Focal Adhesion Genes Refine the Intermediate-Risk Cytogenetic Classification of Acute Myeloid Leukemia

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
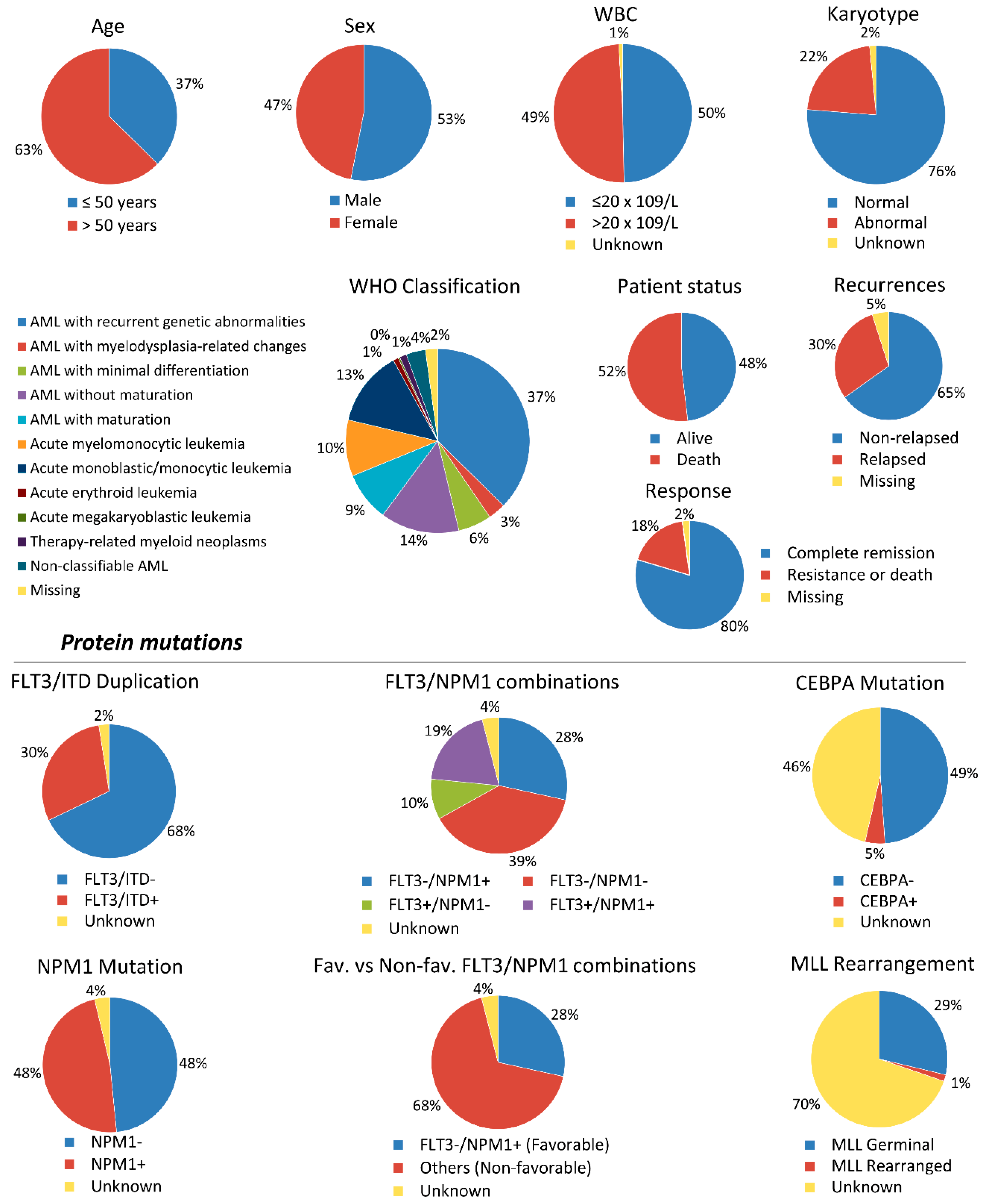
2.1. Patient Characteristics
2.2. PTK2B and LYN Overexpression Are Independent Favorable Prognostic Factors for OS and DFS, Whereas Overexpression of PTK2B Prognosticates also a Favorable CIR in IR-AML Patients
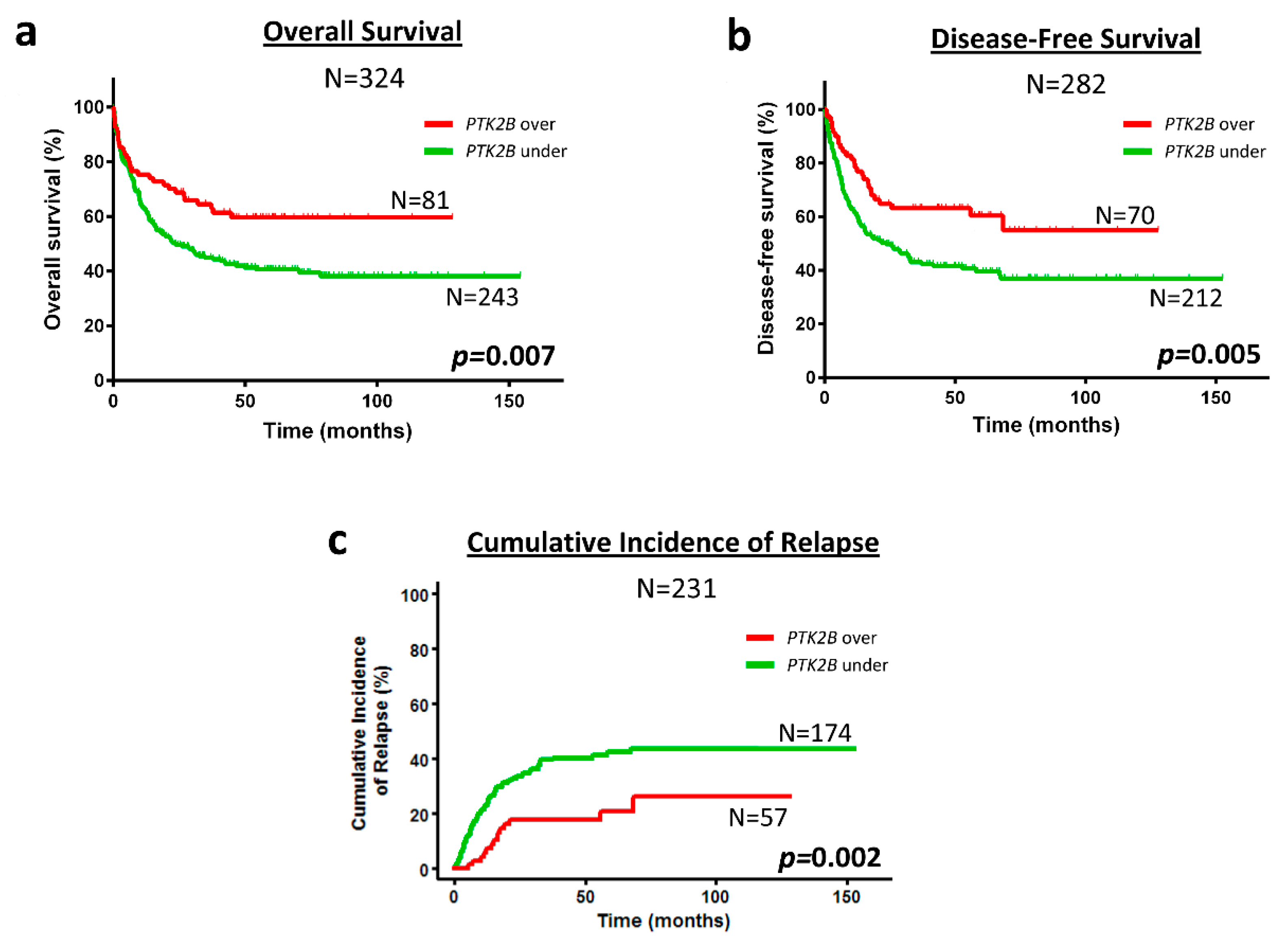
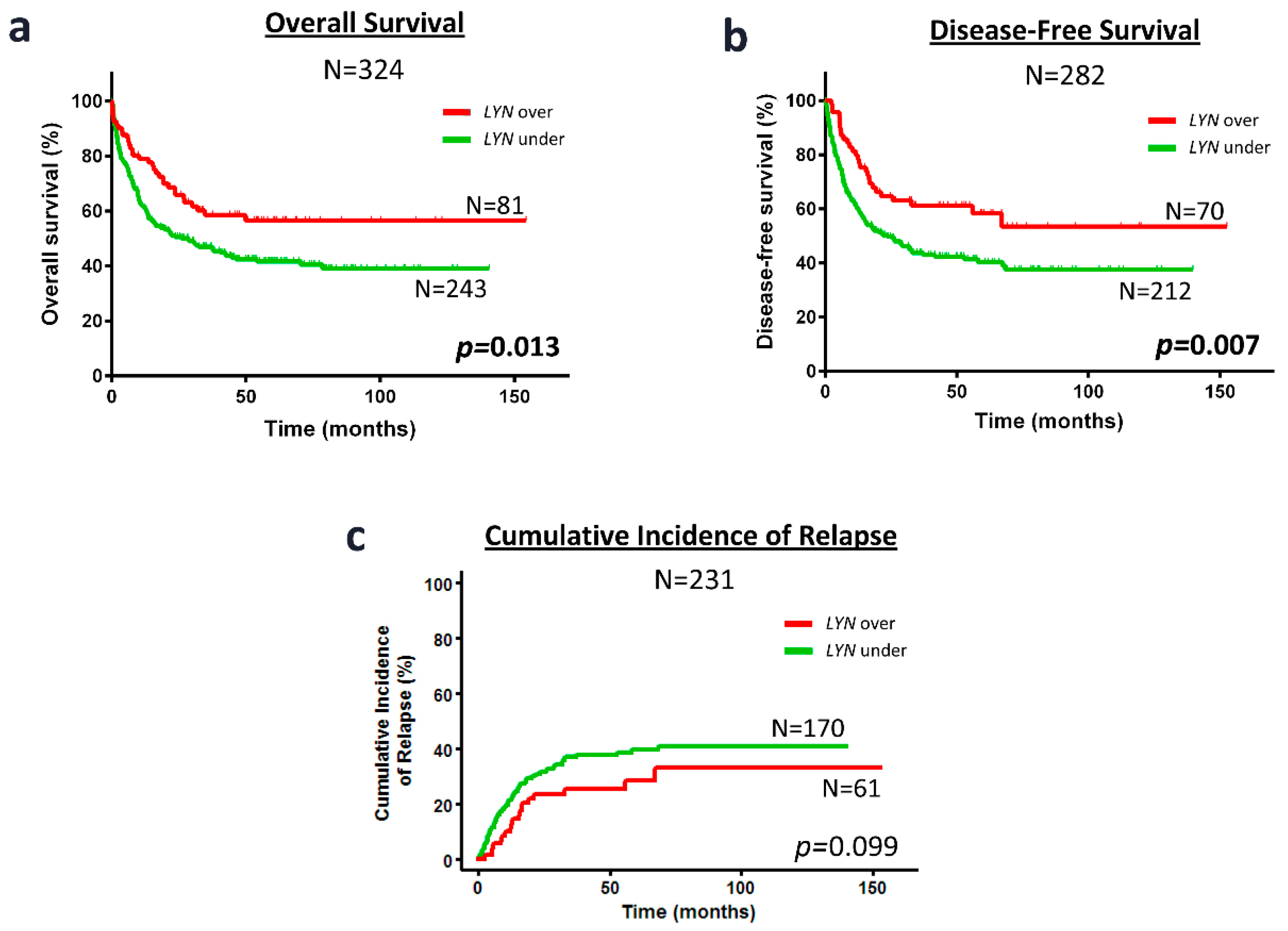
2.3. Kaplan-Meier Curves Confirm the Favorable Prognosis of PKT2B or LYN Overexpression Regarding IR-AML Patient OS, DFS or CIR
2.4. Overexpression of PTK2B or LYN Associated with Higher Rate of Alive Patients and Lower Rate of Relapse in Cytogenetic IR-AML Patients
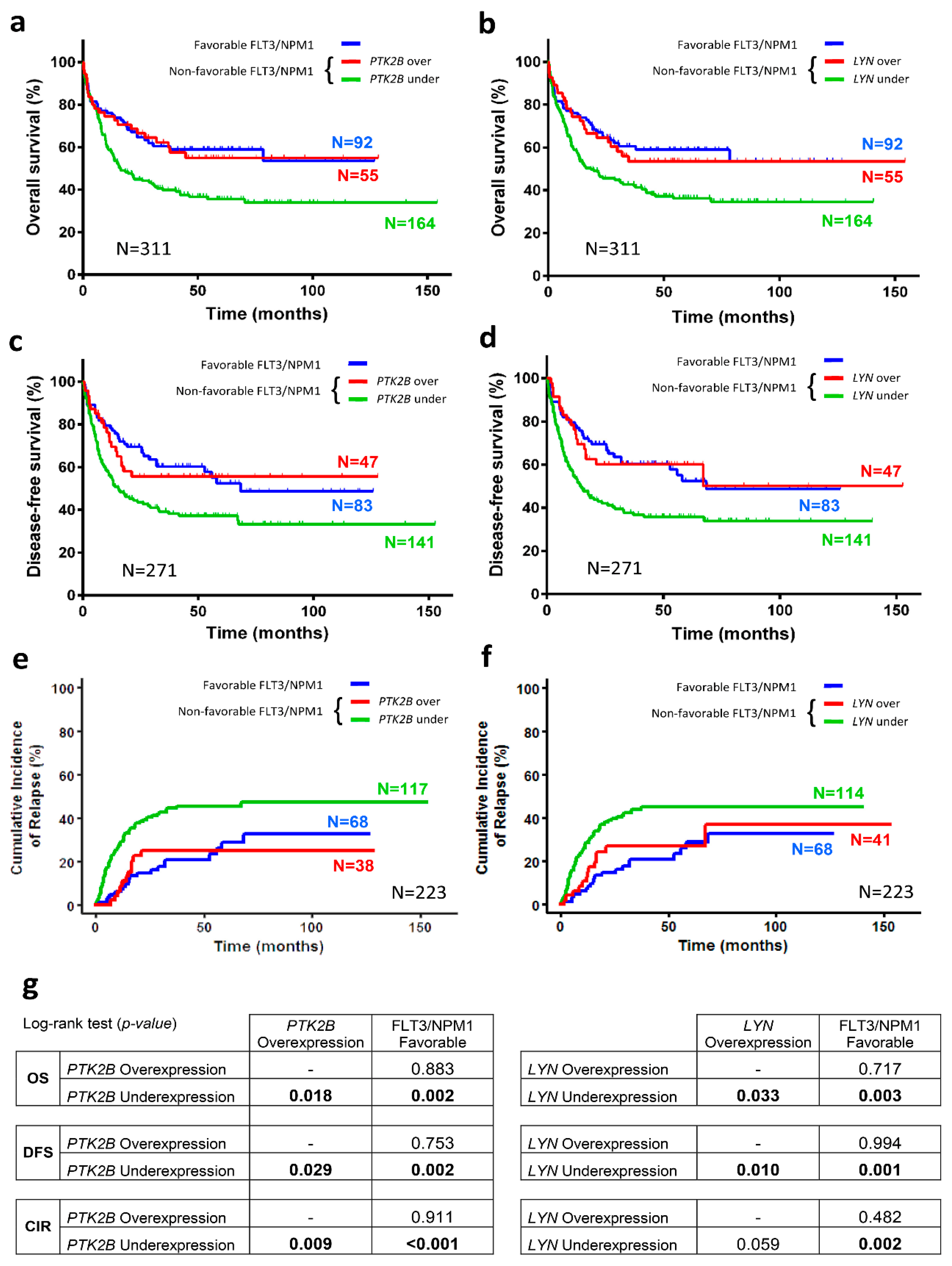
2.5. Overexpression of PTK2B or LYN in Cytogenetic IR-AML Patients with Non-Favorable FLT3/NPM1 Combinations Is as Good in Prognosticating Survival or Recurrence as the Favorable FLT3/NPM1 Combination
2.6. PTK2B or LYN Overexpression Are Independent Favorable Prognostic Factors for OS, DFS and CIR in Cytogenetic IR-AML Patients with Non-Favorable FLT3/NPM1 Combinations
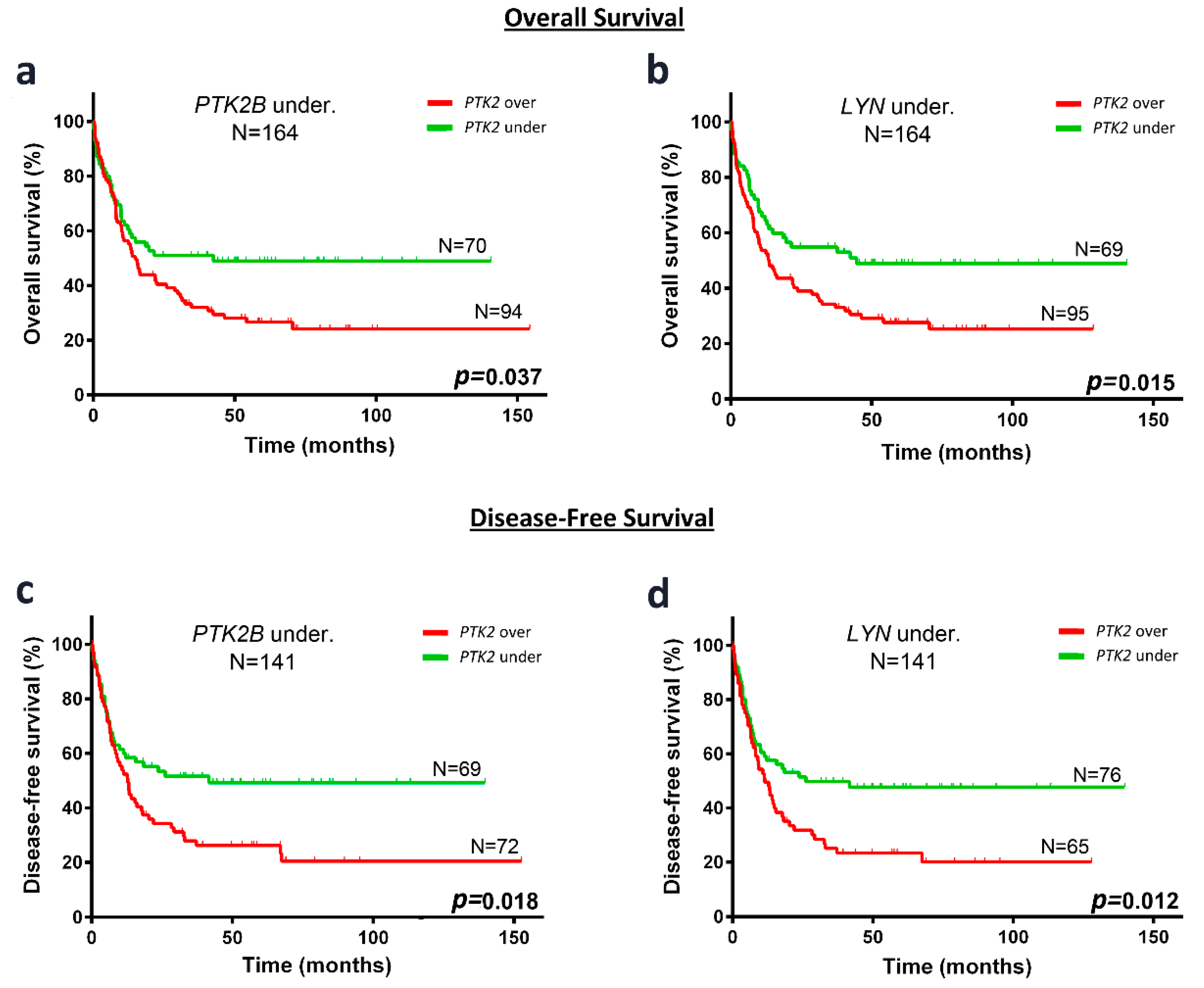
2.7. In Cytogenetic IR-AML Patients with Non-Favorable FLT3/NPM1 Combinations and PTK2B or LYN Underexpression, PTK2 Overexpression Identify a Subgroup with Unfavorable OS and DFS
2.8. A Multivariate Analysis Confirms PTK2 Overexpression as an Independent Prognostic Factor for OS and DFS in Cytogenetic IR-AML Patients with Non-Favorable FLT3/NPM1 Combinations and PTK2B or LYN Underexpression
3. Discussion
3.1. PTK2B and LYN Overexpression Are Independent Prognostic Factors for Favorable Outcome in Cytogenetic IR-AML Patients
3.2. PTK2B or LYN Overexpression Add Prognostic Value to the Cytogenetic IR-AML Patient Subgroup with Non-Favorable FLT3/NPM1 Combinations
3.3. Impact of the PTK2 Overexpression on the Prognosis of Cytogenetic IR-AML Patients with Non-Favorable FLT3/NPM1 Combinations that Underexpress PTK2B or LYN
4. Materials and Methods
4.1. Patients
4.2. Time-Dependent Clinical Outcome Endpoints
4.3. RNA Extraction and Gene Expression Analyses
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Endnotes
Author Contributions
Funding
Conflicts of Interest
References
- Döhner, H.; Weisdorf, D.J.; Bloomfield, C.D. Acute Myeloid Leukemia. N. Engl. J. Med. 2015, 373, 1136–1152. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.L.; Bailey, N.G. Acute Myeloid Leukemia Genetics: Risk Stratification and Implications for Therapy. Arch. Pathol. Lab. Med. 2015, 139, 1215–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinisch, A.; Chan, S.M.; Thomas, D.; Majeti, R. Biology and Clinical Relevance of Acute Myeloid Leukemia Stem Cells. Semin. Hematol. 2015, 52, 150–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.-H.; Li, Y.-H.; Yu, L. Genomics-based Approach and Prognostic Stratification Significance of Gene Mutations in Intermediate-risk Acute Myeloid Leukemia. Chin. Med. J. 2015, 128, 2395–2403. [Google Scholar] [CrossRef] [PubMed]
