Adherence to Mediterranean Diet Related with Physical Fitness and Physical Activity in Schoolchildren Aged 6–13

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Procedures
2.2.1. Adherence to the Mediterranean Diet (MD)
Mediterranean Diet Quality Index for Children and Teenagers (KIDMED Index)
2.2.2. ALPHA-FIT Test Battery
Anthropometric Measurements
Cardiorespiratory Fitness (CRF)
Muscular Fitness
Motor Fitness
2.2.3. Physical Activity
Physical Activity Questionnaire for Older Children (PAQ-C)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pate, R.R. The Evolving Definition of Physical Fitness. Quest 1988, 40, 174–179. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefits in Children and Adolescents? A Systematic Review and Meta-Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Mintjens, S.; Menting, M.D.; Daams, J.G.; van Poppel, M.N.M.; Roseboom, T.J.; Gemke, R.J.B.J. Cardiorespiratory Fitness in Childhood and Adolescence Affects Future Cardiovascular Risk Factors: A Systematic Review of Longitudinal Studies. Sports Med. 2018, 48, 2577–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Lear, S.A.; Hu, W.; Rangarajan, S.; Gasevic, D.; Leong, D.; Iqbal, R.; Casanova, A.; Swaminathan, S.; Anjana, R.M.; Kumar, R.; et al. The effect of physical activity on mortality and cardiovascular disease in 130,000 people from 17 high-income, middle-income, and low-income countries: The PURE study. Lancet 2017, 390, 2643–2654. [Google Scholar] [CrossRef]
- Teran-Garcia, M.; Rankinen, T.; Bouchard, C. Genes, exercise, growth, and the sedentary, obese child. J. Appl. Physiol. 2008, 105, 988–1001. [Google Scholar] [CrossRef]
- Labayen, I.; Ruiz, J.R.; Ortega, F.B.; Loit, H.M.; Harro, J.; Veidebaum, T.; Sjostrom, M. Intergenerational Cardiovascular Disease Risk Factors Involve Both Maternal and Paternal BMI. Diabetes Care 2010, 33, 894–900. [Google Scholar] [CrossRef] [Green Version]
- Cabanas-Sánchez, V.; Martínez-Gómez, D.; Izquierdo-Gómez, R.; Segura-Jiménez, V.; Castro-Piñero, J.; Veiga, O.L. Association between Clustering of Lifestyle Behaviors and Health-Related Physical Fitness in Youth: The UP&DOWN Study. J. Pediatr. 2018, 199, 41–48. [Google Scholar]
- Mendis, S.; Puska, P.; Norrving, B. Global Atlas on Cardiovascular Disease Prevention and Control; World Heart Federation, World Stroke Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Ribas, L.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Nutrient adequacy and Mediterranean Diet in Spanish school children and adolescents. Eur. J. Clin. Nutr. 2003, 57, S35–S39. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F. Mediterranean diet and non-alcoholic fatty liver disease: New therapeutic option around the corner? World J. Gastroenterol. 2014, 20, 7339. [Google Scholar] [CrossRef] [PubMed]
