The Effect of a Mediterranean Diet on the Incidence of Cataract Surgery

 , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. PREDIMED Trial
2.2. Participants
2.3. Randomization and Intervention
2.4. Follow-Up and Adherence
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Funding
Author Contributions
Conflicts of Interest
Abbreviations
| MedDiet | Mediterranean Diet |
| EVOO | Extra-virgin Olive Oil |
| CVD | Cardiovascular Disease |
| MUFA | Mono-unsaturated fatty acids |
| PUFA | Poly-unsaturated fatty acids |
| TAC | Total anti-oxidant capacity |
References
- Klein, R.; Klein, B.E.K. The prevalence of age-related eye disease and visual impairment in aging: Current estimates. Investig. Ophthalmol. Vis. Sci. 2013, 54, ORSF5–ORSF13. [Google Scholar] [CrossRef] [PubMed]
- Congdon, N.; O’Colmain, B.; Klaver, C.C.; Klein, R.; Muñoz, B.; Friedman, D.S.; Kempen, J.; Taylor, H.R.; Mitchell, P.; Eye Diseases Prevalence Research group. Causes and prevalence of visual impairment among adults in the United States. Arch. Ophthalmol. 2004, 122, 477–485. [Google Scholar] [PubMed]
- Malot, J.; Combe, C.; Svary, P.; Moss, A.; Ligeon-Ligeonnet, P.; Hida, H. Direct cost of cataract surgery in public hospital. Ann. Pharm. Fr. 2010, 68, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Tinaztepe, O.E.; Ay, M.; Eser, E. Nuclear and mithocondrial DNA of age-related cataract patients are susceptible to oxidative damage. Curr. Eye Res. 2017, 42, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Vinson, J.A. Oxidative stress in cataracts. Pathophysiology 2006, 13, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Lou, M.F. Redox regulation in the lens. Prog. Retin. Eye Res. 2003, 22, 657–682. [Google Scholar] [CrossRef]
- Ye, J.; He, J.; Wang, C.; Wu, H.; Shi, X.; Zhang, H.; Xie, J.; Lee, S.Y. Smoking and risk of age-related cataract: A meta-analysis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3885–3895. [Google Scholar] [CrossRef] [PubMed]
- Rautiainen, S.; Lindblad, B.E.; Morgenstern, R.; Wolk, A. Total antioxidant capacity of the diet and risk of age related cataract: A population-based prospective cohort of women. JAMA Ophthalmol. 2014, 132, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Theodoropoulou, S.; Samoli, E.; Theodossiadis, P.G.; Papathanassiou, M.; Lagiou, A.; Lagiou, P.; Tzonou, A. Diet and cataract: A case control study. Int. Ophthalmol. 2014, 34, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Thiagarajan, R.; Manikandan, R. Antioxidant and cataract. Free Radic. Res. 2013, 47, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Zheng Selin, J.; Rautiainen, S.; Lindblad, B.E.; Morgenstern, R.; Wolk, A. High-dose supplements of vitamins C and E, low-dose multivitamins, and the risk of age-related cataract: A popoulation based prospective cohort study of men. Am. J. Epidemiol. 