Maternal Folic Acid Supplementation during Pregnancy and Childhood Allergic Disease Outcomes: A Question of Timing?

Abstract
:1. Introduction
2. Folate Requirements in Pregnancy
3. History of Folic Acid Supplementation
4. Time Trends in Folic Acid Supplementation Practices
5. Dietary Intake of Folate from Food Sources
6. Folic Acid Food Fortification
7. Dietary Intake and Folate Status Post Folic Acid Food Fortification
8. Timelines of Changing Folate Status and Increasing Prevalence of Allergic Diseases
9. Observational Studies Investigating the Relationship between Maternal Folic Acid Supplementation and/or Folate Status during Pregnancy and Childhood Allergic Disease
9.1. Periconceptional and First Trimester Folic Acid Supplementation
9.2. Folate Status and/or Folic Acid Supplementation at Some Time during Pregnancy
9.3. Second and Third Trimester Pregnancy Folic Acid Supplementation
10. Epigenetic Effect of Folate on Immune Gene Regulation
11. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
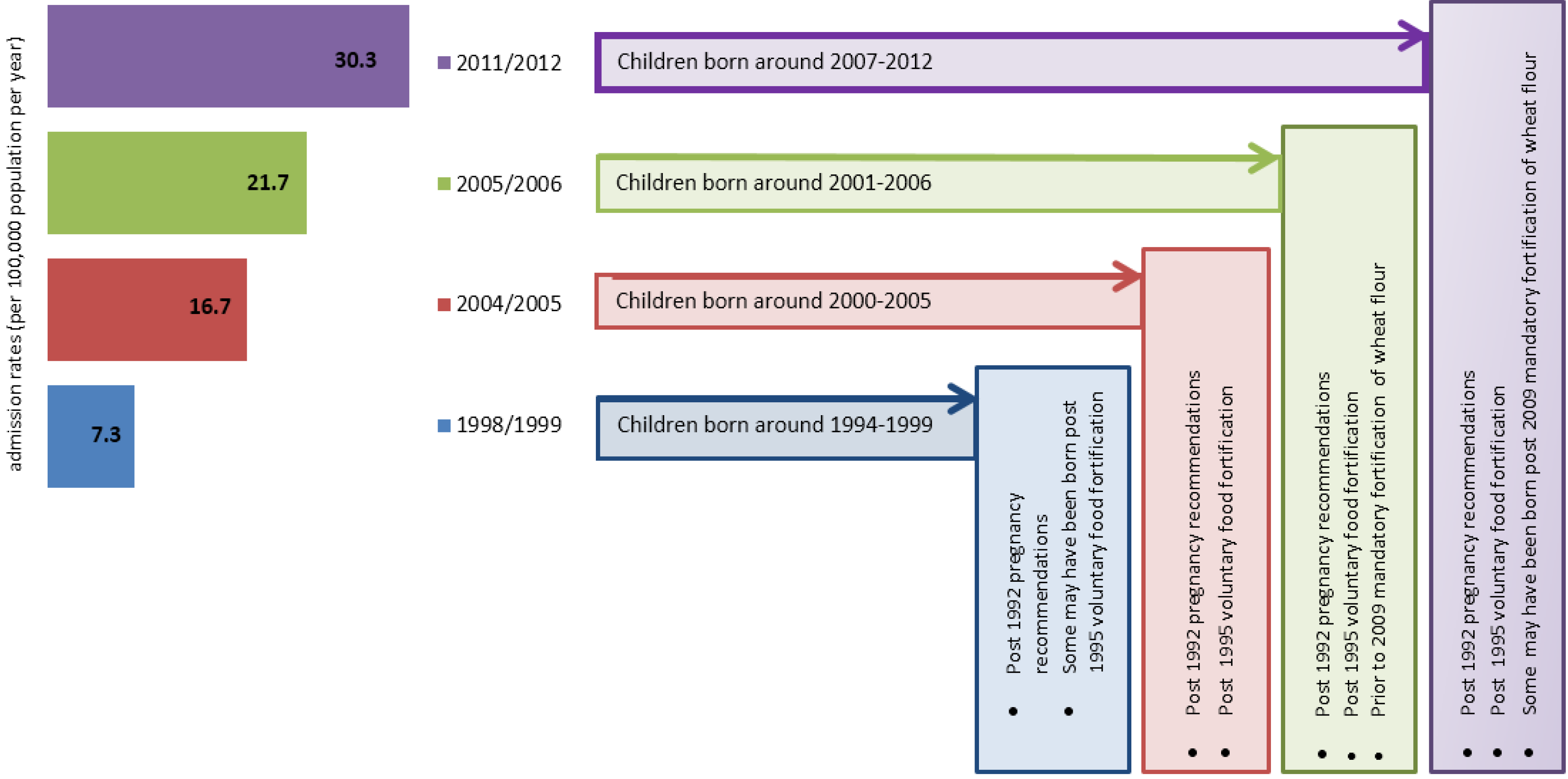
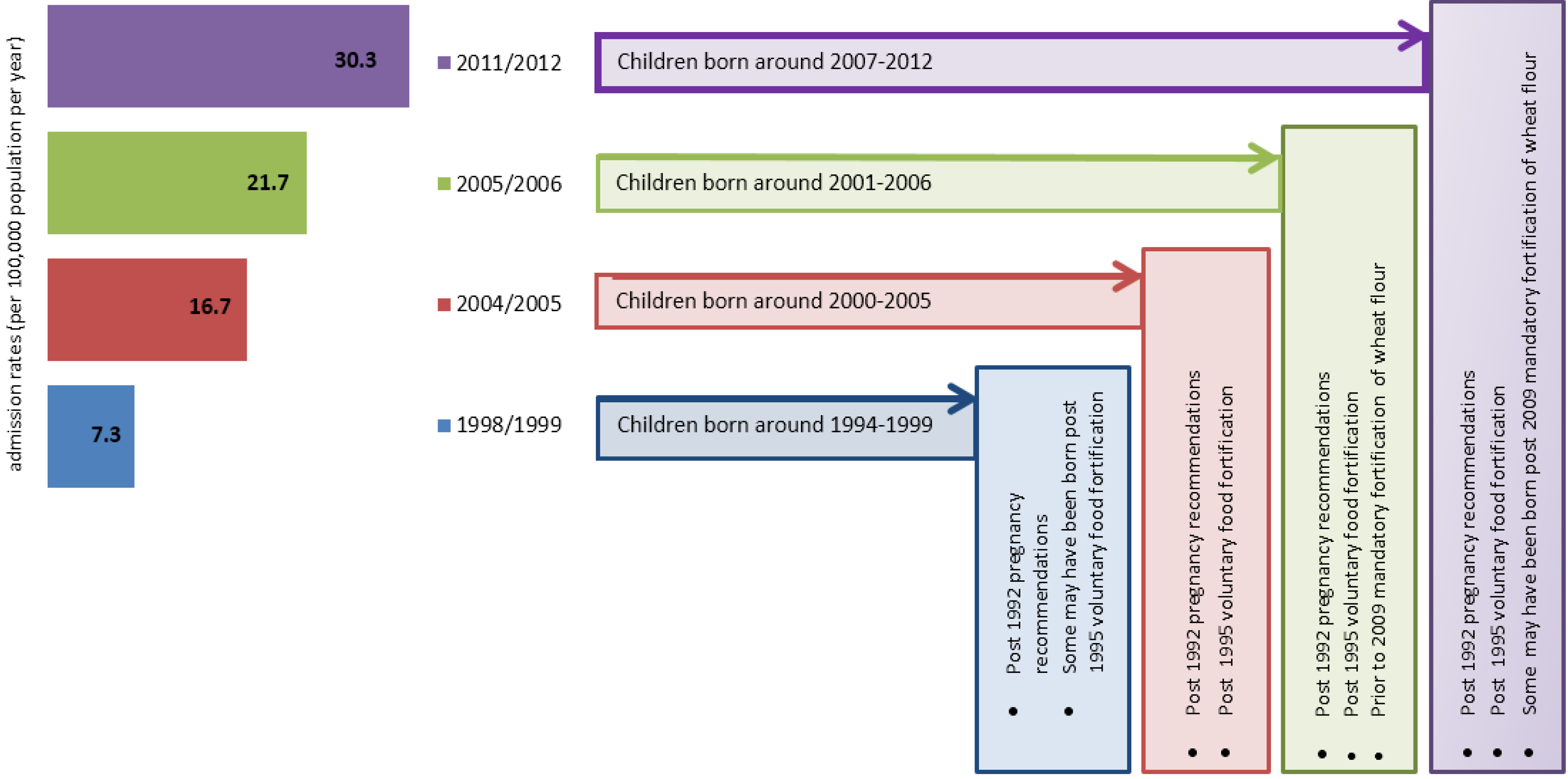
- Mullins, R.J.; Dear, K.B.; Tang, M.L. Time trends in Australian hospital anaphylaxis admissions in 1998–1999 to 2011–2012. J. Allergy Clin. Immunol. 2015, 136, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Lowe, A.J.; Matheson, M.C.; Ponsonby, A.L.; Wake, M.; Tang, M.L.; Dharmage, S.C.; et al. Prevalence of challenge-proven ige-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J. Allergy Clin. Immunol. 2011, 127, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Pawankar, R.; Canonica, G.W.; Holgate, S.T.; Lockey, R.F. Allergic diseases and asthma: A major global health concern. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Pawankar, R.; Allen, K.J.; Campbell, D.E.; Sinn, J.; Fiocchi, A.; Ebisawa, M.; Sampson, H.A.; Beyer, K.; Lee, B.W. A global survey of changing patterns of food allergy burden in children. World Allergy Organ. J. 2013, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Barua, S.; Junaid, M.A. Lifestyle, pregnancy and epigenetic effects. Epigenomics 2015, 7, 85–102. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.B.; Reeves, K.W.; Bertone-Johnson, E.R. Maternal folate exposure in pregnancy and childhood asthma and allergy: A systematic review. Nutr. Rev. 2014, 72, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.E.; Boyle, R.J.; Thornton, C.A.; Prescott, S.L. Mechanisms of allergic disease—Environmental and genetic determinants for the development of allergy. Clin. Exp. Allergy 2015, 45, 844–858. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J. In utero programming of chronic disease. Clin. Sci. 1998, 95, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J.; Huang, R.C.; Craig, J.M.; Prescott, S.L. Nutritional influences on epigenetic programming: Asthma, allergy, and obesity. Immunol. Allergy Clin. N. Am. 2014, 34, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Waterland, R.A.; Michels, K.B. Epigenetic epidemiology of the developmental origins hypothesis. Ann. Rev. Nutr. 2007, 27, 363–388. [Google Scholar] [CrossRef] [PubMed]
