Reducing Postpartum Weight Retention and Improving Breastfeeding Outcomes in Overweight Women: A Pilot Randomised Controlled Trial


Abstract
:1. Introduction
2. Experimental Section

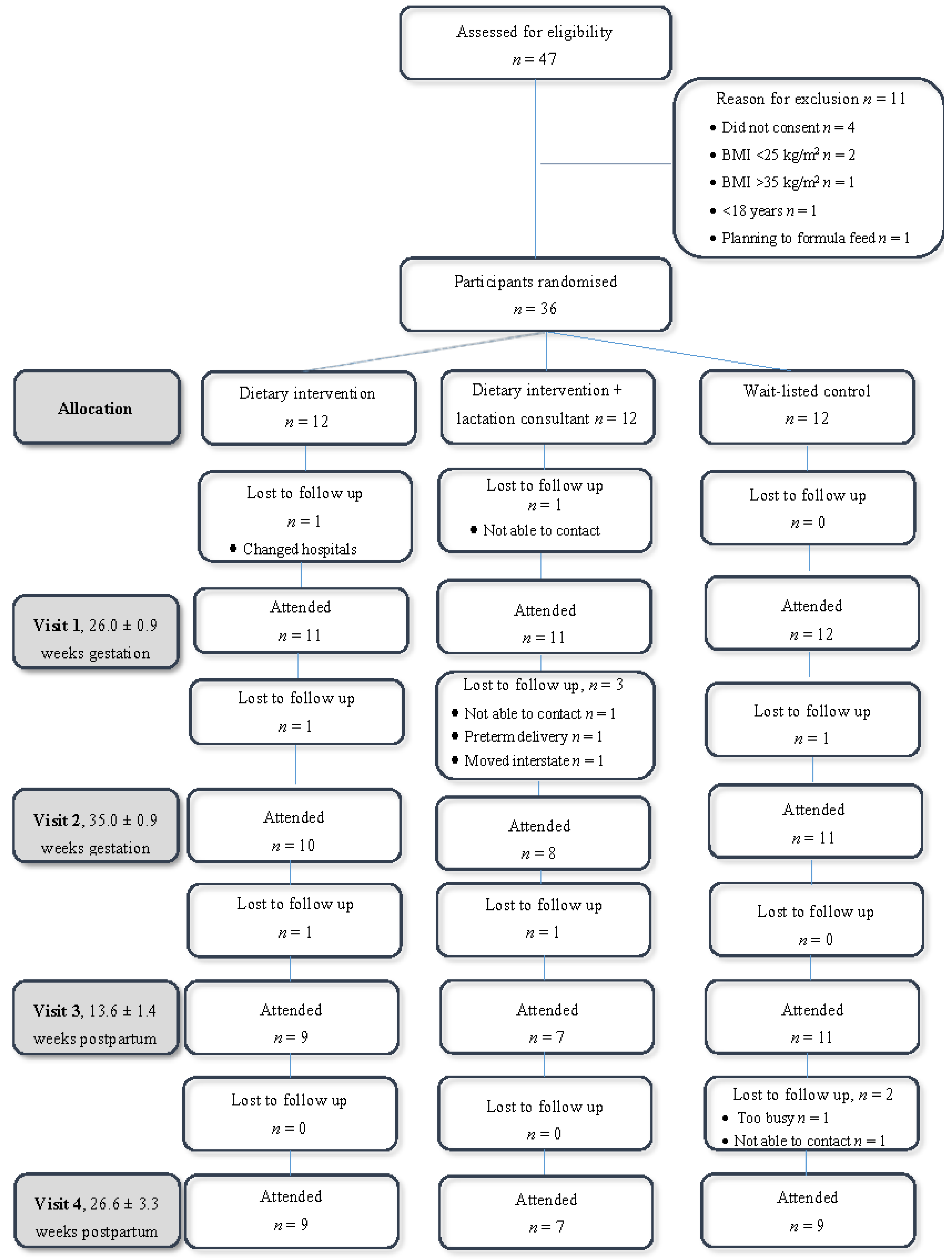
2.1. Participants
2.2. Study Design
2.2.1. Randomisation
2.2.2. Blinding
2.2.3. Dietary Intervention
- Eat a healthy breakfast;
- Pack a daily lunch and snack box ahead of time;
- Use TEMplate™ dinner disc to guide portion size at main meals, including four different coloured vegetables;
- Adjust “extras” (1 extra = 500 kJ) to balance energy expenditure from physical activity and lactation, for example women exclusively breastfeeding were given advice on adding an additional 4 extras to their eating plan, partially breastfeeding were allowed an additional 2 extra servings The APD provided advice on appropriate nutrient dense “extras” that could be added to the diet.