2013, 177, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Moise, M.M.; Benjamin, L.M.; Doris, T.M.; Dalida, K.N.; Augustin, N.O. Role of mediterranean diet, tropical vegetables rich in antioxidants, and sunlight exposure in blindness, cataract and glaucoma among African type 2 diabetics. Int. J. Ophthalmol. 2012, 5, 231–237. [Google Scholar] [PubMed]
- Weikel, K.A.; Garber, C.; Baburins, A.; Taylor, A. Nutritional modulation of cataract. Nutr. Rev. 2014, 72, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, R.D.; Vashist, P.; Gupta, S.K.; Young, I.S.; Maraini, G.; Camparini, M.; Jayanthi, R.; John, N.; Fitzpatrick, K.E.; Chakravarthy, V.; et al. Inverse association of vitamin C with cataract in older people in India. Ophthalmology 2011, 118, 1958–1965. [Google Scholar] [CrossRef] [PubMed]
- Costagliola, C.; Lobefalo, L.; Gallenga, P.E. Role of higher dietary carbohydrate intake in cataract devolpment. Investig. Ophthalmol. Vis. Sci. 2011, 52, 3593. [Google Scholar] [CrossRef] [PubMed]
- Lubick, N. A balance diet? Selenium may offset the effects of methylmercury on cataract devolpment. Environ. Health Perspect. 2010, 118, A491. [Google Scholar] [CrossRef] [PubMed]
- Kanthan, G.L.; Mitchell, P.; Burlustski, G.; Wang, J.J. Fasting blood glucose levels and the long–term incidence and progression of cataract–The blue montains eye study. Acta Ophthalmol. 2011, 89, e434–e438. [Google Scholar] [CrossRef] [PubMed]
- Appleby, P.N.; Allen, N.E.; Key, T.J. Diet, vegetarianism, and cataract risk. Am. J. Clin. Nutr. 2011, 93, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Liang, G.; Cai, C.; Lv, J. Association of Vitamin C with the risk of age-related cataract: A meta-analysis. Acta Ophthalmol. 2016, 94, e170–e176. [Google Scholar]
- Delcourt, C.; Korobelnik, J.F.; Barbeger-Gateau, P.; Delyfer, M.N.; Rougier, M.B.; Le Goff, M.; Malet, F.; Colin, J.; Dartigues, J.F. Nutrition and age-related eye disease: The alienor (antioxidants, lipides essentiels, nutrition et maladies oculaires) study. J. Nutr. Health Aging 2010, 14, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Ghanavati, M.; Behrooz, M.; Rashidkhani, B.; Ashtray-Larky, D.; Zameni, S.D.; Alipour, M. Healthy eating index in patients with cataract: A case-control study. Iran. Red Crescent Med. J. 2015, 17, e22490. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Wu, J.; Cho, E.; Ogata, S.; Jacques, P.; Taylor, A.; Chiu, C.J.; Wiggs, J.L.; Seddon, J.M.; Hankinson, S.E.; et al. Contribution of the nurses health study to the epidemiology of cataract, age-related macular degeneration and glaucoma. Am. J. Public Health 2016, 106, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Mares, J.A.; Voland, R.; Adler, R.; Tinker, L.; Miller, A.E.; Moeller, S.M.; Blodi, B.; Gehrs, K.M.; Wallace, R.B.; Chappel, R.J.; et al. Healthy diets and the subsequent prevalence of nuclear and the subsequent prevalence of nuclear cataract in women. Arch. Ophthalmol. 2010, 128, 738–749. [Google Scholar] [CrossRef] [PubMed]
