diversity of facilities represents more activities and higher vitality [48]. High accessibility to facilities and mixed land use were associated with more transport via walking, and walking is an activity that can reduce the non-accident mortality risk [11,44].
We surprisingly found that greenness appeared to aggravate the effect of PM2.5 and NO2 on mortality in mid-rise with high-density and high-rise with low-density areas, respectively. A study in China found a nonlinear, inverted U-shaped association between greenness and health [18]. One potential explanation for the heterogeneity is that larger NDVI values are probably areas with a large proportion of wild environment and agricultural farmland, which means supporting service facilities and lower physical activity [49]. Hygiene facility, government agency, residential community, and catering facility can mitigate the effect of NO2 on mortality in high-rise with low-density areas, while they appear to intensify the effect on the whole.
4.3. Implications for Urban Planning
Air pollution has been recognized as a global concern to human health for decades [47]. In recent years, the built environment, being the human-made physical environment surroundings and conditions, was confirmed to be linked with human health [9,50]. Based on the moderating effect analysis in Nanjing city, we put forward the following suggestions for mortality risk mitigation measures from the perspective of the built environment:
In general, greenness can help effectively mitigate the effect of O3 and NO2 on cause-specific mortality, including non-accident, cardiovascular disease, and respiratory disease. Controlling the building density may help effectively reduce the adverse effect of air pollution. However, it is difficult to reduce the building density on an original basis. In contrast, optimizing landscape patterns and facilities can mitigate the effect of air pollution on mortality. Landscapes such as ED, PAFRAC, and PD have a negative effect in the relationship between NO2 and mortality. The diversity of land cover can mitigate the effect of NO2 on mortality, as well as the effect of PM2.5 on non-accident and cardiovascular disease mortality. We can increase the proportion of grassland, forestland, and water area appropriately to improve the landscape patterns.
Moreover, the built environment as a mitigation measure to moderate the effect of air pollution on mortality should consider heterogeneity between areas. In this study, we also provided suggestions for different building height and density areas. We can improve the diversity of land cover, especially water area, to mitigate the mortality risk from air pollution in high-rise with high-density areas. The adverse effect of air pollution can be mitigated by hygiene facility, government agency, residential community, and catering facility in mid-rise with high-density areas. We can focus on the SDBH and PAFRAC in low-rise with high-density areas, controlling the effect of air pollution on mortality by increasing the complexity of the landscape. In low density areas, landscape configuration plays a vital role in mitigating the effect of air pollution on mortality. In high-rise with low-density areas, respiratory disease mortality was more severely affected by the built environment. Traffic facility has a negative effect on the relationship between PM2.5 and respiratory disease mortality. The adverse effect from PM2.5 and O3 in mid-rise with low-density areas can be mitigated by placing more government agencies. In low-rise with low-density areas, the effect of air pollution on mortality can be moderated by increasing the diversity of land cover, greenness, and gas stations. Our results highlight that the effects of the built environment vary across different areas classified by building density and height.
4.4. Limitations and Future Studies
In this paper, a moderating effect model was used to explored the relationship among built environment, air pollution, and mortality. Nevertheless, it is important to note that there are several limitations. Firstly, only the spatial built environment was quantified, and the change in the built environment over time was not taken into consideration in the moderating effect model. Secondly, we ignored the effects of meteorology and seasonal changes, which can modify the impact on health. Climate and weather changes may have an impact on aero-allergens through variability in meteorological factors (temperature, wind, rain, storm, blizzard, and so on), thus resulting in health risks [51]. Increased temperatures in autumn significantly contributed to the increase in ozone-related health effects [52]. There is a seasonal variation in the effect of particulate air pollution on mortality, with the greatest effect occurring in winter and summer in China [53]. Lastly, our study did not analyze the moderating effect of all built environment factors systematically, partly because too many variables can cause instability in the model.
Therefore, in future research, it is necessary to pay attention to the seasonal differences in the moderating effects of the built environment, and analyze the effects of the built environment combination on air pollution and mortality from a systematic perspective. At the same time, we are also searching for a suitable algorithm model to explore the best built environment combination to reduce air pollution concentration and mortality from the perspective of optimal design.