2.2.4. Lactation Support
2.2.5. Outcome Measures
2.2.6. Weight and BMI
2.2.7. Biomarkers
2.2.8. Breastfeeding
2.2.9. Further Data Collection
2.3. Statistical Analyses
3. Results

{kind=link}
| Participant Characteristic | All (n = 34) | Diet (n = 11) | Diet + Lactation Support (n = 11) | Control (n = 12) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 30.9 ± 6.0 | 29.5 ± 7.8 | 31.6 ± 5.1 | 31.3 ± 5.6 | 0.27 |
| Height (cm) | 165.4 ± 6.2 | 165.1 ± 6.5 | 166.8 ± 5.7 | 164.4 ± 6.5 | 0.44 |
| Born in Australia, n (%) | 33/34 (97) | 10/11 (91) | 11/11 (100) | 12/12 (100) | 0.65 |
| Married or de facto, n (%) | 25/31 (81) | 7/10 (70) | 8/9 (89) | 10/12 (83) | 0.63 |
| Education ≥ year 12, n (%) | 26/31 (84) | 9/10 (90) | 8/9 (89) | 9/12 (75) | 0.79 |
| IRSAD ≥ 5, n (%) | 23/32 (72) | 7/10 (70) | 9/10 (90) | 7/12 (58) | 0.22 |
| Smoking, n (%) | 4/34 (12) | 2/11 (18) | 1/11 (9) | 1/12 (8) | 1.00 |
| Multiparous, n (%) | 5/34 (15) | 1/11 (9) | 2/11 (18) | 2/12 (17) | 0.39 |
| Gestational diabetes, n (%) | 3/34 (9) | 2/11 (18) | 1/11 (9) | 0/12 (0) | 0.76 |
| Infant sex, male n (%) | 14/33 (42) | 3/11 (27) | 6/10 (60) | 5/12 (42) | 0.23 |
| Birth weight (kg) | 3.7 (3.3, 4.0) | 3.9 (3.7, 4.1) | 3.5 (3.1, 3.7) | 3.5 (3.2, 4.0) | 0.19 |
| Time | Variable | All (n = 34) | Diet (n = 11) | Diet + Lactation Support (n = 11) | Control (n = 12) |
|---|---|---|---|---|---|
| Pre-pregnancy | Weight (kg) | 80.5 ± 12.0 | 81.5 ± 15.1 | 81.6 ± 9.8 | 78.5 ± 11.3 |
| BMI (kg/m2) | 28.8 (25.4, 32.3) | 27.7 (25.1, 33.7) | 29.4 (25.5, 32.3) | 28.9 (25.2, 32.9) | |
| Pregnancy | Weight gain (kg) a | 13.6 ± 6.6 | 9.8 ± 4.5 | 15.3 ± 7.2 | 16.0 ± 6.7 |
| Postpartum—3 months | Weight | 84.9 ± 13.7 | 84.2 ± 14.0 | 85.9 ± 14.3 | 84.8 ± 14.3 |
| BMI | 30.8 ± 4.2 | 30.7 ± 4.1 | 30.6 ± 5.4 | 31.1 ± 3.9 | |
| Weight retention (kg) b | 4.6 ± 7.4 | 0.91 ± 7.03 | 4.4 ± 7.6 | 7.7 ± 6.8 | |
| Postpartum—6 months | Weight | 85.3 ± 13.0 | 84.2 ± 14.7 | 89.9 ± 11.3 | 82.7 ± 13.1 |
| BMI | 30.7 ± 3.7 | 30.6 ± 4.3 | 31.2 ± 4.4 | 30.3 ± 3.0 | |
| Weight retention | 3.3 ± 4.0 | 0.8 ± 7.2 | 5.6 ± 8.8 | 5.9 ± 4.9 | |
| Weight ≤ pre-pregnancy, n (%) | 5/25 (20) | 3/9 (33) | 2/7 (29) | 1/9 (11) | |
| Weight retention ≥ 5 kg, n (%) | 10/25 (40) | 1/9 (11) | 4/7 (57) | 5/9 (56) |
| Time | Variable | All (n = 34) | Diet (n = 11) | Diet + Lactation Support (n = 11) | Control (n = 12) | p-Value |
|---|---|---|---|---|---|---|
| Pregnancy | Glucose (mmol/L) | 4.2 ± 0.4 | 4.3 ± 0.5 | 4.2 ± 0.4 | 4.2 ± 0.2 | 0.99 |
| Insulin (mIU/L) | 9.1 ± 3.6 | 8.3 ± 3.0 | 8.8 ± 4.4 | 10.1 ± 3.4 | 0.46 | |
| HbA1c (%) | 5.3 (5.2, 5.5) | 5.3 (5.1, 5.5) | 5.3 (5.1, 5.5) | 5.4 (5.2, 5.6) | 0.48 | |
| HOMA-IR a | 1.7 ± 0.8 | 1.6 ± 0.7 | 1.7 ± 0.9 | 1.9 ± 0.7 | 0.62 | |
| Total cholesterol (mmol/L) | 6.8 ± 1.2 | 6.7 ± 1.0 | 6.6 ± 1.2 | 7.1 ± 1.4 | 0.77 | |
| Triglycerides (mmol/L) | 2.3 ± 0.7 | 2.0 ± 0.4 | 2.3 ± 0.8 | 2.6 ± 0.7 | 0.11 | |
| LDL-C (mmol/L) | 3.9 ± 1.1 | 4.0 ± 0.7 | 3.6 ± 1.1 | 4.1 ± 1.3 | 0.56 | |
| HDL-C (mmol/L) | 1.9 ± 0.5 | 1.9 ± 0.6 | 1.9 ± 0.5 | 1.9 ± 0.4 | 0.95 | |
| Total/HDL-C | 3.8 ± 0.8 | 3.7 ± 0.8 | 3.7 ± 1.0 | 3.9 ± 0.7 | 0.78 | |
| CRP (mg/L) | 7.3 (4.8, 12.9) | 11.1 (6.3, 13.7) | 6.7 (3.0, 14.6) | 7.3 (5.2, 9.5) | 0.91 | |