- García, S.; Herrera, N.; Rodríguez, C.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. KIDMED test; prevalence of low adherence to the mediterranean diet in children and young; a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Serra-Majem, L.; Roman, B.; Estruch, R. Scientific evidence of interventions using the Mediterranean diet: A systematic review. Nutr. Rev. 2006, 64, S27–S47. [Google Scholar] [CrossRef] [PubMed]
- Gotsis, E.; Anagnostis, P.; Mariolis, A.; Vlachou, A.; Katsiki, N.; Karagiannis, A. Health benefits of the Mediterranean Diet: An update of research over the last 5 years. Angiology 2015, 66, 304–318. [Google Scholar] [CrossRef] [PubMed]
- Fraser, B.J.; Schmidt, M.D.; Huynh, Q.L.; Dwyer, T.; Venn, A.J.; Magnussen, C.G. Tracking of muscular strength and power from youth to young adulthood: Longitudinal findings from the Childhood Determinants of Adult Health Study. J. Sci. Med. Sport 2017, 20, 927–931. [Google Scholar] [CrossRef]
- Arriscado, D.; Muros, J.J.; Zabala, M.; Dalmau, J.M. Factors associated with low adherence to a Mediterranean diet in healthy children in northern Spain. Appetite 2014, 80, 28–34. [Google Scholar] [CrossRef]
- Muros, J.J.; Cofre-Bolados, C.; Arriscado, D.; Zurita, F.; Knox, E. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition 2017, 35, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Hermoso, A.; Vegas-Heredia, E.D.; Fernández-Vergara, O.; Ceballos-Ceballos, R.; Andrade-Schnettler, R.; Arellano-Ruiz, P.; Ramírez-Vélez, R. Independent and combined effects of handgrip strength and adherence to a Mediterranean diet on blood pressure in Chilean children. Nutrition 2019, 60, 170–174. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Correa-Bautista, J.; Ojeda-Pardo, M.; Sandoval-Cuellar, C.; García-Hermoso, A.; Carrillo, H.; González-Ruíz, K.; Prieto-Benavides, D.; Tordecilla-Sanders, A.; Martinkėnas, A.; et al. Optimal Adherence to a Mediterranean Diet and High Muscular Fitness Are Associated with a Healthier Cardiometabolic Profile in Collegiate Students. Nutrients 2018, 10, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosa Guillamón, A.; García-Cantó, E.; Rodríguez García, P.L.; Pérez Soto, J.J.; Tárraga Marcos, L.; Tárraga López, P.J. Actividad física, condición física y estatus nutricional en escolares de 8 a 12 años. Physical activity, physical fitness and nutritional status in schoolchildren from 8 to 12 years. Nutr. Hosp. 2017, 34, 1292–1298. [Google Scholar]
- Evaristo, O.S.; Moreira, C.; Lopes, L.; Abreu, S.; Agostinis-Sobrinho, C.; Oliveira-Santos, J.; Póvoas, S.; Oliveira, A.; Santos, R.; Mota, J. Associations between physical fitness and adherence to the Mediterranean diet with health-related quality of life in adolescents: Results from the LabMed Physical Activity Study. Eur. J. Public Health 2018, 28, 631–635. [Google Scholar] [CrossRef]
