FRoG—A New Calculation Engine for Clinical Investigations with Proton and Carbon Ion Beams at CNAO

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Comparison of FLUKA- and FRoG-Calculated Spread Out Bragg Peaks
2.2. Comparison of FLUKA- and FRoG-Calculated Patient Cases
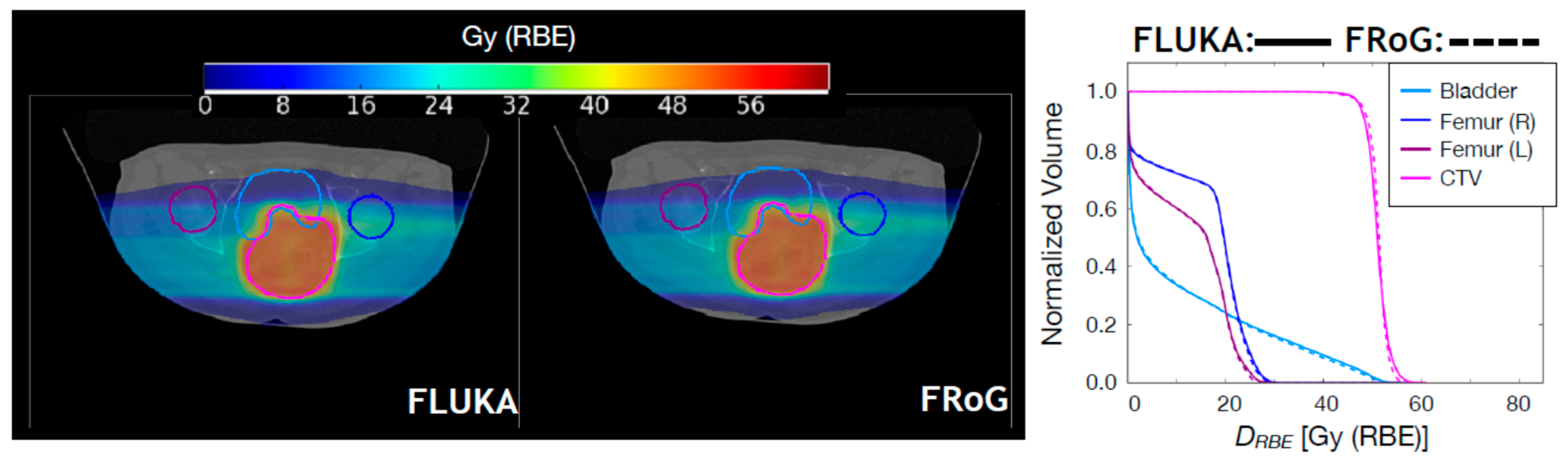
2.2.1. Proton Beams
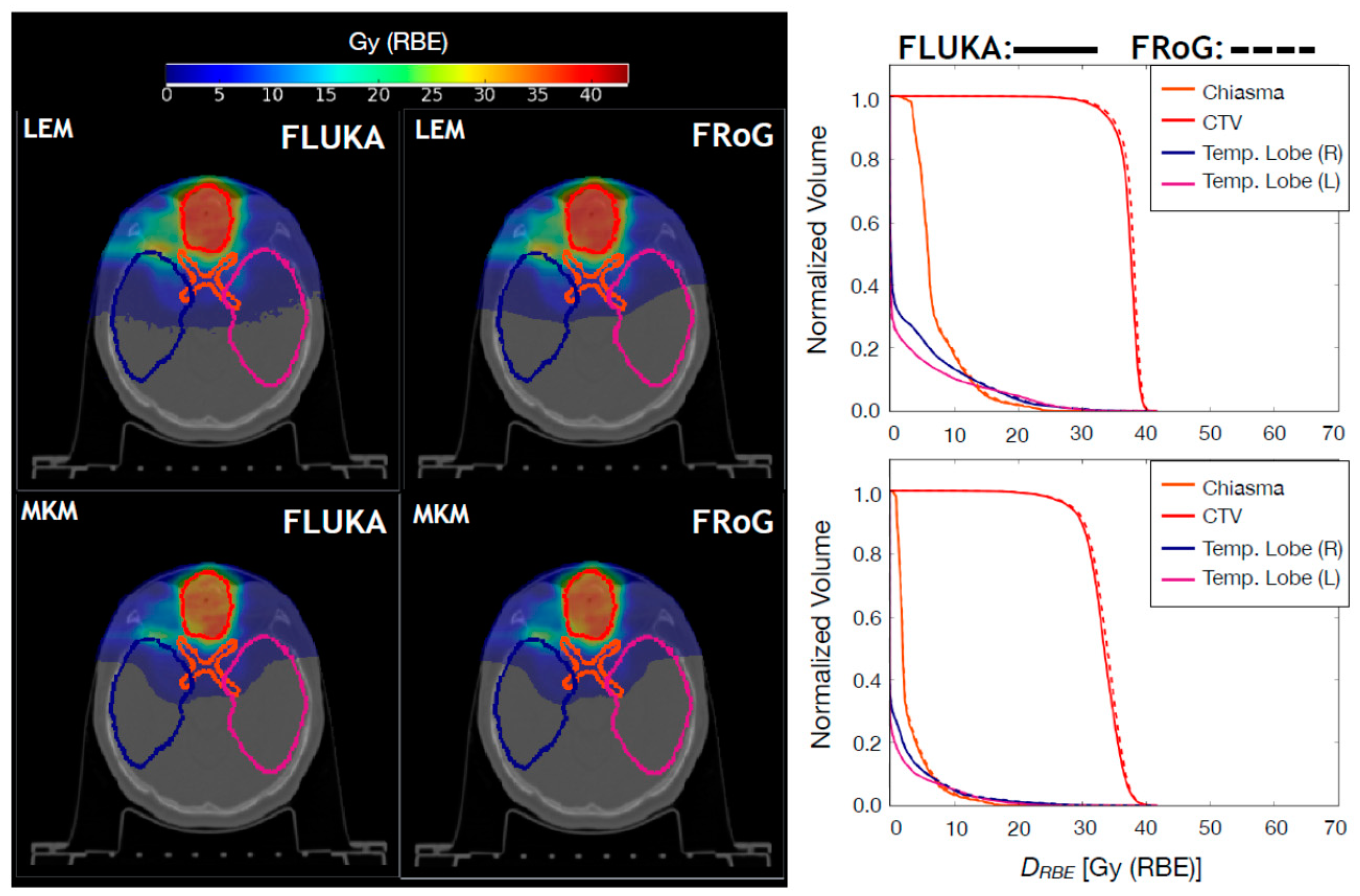
2.2.2. Carbon Ion Beams
2.3. Comparison against Dosimetric Data
3. Discussion
4. Materials and Methods
4.1. FRoG Workflow and Design Information
4.2. Benchmark of the FRoG Predictions with Proton and Carbon Ion Beams
4.2.1. Comparison against FLUKA Predictions
4.2.2. Comparison against Dosimetric Data
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saini, J.; Maes, D.; Egan, A.; Bowen, S.R.; James, S.S.; Janson, M.; Wong, T.; Bloch, C. Dosimetric evaluation of a commercial proton spot scanning Monte-Carlo dose algorithm: Comparisons against measurements and simulations. Phys. Med. Biol. 2017, 62, 7659–7681. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Schümann, J.; Paganetti, H.; Jiang, S.B. GPU-based fast Monte Carlo dose calculation for proton therapy. Phys. Med. Biol. 2012, 57, 7783–7797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, N.; Pinto, M.; Tian, Z.; Dedes, G.; Pompos, A.; Jiang, S.B.; Parodi, K.; Jia, X. Initial development of goCMC: A GPU-oriented fast cross-platform Monte Carlo engine for carbon ion therapy. Phys. Med. Biol. 2017, 62, 3682–3699. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S. The national centre for oncological hadrontherapy (CNAO): Status and perspectives. Phys. Med. 2015, 31, 333–351. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiation Units & Measurements. Prescribing, Recording and Reporting Proton-Beam Therapy (ICRU Report 78). Available online: https://icru.org/home/reports/prescribing-recording-and-reporting-proton-beam-therapy-icru-report-78 (accessed on 15 August 2018).