| Postpartum—3 months | Glucose | 4.6 ± 0.5 | 4.5 ± 0.5 | 4.4 ± 0.4 | 4.7 ± 0.5 | 0.58 |
| Insulin | 5.5 (3.3, 6.8) | 5.2 (4.6, 10.3) | 5.5 (3.2, 6.4) | 5.4 (3.2, 6.8) | 0.61 | |
| HbA1c | 5.3 ± 0.2 | 5.3 ± 0.2 | 5.3 ± 0.2 | 5.5 ± 0.4 | 0.39 | |
| HOMA-IR | 1.0 (0.7, 1.4) | 1.0 (0.8, 2.2) | 1.2 (0.6, 1.4) | 1.1 (0.6, 1.4) | 0.69 | |
| Total cholesterol | 5.0 ± 1.0 | 5.2 ± 1.3 | 4.4 ± 0.6 | 5.2 ± 0.7 | 0.31 | |
| Triglycerides | 1.0 ± 0.6 | 1.2 ± 0.8 | 0.7 ± 0.2 | 1.0 ± 0.6 | 0.25 | |
| LDL-C | 3.0 ± 0.7 | 2.9 ± 0.7 | 2.6 ± 0.6 | 3.1 ± 0.7 | 0.36 | |
| HDL-C | 1.6 ± 0.5 | 1.7 ± 0.7 | 1.5 ± 0.3 | 1.6 ± 0.4 | 0.84 | |
| Total/HDL-C | 3.4 (2.5, 3.6) | 3.5 (2.7, 3.8) | 3.0 (2.9, 3.4) | 3.4 (2.5, 4.4) | 0.61 | |
| CRP | 6.2 ± 4.9 | 7.8 ± 6.4 | 5.6 ± 3.5 | 5.3 ± 4.1 | 0.56 | |
| Postpartum—6 months | Glucose | 4.5 ± 0.4 | 4.5 ± 0.5 | 4.5 ± 0.4 | 4.6 ± 0.4 | 0.91 |
| Insulin | 5.4 (3.2, 6.1) | 5.8 (4.5, 10.2) | 3.5 (2.7, 9.3) | 5.4 (2.9, 6.0) | 0.55 | |
| HbA1c | 5.3 ± 0.3 | 5.3 ± 0.4 | 5.3 ± 0.2 | 5.3 ± 0.3 | 0.88 | |
| HOMA-IR | 1.1 (0.6, 1.4) | 1.1 (0.87, 1.83) | 0.7 (0.5, 2.0) | 1.0 (0.6, 1.3) | 0.65 | |
| Total cholesterol | 4.8 ± 1.2 | 4.7 ± 1.6 | 4.8 ± 1.0 | 4.9 ± 1.0 | 0.95 | |
| Triglycerides | 0.9 (0.5, 1.2) | 1.0 (0.5, 1.4) | 0.8 (0.7, 1.1) | 0.9 (0.5, 1.4) | 0.70 | |
| LDL-C | 2.9 ± 1.0 | 2.7 ± 1.0 | 3.0 ± 1.2 | 3.0 ± 1.0 | 0.83 | |
| HDL-C | 1.3 (1.1, 1.8) | 1.2 (1.1, 1.9) | 1.3 (1.3, 1.3) | 1.5 (1.1, 1.7) | 0.94 | |
| Total/HDL-C | 3.4 (2.6, 4.3) | 3.4 (2.7, 4.3) | 3.7 (3.0, 4.3) | 3.1 (3.0, 4.4) | 0.92 | |
| CRP | 3.5 (3.0, 6.1) | 3.3 (2.0, 6.1) | 5.2 (2.5, 6.6) | 3.1 (3.0, 4.4) | 0.98 |
Trial Evaluation
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Statistics, A.B.O. Australian Health Survey: First Results, 2011–12. 2012. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4364.0.55.0012011-12?OpenDocument (accessed on 17th December 2014). [Google Scholar]
- Linne, Y.; Dye, L; Barkeling, B; Rossner, S. Long-Term Weight Development in Women: A 15-Year Follow-up of the Effects of Pregnancy. Obesity 2004, 12, 1166–1178. [Google Scholar] [CrossRef]
- Olson, C.M.; Strawderman, M.S.; Hinton, P.S.; Pearson, T.A. Gestational Weight Gain and Postpartum Behaviors Associated with Weight Change from Early Pregnancy to 1 y Postpartum. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Schauberger, C.W.; Rooney, B.L.; Brimer, L.M. Factors that influence weight loss in the puerperium. Obstet. Gynecol. 1992, 79, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Rothberg, B.E.G.; Magriples, U.; Kershaw, T.S.; Rising, S.S.; Ickovics, J.R. Gestational weight gain and subsequent postpartum weight loss among young, low-income, ethnic minority women. Am. J. Obstet. Gynecol. 2011, 204, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ohlin, A.; Rossner, S. Maternal body weight development after pregnancy. Int. J. Obes. 1990, 14, 159–173. [Google Scholar] [PubMed]