- Agostinis-Sobrinho, C.; Santos, R.; Rosário, R.; Moreira, C.; Lopes, L.; Mota, J.; Martinkenas, A.; García-Hermoso, A.; Correa-Bautista, J.; Ramírez-Vélez, R. Optimal Adherence to a Mediterranean Diet May Not Overcome the Deleterious Effects of Low Physical Fitness on Cardiovascular Disease Risk in Adolescents: A Cross-Sectional Pooled Analysis. Nutrients 2018, 10, 815. [Google Scholar] [CrossRef] [Green Version]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Concomitant Associations between Lifestyle Characteristics and Physical Activity Status in Children and Adolescents. J. Res. Health Sci. 2019, 19, e00439. [Google Scholar] [PubMed]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef] [PubMed]
- IDEFICS Consortium; Tognon, G.; Moreno, L.A.; Mouratidou, T.; Veidebaum, T.; Molnár, D.; Russo, P.; Siani, A.; Akhandaf, Y.; Krogh, V.; et al. Adherence to a Mediterranean-like dietary pattern in children from eight European countries. The IDEFICS study. Int. J. Obes. 2014, 38, S108–S114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, M.; Bilal, U.; Díez, J. Food Environment. In Encyclopedia of Food and Health; Elsevier: Amsterdam, The Netherlands, 2016; pp. 22–26. [Google Scholar]
- Grao-Cruces, A.; Fernández-Martínez, A.; Nuviala, A. Association of Fitness with Life Satisfaction, Health Risk Behaviors, and Adherence to the Mediterranean Diet in Spanish Adolescents. J. Strength Cond. Res. 2014, 28, 2164–2172. [Google Scholar] [CrossRef]
- Roman-Viñas, B.; Zazo, F.; Martínez-Martínez, J.; Aznar-Laín, S.; Serra-Majem, L. Results from Spain’s 2018 Report Card on Physical Activity for Children and Youth. J. Phys. Act. Health 2018, 15, S411–S412. [Google Scholar] [CrossRef] [Green Version]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2019, 53, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Castro-Pinero, J.; Espana-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavon, D.; Chillon, P.; Girela-Rejon, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Brook, C.G. Determination of body composition of children from skinfold measurements. Arch. Dis. Child. 1971, 46, 182–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siri, W.E. The Gross Composition of the Body. In Advances in Biological and Medical Physics; Lawrence, J.H., Gofman, J.W., Eds.; Elsevier: Amsterdam, The Netherlands, 1956; Volume 4, pp. 239–280. [Google Scholar]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 m shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- España-Romero, V.; Artero, E.G.; Santaliestra-Pasias, A.M.; Gutierrez, A.; Castillo, M.J.; Ruiz, J.R. Hand Span Influences Optimal Grip Span in Boys and Girls Aged 6 to 12 Years. J. Hand Surg. 2008, 33, 378–384. [Google Scholar] [CrossRef]