- Tsang, B.L.; Devine, O.J.; Cordero, A.M.; Marchetta, C.M.; Mulinare, J.; Mersereau, P.; Guo, J.; Qi, Y.P.; Berry, R.J.; Rosenthal, J.; et al. Assessing the association between the methylenetetrahydrofolate reductase (MTHFR) 677C>T polymorphism and blood folate concentrations: A systematic review and meta-analysis of trials and observational studies. Am. J. Clin. Nutr. 2015, 101, 1286–1294. [Google Scholar] [CrossRef] [PubMed]
- Miles, E.A.; Calder, P.C. Maternal diet and its influence on the development of allergic disease. Clin. Exp. Allergy 2015, 45, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L. Early-life environmental determinants of allergic diseases and the wider pandemic of inflammatory noncommunicable diseases. J. Allergy Clin. Immunol. 2013, 131, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Martino, D.; Prescott, S. Epigenetics and prenatal influences on asthma and allergic airways disease. Chest 2011, 139, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Amarasekera, M.; Prescott, S.L.; Palmer, D.J. Nutrition in early life, immune-programming and allergies: The role of epigenetics. Asian Pac. J. Allergy Immunol. 2013, 31, 175–182. [Google Scholar] [PubMed]
- Ashley, S.; Dang, T.; Koplin, J.; Martino, D.; Prescott, S. Food for thought: Progress in understanding the causes and mechanisms of food allergy. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Macaubas, C.; Holt, B.J.; Smallacombe, T.B.; Loh, R.; Sly, P.D.; Holt, P.G. Transplacental priming of the human immune system to environmental allergens: Universal skewing of initial T cell responses toward the Th2 cytokine profile. J. Immunol. 1998, 160, 4730–4737. [Google Scholar] [PubMed]
- Mold, J.E.; Michaelsson, J.; Burt, T.D.; Muench, M.O.; Beckerman, K.P.; Busch, M.P.; Lee, T.H.; Nixon, D.F.; McCune, J.M. Maternal alloantigens promote the development of tolerogenic fetal regulatory T cells in utero. Science 2008, 322, 1562–1565. [Google Scholar] [CrossRef] [PubMed]
- Schaub, B.; Liu, J.; Hoppler, S.; Schleich, I.; Huehn, J.; Olek, S.; Wieczorek, G.; Illi, S.; von Mutius, E. Maternal farm exposure modulates neonatal immune mechanisms through regulatory T cells. J. Allergy Clin. Immunol. 2009, 123, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Tulic, M.K.; Hodder, M.; Forsberg, A.; McCarthy, S.; Richman, T.; D’Vaz, N.; van den Biggelaar, A.H.; Thornton, C.A.; Prescott, S.L. Differences in innate immune function between allergic and nonallergic children: New insights into immune ontogeny. J. Allergy Clin. Immunol. 2011, 127, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Macaubas, C.; Smallacombe, T.; Holt, B.J.; Sly, P.D.; Holt, P.G. Development of allergen-specific T-cell memory in atopic and normal children. Lancet 1999, 353, 196–200. [Google Scholar] [CrossRef]
