Relationship between Erythrocyte Omega-3 Content and Obesity Is Gender Dependent

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Participants and Data
2.2. Assessments
2.2.1. Anthropometric Measurements
2.2.2. Body Composition
2.2.3. Assessment of Fatty Acid Profiles
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics

{kind=link}
{kind=link}
| Males | Females | |
|---|---|---|
| Age (year) | 45.6 ± 11.6 (185) | 47.5 ± 12.3 (291) |
| Weight (kg) | 99.4 ± 17.3 (185) | 91.3 ± 19.9 (291) |
| Height (m) | 177.7 ± 7.0 (185) | 163.6 ± 6.8 (291) |
| Body mass index (kg/m2) | 31.4 ± 5.0 (185) | 34.0 ± 6.8 (291) |
| Waist circumference (cm) | 110.0 ± 13.3 (133) | 105.3 ± 16.1 (244) |
| Fat mass (% of total mass) | 34.5 ± 6.3 (133) | 48.2 ± 5.2 (243) |
3.2. Erythrocyte Fatty Acids
| Males (185) | Females (282) | |
|---|---|---|
| EPA | 0.85 ± 0.35 | 0.91 ± 0.42 |
| DPA ** | 2.47 ± 0.37 | 2.32 ± 0.36 |
| DHA | 4.25 ± 0.95 | 4.42 ± 1.02 |
| Omega-3 Index * | 5.10 ± 1.18 | 5.33 ± 1.33 |
| Body mass index (kg/m2) | Waist circumference (cm) | Body Fat (%) | |
|---|---|---|---|
| N (all subjects) | 476 | 377 | 376 |
| EPA | −0.016 | −0.143 * | −0.054 |
| DPA | −0.073 | −0.116 | −0.264 *** |
| DHA | −0.191 *** | −0.298 *** | −0.117 |
| Omega-3 Index | −0.154 ** | −0.275 *** | −0.108 |
| N (males only) | 185 | 133 | 133 |
| EPA | 0.087 | −0.062 | −0.147 |
| DPA | −0.016 | −0.201 | −0.228 * |
| DHA | −0.077 | −0.144 | −0.185 |
| Omega-3 Index | −0.037 | −0.133 | −0.192 |
| N (females only) | 291 | 244 | 243 |
| EPA | 0.080 | −0.164 * | −0.172 * |
| DPA | −0.047 | −0.125 | −0.143 |
| DHA | −0.276 ** | −0.353 *** | −0.329 ** |
| Omega-3 Index | −0.236 ** | −0.322 *** | −0.306 ** |
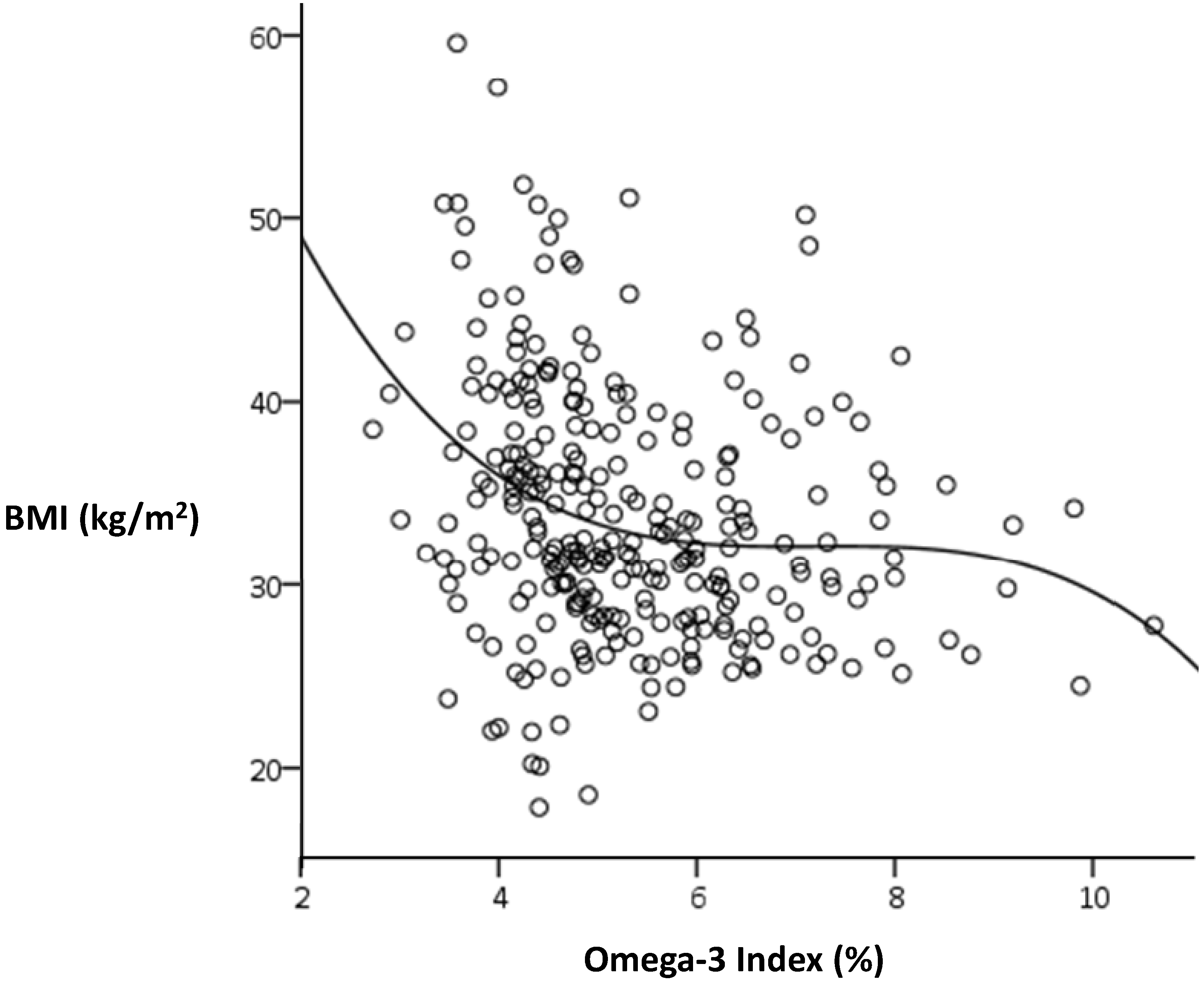
3.3. Associations between the Omega-3 Index and BMI

4. Discussion

Abbreviations
| BMI | body mass index |
| WC | waist circumference |
| BF | body fat |
| LC n-3 PUFA | long-chain omega-3 polyunsaturated fatty acids |
| EPA | eicosapentaenoic acid |
| DPA | docosapentaenoic acid |
| DHA | docosahexaenoic acid |
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Buckley, J.D.; Howe, P.R.C. Anti-obesity effects of long-chain omega-3 polyunsaturated fatty acids. Obes. Rev. 2009, 10, 648–659. [Google Scholar] [CrossRef]
- Buckley, J.D.; Howe, P.R.C. Long-chain omega-3 polyunsaturated fatty acids may be beneficial for reducing obesity-a review. Nutrients 2010, 2, 1212–1230. [Google Scholar] [CrossRef]
- Munro, I.A.; Garg, M.L. Prior supplementation with long chain omega-3 polyunsaturated fatty acids promotes weight loss in obese adults: A double-blinded randomised controlled trial. Food Funct. 2013, 4, 650–658. [Google Scholar] [CrossRef]
- He, K.; Rimm, E.; Merchant, A.; Rosner, B.; Stampfer, M.; Willett, W.; Ascherio, A. Fish consumption and risk of stroke in men. J. Am. Med. Assoc. 2002, 288, 3130–3136. [Google Scholar] [CrossRef]