- Kowalski, K.C.; Crocker, P.R.E.; Kowalski, N.P. Convergent Validity of the Physical Activity Questionnaire for Adolescents. Pediatr. Exerc. Sci. 1997, 9, 342–352. [Google Scholar] [CrossRef]
- Martínez-Gómez, D.; Martínez-de-Haro, V.; Pozo, T.; Welk, G.J.; Villagra, A.; Calle, M.E.; Marcos, A.; Veiga, O.L. Reliability and validity of the PAQ-A questionnaire to assess physical activity in Spanish adolescents. Rev. Esp. Salud Publica 2009, 83, 427–439. [Google Scholar] [CrossRef]
- Bervoets, L.; Van Noten, C.; Van Roosbroeck, S.; Hansen, D.; Van Hoorenbeeck, K.; Verheyen, E.; Van Hal, G.; Vankerckhoven, V. Reliability and Validity of the Dutch Physical Activity Questionnaires for Children (PAQ-C) and Adolescents (PAQ-A). Arch. Public Health 2014, 72, 47. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Archero, F.; Ricotti, R.; Solito, A.; Carrera, D.; Civello, F.; Di Bella, R.; Bellone, S.; Prodam, F. Adherence to the Mediterranean Diet among School Children and Adolescents Living in Northern Italy and Unhealthy Food Behaviors Associated to Overweight. Nutrients 2018, 10, 1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Marventano, S.; Buscemi, S.; Scuderi, A.; Matalone, M.; Platania, A.; Giorgianni, G.; Rametta, S.; Nolfo, F.; Galvano, F.; et al. Factors Associated with Adherence to the Mediterranean Diet among Adolescents Living in Sicily, Southern Italy. Nutrients 2013, 5, 4908–4923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schutte, N.M.; Nederend, I.; Hudziak, J.J.; de Geus, E.J.C.; Bartels, M. Differences in Adolescent Physical Fitness: A Multivariate Approach and Meta-analysis. Behav. Genet. 2016, 46, 217–227. [Google Scholar] [CrossRef] [Green Version]
- Foster, C.; Moore, J.B.; Singletary, C.R.; Skelton, J.A. Physical activity and family-based obesity treatment: A review of expert recommendations on physical activity in youth. Clin. Obes. 2018, 8, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Tubb, L.; Fingers, S.T.; Chen, S.; Caffrey, J.L. Associations of Physical Activity and Dietary Behaviors with Children’s Health and Academic Problems. J. Sch. Health 2013, 83, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Galvano, F. Mediterranean diet adherence in children and adolescents in southern European countries. NFS J. 2016, 3, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Zurita-Ortega, F.; San Román-Mata, S.; Chacón-Cuberos, R.; Castro-Sánchez, M.; Muros, J. Adherence to the Mediterranean Diet Is Associated with Physical Activity, Self-Concept and Sociodemographic Factors in University Student. Nutrients 2018, 10, 966. [Google Scholar] [CrossRef] [Green Version]