5. Conclusions
Based on an empirical study of Nanjing in China from 2007 to 2015, this paper revealed the moderating effect of the built environment on the relationship between air pollution and mortality. The result was obtained by the moderating effect model based on hierarchical regression. In particular, the greenness, water body, and landscape elements can effectively mitigate the adverse effect of air pollution, while the intensity of the development may aggravate it. The sensitivity of different populations to air pollution varies, and the moderating effect of the built environment is also heterogeneous. We should pay more attention to the diversity of land cover. A single land cover type may not significantly reduce the adverse impact of air pollutants, or even aggravate it. For example, forestland, construction land, and water body have no significant impact on the association between PM2.5 and cardiovascular mortality, while their diversity can mitigate the effect of PM2.5 on cardiovascular mortality.
Identifying the heterogeneity of the moderating effect of the built environment can help to formulate more accurate mitigation planning. The moderating effect of the built environment is the strongest in areas with high building density and height. Water body and landscape patterns can effectively mitigate the adverse effect of air pollution. A hygiene facility can mitigate the association between air pollution and mortality in mid-rise with high-density areas. At the same time, the height of the building also has a mitigating effect. It is worth noting that government agency can improve the air-pollution-related mortality in mid-rise areas, while it may aggravate the adverse effects of air pollution in other areas. Our findings suggest that the built environment could be integrated into urban planning to mitigate the effect of air pollution on human health. In addition, the development of mitigating measures needs to take into account the heterogeneity of areas and consider the mix of built environment factors.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/rs14153703/s1, Figure S1: Spatial correlation of air pollution (O3, PM2.5 and NO2) and mortality with built environment respectively; Figure S2: Moderating effect of built environment in the relationship between air pollution and mortality in (1) unclassified area and (2) areas classified by building density and height. Table S1: The percentage of H-H type grids corresponding to Figure S1; Table S2: The percentage of L-L type grids corresponding to Figure S1; Table S3: The percentage of L-H type grids corresponding to Figure S1; Table S4: The percentage of H-L type grids corresponding to Figure S1; Table S5: The percentage of not significant type grids corresponding to Figure S1.
Author Contributions
Conceptualization, P.W. and C.W.; methodology, C.W.; software, Y.S.; validation, C.W. and Y.S.; formal analysis, C.W.; investigation, J.W. and Y.W.; resources, L.H.; data curation, C.W.; writing—original draft preparation, C.W., Y.S., J.W. and Y.W.; writing—review and editing, Y.S. and J.W.; visualization, J.W.; supervision, C.W. and Y.S.; project administration, P.W.; funding acquisition, P.W. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Natural Science Foundation of China [Grant No. 51908249], the Natural Science Foundation of the Jiangsu Higher Education Institutions of China [Grant No. 19KIB560012], the High-level Scientific Research Foundation for the introduction of talent for Jiangsu University [Grant No. 18JDG038], and the Innovative Approaches Special Project of the Ministry of Science and Technology of China [Grant No. 2020IM020300].
Data Availability Statement
The data used in this study are presented in Table 1.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Xu, H.; Wang, Q.; Zhu, H.; Zhang, Y.; Ma, R.; Ban, J.; Li, T. Air Pollution Control of China Brought Significant Health and Economic Benefit but the Health Burden Is Still Heavy and Keeps Rising. SSRN Electron. J. 2022. [Google Scholar] [CrossRef]
- Yang, J.; Shi, B.; Zheng, Y.; Shi, Y.; Xia, G. Urban Form and Air Pollution Disperse: Key Indexes and Mitigation Strategies. Sustain. Cities Soc. 2020, 57, 101955. [Google Scholar] [CrossRef]