- Iso, H.; Rexrode, K.M.; Stampfer, M.J.; Manson, J.E.; Colditz, G.A.; Speizer, F.E.; Hennekens, C.H.; Willett, W.C. Intake of fish and omega-3 fatty acids and risk of stroke in women. J. Am. Med. Assoc. 2001, 285, 304–312. [Google Scholar] [CrossRef]
- Dewailly, E.; Blanchet, C.; Gingras, S.; Lemieux, S.; Holub, B.J. Cardiovascular disease risk factors and n-3 fatty acid status in the adult population of James Bay Cree. Am. J. Clin. Nutr. 2002, 76, 85–92. [Google Scholar]
- Dewailly, E.E.; Blanchet, C.; Gingras, S.; Lemieux, S.; Sauve, L.; Bergeron, J.; Holub, B.J. Relations between n-3 fatty acid status and cardiovascular disease risk factors among Quebecers. Am. J. Clin. Nutr. 2001, 74, 603–611. [Google Scholar]
- Dewailly, E.; Blanchet, C.; Lemieux, S.; Sauve, L.; Gingras, S.; Ayotte, P.; Holub, B.J. n-3 Fatty acids and cardiovascular disease risk factors among the Inuit of Nunavik. Am. J. Clin. Nutr. 2001, 74, 464–473. [Google Scholar]
- Micallef, M.; Munro, I.; Phang, M.; Garg, M. Plasma n-3 Polyunsaturated fatty acids are negatively associated with obesity. Br. J. Nutr. 2009, 102, 1370–1374. [Google Scholar] [CrossRef]
- Klein-Platat, C.; Drai, J.; Oujaa, M.; Schlienger, J.L.; Simon, C. Plasma fatty acid composition is associated with the metabolic syndrome and low-grade inflammation in overweight adolescents. Am. J. Clin. Nutr. 2005, 82, 1178–1184. [Google Scholar]
- Karlsson, M.; Marild, S.; Brandberg, J.; Lonn, L.; Friberg, P.; Strandvik, B. Serum phospholipid fatty acids, adipose tissue, and metabolic markers in obese adolescents. Obesity 2006, 14, 1931–1939. [Google Scholar] [CrossRef]
- Brown, A.; Pang, E.; Roberts, D. Persistent changes in the fatty acid composition of erythrocyte membranes after moderate intake of n-3 polyunsaturated fatty acids: Study design implications. Am. J. Clin. Nutr. 1991, 54, 668–673. [Google Scholar]
- Katan, M.; Deslypere, J.; van Birgelen, A.; Penders, M.; Zegwaard, M. Kinetics of the incorporation of dietary fatty acids into serum cholesteryl esters, erythrocyte membranes, and adipose tissue: An 18-month controlled study. J. Lipid Res. 1997, 38, 2012–2022. [Google Scholar]
- Harris, W.S.; Pottala, J.V.; Lacey, S.M.; Vasan, R.S.; Larson, M.G.; Robins, S.J. Clinical correlates and heritability of erythrocyte eicosapentaenoic and docosahexaenoic acid content in the Framingham Heart Study. Atherosclerosis 2012, 225, 425–431. [Google Scholar] [CrossRef]
- Norton, K.I.; Olds, T.S. Anthropometrica; New South Wales Press: Sydney, Australia, 1996. [Google Scholar]
- Milte, C.M.; Sinn, N.; Street, S.J.; Buckley, J.D.; Coates, A.M.; Howe, P.R. Erythrocyte polyunsaturated fatty acid status, memory, cognition and mood in older adults with mild cognitive impairment and healthy controls. Prostaglandins Leukot. Essent. Fat. Acids 2011, 84, 153–161. [Google Scholar] [CrossRef]