- Hollingsworth, J.W.; Maruoka, S.; Boon, K.; Garantziotis, S.; Li, Z.; Tomfohr, J.; Bailey, N.; Potts, E.N.; Whitehead, G.; Brass, D.M.; et al. In utero supplementation with methyl donors enhances allergic airway disease in mice. J. Clin. Investig. 2008, 118, 3462–3469. [Google Scholar] [CrossRef] [PubMed]
- Daly, L.E.; Kirke, P.N.; Molloy, A.; Weir, D.G.; Scott, J.M. Folate levels and neural tube defects. Implications for prevention. JAMA 1995, 274, 1698–1702. [Google Scholar] [CrossRef] [PubMed]
- Abbassi-Ghanavati, M.; Greer, L.G.; Cunningham, F.G. Pregnancy and laboratory studies: A reference table for clinicians. Obstet. Gynecol. 2009, 114, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Hursthouse, N.A.; Gray, A.R.; Miller, J.C.; Rose, M.C.; Houghton, L.A. Folate status of reproductive age women and neural tube defect risk: The effect of long-term folic acid supplementation at doses of 140 microg and 400 microg per day. Nutrients 2011, 3, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Wills, L. Treatment of “pernicious anaemia of pregnancy” and “tropical anaemia”. Br. Med. J. 1931, 1, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Al-Gailani, S. Making birth defects ‘preventable’: Pre-conceptional vitamin supplements and the politics of risk reduction. Stud. Hist. Philos. Biol. Biomed. Sci. 2014, 47 Pt B, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Chanarin, I.; Macgibbon, B.M.; O'Sullivan, W.J.; Mollin, D.L. Folic-acid deficiency in pregnancy. The pathogenesis of megaloblastic anaemia of pregnancy. Lancet 1959, 2, 634–639. [Google Scholar] [CrossRef]
- Giles, C. An account of 335 cases of megaloblastic anaemia of pregnancy and the puerperium. J. Clin. Pathol. 1966, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.A. The incidence of pernicious anaemia and the etiology of folic acid deficiency in pregnancy. Acta Obstet. Gynecol. Scand. 1967, 46 (Suppl. 7), 113–115. [Google Scholar] [CrossRef]
- Willoughby, M.L.; Jewell, F.J. Investigation of folic acid requirements in pregnancy. Br. Med. J. 1966, 2, 1568–1571. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, B.M.; Hibbard, E.D. Folate deficiency in pregnancy. Br. Med. J. 1968, 4, 452–453. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, B.M.; Hibbard, E.D.; Jeffcoate, T.N. Folic acid and reproduction. Acta Obstet. Gynecol. Scand. 1965, 44, 375–400. [Google Scholar] [CrossRef] [PubMed]
- Bower, C.; Stanley, F.J. Dietary folate as a risk factor for neural-tube defects: Evidence from a case-control study in Western Australia. MJA 1989, 150, 613–619. [Google Scholar] [PubMed]
- Czeizel, A.E.; Dudas, I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. NEJM 1992, 327, 1832–1835. [Google Scholar] [CrossRef] [PubMed]
- Milunsky, A.; Jick, H.; Jick, S.S.; Bruell, C.L.; MacLaughlin, D.S.; Rothman, K.J.; Willett, W. Multivitamin/folic acid supplementation in early pregnancy reduces the prevalence of neural tube defects. JAMA 1989, 262, 2847–2852. [Google Scholar] [CrossRef] [PubMed]
- Mulinare, J.; Cordero, J.F.; Erickson, J.D.; Berry, R.J. Periconceptional use of multivitamins and the occurrence of neural tube defects. JAMA 1988, 260, 3141–3145. [Google Scholar] [CrossRef] [PubMed]