- Tarwadi, K.V.; Agte, V.V. Interrelationship between nutritional status, socioeconomic factors, and lifestyle in Indian cataract patients. Nutrition 2011, 27, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Valero, M. Fruit and vegetable intake and vitamins C and E are associated with a reduced prevalence of cataract in a Spanish Mediterranean population. BMC Ophthalmol. 2013, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Mathew, M.C.; Ervin, A.M.; Tao, J.; Davis, R.M. Antioxidant vitamin supplementation for preventing and slowing the progression of age-related cataract. Cochrane Database Syst. Rev. 2012, 6, CD004567. [Google Scholar]
- Ma, L.; Hao, Z.X.; Liu, R.R.; Yu, R.B.; Shi, Q.; Pan, J.P. A dose-response meta-analysis of dietary lutein and zeaxanthin intake in relation to risk of age-related cataract. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.H.; Jing, C.X.; Pan, H.W. Association of blood anti-oxidants and vitamins with risk of age-related cataract: A meta-analysis of observational studies. Am. J. Clin. Nutr. 2013, 98, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.Y.; SanGiovanni, J.P.; Ferris, F.L.; Wong, W.T.; Agron, E.; Clemons, T.E.; Sperduto, R.; Danis, R.; Chandra, S.R.; Blodi, B.A.; et al. Lutein/zeaxanthin for the treatment of age-related cataract: AREDS2 randomized trial report no. 4. Age-related eye disease study 2 (AREDS2) research group. JAMA Ophthalmol. 2013, 131, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Karppi, J.; Laukkanen, J.A.; Kurl, S. Plasma lutein and zeaxanthin and the risk of age-related nuclear cataract among the elderly Finnish population. J. Nutr. 2012, 108, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Townend, B.S.; Townend, M.E.; Flood, V.; Burlutsky, G.; Rochtchina, E.; Wang, J.J.; Mitchell, P. Dietary macronutrient intake and five year incident cataract: The blue montain eye study. Am. J. Ophthalmol. 2007, 143, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Lapiscina, E.H.; Martínez-González, M.A.; Guillén Grima, F.; Olmo Jiménez, N.; Zarranz-Ventura, J.; Moreno-Montañés, J. Dietary fat intake and incidence of cataracts: The SUN prospective study in the cohort of Navarra, Spain. Med. Clin. (Barc.) 2010, 134, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Hartley, L.; Flowers, N.; Clarke, A.; Hooper, L.; Thorogood, M.; Stranges, S. Mediterranean dietary pattern for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013, 8, CD009825. [Google Scholar]