- Sun, S.; Sarkar, C.; Kumari, S.; James, P.; Cao, W.; Lee, R.S.Y.; Tian, L.; Webster, C. Air Pollution Associated Respiratory Mortality Risk Alleviated by Residential Greenness in the Chinese Elderly Health Service Cohort. Environ. Res. 2020, 183, 109139. [Google Scholar] [CrossRef]
- Michetti, M.; Gualtieri, M.; Anav, A.; Adani, M.; Benassi, B.; Dalmastri, C.; D’Elia, I.; Piersanti, A.; Sannino, G.; Zanini, G.; et al. Climate Change and Air Pollution: Translating Their Interplay into Present and Future Mortality Risk for Rome and Milan Municipalities. Sci. Total Environ. 2022, 830, 154680. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240034228. [Google Scholar]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological Time Series Studies of PM2.5 and Daily Mortality and Hospital Admissions: A Systematic Review and Meta-Analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stafoggia, M.; Bellander, T. Short-Term Effects of Air Pollutants on Daily Mortality in the Stockholm County—A Spatiotemporal Analysis. Environ. Res. 2020, 188, 109854. [Google Scholar] [CrossRef] [PubMed]
- Travert, A.S.; Annerstedt, K.; Daivadanam, M. Built Environment and Health Behaviors: Deconstructing the Black Box of Interactions—A Review of Reviews. Int. J. Environ. Res. Public Health 2019, 16, 1454. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Leung, J.; Yu, B.; Woo, J.; Kwok, T.; Ka-Lun Lau, K. Socioeconomic Status as an Effect Modifier of the Association between Built Environment and Mortality in Elderly Hong Kong Chinese: A Latent Profile Analysis. Environ. Res. 2021, 195, 110830. [Google Scholar] [CrossRef]
- Epstein, S.A.; Lee, S.M.; Katzenstein, A.S.; Carreras-Sospedra, M.; Zhang, X.; Farina, S.C.; Vahmani, P.; Fine, P.M.; Ban-Weiss, G. Air-Quality Implications of Widespread Adoption of Cool Roofs on Ozone and Particulate Matter in Southern California. Proc. Natl. Acad. Sci. USA 2017, 114, 8991–8996. [Google Scholar] [CrossRef] [Green Version]
- Frank, L.D.; Iroz-Elardo, N.; MacLeod, K.E.; Hong, A. Pathways from Built Environment to Health: A Conceptual Framework Linking Behavior and Exposure-Based Impacts. J. Transp. Health 2019, 12, 319–335. [Google Scholar] [CrossRef]
- Sinharay, R.; Gong, J.; Barratt, B.; Ohman-Strickland, P.; Ernst, S.; Kelly, F.J.; Zhang, J.; Collins, P.; Cullinan, P.; Chung, K.F. Respiratory and Cardiovascular Responses to Walking down a Traffic-Polluted Road Compared with Walking in a Traffic-Free Area in Participants Aged 60 Years and Older with Chronic Lung or Heart Disease and Age-Matched Healthy Controls: A Randomised, Crosso. Lancet 2018, 391, 339–349. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Kim, I.; Chung, H. The Effects of Built Environment Spatial Variation on Bike-Sharing Usage: A Case Study of Suzhou, China. Cities 2021, 110, 103063. [Google Scholar] [CrossRef]
- Yuan, M.; Yin, C.; Sun, Y.; Chen, W. Examining the Associations between Urban Built Environment and Noise Pollution in High-Density High-Rise Urban Areas: A Case Study in Wuhan, China. Sustain. Cities Soc. 2019, 50, 101678. [Google Scholar] [CrossRef]
- Chen, E.; Ye, Z.; Wu, H. Nonlinear Effects of Built Environment on Intermodal Transit Trips Considering Spatial Heterogeneity. Transp. Res. Part D Transp. Environ. 2021, 90, 102677. [Google Scholar] [CrossRef]
- Opdam, P. Implementing Human Health as a Landscape Service in Collaborative Landscape Approaches. Landsc. Urban Plan. 2020, 199, 103819. [Google Scholar] [CrossRef]
- Brochu, P.; Jimenez, M.P.; James, P.; Kinney, P.L.; Lane, K. Benefits of Increasing Greenness on All-Cause Mortality in the Largest Metropolitan Areas of the United States Within the Past Two Decades. Front. Public Health 2022, 10. [Google Scholar] [CrossRef]
- Huang, B.; Yao, Z.; Pearce, J.R.; Feng, Z.; James Browne, A.; Pan, Z.; Liu, Y. Non-Linear Association between Residential Greenness and General Health among Old Adults in China. Landsc. Urban Plan. 2022, 223, 104406. [Google Scholar] [CrossRef]