- Smithells, R.W.; Sheppard, S.; Schorah, C.J.; Seller, M.J.; Nevin, N.C.; Harris, R.; Read, A.P.; Fielding, D.W. Possible prevention of neural-tube defects by periconceptional vitamin supplementation. Lancet 1980, 1, 339–340. [Google Scholar] [CrossRef]
- Smithells, R.W.; Sheppard, S.; Schorah, C.J.; Seller, M.J.; Nevin, N.C.; Harris, R.; Read, A.P.; Fielding, D.W. Apparent prevention of neural tube defects by periconceptional vitamin supplementation. Arch. Dis. Child. 1981, 56, 911–918. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Fernandez-Gaxiola, A.C.; Dowswell, T.; Pena-Rosas, J.P. Effects and safety of periconceptional folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2010, CD007950. [Google Scholar] [CrossRef]
- Bower, C.; Blum, L.; O’Daly, K.; Higgins, C.; Loutsky, F.; Kosky, C. Promotion of folate for the prevention of neural tube defects: Knowledge and use of periconceptional folic acid supplements in Western Australia, 1992 to 1995. Aust. N. Z. J. Public Health 1997, 21, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Bower, C.; Miller, M.; Payne, J.; Serna, P. Promotion of folate for the prevention of neural tube defects: Who benefits? Paediatr. Perinat. Epidemiol. 2005, 19, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Mallard, S.R.; Houghton, L.A. Folate knowledge and consumer behaviour among pregnant New Zealand women prior to the potential introduction of mandatory fortification. Asia Pac. J. Clin. Nutr. 2012, 21, 440–449. [Google Scholar] [PubMed]
- Stockley, L.; Lund, V. Use of folic acid supplements, particularly by low-income and young women: A series of systematic reviews to inform public health policy in the UK. Public Health Nutr. 2008, 11, 807–821. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.F.; Brown, S.J.; Davey, M.A. Use of periconceptional folic acid supplements in Victoria and New South Wales, Australia. Aust. N. Z. J. Public Health 2006, 30, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ge, X.; Zhu, B.; Xuan, Y.; Huang, K.; Rutayisire, E.; Mao, L.; Huang, S.; Yan, S.; Tao, F. Maternal continuing folic acid supplementation after the first trimester of pregnancy increased the risk of large-for-gestational-age birth: A population-based birth cohort study. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, M.L.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. A systematic review and meta-analysis of micronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2013, 71, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Crider, K.S.; Bailey, L.B.; Berry, R.J. Folic acid food fortification-its history, effect, concerns, and future directions. Nutrients 2011, 3, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.A.; Chai, W.; Kara, R.; Rosenberg, I.H.; Scott, J.; Tedstone, A. Examination of selected national policies towards mandatory folic acid fortification. Nutr. Rev. 2009, 67 (Suppl. 1), S73–S78. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L.; Signore, C. Neural tube defect rates before and after food fortification with folic acid. Birth Defects Res. A Clin. Mol. Teratol. 2004, 70, 844–845. [Google Scholar] [CrossRef] [PubMed]