- Scholz, M.; Kellerer, A.M.; Kraft-Weyrather, W.; Kraft, G. Computation of cell survival in heavy ion beams for therapy. Radiat. Environ. Biophys. 1997, 36, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Molinelli, S.; Mairani, A.; Mirandola, A.; Panizza, D.; Russo, S.; Ferrari, A.; Valvo, F.; Fossati, P.; Ciocca, M. Dosimetric accuracy of a treatment planning system for actively scanned proton beams and small target volumes: Monte Carlo and experimental validation. Phys. Med. Biol. 2015, 60, 6865–6880. [Google Scholar] [CrossRef] [PubMed]
- Inaniwa, T.; Furukawa, T.; Kase, Y.; Matsufuji, N.; Toshito, T.; Matsumoto, Y.; Furusawa, Y.; Noda, K. Treatment planning for a scanned carbon beam with a modified microdosimetric kinetic model. Phys. Med. Biol. 2010, 55, 6721–6737. [Google Scholar] [CrossRef] [PubMed]
- Inaniwa, T.; Kanematsu, N.; Matsufuji, N.; Kanai, T.; Shirai, T.; Noda, K.; Tsuji, H.; Kamada, T.; Tsujii, H. Reformulation of a clinical-dose system for carbon-ion radiotherapy treatment planning at the National Institute of Radiological Sciences, Japan. Phys. Med. Biol. 2015, 60, 3271–3286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fossati, P.; Molinelli, S.; Matsufuji, N.; Ciocca, M.; Mirandola, A.; Mairani, A.; Mizoe, J.; Hasegawa, A.; Imai, R.; Kamada, R.; et al. Dose prescription in carbon ion radiotherapy: A planning study to compare NIRS and LEM approaches with a clinically-oriented strategy. Phys. Med. Biol. 2012, 57, 7543–7554. [Google Scholar] [CrossRef] [PubMed]
- Molinelli, S.; Magro, G.; Mairani, A.; Matsufuji, N.; Kanematsu, N.; Inaniwa, T.; Mirandola, A.; Russo, S.; Mastella, E.; Hasegawa, A.; et al. Dose prescription in carbon ion radiotherapy: How to compare two different RBE-weighted dose calculation systems. Radiother. Oncol. 2016, 120, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Haberer, T.; Debus, J.; Jäkel, O.; Schulz-Ertner, D.; Weber, U. The Heidelberg ion therapy center. Radiother. Oncol. 2004, 73, 186–190. [Google Scholar] [CrossRef]
- Giovannini, G.; Böhlen, T.T.; Cabal, G.; Bauer, J.; Tessonnier, T.; Frey, K.; Debus, J.; Mairani, K.; Parodi, A. Variable RBE in proton therapy: Comparison of different model predictions and their influence on clinical-like scenario. Radiat. Oncol. 2016, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Mairani, A.; Dokic, I.; Magro, G.; Tessonnier, T.; Bauer, J.; Böhlen, T.T.; Ciocca, M.; Ferrari, A.; Sala, P.R.; Jäkel, O.; et al. A phenomenological relative biological effectiveness approach for proton therapy based on an improved description of the mixed radiation field. Phys. Med. Biol. 2017, 61, 1378–1395. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Sala, P.R.; Fassò, A.; Ranft, J. FLUKA: A Multi-Particle Transport Code. CERN-2005-10, SLAC-R-773. Available online: https://www.slac.stanford.edu/pubs/slacreports/reports16/slac-r-773.pdf (accessed on 15 August 2018).