- Sarkar, C.; Zhang, B.; Ni, M.; Kumari, S.; Bauermeister, S.; Gallacher, J.; Webster, C. Environmental Correlates of Chronic Obstructive Pulmonary Disease in 96,779 Participants from the UK Biobank: A Cross-Sectional, Observational Study. Lancet Planet. Health 2019, 3, e478–e490. [Google Scholar] [CrossRef] [Green Version]
- Gronlund, C.J.; Zanobetti, A.; Wellenius, G.A.; Schwartz, J.D.; O’Neill, M.S. Vulnerability to Renal, Heat and Respiratory Hospitalizations During Extreme Heat Among U.S. Elderly. Clim. Chang. 2016, 136, 631–645. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Dadvand, P.; Barrera-Gómez, J.; Sartini, C.; Marí-Dell’Olmo, M.; Borrell, C.; Medina-Ramón, M.; Sunyer, J.; Basagaña, X. Differences on the Effect of Heat Waves on Mortality by Sociodemographic and Urban Landscape Characteristics. J. Epidemiol. Community Health 2013, 67, 519–525. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, J.; Kwong, J.C.; Burnett, R.T.; van Donkelaar, A.; Hystad, P.; Martin, R.V.; Bai, L.; McLaughlin, J.; Chen, H. Long-Term Exposure to Air Pollution and Mortality in a Prospective Cohort: The Ontario Health Study. Environ. Int. 2021, 154, 106570. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City Planning and Population Health: A Global Challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef]
- Patino, J.E.; Hong, A.; Duque, J.C.; Rahimi, K.; Zapata, S.; Lopera, V.M. Built Environment and Mortality Risk from Cardiovascular Disease and Diabetes in Medellín, Colombia: An Ecological Study. Landsc. Urban Plan. 2021, 213, 104126. [Google Scholar] [CrossRef]
- Engineer, A.; Gualano, R.J.; Crocker, R.L.; Smith, J.L.; Maizes, V.; Weil, A.; Sternberg, E.M. An Integrative Health Framework for Wellbeing in the Built Environment. Build. Environ. 2021, 205, 108253. [Google Scholar] [CrossRef]
- Dai, L.; Zhang, L.; Chen, D.; Zhao, Y. Assessment of Carbonaceous Aerosols in Suburban Nanjing under Air Pollution Control Measures: Insights from Long-Term Measurements. Environ. Res. 2022, 212, 113302. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Hu, J.; Xue, T.; Xu, H.; Wang, M. High-Resolution Spatiotemporal Modeling for Ambient PM2.5Exposure Assessment in China from 2013 to 2019. Environ. Sci. Technol. 2021, 55, 2152–2162. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, C.; Hu, J.; Wang, M. Development of High-Resolution Spatio-Temporal Models for Ambient Air Pollution in a Metropolitan Area of China from 2013 to 2019. Chemosphere 2022, 291, 132918. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Zhou, L.; Chen, K. Burden of Cause-Specific Mortality Attributable to Heat and Cold: A Multicity Time-Series Study in Jiangsu Province, China. Environ. Int. 2020, 144, 105994. [Google Scholar] [CrossRef]
- Chen, K.; Bi, J.; Chen, J.; Chen, X.; Huang, L.; Zhou, L. Influence of Heat Wave Definitions to the Added Effect of Heat Waves on Daily Mortality in Nanjing, China. Sci. Total Environ. 2015, 506–507, 18–25. [Google Scholar] [CrossRef]
- Wang, P.; Qiao, W.; Wang, Y.; Cao, S.; Zhang, Y. Urban Drought Vulnerability Assessment–A Framework to Integrate Socio-Economic, Physical, and Policy Index in a Vulnerability Contribution Analysis. Sustain. Cities Soc. 2020, 54, 102004. [Google Scholar] [CrossRef]
- Frank, L.D.; Pivo, G. Impacts of Mixed Use and Density on Utilization of Three Modes of Travel: Single-Occupant Vehicle, Transit, and Walking. Transp. Res. Rec. 1994, 1466, 44–52. [Google Scholar]
- Beenackers, M.A.; Oude Groeniger, J.; Kamphuis, C.B.M.; Van Lenthe, F.J. Urban Population Density and Mortality in a Compact Dutch City: 23-Year Follow-up of the Dutch GLOBE Study. Health Place 2018, 53, 79–85. [Google Scholar] [CrossRef]
- Meijer, M.; Mette Kejs, A.; Stock, C.; Bloomfield, K.; Ejstrud, B.; Schlattmann, P. Population Density, Socioeconomic Environment and All-Cause Mortality: A Multilevel Survival Analysis of 2.7 Million Individuals in Denmark. Health Place 2012, 18, 391–399. [Google Scholar] [CrossRef]
- Wu, S.; Zhou, S.; Bao, H.; Chen, D.; Wang, C.; Li, B.; Tong, G.; Yuan, Y.; Xu, B. Improving Risk Management by Using the Spatial Interaction Relationship of Heavy Metals and PAHs in Urban Soil. J. Hazard. Mater. 2019, 364, 108–116. [Google Scholar] [CrossRef]