- Mallard, S.R.; Gray, A.R.; Houghton, L.A. Periconceptional bread intakes indicate New Zealand’s proposed mandatory folic acid fortification program may be outdated: Results from a postpartum survey. BMC Pregnancy Childbirth 2012, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Bower, C.; Ryan, A.; Rudy, E.; Miller, M. Trends in neural tube defects in Western Australia. Aust. N. Z. J. Public Health 2002, 26, 150–151. [Google Scholar] [CrossRef] [PubMed]
- Hertrampf, E.; Cortes, F. National food-fortification program with folic acid in Chile. Food Nutr. Bull. 2008, 29, S231–S237. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, H.; Nyarko, K.A.; Goco, N.; Moore, J.; Moretti-Ferreira, D.; Murray, J.C.; Wehby, G.L. Folic acid fortification and women’s folate levels in selected communities in Brazil—A first look. Int. J. Vitam. Nutr. Res. 2014, 84, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Sayed, A.R.; Bourne, D.; Pattinson, R.; Nixon, J.; Henderson, B. Decline in the prevalence of neural tube defects following folic acid fortification and its cost-benefit in South Africa. Birth Defects Res. A Clin. Mol. Teratol. 2008, 82, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Dugbaza, J.; Cunningham, J. Estimates of total dietary folic acid intake in the Australian population following mandatory folic acid fortification of bread. J. Nutr. Metab. 2012, 2012, 492353. [Google Scholar] [CrossRef] [PubMed]
- Emmett, J.K.; Lawrence, M.; Riley, M. Estimating the impact of mandatory folic acid fortification on the folic acid intake of Australian women of childbearing age. Aust. N. Z. J. Public Health 2011, 35, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey. Nutrition First Results: Foods and Nutrients, 2011–12. Mean Daily Energy and Nutrient Intake. Available online: http://www.abs.gov.au/ausstats/[email protected]/detailspage/4364.0.55.0072011-12 (accessed on 1 November 2016).
- Frigolet, M.E.; Ramos Barragan, V.E.; Tamez Gonzalez, M. Low-carbohydrate diets: A matter of love or hate. Ann. Nutr. Metab. 2011, 58, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Plumptre, L.; Masih, S.P.; Ly, A.; Aufreiter, S.; Sohn, K.J.; Croxford, R.; Lausman, A.Y.; Berger, H.; O’Connor, D.L.; Kim, Y.I. High concentrations of folate and unmetabolized folic acid in a cohort of pregnant canadian women and umbilical cord blood. Am. J. Clin. Nutr. 2015, 102, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; Montefort, S.; Bjorksten, B.; Lai, C.K.; Strachan, D.P.; Weiland, S.K.; Williams, H.; Group, I.P.T.S. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: Isaac phases one and three repeat multicountry cross-sectional surveys. Lancet 2006, 368, 733–743. [Google Scholar] [CrossRef]