- Althuizen, E.; Van Poppel, M.N.M.; de Vries, J.H.; Seidell, J.C.; Mechelen, W.V. Postpartum behavior as predictor of weight change from before pregnancy to one year postpartum. BMC Public Health 2011, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, E.P. Childbearing and obesity in women: Weight before, during, and after pregnancy. Obstet. Gynecol. Clin. North Am. 2009, 36, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Sirimi, N.; Goulis, D.G. Obesity in pregnancy. Hormones 2010, 9, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, I.; Graves, N.; deJersey, S.; McIntyre, H.D.; Callaway, L.K. Obesity in pregnancy: Outcomes and economics. Semin. Fetal Neonatal Med. 2010, 15, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Solomon, C.G.; Willett, W.C.; Carey, V.J.; Rich-Edwards, J.; Hunter, D.J.; Colditz, G.A; Stampfer, M.J.; Spelzer, F.E.; Spiegelma, D.; Manson, J.E. A prospective study of pregravid determinants of gestational diabetes mellitus. J. Am. Med. Assoc. 1997, 278, 1078–1083. [Google Scholar] [CrossRef]
- Sebire, N.J.; Jolly, M.; Harris, J.P.; Wadsworth, J.; Joffe, M.; Beard, R.W.; Regan, L.; Robinson, S. Maternal obesity and pregnancy outcome a study of 287213 pregnancies in London. Int. J. Obes. 2001, 25, 1175–1182. [Google Scholar] [CrossRef]
- Dzakpasu, S.; Fahey, J.; Kirby, R.S.; Tough, S.; Chalmers, B.; Heaman, M.; Bartholomew, S.; Biringer, A.; Darling, E.K.; Lee, L.S.; McDonald, S.D. Contribution of prepregnancy body mass index and gestational weight gain to caesarean birth in Canada. BMC Pregnancy Childbirth 2014, 14, 106. [Google Scholar] [CrossRef] [PubMed]
- Donath, S.M.; Amir, L.H. Maternal obesity and initiation and duration of breastfeeding: data from the longitudinal study of Australian children. Matern. Child Nutr. 2008, 4, 163–170. [Google Scholar] [CrossRef]
- Donath, S.M.; Amir, L.H. Does maternal obesity adversely affect breastfeeding initiation and duration? J. Paediatr. Child Health 2000, 36, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.; Hure, A.J.; MacDonald-Wicks, L.; Patterson, A.J.; Smith, R.; Collins, C.E. Disparities exist between national food group recommendations and the dietary intakes of Australian women. BMC Women’s Health 2011, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.A.; Rifas-Shiman, S.L.; Kleinman, K.P.; Rich-Edwards, J.W.; Peterson, K.E.; Gillman, M.W. Predictors of Change in Physical Activity During and After Pregnancy: Project Viva. Am. J. Prev. Med. 2007, 32, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Craigie, A.M.; Barbour, R.S.; Anderson, A.S. How can we help women lose weight after child birth? Formative findings from the WeightWell weight managment study. Proc. Nutr. Soc. 2010, 69, 1. [Google Scholar] [CrossRef] [PubMed]
- Walker, L.O.; Grobe, S.J. The Construct of Thriving in Pregnancy and Postpartum. Nurs. Sci. Q. 1999, 12, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Lewallen, L.P. Healthy Behaviors and Sources of Health Information Among Low-Income Pregnant Women. Public Health Nurs. 2004, 21, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Wojcicki, J.M. Maternal Prepregnancy Body Mass Index and Initiation and Duration of Breastfeeding: A Review of the Literature. J. Women’s Health 2011, 20, 7. [Google Scholar] [CrossRef]