- Ros, E.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Fitó, M.; Martínez, J.A.; Corella, D. Mediterranean diet and cardiovascular health: Teachings of the PREDIMED study. Adv. Nutr. 2014, 5, 330S–336S. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ros, E.; Covas, M.I.; Fiol, M.; Warnberg, J.; Aros, F.; Ruiz-Gutierrez, V.; Lamuela-Raventos, R.M.; et al. Investigators for the PS. cohort profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Age-Related Eye Disease Study Research Group. A Randomized, Placebo-controlled, clinical trial of high-dose supplementation with vitamincs C and E and beta carotene for age-related cataract and vision loss: AREDS report No. 9. Arch. Ophthalmol. 2001, 119, 1439–1452. [Google Scholar]
- Chiu, C.J.; Taylor, A. Nutritional antioxidants and age-related cataract and maculopathy. Exp. Eye Res. 2007, 84, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Christen, W.G.; Glynn, R.J.; Gaziano, J.M.; Darke, A.K.; Crowley, J.J.; Goodman, P.J.; Lippman, S.M.; Lad, T.E.; Bearden, J.D.; Goodman, G.E.; et al. Age-related cataract in men in the selenium and vitamin E cáncer prevention trial eye endpoints study: A randomized trial. JAMA Ophthalmol. 2015, 133, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Lo, M.; Cho, E.; Taylor, A.; Hankinson, S.E.; Willet, W.C.; Jacques, P.F. Prospective study of dietary fat and risk of cataract extraction among US women. Am. J. Epidemiol. 2005, 161, 948–959. [Google Scholar]
- Javadi, M.; Zarei-Ghanavati, S. Cataracts in diabetic patients: A review article. J. Ophthalmic Vis. Res. 2008, 3, 52–65. [Google Scholar] [PubMed]
- Koo, E.; Chang, J.R.; Agrón, E.; Clemons, T.E.; Sperduto, R.D.; Ferris, F.L., 3rd; Chew, E.Y.; Age-related eye disease study group. Ten-year incidence rates of age-related cataract in Age-related eye disease study (AREDS): AREDS report No. 33. Ophthalmic Epidemiol. 2013, 20, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Klein, B.E.; Klein, R.; Lee, K.E.; Gangnon, R.E. Incidence of age-related cataract over 15 year interval the Beaver Dam Eye Study. Ophthalmology 2008, 115, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Taylor, A.; Chylack, L.T., Jr.; Rogers, G.; Hankinson, S.E.; Willett, W.C.; Jacques, P.F. Dietary fat intake and early age-related lens opacities. Am. J. Clin. Nutr. 2005, 81, 773–779. [Google Scholar] [PubMed]
- Greenland, S.; Lash, T.L. Bias analysis. In Modern Epidemiology, 3rd ed.; Rothman, K.J., Greenland, S., Lash, T.L., Eds.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2008; p. 359. [Google Scholar]

{kind=link}
| Characteristic | Mediterranean Diet with EVOO | Mediterranean Diet with Nuts | Control Diet |