- Bekkers, M.B.; Elstgeest, L.E.; Scholtens, S.; Haveman-Nies, A.; de Jongste, J.C.; Kerkhof, M.; Koppelman, G.H.; Gehring, U.; Smit, H.A.; Wijga, A.H. Maternal use of folic acid supplements during pregnancy, and childhood respiratory health and atopy. Eur. Respir. J. 2012, 39, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, J.A.; West, C.; McCarthy, S.; Metcalfe, J.; Meldrum, S.; Oddy, W.H.; Tulic, M.K.; D’Vaz, N.; Prescott, S.L. The relationship between maternal folate status in pregnancy, cord blood folate levels, and allergic outcomes in early childhood. Allergy 2012, 67, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Granell, R.; Heron, J.; Lewis, S.; Davey Smith, G.; Sterne, J.A.; Henderson, J. The association between mother and child MTHFR C677T polymorphisms, dietary folate intake and childhood atopy in a population-based, longitudinal birth cohort. Clin. Exp. Allergy 2008, 38, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Haberg, S.E.; London, S.J.; Nafstad, P.; Nilsen, R.M.; Ueland, P.M.; Vollset, S.E.; Nystad, W. Maternal folate levels in pregnancy and asthma in children at age 3 years. J. Allergy Clin. Immunol. 2011, 127, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Haberg, S.E.; London, S.J.; Stigum, H.; Nafstad, P.; Nystad, W. Folic acid supplements in pregnancy and early childhood respiratory health. Arch. Dis. Child. 2009, 94, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Kiefte-de Jong, J.C.; Timmermans, S.; Jaddoe, V.W.; Hofman, A.; Tiemeier, H.; Steegers, E.A.; de Jongste, J.C.; Moll, H.A. High circulating folate and vitamin b-12 concentrations in women during pregnancy are associated with increased prevalence of atopic dermatitis in their offspring. J. Nutr. 2012, 142, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Jeong, K.S.; Ha, E.H.; Park, H.; Ha, M.; Hong, Y.C.; Bhang, S.Y.; Lee, S.J.; Lee, K.Y.; Lee, S.H.; et al. Relationship between prenatal and postnatal exposures to folate and risks of allergic and respiratory diseases in early childhood. Pediatr. Pulmonol. 2015, 50, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Magdelijns, F.J.; Mommers, M.; Penders, J.; Smits, L.; Thijs, C. Folic acid use in pregnancy and the development of atopy, asthma, and lung function in childhood. Pediatrics 2011, 128, e135–e144. [Google Scholar] [CrossRef] [PubMed]
- Tuokkola, J.; Luukkainen, P.; Kaila, M.; Takkinen, H.M.; Niinisto, S.; Veijola, R.; Virta, L.J.; Knip, M.; Simell, O.; Ilonen, J.; et al. Maternal dietary folate, folic acid and vitamin d intakes during pregnancy and lactation and the risk of cows’ milk allergy in the offspring. Br. J. Nutr. 2016, 116, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Whitrow, M.J.; Moore, V.M.; Rumbold, A.R.; Davies, M.J. Effect of supplemental folic acid in pregnancy on childhood asthma: A prospective birth cohort study. Am. J. Epidemiol. 