- Chacón-Cuberos, R.; Zurita-Ortega, F.; Martínez-Martínez, A.; Olmedo-Moreno, E.; Castro-Sánchez, M. Adherence to the Mediterranean Diet Is Related to Healthy Habits, Learning Processes, and Academic Achievement in Adolescents: A Cross-Sectional Study. Nutrients 2018, 10, 1566. [Google Scholar] [CrossRef] [Green Version]
- Arriscado, D.; Muros, J.J.; Zabala, M.; Dalmau, J.M. Hábitos de práctica física en escolares: Factores influyentes y relaciones con la condición física. Nutr. Hosp. 2015, 31, 1232–1239. [Google Scholar]


{kind=link}
| Variables | Boys | Girls | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
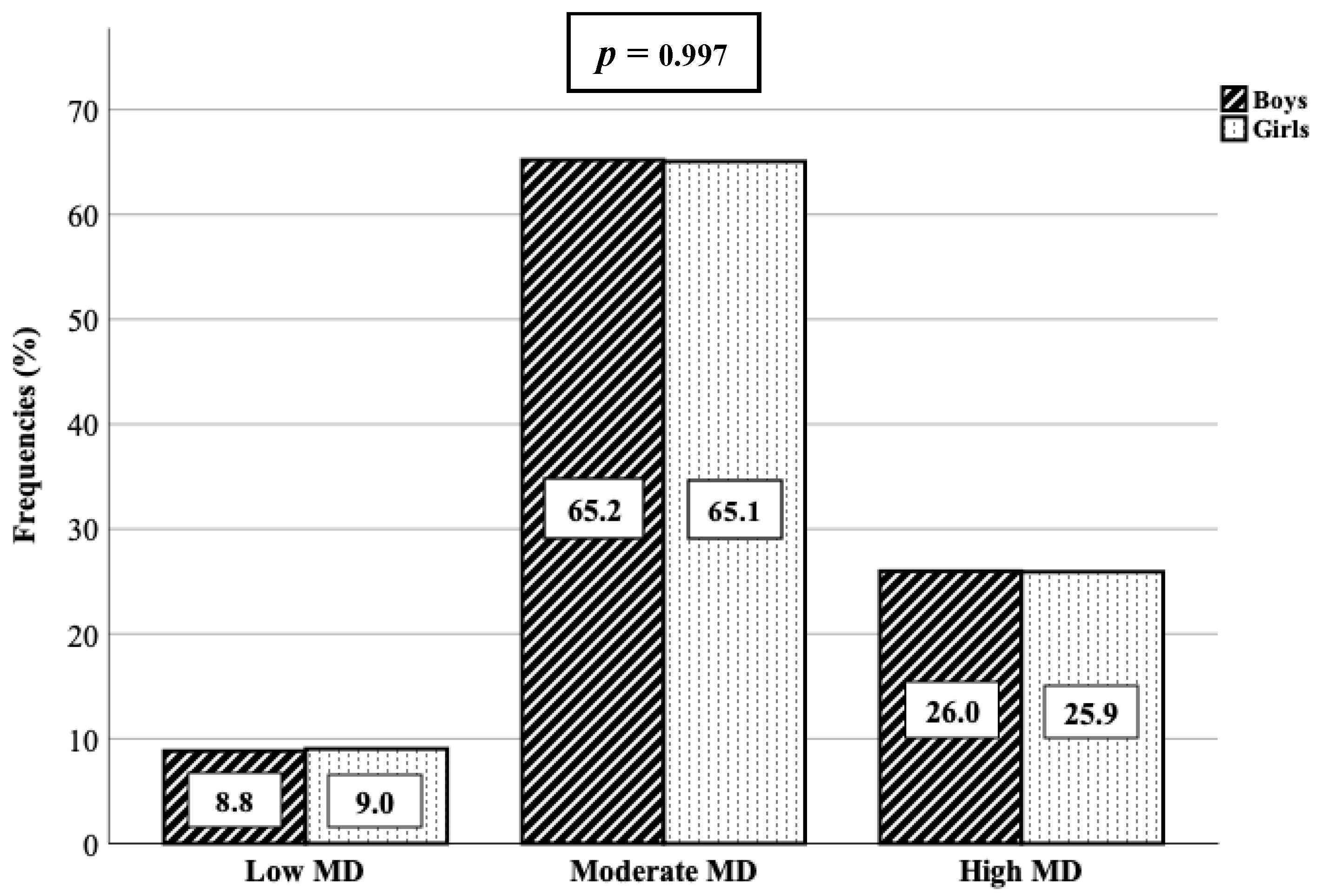
| Low MD n = 18 (8.8%) | Moderate MD n = 133 (65.2%) | High MD n = 53 (26.0%) | p | d | Low MD n = 15 (9.0%) | Moderate MD n = 108 (65.1%) | High MD n = 43 (25.9%) | p | d | |
| Age (years) | 9.1 ± 1.3 | 8.9 ± 1.8 | 8.5 ± 1.9 | 0.378 | 0.03 | 8.7 ± 1.7 | 8.4 ± 1.8 | 8.6 ± 1.8 | 0.779 | 0.19 |
| Weight (kg) | 39.07 ± 10.77 | 36.19 ± 10.15 | 36.03 ± 12.23 | 0.451 | 0.09 | 33.30 ± 12.05 | 34.04 ± 10.34 | 37.48 ± 12.38 | 0.208 | 0.17 |
| Height (m) | 1.39 ± 0.07 | 1.37 ± 0.11 | 1.36 ± 0.13 | 0.637 | 0.15 | 1.34 ± 0.12 | 1.34 ± 0.12 | 1.35 ± 0.14 | 0.812 | 0.20 |
| BMI (kg/m2) | 20.07 ± 4.23 | 18.96 ± 3.39 | 19.02 ± 3.68 | 0.560 | 0.13 | 18.11 ± 3.84 | 18.73 ± 3.69 | 20.07 ± 4.41 | 0.043* | 0.33 |
| BMI (z-score) | 0.84 ± 0.94 | 1.12 ± 1.36 | 1.27 ± 1.04 | 0.385 | 0.04 | 0.99 ± 0.88 | 1.20 ± 1.25 | 1.09 ± 1.17 | 0.832 | 0.20 |
| WC (cm) | 64.27±5.98 | 63.18 ± 7.52 | 62.33 ± 8.6 | 0.202 | 0.16 | 59.18 ± 8.13 | 60.35 ± 8.88 | 62.64 ± 8.03 | 0.120 | 0.24 |
| WHtR (WC/Height (cm)) | 0.46 ± 0.04 | 0.46 ± 0.04 | 0.46 ± 0.04 | 0.884 | 0.19 | 0.44 ± 0.04 | 0.45 ± 0.06 | 0.46 ± 0.05 | 0.082 | 0.27 |
| BF (kg) | 12.50 ± 6.39 | 10.91 ± 5.43 | 11.04 ± 6.46 | 0.491 | 0.11 | 10.72 ± 6.23 | 10.77 ± 5.78 | 12.76 ± 6.73 | 0.161 | 0.20 |
| BF (%) | 30.40 ± 7.68 | 28.76 ± 6.36 | 28.67 ± 7.06 | 0.632 | 0.15 | 30.14 ± 7.12 | 29.88 ± 7.70 | 32.35 ± 7.40 | 0.181 | 0.19 |
| FFM (kg) | 26.56 ± 4.83 | 25.29 ± 5.21 | 24.99 ± 6.12 | 0.509 | 0.11 | 22.58 ± 6.04 | 23.27 ± 5.26 | 24.72 ± 6.41 | 0.328 | 0.08 |
| FFM (%) | 69.60 ± 7.68 | 71.24 ± 6.36 | 71.33 ± 7.06 | 0.632 | 0.15 | 69.86 ± 7.12 | 70.12 ± 7.70 | 67.65 ± 7.40 | 0.181 | 0.19 |
| Handgrip strength (kg) | 13.08 ± 2.46 | 13.86 ± 4.07 | 13.12 ± 4.04 | 0.433 | 0.18 | 12.51 ± 4.35 | 11.91 ± 3.54 | 12.90 ± 4.19 | 0.339 | 0.23 |
| Handgrip strength/BW | 0.34 ± 0.08 | 0.39 ± 0.08 | 0.38 ± 0.09 | 0.154 | 0.27 | 0.38 ± 0.05 | 0.36 ± 0.08 | 0.35 ± 0.07 | 0.484 | 0.19 |
| Standing broad jump (cm) | 120.2 ± 29.9 | 116.2 ± 24.6 | 120.5 ± 26.9 | 0.538 | 0.16 | 108.6 ± 25.8 | 106.6 ± 22.2 | 111.2 ± 23.5 | 0.537 | 0.18 |
| 4 × 10 m Shuttle Run Test (s) | 13.49 ± 1.44 | 13.52 ± 1.64 | 13.57 ± 1.25 | 0.710 | 0.16 | 14.32 ± 1.53 | 14.05 ± 1.11 | 14.03 ± 1.61 | 0.690 | 0.18 |