- Döhner, K.; Paschka, P. Intermediate-risk acute myeloid leukemia therapy: Current and future. Hematology Am. Soc. Hematol. Educ. Program. 2014, 2014, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Hefazi, M.; Siddiqui, M.; Patnaik, M.; Wolanskyj, A.; Alkhateeb, H.; Zblewski, D.; Elliott, M.; Hogan, W.; Litzow, M.; Al-Kali, A. Prognostic impact of combined NPM1+/FLT3− genotype in patients with acute myeloid leukemia with intermediate risk cytogenetics stratified by age and treatment modalities. Leuk. Res. 2015, 39, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- How, J.; Sykes, J.; Minden, M.D.; Gupta, V.; Yee, K.W.L.; Schimmer, A.D.; Schuh, A.C.; Kamel-Reid, S.; Brandwein, J.M. The prognostic impact of FLT3-ITD and NPM1 mutations in patients with relapsed acute myeloid leukemia and intermediate-risk cytogenetics. Blood Cancer J. 2013, 3, e116. [Google Scholar] [CrossRef] [PubMed]
- Schlenk, R.F.; Döhner, K.; Krauter, J.; Fröhling, S.; Corbacioglu, A.; Bullinger, L.; Habdank, M.; Späth, D.; Morgan, M.; Benner, A.; et al. German-Austrian Acute Myeloid Leukemia Study Group Mutations and treatment outcome in cytogenetically normal acute myeloid leukemia. N. Engl. J. Med. 2008, 358, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- Pratcorona, M.; Brunet, S.; Nomdedéu, J.; Ribera, J.M.; Tormo, M.; Duarte, R.; Escoda, L.; Guàrdia, R.; Queipo de Llano, M.P.; Salamero, O.; et al. Grupo Cooperativo Para el Estudio y Tratamiento de las Leucemias Agudas Mieloblásticas Favorable outcome of patients with acute myeloid leukemia harboring a low-allelic burden FLT3-ITD mutation and concomitant NPM1 mutation: Relevance to post-remission therapy. Blood 2013, 121, 2734–2738. [Google Scholar] [CrossRef] [PubMed]
- Green, C.L.; Koo, K.K.; Hills, R.K.; Burnett, A.K.; Linch, D.C.; Gale, R.E. Prognostic significance of CEBPA mutations in a large cohort of younger adult patients with acute myeloid leukemia: Impact of double CEBPA mutations and the interaction with FLT3 and NPM1 mutations. J. Clin. Oncol. 2010, 28, 2739–2747. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.P.; Gönen, M.; Figueroa, M.E.; Fernandez, H.; Sun, Z.; Racevskis, J.; Van Vlierberghe, P.; Dolgalev, I.; Thomas, S.; Aminova, O.; et al. Prognostic Relevance of Integrated Genetic Profiling in Acute Myeloid Leukemia. N. Engl. J. Med. 2012, 366, 1079–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gocek, E.; Moulas, A.N.; Studzinski, G.P. Non-receptor protein tyrosine kinases signaling pathways in normal and cancer cells. Crit. Rev. Clin. Lab. Sci. 2014, 51, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Yu, D. Targeting Src family kinases in anti-cancer therapies: Turning promise into triumph. Trends Pharmacol. Sci. 2012, 33, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Ingley, E. Functions of the Lyn tyrosine kinase in health and disease. Cell. Commun. Signal. 2012, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.M.; Park, H.; Lim, S.-T.S. FAK and Pyk2 in disease. Front. Biol. 2016, 11, 1–9. [Google Scholar] [CrossRef]