2009, 170, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Duthie, S.J.; Horgan, G.; de Roos, B.; Rucklidge, G.; Reid, M.; Duncan, G.; Pirie, L.; Basten, G.P.; Powers, H.J. Blood folate status and expression of proteins involved in immune function, inflammation, and coagulation: Biochemical and proteomic changes in the plasma of humans in response to long-term synthetic folic acid supplementation. J. Proteome Res. 2010, 9, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Steegers-Theunissen, R.P.; Obermann-Borst, S.A.; Kremer, D.; Lindemans, J.; Siebel, C.; Steegers, E.A.; Slagboom, P.E.; Heijmans, B.T. Periconceptional maternal folic acid use of 400 microg per day is related to increased methylation of the IGF2 gene in the very young child. PLoS ONE 2009, 4, e7845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martino, D.; Dang, T.; Sexton-Oates, A.; Prescott, S.; Tang, M.L.; Dharmage, S.; Gurrin, L.; Koplin, J.; Ponsonby, A.L.; Allen, K.J.; et al. Blood DNA methylation biomarkers predict clinical reactivity in food-sensitized infants. J. Allergy Clin. Immunol. 2015, 135, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Martino, D.; Joo, J.E.; Sexton-Oates, A.; Dang, T.; Allen, K.; Saffery, R.; Prescott, S. Epigenome-wide association study reveals longitudinally stable DNA methylation differences in CD4+ T cells from children with IgE-mediated food allergy. Epigenetics 2014, 9, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Ladd-Acosta, C.; Hao, K.; Sherwood, B.; Ji, H.; Keet, C.A.; Kumar, R.; Caruso, D.; Liu, X.; Wang, G.; et al. Epigenome-wide association study links site-specific DNA methylation changes with cow’s milk allergy. J. Allergy Clin. Immunol. 2016, 138, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Petrus, N.C.; Henneman, P.; Venema, A.; Mul, A.; van Sinderen, F.; Haagmans, M.; Mook, O.; Hennekam, R.C.; Sprikkelman, A.B.; Mannens, M. Cow’s milk allergy in Dutch children: An epigenetic pilot survey. Clin. Transl. Allergy 2016, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Berni Canani, R.; Paparo, L.; Nocerino, R.; Cosenza, L.; Pezzella, V.; Di Costanzo, M.; Capasso, M.; Del Monaco, V.; D’Argenio, V.; Greco, L.; et al. Differences in DNA methylation profile of Th1 and Th2 cytokine genes are associated with tolerance acquisition in children with IgE-mediated cow’s milk allergy. Clin. Epigenet. 2015, 7, 38. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Reference | Study Design | Study Characterisitics | Key Allergic Disease Outcomes | Main Findings |
|---|---|---|---|---|
| Granell et al. 2008 [64] United Kingdom | Prospective cohort, pregnant women due date 1991–1992 with live births (n = 14,062); children aged 7–8 years (n = 5364). | Reported early and late pregnancy folic acid supplementation use; dietary folate intake at 32 weeks gestation, maternal and offspring methylenetetrahydrofolate reductase (MTHFR) C677T allele. | Skin prick test where positive SPT ≥ 2 mm weal; maternal reported child wheeze, and/or asthma diagnosed by physician. | No association between MTHFR C677T variant and atopy in children and maternal folic acid supplementation at 18 weeks and 32 weeks, or maternal folate intake at 32 weeks gestation. |