- Hou, X.; Wu, S.; Chen, D.; Cheng, M.; Yu, X.; Yan, D.; Dang, Y.; Peng, M. Can Urban Public Services and Ecosystem Services Achieve Positive Synergies? Ecol. Indic. 2021, 124, 107433. [Google Scholar] [CrossRef]
- Stewart, I.D.; Oke, T.R. Local Climate Zones for Urban Temperature Studies. Bull. Am. Meteorol. Soc. 2012, 93, 1879–1900. [Google Scholar] [CrossRef]
- Liu, M.; Huang, Y.; Ma, Z.; Jin, Z.; Liu, X.; Wang, H.; Liu, Y.; Wang, J.; Jantunen, M.; Bi, J.; et al. Spatial and Temporal Trends in the Mortality Burden of Air Pollution in China: 2004–2012. Environ. Int. 2017, 98, 75–81. [Google Scholar] [CrossRef] [Green Version]
- So, R.; Andersen, Z.J.; Chen, J.; Stafoggia, M.; de Hoogh, K.; Katsouyanni, K.; Vienneau, D.; Rodopoulou, S.; Samoli, E.; Lim, Y.-H.; et al. Long-Term Exposure to Air Pollution and Mortality in a Danish Nationwide Administrative Cohort Study: Beyond Mortality from Cardiopulmonary Disease and Lung Cancer. Environ. Int. 2022, 164, 107241. [Google Scholar] [CrossRef]
- Zhang, P.; Yang, L.; Ma, W.; Wang, N.; Wen, F.; Liu, Q. Spatiotemporal Estimation of the PM2.5 Concentration and Human Health Risks Combining the Three-Dimensional Landscape Pattern Index and Machine Learning Methods to Optimize Land Use Regression Modeling in Shaanxi, China. Environ. Res. 2022, 208, 112759. [Google Scholar] [CrossRef]
- Aram, F.; Higueras García, E.; Solgi, E.; Mansournia, S. Urban Green Space Cooling Effect in Cities. Heliyon 2019, 5, e01339. [Google Scholar] [CrossRef] [Green Version]
- Tan, X.; Sun, X.; Huang, C.; Yuan, Y.; Hou, D. Comparison of Cooling Effect between Green Space and Water Body. Sustain. Cities Soc. 2021, 67, 102711. [Google Scholar] [CrossRef]
- Shareef, S.; Abu-Hijleh, B. The Effect of Building Height Diversity on Outdoor Microclimate Conditions in Hot Climate. A Case Study of Dubai-UAE. Urban Clim. 2020, 32, 100611. [Google Scholar] [CrossRef]
- Li, J.; Auchincloss, A.H.; Hirsch, J.A.; Melly, S.J.; Moore, K.A.; Peterson, A.; Sánchez, B.N. Exploring the Spatial Scale Effects of Built Environments on Transport Walking: Multi-Ethnic Study of Atherosclerosis. Health Place 2021, 73, 102722. [Google Scholar] [CrossRef]
- Ghasemi, Z.; Esfahani, M.A.; Bisadi, M. Promotion of Urban Environment by Consideration of Human Thermal & Wind Comfort: A Literature Review. Procedia Soc. Behav. Sci. 2015, 201, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Stathopoulos, T.; Wu, H.; Zacharias, J. Outdoor Human Comfort in an Urban Climate. Build. Environ. 2004, 39, 297–305. [Google Scholar] [CrossRef]
- Huangfu, P.; Atkinson, R. Long-Term Exposure to NO2 and O3 and All-Cause and Respiratory Mortality: A Systematic Review and Meta-Analysis. Environ. Int. 2020, 144, 105998. [Google Scholar] [CrossRef]
- Li, C.; Wang, Z.; Li, B.; Peng, Z.R.; Fu, Q. Investigating the Relationship between Air Pollution Variation and Urban Form. Build. Environ. 2019, 147, 559–568. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, R.; Xiao, Y.; Huang, B.; Chen, H.; Li, Z. Exploring the Linkage between Greenness Exposure and Depression among Chinese People: Mediating Roles of Physical Activity, Stress and Social Cohesion and Moderating Role of Urbanicity. Health Place 2019, 58, 102168. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; Gascon, M.; Perez-Leon, D.; Mudu, P. Green Spaces and Mortality: A Systematic Review and Meta-Analysis of Cohort Studies. Lancet Planet. Health 2019, 3, e469–e477. [Google Scholar] [CrossRef] [Green Version]
- Dunea, D.; Liu, H.Y.; Iordache, S.; Buruleanu, L.; Pohoata, A. Liaison between Exposure to Sub-Micrometric Particulate Matter and Allergic Response in Children from a Petrochemical Industry City. Sci. Total Environ. 2020, 745, 141170. [Google Scholar] [CrossRef]
- Guan, Y.; Xiao, Y.; Wang, F.; Qiu, X.; Zhang, N. Health Impacts Attributable to Ambient PM2.5 and Ozone Pollution in Major Chinese Cities at Seasonal-Level. J. Clean. Prod. 2021, 311, 127510. [Google Scholar] [CrossRef]
- Chen, R.; Peng, R.D.; Meng, X.; Zhou, Z.; Chen, B.; Kan, H. Seasonal Variation in the Acute Effect of Particulate Air Pollution on Mortality in the China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2013, 450–451, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Location of the study area.