- Sen, B.; Johnson, F.M. Regulation of Src Family Kinases in Human Cancers. J. Signal. Transduct. 2011, 2011, e865819. [Google Scholar] [CrossRef] [PubMed]
- Recher, C.; Ysebaert, L.; Beyne-Rauzy, O.; Mansat-De Mas, V.; Ruidavets, J.-B.; Cariven, P.; Demur, C.; Payrastre, B.; Laurent, G.; Racaud-Sultan, C. Expression of focal adhesion kinase in acute myeloid leukemia is associated with enhanced blast migration, increased cellularity, and poor prognosis. Cancer Res. 2004, 64, 3191–3197. [Google Scholar] [CrossRef] [PubMed]
- Tavernier-Tardy, E.; Cornillon, J.; Campos, L.; Flandrin, P.; Duval, A.; Nadal, N.; Guyotat, D. Prognostic value of CXCR4 and FAK expression in acute myelogenous leukemia. Leuk. Res. 2009, 33, 764–768. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.Z.; Mak, P.Y.; Wang, X.; Yang, H.; Garcia-Manero, G.; Mak, D.; Mu, H.; Ruvolo, V.; Qiu, Y.; Coombes, K.; et al. Focal Adhesion Kinase as a Potential Target in AML and MDS. Mol. Cancer Ther. 2017, 16, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Despeaux, M.; Chicanne, G.; Rouer, E.; De Toni-Costes, F.; Bertrand, J.; Mansat-De Mas, V.; Vergnolle, N.; Eaves, C.; Payrastre, B.; Girault, J.-A.; et al. Focal adhesion kinase splice variants maintain primitive acute myeloid leukemia cells through altered Wnt signaling. Stem Cells 2012, 30, 1597–1610. [Google Scholar] [CrossRef] [PubMed]
- Avraham, H.; Park, S.Y.; Schinkmann, K.; Avraham, S. RAFTK/Pyk2-mediated cellular signalling. Cell. Signal. 2000, 12, 123–133. [Google Scholar] [CrossRef]
- Llewellyn, R.A.; Thomas, K.S.; Gutknecht, M.F.; Bouton, A.H. The nonreceptor protein tyrosine kinase Pyk2 promotes the turnover of monocytes at steady state. J. Leukoc. Biol. 2017, 102, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Naser, R.; Aldehaiman, A.; Díaz-Galicia, E.; Arold, S.T. Endogenous Control Mechanisms of FAK and PYK2 and Their Relevance to Cancer Development. Cancers 2018, 10, 196. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, D.; Hideshima, T.; Pandey, P.; Treon, S.; Teoh, G.; Raje, N.; Rosen, S.; Krett, N.; Husson, H.; Avraham, S.; et al. RAFTK/PYK2-dependent and -independent apoptosis in multiple myeloma cells. Oncogene 1999, 18, 6733–6740. [Google Scholar] [CrossRef] [PubMed]
- Avdi, N.J.; Nick, J.A.; Whitlock, B.B.; Billstrom, M.A.; Henson, P.M.; Johnson, G.L.; Worthen, G.S. Tumor Necrosis Factor-α Activation of the c-Jun N-terminal Kinase Pathway in Human Neutrophils INTEGRIN INVOLVEMENT IN A PATHWAY LEADING FROM CYTOPLASMIC TYROSINE KINASES TO APOPTOSIS. J. Biol. Chem. 2001, 276, 2189–2199. [Google Scholar] [CrossRef] [PubMed]
- Pandey, P.; Avraham, S.; Place, A.; Kumar, V.; Majumder, P.K.; Cheng, K.; Nakazawa, A.; Saxena, S.; Kharbanda, S. Bcl-xL blocks activation of related adhesion focal tyrosine kinase/proline-rich tyrosine kinase 2 and stress-activated protein kinase/c-Jun N-terminal protein kinase in the cellular response to methylmethane sulfonate. J. Biol. Chem. 1999, 274, 8618–8623. [Google Scholar] [CrossRef] [PubMed]