- Böhlen, T.T.; Cerutti, F.; Chin, M.P.W.; Fassò, A.; Ferrari, A.; Ortega, P.G.; Mairani, A.; Sala, P.R.; Smirnov, G.; Vlachoudis, V. The FLUKA Code: Developments and Challenges for High Energy and Medical Applications. Nucl. Data Sheets 2014, 120, 211–214. [Google Scholar] [CrossRef]
- Battistoni, G.; Bauer, J.; Böhlen, T.T.; Cerutti, F.; Chin, M.P.W.; Dos Santos Augusto, R.; Ferrari, A.; Ortega, G.; Kozlowska, W.; Magro, G.; et al. The FLUKA Code: An Accurate Simulation Tool for Particle Therapy. Front. Oncol. 2016, 6, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Molinelli, S.; Mairani, A.; Mirandola, A.; Vilches Freixas, G.; Tessonnier, T.; Giordanengo, S.; Parodi, K.; Ciocca, M.; Orecchia, R. Dosimetric accuracy assessment of a treatment plan verification system for scanned proton beam radiotherapy: One-year experimental results and Monte Carlo analysis of the involved uncertainties. Phys. Med. Biol. 2013, 58, 3837–3847. [Google Scholar] [CrossRef] [PubMed]
- Mairani, A.; Böhlen, T.T.; Schiavi, A.; Tessonnier, T.; Molinelli, S.; Brons, S.; Battistoni, G.; Parodi, K.; Patera, V. A Monte Carlo-based treatment planning tool for proton therapy. Phys. Med. Biol. 2013, 58, 2471–2490. [Google Scholar] [CrossRef] [PubMed]
- Mirandola, A.; Molinelli, S.; Vilches Freixas, G.; Mairani, A.; Gallio, E.; Panizza, D.; Russo, S.; Ciocca, M.; Donetti, M.; Magro, G.; et al. Dosimetric commissioning and quality assurance of scanned ion beams at the Italian National Center for Oncological Hadrontherapy. Med. Phys. 2015, 42, 5287–5300. [Google Scholar] [CrossRef] [PubMed]
- Parodi, K.; Mairani, A.; Sommerer, F. Monte Carlo-based parametrization of the lateral dose spread for clinical treatment planning of scanned proton and carbon ion beams. J. Radiat. Res. 2013, 54, i91–i96. [Google Scholar] [CrossRef] [PubMed]
- Low, D.A.; Harms, W.B.; Mutic, S.; Purdy, J.A. A technique for quantitative evaluation of dose distributions. Med. Phys. 1998, 25, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Wendling, M.; Zijp, L.J.; McDermott, L.N.; Smit, E.J.; Sonke, J.J.; Mijnheer, B.J.; van Herk, M. A fast algorithm for gamma evaluation in 3D. Med. Phys. 2007, 34, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Mein, S.; Choi, K.; Kopp, B.; Tessonnier, T.; Bauer, J.; Ferrari, A.; Haberer, T.; Debus, J.; Abdollahi, A.; Mairani, A. Fast robust dose calculation on GPU for high-precision 1H, 4He, 12C and 16O ion therapy: The FRoG platform. Sci. Rep. 2018, 8, 14829. [Google Scholar] [CrossRef] [PubMed]
- Szymanowski, H.; Oelfke, U. Two-dimensional pencil beam scaling: An improved proton dose algorithm for heterogeneous media. Phys. Med. Biol. 2002, 47, 3313–3330. [Google Scholar] [CrossRef] [PubMed]
- Inaniwa, T.; Kanematsu, N. A trichrome beam model for biological dose calculation in scanned carbon-ion radiotherapy treatment planning. Phys. Med. Biol. 2014, 60, 437–451. [Google Scholar] [CrossRef]