|---|---|---|---|
| N = 1998 | N = 1914 | N = 1890 | |
| Age—year (mean ± SD) | 66.1 ± 6.1 | 65.8 ± 5.9 | 66.3 ± 6.2 |
| Sex (female)—No. (%) | 1120 (56.1) | 985 (51.5) | 1099 (58.2) |
| Smoking—No. (%) | |||
| Never smoker | 1189 (59.5) | 1117 (58.4) | 1147 (60.7) |
| Former smoker | 510 (25.5) | 497 (26.0) | 449 (23.8) |
| Current smoker | 299 (15.0) | 300 (15.7) | 294 (15.6) |
| Body mass index † (mean ± SD) | 30.0 ± 3.7 | 30.0 ± 3.8 | 30.3 ± 4.1 |
| Waist to height ratio (mean ± SD) | 0.63 ± 0.06 | 0.62 ± 0.06 | 0.63 ± 0.07 |
| Waist circumference (mean ± SD) | 100 ± 10 | 100 ± 11 | 101 ± 11 |
| Hypertension ‡—No. (%) | 1634 (81.8) | 1591 (83.1) | 1577 (83.4) |
| Type-2 diabetes §—No. (%) | 970 (48.6) | 851 (44.5) | 897 (47.5) |
| Dyslipidemia ¶—No. (%) | 1440 (72.1) | 1414 (73.9) | 1369 (72.4) |
| Family history of premature CHD—No. (%) | | 447 (22.4) | 426 (22.3) | 442 (23.4) |
| Physical activity—METS-min/day (mean ± SD) | 232 ± 229 | 248 ± 249 | 213 ± 236 |
| Variable | Mediterranean Diet with EVOO | Mediterranean Diet with Nuts | Control Diet |
|---|---|---|---|
| N = 1998 | N = 1914 | N = 1890 | |
| Total energy intake (kcal/day) (mean ± SD) | 2288 ± 612 | 2329 ± 620 | 2222 ± 602 |
| Carbohydrate (g/day) (mean ± SD) | 238.8 ± 81.7 | 242.6 ± 83.4 | 234.3 ± 79.2 |
| Fiber (g/day) (mean ± SD) | 25.4 ± 9.1 | 25.9 ± 9.2 | 24.7 ± 8.6 |
| Protein (g/day) (mean ± SD) | 93.3 ± 24.3 | 94.4 ± 23.2 | 90.4 ± 22.3 |
| Fat (g/day) (mean ± SD) | 99.5 ± 30.5 | 101.3 ± 30.2 | 96.3 ± 31.0 |
| Saturated fatty acids | 25.4 ± 9.1 | 25.8 ± 9.1 | 24.8 ± 9.3 |
| Monounsaturated fatty acids | 49.6 ± 16.0 | 50.0 ± 15.6 | 47.7 ± 16.5 |
| ω-6 Polyunsaturated fatty acids | 13.0 ± 6.4 | 13.7 ± 6.6 | 12.8 ± 6.2 |
| ω-3 Marine PUFA | 1.39 ± 0.75 | 1.51 ± 0.79 | 1.32 ± 0.65 |
| Cholesterol (mg/day) (mean ± SD) | 369.1 ± 137.5 | 374.3 ± 130.4 | 362.1 ± 128.5 |
| Cereals (g/day) (mean ± SD) | 231.4 ± 114.1 | 234.6 ± 108.6 | 225.6 ± 106.0 |
| Vegetables (g/day) (mean ± SD) | 344.5 ± 159.6 | 339.4 ± 152.1 | 324.8 ± 143.9 |
| Fruits (g/day) (mean ± SD) | 369.4 ± 212.5 | 370.2 ± 203.1 | 357.1 ± 200.6 |
| Total nuts (g/day) (mean ± SD) | 9.6 ± 13.9 | 12.5 ± 15.2 | 8.9 ± 12.6 |
| Dairy Products (g/day) (mean ± SD) | 378.8 ± 214.0 | 374.0 ± 220.6 | 376.0 ± 226.0 |
| Red Meat (g/day) (mean ± SD) | 134.7 ± 63.2 | 137.4 ± 59.8 | 130.0 ± 55.8 |
| Seafood (g/day) (mean ± SD) | 103.5 ± 54.7 | 102.4 ± 53.4 | 98.4 ± 48.2 |
| Olive Oil (g/day) (mean ± SD) | 40.5 ± 17.9 | 39.8 ± 17.4 | 38.4 ± 18.6 |
| Alcohol consumption (g/day) (mean | 9.1 ± 14.9 | 9.8 ± 15.5 | 7.9 ± 13.5 |
| MedDiet Adherence score ‖ (mean ± SD) | 8.7 ± 2.0 | 8.8 ± 2.0 | 8.4 ± 2.1 |
| Control Diet | Mediterranean Diet with EVOO | Mediterranean Diet with Nuts | |