- Otte, A.; Mandel, K.; Reinstrom, G.; Hass, R. Abolished adherence alters signaling pathways in phorbol ester-induced human U937 cells. Cell. Commun. Signal. 2011, 9, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, Y.; Tohyama, Y.; Hishita, T.; Lala, A.; De Nardin, E.; Yoshida, Y.; Yamamura, H.; Uchiyama, T.; Tohyama, K. Pyk2 and Syk participate in functional activation of granulocytic HL-60 cells in a different manner. Blood 2000, 96, 1733–1739. [Google Scholar] [PubMed]
- Dos Santos, C.; Demur, C.; Bardet, V.; Prade-Houdellier, N.; Payrastre, B.; Récher, C. A critical role for Lyn in acute myeloid leukemia. Blood 2008, 111, 2269–2279. [Google Scholar] [CrossRef] [PubMed]
- Karur, V.G.; Lowell, C.A.; Besmer, P.; Agosti, V.; Wojchowski, D.M. Lyn kinase promotes erythroblast expansion and late-stage development. Blood 2006, 108, 1524–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harder, K.W.; Parsons, L.M.; Armes, J.; Evans, N.; Kountouri, N.; Clark, R.; Quilici, C.; Grail, D.; Hodgson, G.S.; Dunn, A.R.; et al. Gain- and Loss-of-Function Lyn Mutant Mice Define a Critical Inhibitory Role for Lyn in the Myeloid Lineage. Immunity 2001, 15, 603–615. [Google Scholar] [CrossRef]
- Iriyama, N.; Yuan, B.; Hatta, Y.; Takagi, N.; Takei, M. Lyn, a tyrosine kinase closely linked to the differentiation status of primary acute myeloid leukemia blasts, associates with negative regulation of all-trans retinoic acid (ATRA) and dihydroxyvitamin D3 (VD3)-induced HL-60 cells differentiation. Cancer Cell. Int. 2016, 16, 37. [Google Scholar] [CrossRef] [PubMed]
- Stafford, S.; Lowell, C.; Sur, S.; Alam, R. Lyn tyrosine kinase is important for IL-5-stimulated eosinophil differentiation. J. Immunol. 2002, 168, 1978–1983. [Google Scholar] [CrossRef] [PubMed]
- Tilbrook, P.A.; Ingley, E.; Williams, J.H.; Hibbs, M.L.; Klinken, S.P. Lyn tyrosine kinase is essential for erythropoietin-induced differentiation of J2E erythroid cells. EMBO J. 1997, 16, 1610–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, M.B.; Johnson, D.E. Signal transduction pathways that contribute to myeloid differentiation. Leukemia 2007, 21, 1363–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatterjee, A.; Ghosh, J.; Ramdas, B.; Mali, R.S.; Martin, H.; Kobayashi, M.; Vemula, S.; Canela, V.H.; Waskow, E.R.; Visconte, V.; et al. Regulation of Stat5 by FAK and PAK1 in Oncogenic FLT3- and KIT-Driven Leukemogenesis. Cell. Rep. 2014, 9, 1333–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gombart, A.F.; Hofmann, W.-K.; Kawano, S.; Takeuchi, S.; Krug, U.; Kwok, S.H.; Larsen, R.J.; Asou, H.; Miller, C.W.; Hoelzer, D.; et al. Mutations in the gene encoding the transcription factor CCAAT/enhancer binding protein alpha in myelodysplastic syndromes and acute myeloid leukemias. Blood 2002, 99, 1332–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimwade, D.; Hills, R.K.; Moorman, A.V.; Walker, H.; Chatters, S.; Goldstone, A.H.; Wheatley, K.; Harrison, C.J.; Burnett, A.K.; on behalf of the