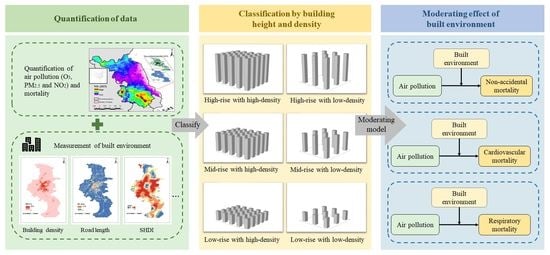
Figure 2.
Overall framework of this study.

Figure 3.
Spatial patterns of the built environment. (a) Building density; (b) building height; (c) standard deviation of building height; (d) NDVI; (e) road length; (f) road crossing; (g) POI of seven types; (h) proportion of construction land; (i) proportion of forestland; (j) proportion of water body; (k) aggregation index; (l) edge density; (m) perimeter-area fractal dimension; (n) patch density; (o) diversity of the built environment; (p) diversity of design; (q) diversity of design; (q) diversity of POI; (r) diversity of land cover.
Figure 3.
Spatial patterns of the built environment. (a) Building density; (b) building height; (c) standard deviation of building height; (d) NDVI; (e) road length; (f) road crossing; (g) POI of seven types; (h) proportion of construction land; (i) proportion of forestland; (j) proportion of water body; (k) aggregation index; (l) edge density; (m) perimeter-area fractal dimension; (n) patch density; (o) diversity of the built environment; (p) diversity of design; (q) diversity of design; (q) diversity of POI; (r) diversity of land cover.


Figure 4.
Correlation coefficient (n = 17,715).

Figure 5.
Moderating effect of the built environment in the relationship between air pollution and mortality in an unclassified area. (a) Moderating effect of the built environment in the relationship between O3 and mortality; (b) moderating effect of the built environment in the relationship between PM2.5 and mortality; (c) moderating effect of the built environment in the relationship between NO2 and mortality.
Figure 5.
Moderating effect of the built environment in the relationship between air pollution and mortality in an unclassified area. (a) Moderating effect of the built environment in the relationship between O3 and mortality; (b) moderating effect of the built environment in the relationship between PM2.5 and mortality; (c) moderating effect of the built environment in the relationship between NO2 and mortality.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Date, resolution, and sources.
| Data | Resolution | Sources |
|---|---|---|
| Road data | OpenStreetMap (http://download.geofabrik.de/asia/china.html# (accessed on 10 February 2022)) | |
| Building dataset | BIGEMAP (http://www.bigemap.com/ (accessed on 16 August 2020)) | |
| Point of interest | point | |
| NDVI | 1 km × 1 km | Resource and Environment Science and Date Center (https://www.resdc.cn/DOI/DOI.aspx?DOIID=49 (accessed on 4 June 2021)) |
| Land cover | 30 m | Resource and Environment Science and Date Center (https://www.resdc.cn/data.aspx?DATAID=184 (accessed on 27 April 2020)) |
| Air pollution (O3, PM2.5, and NO2) | 1 km × 1 km | [27,28] |
| Population density | 1 km × 1 km | WorldPop (www.worldpop.org (accessed on 7 February 2022)) |
| Mortality | Jiangsu Provincial Center for Disease Prevention and Control [29,30] |
Table 2.