- Poudyal, H.; Panchal, S.K.; Diwan, V.; Brown, L. Omega-3 fatty acids and metabolic syndrome: Effects and emerging mechanisms of action. Prog. Lipid Res. 2011, 50, 372–387. [Google Scholar] [CrossRef]
- Barber, E.; Sinclair, A.J.; Cameron-Smith, D. Comparative actions of omega-3 fatty acids on in-vitro lipid droplet formation. Prostaglandins Leukot. Essent. Fat. Acids 2013, 89, 359–366. [Google Scholar] [CrossRef]
- Groh-Wargo, S.; Jacobs, J.; Auestad, N.; O’Connor, D.L.; Moore, J.J.; Lerner, E. Body composition in preterm infants who are fed long-chain polyunsaturated fatty acids: A prospective, randomized, controlled trial. Pediatr. Res. 2005, 57, 712–718. [Google Scholar] [CrossRef]
- Hill, A.; Buckley, J.; Murphy, K.; Howe, P. Combining fish oil supplementation with regular aerobic exercise improves body composition and cardiovascular risk factors. Am. J. Clin. Nutr. 2007, 85, 1267–1274. [Google Scholar]
- Decsi, T.; Kennedy, K. Sex-specific differences in essential fatty acid metabolism. Am. J. Clin. Nutr. 2011, 94, 1914S–1919S. [Google Scholar] [CrossRef]
- Phang, M.; Lincz, L.F.; Garg, M.L. Eicosapentaenoic and docosahexaenoic acid supplementations reduce platelet aggregation and hemostatic markers differentially in men and women. J. Nutr. 2013, 143, 457–463. [Google Scholar] [CrossRef]
- Von Schacky, C. Omega-3 index and cardiovascular health. Nutrients 2014, 6, 799–814. [Google Scholar] [CrossRef]
- Baghai, T.C.; Varallo-Bedarida, G.; Born, C.; Hafner, S.; Schule, C.; Eser, D.; Rupprecht, R.; Bondy, B.; von Schacky, C. Major depressive disorder is associated with cardiovascular risk factors and low Omega-3 Index. J. Clin. Psychiatry 2011, 72, 1242–1247. [Google Scholar] [CrossRef]
- Milte, C.M.; Sinn, N.; Howe, P.R. Polyunsaturated fatty acid status in attention deficit hyperactivity disorder, depression, and Alzheimer’s disease: Towards an omega-3 index for mental health? Nut. Rev. 2009, 67, 573–590. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Howe, P.R.C.; Buckley, J.D.; Murphy, K.J.; Pettman, T.; Milte, C.; Coates, A.M. Relationship between Erythrocyte Omega-3 Content and Obesity Is Gender Dependent. Nutrients 2014, 6, 1850-1860. https://doi.org/10.3390/nu6051850
Howe PRC, Buckley JD, Murphy KJ, Pettman T, Milte C, Coates AM. Relationship between Erythrocyte Omega-3 Content and Obesity Is Gender Dependent. Nutrients. 2014; 6(5):1850-1860. https://doi.org/10.3390/nu6051850
Chicago/Turabian StyleHowe, Peter R. C., Jonathan D. Buckley, Karen J. Murphy, Tahna Pettman, Catherine Milte, and Alison M. Coates. 2014. "Relationship between Erythrocyte Omega-3 Content and Obesity Is Gender Dependent" Nutrients 6, no. 5: 1850-1860. https://doi.org/10.3390/nu6051850