N.C.R.I.A.L.W. Group. Refinement of cytogenetic classification in acute myeloid leukemia: Determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood 2010, 116, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Grimwade, D.; Walker, H.; Oliver, F.; Wheatley, K.; Harrison, C.; Harrison, G.; Rees, J.; Hann, I.; Stevens, R.; Burnett, A.; et al. The importance of diagnostic cytogenetics on outcome in AML: Analysis of 1612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children’s Leukaemia Working Parties. Blood 1998, 92, 2322–2333. [Google Scholar] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Perea, G.; Lasa, A.; Aventín, A.; Domingo, A.; Villamor, N.; Queipo de Llano, M.P.; Llorente, A.; Juncà, J.; Palacios, C.; Fernández, C.; et al. Grupo Cooperativo para el Estudio y Tratamiento de las Leucemias Agudas y Miel Prognostic value of minimal residual disease (MRD) in acute myeloid leukemia (AML) with favorable cytogenetics [t(8;21) and inv(16)]. Leukemia 2006, 20, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef] [PubMed]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014.
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. REporting recommendations for tumor MARKer prognostic studies (REMARK). Nat. Clin. Pract. Oncol. 2005, 2, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Mallett, S.; Timmer, A.; Sauerbrei, W.; Altman, D.G. Reporting of prognostic studies of tumour markers: A review of published articles in relation to REMARK guidelines. Br. J. Cancer 2010, 102, 173–180. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OS (N = 324) | DFS (N = 282) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | ||||||||||
| Variable | Item | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≤50 years | 1 | 1 | ||||||||||
| >50 years | 1.947 | 1.389–2.730 | <0.001 | 2.131 | 1.501–3.025 | <0.001 | 1.639 | 1.158–2.319 | 0.005 | 1.798 | 1.254–2.580 | 0.001 | |
| Sex | Male | 1 | 1 | ||||||||||
| Female | 0.953 | 0.703–1.291 | 0.756 | - | - | - | 0.985 | 0.712–1.362 | 0.927 | - | - | - | |
| WBC | ≤20 × 109/L | 1 | 1 | ||||||||||
| >20 × 109/L | 0.856 | 0.631–1.161 | 0.318 | - | - | - | 0.792 | 0.571–1.098 | 0.162 | - | - | - | |
| FLT3 | FLT3/ITD− | 1 | 1 | ||||||||||
| FLT3/ITD+ | 1.209 | 0.871–1.678 | 0.256 | - | - | - | 1.231 | 0.867–1.748 | 0.246 | - | - | - | |
| NPM1 | NPM1− | 1 | 1 | ||||||||||
| NPM1+ | 0.834 | 0.612–1.138 | 0.252 | - | - | - | 0.907 | 0.652–1.263 | 0.564 | - | - | - | |
| FLT3/NPM1 | Favorable | 1 | 1 | ||||||||||
| Non-favorable | 1.586 | 1.098–2.292 | 0.014 | 1.859 | 1.281–2.699 | 0.001 | 1.617 | 1.102–2.372 | 0.014 | 1.809 | 1.226–2.668 | 0.003 | |
| Karyotype | Normal | 1 | 1 | ||||||||||
| Abnormal | 1.285 | 0.905–1.824 | 0.162 | - | - | - | 0.972 | 0.650–1.454 | 0.890 | - | - | - | |
| PTK2B | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 0.589 | 0.398–0.870 | 0.008 | 0.630 | 0.423–0.939 | 0.023 | 0.552 | 0.363–0.838 | 0.005 | 0.585 | 0.382–0.896 | 0.014 | |