|---|---|---|---|
| (n = 1890) | (n = 1998) | (n = 1914) | |
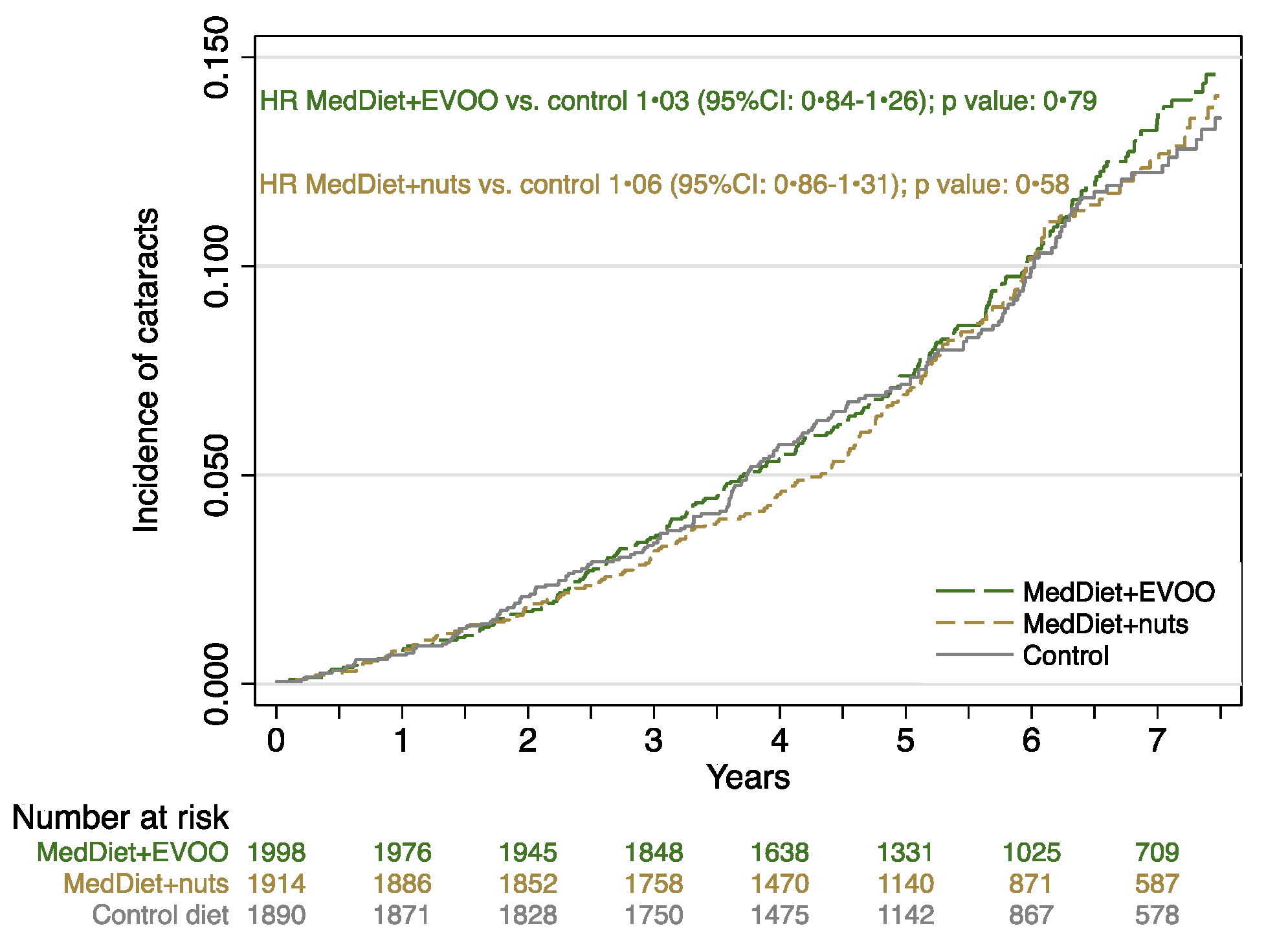
| Cases/Person-years | 179/10,633 | 206/11,728 | 174/10,719 |
| Rate (/1000 person-years) | 16.9 | 17.6 | 16.2 |
| Crude rate ratio | 1 (ref) | 1.02 (0.84 to 1.25) | 0.97 (0.78 to 1.19) |
| Multivariable adjusted rate ratio * | 1 (ref) | 1.03 (0.84 to 1.26) | 1.06 (0.86 to 1.31) |
| Control Diet | Mediterranean Diet with EVOO | Mediterranean Diet with Nuts | |
|---|---|---|---|
| (n = 1890) | (n = 1998) | (n = 1914) | |
| Age | |||
| Participants aged < 60 years | |||
| Cases/Person-years | 5/1375 | 14/1420 | 6/1559 |
| Multivariable adjusted rate ratio * | 1 (ref.) | 2.53 (0.88–7.24) | 1.21 (0.35–4.20) |
| 60 ≤ Participants aged < 70 years | |||
| Cases/Person-years | 85/6055 | 103/6806 | 94/6430 |
| Multivariable adjusted rate ratio * | 1 (ref.) | 1.05 (0.78–1.40) | 1.07 (0.80–1.44) |
| Participants aged ≥ 70 years | |||
| Cases/Person-years | 89/3204 | 89/3502 | 74/2730 |
| Multivariable adjusted rate ratio * | 1 (ref.) | 0.90 (0.67–1.22) | 1.01 (0.74–1.38) |
| Sex | |||
| Men | |||
| Cases/Person-years | 59/4451 | 86/5137 | 67/5300 |
| Multivariable adjusted rate ratio ** | 1 (ref.) | 1.22 (0.87–1.70) | 1.00 (0.70–1.43) |
| Women | |||
| Cases/Person-years | 120/6183 | 120/6591 | 107/5419 |
| Multivariable adjusted rate ratio ** | 1 (ref.) | 0.92 (0.71–1.19) | 1.12 (0.86–1.45) |
| Body mass index | |||
| <30 kg/m2 | |||
| Cases/Person-years | 81/5412 | 111/6197 | 93/5932 |
| Multivariable adjusted rate ratio *** | 1 (ref.) | 1.23 (0.92–1.64) | 1.14 (0.84–1.54) |
| ≥30 kg/m2 | |||
| Cases/Person-years | 98/5222 | 95/5530 | 81/4786 |
| Multivariable adjusted rate ratio *** | 1 (ref.) | 0.86 (0.65–1.15) | 0.97 (0.72–1.31) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Layana, A.; Ciufo, G.; Toledo, E.; Martínez-González, M.A.; Corella, D.; Fitó, M.; Estruch, R.; Gómez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. The Effect of a Mediterranean Diet on the Incidence of Cataract Surgery. Nutrients 2017, 9, 453. https://doi.org/10.3390/nu9050453
García-Layana A, Ciufo G, Toledo E, Martínez-González MA, Corella D, Fitó M, Estruch R, Gómez-Gracia E, Fiol M, Lapetra J, et al. The Effect of a Mediterranean Diet on the Incidence of Cataract Surgery. Nutrients. 2017; 9(5):453. https://doi.org/10.3390/nu9050453
Chicago/Turabian StyleGarcía-Layana, Alfredo, Gianfranco Ciufo, Estefania Toledo, Miguel A. Martínez-González, Dolores Corella, Montse Fitó, Ramon Estruch, Enrique Gómez-Gracia, Miguel Fiol, José Lapetra, and et al. 2017. "The Effect of a Mediterranean Diet on the Incidence of Cataract Surgery" Nutrients 9, no. 5: 453. https://doi.org/10.3390/nu9050453