| Håberg et al. 2009 [66] Norway | Prospective cohort, pregnant women with children aged 18 months (n = 32,077) born 2000–2005. | Pregnant women reported maternal folic acid supplementation use in 1st trimester and after 1st trimester. | Maternal reported episodes of wheeze in children aged 18 months. | No association with folic acid supplement use after 12 weeks gestation and allergic disease outcomes. |
| Whitrow et al. 2009 [71] Australia | Prospective cohort, pregnant women (n = 557); mothers and their children aged 3.5 years (n = 490), 5.5 years (n = 423) recruited 1998–2000. | Pregnant women recruited in first 16 weeks of gestation. Reported food folate intake, inventory of supplement use at <16 weeks (early gestation) and at 30–34 weeks (late gestation). | Parental report of physician-diagnosed asthma of their child aged 3.5 and 5.5 years. | Late pregnancy folic acid supplementation use (weeks 30–34) was positively associated with risk of physician-diagnosed asthma at 3.5 years. |
| Håberg et al. 2011 [65] Norway | Case control, children aged 3 years (n = 1455 controls; 507 cases) born 2002–2004 | Pregnant women reported maternal folic acid supplementation use after week 13 gestation; plasma folate at median gestation 18 weeks. | Maternal reported asthma diagnosis in children. | Asthma risk at 3 years increased in offspring with increasing quintile of maternal folate intake. Supplementation use associated with 2nd trimester folate status (Spearman correlation = 0.46). |
| Dunstan et al. 2012 [63] Australia | Prospective cohort, pregnant women (n = 628) with a history of allergic disease (n = 592); skin prick test positive (n = 615), children aged 12 months (n = 484), born 2002–2009 | Maternal: food folate intake, folic acid supplement use in 3rd trimester. Calcuated dietary folate equivalants, serum folate; Cord blood: serum folate. | Medically diagnosed allergic diseases in infants aged 12 months of eczema and IgE mediated food allergy (symptoms on contact and sensitization by skin prick test). | Doses of folic acid > 500 µg/day from supplements in 3rd trimester associated with diagnosed eczema at 12 months. Reduced risk of sensitization for fetal serum levels between 50–75 nmol/L |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McStay, C.L.; Prescott, S.L.; Bower, C.; Palmer, D.J. Maternal Folic Acid Supplementation during Pregnancy and Childhood Allergic Disease Outcomes: A Question of Timing? Nutrients 2017, 9, 123. https://doi.org/10.3390/nu9020123
McStay CL, Prescott SL, Bower C, Palmer DJ. Maternal Folic Acid Supplementation during Pregnancy and Childhood Allergic Disease Outcomes: A Question of Timing? Nutrients. 2017; 9(2):123. https://doi.org/10.3390/nu9020123
Chicago/Turabian StyleMcStay, Catrina L., Susan L. Prescott, Carol Bower, and Debra J. Palmer. 2017. "Maternal Folic Acid Supplementation during Pregnancy and Childhood Allergic Disease Outcomes: A Question of Timing?" Nutrients 9, no. 2: 123. https://doi.org/10.3390/nu9020123