| LYN | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 0.621 | 0.424–0.909 | 0.014 | 0.649 | 0.440–0.957 | 0.029 | 0.569 | 0.377–0.859 | 0.007 | 0.596 | 0.392–0.908 | 0.016 | |
| PTK2 | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 1.083 | 0.771–1.520 | 0.646 | - | - | - | 1.267 | 0.886–1.813 | 0.195 | - | - | - | |
| SRC | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 0.981 | 0.693–1.387 | 0.913 | - | - | - | 1.012 | 0.697–1.468 | 0.952 | - | - | - | |
| CIR (N = 282) | |||||||
|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | ||||||
| Variable | Item | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≤50 years | 1 | |||||
| >50 years | 1.180 | 0.779–1.780 | 0.440 | - | - | - | |
| Sex | Male | 1 | |||||
| Female | 1.080 | 0.725–1.610 | 0.710 | - | - | - | |
| WBC | ≤20 × 109/L | 1 | |||||
| >20 × 109/L | 1.070 | 0.717–1.600 | 0.740 | - | - | - | |
| FLT3 | FLT3/ITD− | 1 | |||||
| FLT3/ITD+ | 1.300 | 0.925–1.820 | 0.130 | - | - | - | |
| NPM1 | NPM1− | 1 | |||||
| NPM1+ | 0.819 | 0.576–1.160 | 0.270 | - | - | - | |
| FLT3/NPM1 | Favorable | 1 | |||||
| Non-favorable | 1.920 | 1.190–3.090 | 0.007 | 1.935 | 1.198–3.127 | 0.007 | |
| Karyotype | Normal | 1 | |||||
| Abnormal | 0.795 | 0.500–1.260 | 0.330 | - | - | - | |
| PTK2B | Underexpression | 1 | |||||
| Overexpression | 0.426 | 0.246–0.738 | 0.002 | 0.449 | 0.258–0.781 | 0.005 | |
| LYN | Underexpression | 1 | |||||
| Overexpression | 0.662 | 0.406–1.080 | 0.098 | 0.650 | 0.391–1.080 | 0.097 | |
| PTK2 | Underexpression | 1 | |||||
| Overexpression | 0.838 | 0.525–1.340 | 0.460 | - | - | - | |
| SRC | Underexpression | 1 | |||||
| Overexpression | 0.953 | 0.597–1.520 | 0.840 | - | - | - | |
| Cohort | PTK2B | LYN | |||||
|---|---|---|---|---|---|---|---|
| Parameter | Total (N = 324) | Under-Expressed | Over-Expressed | p-Value | Under-Expressed | Over-Expressed | p-Value |
| Age, median (range) | 55 (17–70) | 243 | 81 | 0.309 ‡ | 243 | 81 | 0.623 ‡ |
| ≤50 years (%) | 121 (37) | 86 | 35 | 0.233 | 90 | 31 | 0.895 |
| >50 years (%) | 203 (63) | 157 | 46 | 153 | 50 | ||
| Sex, (%) | |||||||
| Male | 172 (53) | 129 | 43 | 1.000 | 132 | 40 | 0.444 |
| Female | 152 (47) | 114 | 38 | 111 | 41 | ||
| WBC, median (range) | 20 (0.03–325) | 240 | 81 | 0.138 ‡ | 240 | 81 | 0.066 ‡ |
| ≤20 × 109/L (%) | 161 (50) | 124 | 37 | 0.371 | 128 | 33 | 0.055 |
| >20 × 109/L (%) | 160 (50) | 116 | 44 | 112 | 48 | ||
| Unknown | 3 (<1) | ||||||
| Karyotype, (%) | |||||||
| Normal | 247 (76) | 190 | 57 | 0.091 | 183 | 64 | 0.643 |
| Abnormal | 72 (22) | 48 | 24 | 56 | 16 | ||
| Unknown | 5 (2) | ||||||
| Protein mutations, (%) | |||||||
| FLT3/ITD− | 220 (68) | 167 | 53 | 0.575 | 170 | 50 | 0.161 |
| FLT3/ITD+ | 96 (30) | 70 | 26 | 67 | 29 | ||
| Unknown | 8 (2) | ||||||
| NPM1− | 157 (48) | 116 | 41 | 0.696 | 122 | 35 | 0.242 |
| NPM1+ | 155 (48) | 118 | 37 | 111 | 44 | ||
| Unknown | 12 (4) | ||||||
| FLT3−/NPM1+ | 92 (28) | 69 | 23 | 0.311 * | 66 | 26 | 0.177 * |
| FLT3−/NPM1− | 125 (39) | 96 | 29 | 101 | 24 | ||
| FLT3+/NPM1− | 31 (10) | 19 | 12 | 20 | 11 | ||
| FLT3+/NPM1+ | 63 (19) | 49 | 14 | 45 | 18 | ||