| 20 m Shuttle Run Test (laps) | 16.1 ± 12.8 a | 21.0 ± 14.3 | 23.4 ± 13.4 | 0.048 * | 0.29 | 15.5 ± 7.1 | 16.3 ± 9.7 | 17.9 ± 9.6 | 0.412 | 0.08 |
| CRF (mL/kg/min) | 43.31 ± 4.00 a | 45.20 ± 4.29 | 46.36 ± 4.56 | 0.019 * | 0.35 | 43.98 ± 4.03 | 44.60 ± 4.01 | 44.89 ± 3.73 | 0.699 | 0.18 |
| PAQ-C (score) | 1.87 ± 0.53 a,b | 2.23 ± 0.45 | 2.28 ± 0.52 | 0.040 * | 0.30 | 1.96 ± 0.38 | 2.04 ± 0.40 a | 2.22 ± 0.45 | 0.016 * | 0.40 |
| Variables | Crude | Adjusted # |
|---|---|---|
| Handgrip strength (kg) | −0.015 (0.779) | 0.065 (0.213) |
| Handgrip strength/BW | −0.010 (0.841) | 0.040 (0.442) |
| Standing broad jump (cm) | 0.069 (0.188) | 0.147 ** (0.005) |
| 4 x 10 m Shuttle Run Test (s) | 0.002 (0.967) | −0.057 (0.276) |
| 20 m Shuttle Run Test (laps) | 0.104 * (0.045) | 0.141 ** (0.007) |
| CRF (mL/kg/min) | 0.134 ** (0.010) | 0.144 ** (0.006) |
| PAQ-C (score) | 0.162 ** (0.002) | 0.232 *** (<0.001) |
| Predictors | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| Low MD (0–3) | Moderate MD (4–7) | High MD (≥8) | Low MD (0–3) | Moderate MD (4–7) | High MD (≥8) | |
| Handgrip strength (kg) | 1 | 1.01 (0.92–1.11) | 1.01 (0.92–1.12) | 1 | 1.09 (0.93–1.26) | 1.11 (0.94–1.32) |
| Handgrip strength/BW | 1 | 6.68 (0.08–576.95) | 1.68 (0.01–212.40) | 1 | 11.30 (0.05–2648.77) | 9.52 (0.03–3625.12) |
| Standing broad jump (cm) | 1 | 1.00 (0.98–1.01) | 1.00 (0.99–1.02) | 1 | 0.99 (0.97–1.01) | 1.01 (0.99–1.03) |
| 4 × 10 m Shuttle Run Test (s) | 1 | 0.95 (0.74–1.22) | 0.96 (0.73–1.25) | 1 | 0.91 (0.67–1.25) | 0.83 (0.59–1.17) |
| 20 m Shuttle Run Test (nº laps) | 1 | 1.03 (0.99–1.06) | 1.04 * (1.00–1.08) | 1 | 1.03 (0.99–1.07) | 1.06 ** (1.01–1.11) |
| CRF (mL/kg/min) | 1 | 1.08 (0.99–1.18) | 1.13 * (1.02–1.25) | 1 | 1.11 (0.96–1.28) | 1.23 ** (1.06–1.44) |
| PAQ-C (score) | 1 | 3.72 ** (1.49–9.28) | 6.24 *** (2.33–16.70) | 1 | 4.06 ** (1.58–10.44) | 7.51 *** (2.71–20.86) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gil, J.F.; Brazo-Sayavera, J.; García-Hermoso, A.; Yuste Lucas, J.L. Adherence to Mediterranean Diet Related with Physical Fitness and Physical Activity in Schoolchildren Aged 6–13. Nutrients 2020, 12, 567. https://doi.org/10.3390/nu12020567
López-Gil JF, Brazo-Sayavera J, García-Hermoso A, Yuste Lucas JL. Adherence to Mediterranean Diet Related with Physical Fitness and Physical Activity in Schoolchildren Aged 6–13. Nutrients. 2020; 12(2):567. https://doi.org/10.3390/nu12020567
Chicago/Turabian StyleLópez-Gil, José Francisco, Javier Brazo-Sayavera, Antonio García-Hermoso, and Juan Luis Yuste Lucas. 2020. "Adherence to Mediterranean Diet Related with Physical Fitness and Physical Activity in Schoolchildren Aged 6–13" Nutrients 12, no. 2: 567. https://doi.org/10.3390/nu12020567