- Nommsen-Rivers, L.A.; Chantry, C.J.; Peerson, J.M.; Cohen, R.J.; Dewey, K.G. Delayed onset of lactogenesis among first-time mothers is related to maternal obesity and factors associated with ineffective breastfeeding. Am. J. Clin. Nutr. 2010, 92, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Nommsen-Rivers, L.A.; Heinig, M.J.; cohen, R.J. Risk factors for suboptimal infant breastfeeding behavior, delayed onset of lactation, and excess neonatal weight loss. Pediatrics 2003, 112, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Kjolhede, C.L. Prepregnant Overweight and Obesity Diminish the Prolactin Response to Suckling in the First Week Postpartum. Pediatrics 2004, 113, e465–e471. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.L.; Michaelsen, K.F.; Sorensen, T.I.A.; Rasmussen, K.M. High prepregnant body mass index is associated with early termination of full and any breastfeeding in Danish women. Am. J. Clin. Nutr. 2007, 86, 404. [Google Scholar] [PubMed]
- Dyson, L.; McCormick, F.; Renfrew, M. Interventions for promoting the intiation of breastfeeding. Cochrane Database Sytematic Rev. 2005, 2, CD001688. [Google Scholar]
- Lumbiganon, P.; Martis, R.; Malinee, L.; Festin, M.R.; Ho, J.J.; Hakimi, M. Antenatal breastfeeding education for increasing breastfeeding duration. C Collab. 2010, 12. [Google Scholar] [CrossRef]
- Masiero, J.V.; Tabroff, J.M.; Scannell, E. The Accuracy of Recalled versus Measured Pre-Pregnancy Weight for the Calculation of Pre-pregnancy Body Mass Index; University of Massachusetts Medical School: Worcester, MA, USA, 2014. [Google Scholar]
- Hure, A.J.; Collins, C.E.; Giles, W.B.; Wright, I.M.R.; Smith, R. Protocol for the Women and their Children’s Health (WATCH) study: A cohort of pregnancy and beyond. J. Epidemiol. 2012, 22, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- Calfas, K.J.; Marcus, B.H. Postpartum Weight Retention: A Mother’s Weight to Bear? Am. J. Prev. Med. 2007, 32, 356–357. [Google Scholar] [CrossRef] [PubMed]
- Carter-Edwards, L.; Ostbye, T.; Bastian, L.; Yarnall, K.; Krause, K.; Simmons, T-J.I. Barriers to adopting a healthy lifestyle: insight from postpartum women. BMC Res. Notes 2009, 2, 161. [Google Scholar] [CrossRef] [PubMed]
- Ostbye, T.; Krause, K.M.; Lovelady, C.A.; Morey, M.C.; Bastian, L.A.; Peterson, B.L.; Swamy, G.K.; Brouwer, R.J.; McBride, C.M. Active Mothers Postpartum: A Randomized Controlled Weight-Loss Intervention Trial. Am. J. Prev. Med. 2009, 37, 173–180. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, M.L.; Sawicki, M.A.; Artal, R. Structured diet and physical activity prevent postpartum weight retention. J. Womens Health (Larchmt.) 2003, 12, 991–998. [Google Scholar] [CrossRef]
- Leermarkers, E.A.; Anglin, K.; Wing, R.R. Reducing postpartum weight retention through a correspondance intervention. Int. J. Obes. 1998, 22, 1103–1109. [Google Scholar] [CrossRef]
- Baker, J.L.; Michaelsen, K.F.; Rasmussen, K.M.; Sorensen, T.I.A. Maternal prepregnant body mass index, duration of breastfeeding, and timing of complementary food introduction are associated with infant weight gain. Am. J. Clin. Nutr. 2004, 80, 1579–1588. [Google Scholar] [PubMed]