| Unknown | 13 (4) | ||||||
| FLT3−/NPM1+ (Fav.) | 92 (28) | 69 | 23 | 1.000 | 66 | 26 | 0.477 |
| Others (Non-fav.) | 219 (68) | 164 | 55 | 166 | 53 | ||
| Unknown | 13 (4) | ||||||
| Patient status, (%) | |||||||
| Alive | 156 (48) | 106 | 50 | 0.007 | 108 | 48 | 0.029 |
| Death | 168 (52) | 137 | 31 | 135 | 33 | ||
| No relapsed | 211 (65) | 148 | 63 | 0.007 | 154 | 57 | 0.259 |
| Relapsed | 97 (30) | 82 | 15 | 77 | 20 | ||
| Missing | 16 (5) | ||||||
| Complete Remission | 258 (80) | 195 | 63 | 0.739 | 191 | 67 | 0.620 |
| Resistance or death | 59 (18) | 43 | 16 | 46 | 13 | ||
| Missing | 7 (2) | ||||||
| OS (N = 219) | DFS (N = 188) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | ||||||||||
| Variable | Item | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≤50 years | 1 | 1 | ||||||||||
| >50 years | 1.913 | 1.319–2.774 | 0.001 | 1.873 | 1.291–2.716 | 0.001 | 1.707 | 1.151–2.533 | 0.008 | 1.673 | 1.127–2.483 | 0.011 | |
| Sex | Male | 1 | 1 | ||||||||||
| Female | 0.885 | 0.618–1.265 | 0.502 | - | - | - | 0.921 | 0.626–1.354 | 0.675 | - | - | - | |
| WBC | ≤20 × 109/L | 1 | 1 | ||||||||||
| >20 × 109/L | 0.868 | 0.609–1.239 | 0.436 | - | - | - | 0.939 | 0.639–1.380 | 0.749 | - | - | - | |
| FLT3 | FLT3/ITD− | 1 | 1 | ||||||||||
| FLT3/ITD+ | 0.993 | 0.693–1.422 | 0.969 | - | - | - | 1.021 | 0.693–1.502 | 0.918 | - | - | - | |
| NPM1 | NPM1− | 1 | 1 | ||||||||||
| NPM1+ | 1.180 | 0.799–1.742 | 0.406 | - | - | - | 1.400 | 0.932–2.103 | 0.105 | - | - | - | |
| Karyotype | Normal | 1 | 1 | ||||||||||
| Abnormal | 1.065 | 0.714–1.590 | 0.757 | - | - | - | 0.789 | 0.496–1.256 | 0.318 | - | - | - | |
| PTK2B | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 0.583 | 0.370–0.918 | 0.020 | 0.605 | 0.384–0.953 | 0.030 | 0.584 | 0.359–0.951 | 0.031 | 0.601 | 0.369–0.979 | 0.041 | |
| LYN | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 0.618 | 0.396–0.966 | 0.035 | 0.625 | 0.400–0.977 | 0.039 | 0.527 | 0.320–0.866 | 0.012 | 0.532 | 0.324–0.875 | 0.013 | |
| PTK2 | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 1.065 | 0.715–1.587 | 0.757 | - | - | - | 1.168 | 0.764–1.784 | 0.473 | - | - | - | |
| SRC | Underexpression | 1 | |||||||||||
| Overexpression | 0.894 | 0.592–1.349 | 0.593 | - | - | - | 0.900 | 0.574–1.411 | 0.646 | - | - | - | |
| CIR (N = 188) | |||||||
|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | ||||||
| Variable | Item | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≤50 years | 1 | |||||
| >50 years | 1.190 | 0.746–1.880 | 0.470 | 1.170 | 0.734–1.865 | 0.510 | |
| Sex | Male | 1 | |||||
| Female | 1.200 | 0.757–1.900 | 0.440 | - | - | - | |
| WBC | ≤20 × 109/L | 1 | |||||
| >20 × 109/L | 1.310 | 0.830–2.080 | 0.250 | - | - | - | |
| FLT3 | FLT3/ITD− | 1 | |||||
| FLT3/ITD+ | 1.220 | 0.766–1.930 | 0.410 | - | - | - | |
| NPM1 | NPM1− | 1 | |||||
| NPM1+ | 1.350 | 0.817–2.240 | 0.240 | - | - | - | |
| Karyotype | Normal | 1 | |||||
| Abnormal | 0.737 | 0.431–1.260 | 0.270 | - | - | - | |
| PTK2B | Underexpression | 1 | |||||