Description of 24 indexes of the built environment.
| Category | Index | Description of Index |
|---|---|---|
| Design | Building density (BD) | The ratio of the building footprint area to grid area |
| Building height (BH) | Average of all building heights within the grid | |
| Standard deviation of building height (SDBH) | The standard deviation of all building heights within the grid | |
| NDVI | The greenness within the grid | |
| Road length (RL) | The total length of roads within the grid | |
| Road crossing (RCS) | Number of road crossings within the grid | |
| Destination | Hygiene facility (HF) | Number of hospital and health care facilities within the grid |
| Government agency (GA) | Number of government agencies within the grid | |
| Residential community (RCM) | Number of residential communities within the grid | |
| Industrial park (IP) | Number of industrial parks within the grid | |
| Traffic facility (TF) | Number of traffic facilities within the grid | |
| Gas station (GS) | Number of gas stations within the grid | |
| Catering facility (CF) | Number of catering service facilities within the grid | |
| Land cover | Construction land (CL) | Proportion of construction land within the grid |
| Forestland (FL) | Proportion of forestland within the grid | |
| Water area (WA) | Proportion of water area within the grid | |
| Landscape | AI | Aggregation index |
| ED | Edge density | |
| PAFRAC | Perimeter-area fractal dimension | |
| PD | Patch density | |
| Diversity | Diversity of built environment (DBE) | Diversity of built environment factors |
| Diversity of design (DD) | Diversity of six indexes of design | |
| Diversity of POI (DPOI) | The POI mix | |
| Shannon’s diversity index (SHDI) | Diversity of land cover |
Table 3.
Results of regression models.
| Dependent variable: non-accidental mortality | ||||
|---|---|---|---|---|
| Independent variable | B | S.E. | β | p |
| O3 | 0.125 | 0.033 | 0.026 | 0.000 |
| Population density | 0.003 | 0.000 | 0.426 | 0.000 |
| PM2.5 | 0.133 | 0.028 | 0.032 | 0.000 |
| Population density | 0.003 | 0.000 | 0.423 | 0.000 |
| NO2 | 0.256 | 0.043 | 0.047 | 0.000 |
| Population density | 0.003 | 0.000 | 0.402 | 0.000 |
| Dependent variable: cardiovascular mortality | ||||
| Independent variable | B | S.E. | β | p |
| O3 | 0.080 | 0.019 | 0.033 | 0.000 |
| Population density | 0.001 | 0.000 | 0.392 | 0.000 |
| PM2.5 | 0.084 | 0.016 | 0.040 | 0.000 |
| Population density | 0.001 | 0.000 | 0.388 | 0.000 |
| NO2 | 0.106 | 0.025 | 0.040 | 0.000 |
| Population density | 0.001 | 0.000 | 0.370 | 0.000 |
| Dependent variable: respiratory mortality | ||||
| Independent variable | B | S.E. | β | p |
| O3 | 0.012 | 0.008 | 0.015 | 0.139 |
| Population density | 0.000 | 0.000 | 0.460 | 0.000 |
| PM2.5 | 0.007 | 0.007 | 0.010 | 0.304 |
| Population density | 0.000 | 0.000 | 0.459 | 0.000 |
| NO2 | 0.029 | 0.009 | 0.039 | 0.000 |
| Population density | 0.000 | 0.000 | 0.438 | 0.000 |
B is the unstandardized coefficient; S.E. is the standard error; β is the standardized coefficient.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wang, C.; Sheng, Y.; Wang, J.; Wang, Y.; Wang, P.; Huang, L. Air Pollution and Human Health: Investigating the Moderating Effect of the Built Environment. Remote Sens. 2022, 14, 3703. https://doi.org/10.3390/rs14153703
AMA Style
Wang C, Sheng Y, Wang J, Wang Y, Wang P, Huang L. Air Pollution and Human Health: Investigating the Moderating Effect of the Built Environment. Remote Sensing. 2022; 14(15):3703. https://doi.org/10.3390/rs14153703
Chicago/Turabian StyleWang, Chenglong, Yunliang Sheng, Jiaming Wang, Yiyi Wang, Peng Wang, and Lei Huang. 2022. "Air Pollution and Human Health: Investigating the Moderating Effect of the Built Environment" Remote Sensing 14, no. 15: 3703. https://doi.org/10.3390/rs14153703
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.