- Bauer, J.; Sommerer, F.; Mairani, A.; Unholtz, D.; Farook, R.; Handrack, J.; Frey, K.; Marcelos, T.; Tessonnier, T.; Ecker, S.; et al. Integration and evaluation of automated Monte Carlo simulations in the clinical practice of scanned proton and carbon ion beam therapy. Phys. Med. Biol. 2014, 59, 4635–4659. [Google Scholar] [CrossRef] [PubMed]
- Peeler, C.R.; Mirkovic, D.; Titt, U.; Blanchard, P.; Gunther, J.R.; Mahajan, A.; Mohan, R.; Grosshans, D.R. Clinical evidence of variable proton biological effectiveness in pediatric patients treated for ependymoma. Radiother. Oncol. 2016, 121, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parodi, K.; Mairani, A.; Brons, S.; Hasch, B.G.; Sommerer, F.; Naumann, J.; Jäkel, O.; Haberer, T.; Debus, J. Monte Carlo simulations to support start-up and treatment planning of scanned proton and carbon ion therapy at a synchrotron-based facility. Phys. Med. Biol. 2012, 57, 3759–3784. [Google Scholar] [CrossRef] [PubMed]
- James, F.; Roos, M. Minuit—A system for function minimization and analysis of the parameter errors and correlations. Comput. Phys. Commun. 1975, 10, 343–367. [Google Scholar] [CrossRef]
- Brun, R.; Rademakers, F. ROOT—An object oriented data analysis framework. Nucl. Instrum. Methods Phys. Res. A 1997, 389, 81–86. [Google Scholar] [CrossRef]
- Tessonnier, T.; Böhlen, T.T.; Ceruti, F.; Ferrari, A.; Sala, P.; Brons, S.; Haberer, T.; Debus, J.; Parodi, K.; Mairani, A. Dosimetric verification in water of a Monte Carlo treatment planning tool for proton, helium, carbon and oxygen ion beams at the Heidelberg Ion Beam Therapy Center. Phys. Med. Biol. 2017, 62, 6579–6594. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Dahle, T.J.; Molinelli, S.; Ciocca, M.; Fossati, P.; Ferrari, A.; Inaniwa, T.; Matsufuji, N.; Ytre-Hauge, K.S.; Mairani, A. The FLUKA Monte Carlo code coupled with the NIRS approach for clinical dose calculations in carbon ion therapy. Phys. Med. Biol. 2017, 62, 3814–3827. [Google Scholar] [CrossRef] [PubMed]
- Mairani, A.; Brons, S.; Cerutti, F.; Fassò, A.; Ferrari, A.; Krämer, M.; Parodi, K.; Scholz, M.; Sommerer, F. The FLUKA Monte Carlo code coupled with the local effect model for biological calculations in carbon ion therapy. Phys. Med. Biol. 2010, 55, 4273–4289. [Google Scholar] [CrossRef] [PubMed]
- De Greef, M.; Crezee, J.; Van Eijk, J.C.; Pool, R.; Bel, A. Accelerated ray tracing for radiotherapy dose calculations on a GPU. Med. Phys. 2009, 36, 4095–4102. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.; Attili, A.; Battistoni, G.; Bertrand, D.; Bourhaleb, F.; Cappucci, F.; Ciocca, M.; Mairani, A.; Milian, F.M.; Molinelli, S.; et al. A novel algorithm for the calculation of physical and biological irradiation quantities in scanned ion beam therapy: The beamlet superposition approach. Phys. Med. Biol. 2016, 61, 183–214. [Google Scholar] [CrossRef] [PubMed]