- Harder, T.; Bergman, R.; Kallinschnigg, G.; Plagemann, A. Duration of breastfeeding and risk of overweight: A meta-analysis. Am. J. Epidemiol. 2005, 162, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Krause, K.; Lovelady, C.; Østbye, T. Predictors of Breastfeeding in Overweight and Obese Women: Data From Active Mothers Postpartum (AMP). Matern. Child Health J. 2011, 15, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Jewell, S.; Grummer-Strawn, L. Maternal obesity and breastfeeding practices. Am. J. Clin. Nutr. 2003, 77, 931–936. [Google Scholar] [PubMed]
- Amir, L.; Donath, S. A systematic review of maternal obesity and breastfeeding intention, initiation and duration. BMC Pregnancy Childbirth 2007, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Amorim Adegboye, A.; Linne, Y.; Lourenco, P. Diet or exercise, or both, for weight reduction in women after childbirth (Review). Cochrane Collaboration 2008, 4, 1–40. [Google Scholar]
- Huang, T.; Yeh, C.; Tsai, Y. A diet and physical activity intervention for preventing weight retention among Taiwanese childbearing women: a randomised controlled trial. Midwifery 2011, 27, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, T.; Pasanen, M.; Aittasalo, M.; Fogelholm, M.; Weiderpass, E.; Luoto, R. Reducing postpartum weight retention—A pilot trial in primary health care. Nutr. J. 2007, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Craigie, A.M.; MacLeod, M.; Barton, K.L.; Treweek, S.; anderson, A.S. Supporting postpartum weight loss in women living in deprived communities: Design implications for a randomised control trial. Eur. J. Clin. Nutr. 2011, 65, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.E.; Hure, A.J.; MacDonald-Wicks, L.; Smith, R.; Collins, C.E. Predictors of post-partum weight retention in a prospective longitudinal study. Matern. Child Nutr. 2014, 10, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Gore, S.; Brown, D.; West, D. The role of postpartum weight retention in obesity among women: A review of the evidence. Ann. Behav. Med. 2003, 26, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Rexrode, K.M.; Carey, V.J.; Hennekens, C.H.; Walters, E.E.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Manson, J.E. Abdominal Adiposity and Coronary Heart Disease in Women. J. Am. Med. Assoc. 1998, 280, 1843–1848. [Google Scholar] [CrossRef]
- Cameron, A.; Welborn, T.; Zimmet, P.; Dunstan, D.; Owen, N.; Salmon, J. Overweight and obesity in Australia: the 1999–2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Med. J. Aust. 2003, 178, 427–432. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, J.; MacDonald-Wicks, L.; Hure, A.; Smith, R.; Collins, C.E. Reducing Postpartum Weight Retention and Improving Breastfeeding Outcomes in Overweight Women: A Pilot Randomised Controlled Trial. Nutrients 2015, 7, 1464-1479. https://doi.org/10.3390/nu7031464
Martin J, MacDonald-Wicks L, Hure A, Smith R, Collins CE. Reducing Postpartum Weight Retention and Improving Breastfeeding Outcomes in Overweight Women: A Pilot Randomised Controlled Trial. Nutrients. 2015; 7(3):1464-1479. https://doi.org/10.3390/nu7031464
Chicago/Turabian StyleMartin, Julia, Lesley MacDonald-Wicks, Alexis Hure, Roger Smith, and Clare E Collins. 2015. "Reducing Postpartum Weight Retention and Improving Breastfeeding Outcomes in Overweight Women: A Pilot Randomised Controlled Trial" Nutrients 7, no. 3: 1464-1479. https://doi.org/10.3390/nu7031464