- Karger, C.P.; Jäkel, O.; Hartmann, G.H.; Heeg, P. A system for three-dimensional dosimetric verification of treatment plans in intensity-modulated radiotherapy with heavy ions. Med. Phys. 1999, 26, 2125–2132. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percent Difference of | Target Volume | 3 cm | 12 cm | 21 cm |
|---|---|---|---|---|
| DRBE,50 | 27 cm3 216 cm3 | 0.67% 0.59% | 0.59% 0.61% | 0.88% 0.71% |
| DRBE,2 | 27 cm3 216 cm3 | 0.91% −0.60% | −0.09% 0.08% | 0.47% 0.73% |
| DRBE,98 | 27 cm3 216 cm3 | 0.52% 0.46% | 0.43% 1.10% | 1.07% 0.47% |
| Percent Difference of | Target Volume | 3 cm | 12 cm | 21 cm |
|---|---|---|---|---|
| DRBE,50 | 27 cm3 216 cm3 | 0.93% 0.58% | 0.39% 0.64% | −0.01% 1.02% |
| DRBE,2 | 27 cm3 216 cm3 | −1.01% −1.14% | −2.45% −0.65% | −2.27% 0.02% |
| DRBE,98 | 27 cm3 216 cm3 | −2.19% 2.14% | −0.18% 2.95% | 2.03% 0.78% |
| Percent Difference of | Target Volume | 3 cm | 12 cm | 21 cm |
|---|---|---|---|---|
| DRBE,50 | 27 cm3 216 cm3 | −1.13% −0.46% | −2.10% −0.41% | −2.97% −0.26% |
| DRBE,2 | 27 cm3 216 cm3 | −0.19% −0.68% | −0.90% −1.41% | −2.11% −2.48% |
| DRBE,98 | 27 cm3 216 cm3 | 0.81% −0.30% | −2.38% 1.91% | −3.86% −0.84% |
| Percent Difference of | Total | H&N No RS | H&N with RS | Pelvic |
|---|---|---|---|---|
| DRBE,50 | 0.68% ± 0.21% | 1.05% ± 0.32% | 0.34% ± 0.50% | 0.65% ± 0.31% |
| DRBE,2 | −0.57% ± 0.41% | −0.91% ± 0.55% | −0.84% ± 1.05% | 0.02% ± 0.67% |
| DRBE,98 | 0.41% ± 0.56% | 1.25% ± 0.42% | −0.79% ± 1.55% | 0.77% ± 0.81% |
| Percent Difference of | Biological Model | Total | H&N | Pelvic |
|---|---|---|---|---|
| DRBE,50 | LEM MKM | 0.96% ± 0.33% 1.46% ± 0.30% | 0.52% ± 0.52% 1.23% ± 0.30% | 1.40% ± 0.38% 1.69% ± 0.50% |
| DRBE,2 | LEM MKM | 0.97% ± 0.30% 1.81% ± 0.46% | 0.93% ± 0.62% 2.57% ± 0.78% | 1.01% ± 0.32% 1.05% ± 0.36% |
| DRBE,98 | LEM MKM | 2.23% ± 0.34% 2.36% ± 0.30% | 2.80% ± 0.65% 2.93% ± 0.46% | 1.67% ± 0.18% 1.79% ± 0.23% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, K.; Mein, S.B.; Kopp, B.; Magro, G.; Molinelli, S.; Ciocca, M.; Mairani, A. FRoG—A New Calculation Engine for Clinical Investigations with Proton and Carbon Ion Beams at CNAO. Cancers 2018, 10, 395. https://doi.org/10.3390/cancers10110395
Choi K, Mein SB, Kopp B, Magro G, Molinelli S, Ciocca M, Mairani A. FRoG—A New Calculation Engine for Clinical Investigations with Proton and Carbon Ion Beams at CNAO. Cancers. 2018; 10(11):395. https://doi.org/10.3390/cancers10110395
Chicago/Turabian StyleChoi, KyungDon, Stewart B Mein, Benedikt Kopp, Giuseppe Magro, Silvia Molinelli, Mario Ciocca, and Andrea Mairani. 2018. "FRoG—A New Calculation Engine for Clinical Investigations with Proton and Carbon Ion Beams at CNAO" Cancers 10, no. 11: 395. https://doi.org/10.3390/cancers10110395