| Overexpression | 0.440 | 0.238–0.814 | 0.009 | 0.442 | 0.238–0.818 | 0.009 | |
| LYN | Underexpression | 1 | |||||
| Overexpression | 0.569 | 0.317–1.020 | 0.059 | 0.573 | 0.319–1.030 | 0.062 | |
| PTK2 | Underexpression | 1 | |||||
| Overexpression | 0.728 | 0.428–1.240 | 0.240 | - | - | - | |
| SRC | Underexpression | 1 | |||||
| Overexpression | 0.838 | 0.482-1.460 | 0.530 | - | - | - | |
| OS (N = 164) | DFS (N = 141) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | ||||||||||
| Variable | Item | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≤50 years | 1 | 1 | ||||||||||
| >50 years | 1.717 | 1.140–2.585 | 0.010 | 1.708 | 1.135–2.572 | 0.010 | 1.627 | 1.048–2.525 | 0.030 | 1.498 | 0.957–2.346 | 0.077 | |
| Sex | Male | 1 | 1 | ||||||||||
| Female | 0.885 | 0.594–1.319 | 0.549 | - | - | - | 0.977 | 0.635–1.502 | 0.914 | - | - | - | |
| WBC | ≤20 × 109/L | 1 | 1 | ||||||||||
| >20 × 109/L | 1.003 | 0.676–1.488 | 0.988 | - | - | - | 1.083 | 0.706–1.662 | 0.714 | - | - | - | |
| FLT3 | FLT3/ITD− | 1 | 1 | ||||||||||
| FLT3/ITD+ | 1.185 | 0.797–1.762 | 0.401 | - | - | - | 1.299 | 0.847–1.994 | 0.231 | - | - | - | |
| NPM1 | NPM1− | 1 | 1 | ||||||||||
| NPM1+ | 1.179 | 0.770–1.803 | 0.449 | - | - | - | 1.498 | 0.958–2.341 | 0.076 | 1.517 | 0.958–2.401 | 0.075 | |
| Karyotype | Normal | 1 | 1 | ||||||||||
| Abnormal | 0.928 | 0.582-1.482 | 0.756 | - | - | - | 0.677 | 0.392–1.169 | 0.161 | - | - | - | |
| PTK2 | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 1.548 | 1.023–2.343 | 0.039 | 1.538 | 1.017–2.328 | 0.042 | 1.686 | 1.089–2.610 | 0.019 | 1.758 | 1.131–2.734 | 0.012 | |
| OS (N = 164) | DFS (N = 141) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | ||||||||||
| Variable | Item | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ≤50 years | 1 | 1 | ||||||||||
| >50 years | 1.928 | 1.272–2.922 | 0.002 | 1.868 | 1.232–2.834 | 0.003 | 1.722 | 1.111–2.670 | 0.015 | 1.556 | 0.995–2.432 | 0.052 | |
| Sex | Male | 1 | 1 | ||||||||||
| Female | 0.733 | 0.487–1.101 | 0.135 | - | - | - | 0.796 | 0.517–1.225 | 0.299 | - | - | - | |
| WBC | ≤20 × 109/L | 1 | 1 | ||||||||||
| >20 × 109/L | 0.901 | 0.605–1.341 | 0.607 | - | - | - | 1.007 | 0.658–1.541 | 0.975 | - | - | - | |
| FLT3 | FLT3/ITD− | 1 | 1 | ||||||||||
| FLT3/ITD+ | 1.031 | 0.687–1.546 | 0.884 | - | - | - | 1.236 | 0.806–1.895 | 0.332 | - | - | - | |
| NPM1 | NPM1− | 1 | 1 | ||||||||||
| NPM1+ | 1.199 | 0.769–1.869 | 0.423 | - | - | - | 1.505 | 0.957–2.367 | 0.077 | 1.584 | 0.991–2.531 | 0.054 | |
| Karyotype | Normal | 1 | 1 | ||||||||||
| Abnormal | 1.013 | 0.650–1.581 | 0.954 | - | - | - | 0.714 | 0.428–1.191 | 0.196 | - | - | - | |
| PTK2 | Underexpression | 1 | 1 | ||||||||||
| Overexpression | 1.669 | 1.098–2.536 | 0.016 | 1.600 | 1.052–2.433 | 0.028 | 1.722 | 1.123–-2.641 | 0.013 | 1.815 | 1.172–2.812 | 0.008 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pallarès, V.; Hoyos, M.; Chillón, M.C.; Barragán, E.; Prieto Conde, M.I.; Llop, M.; Falgàs, A.; Céspedes, M.V.; Montesinos, P.; Nomdedeu, J.F.; et al. Focal Adhesion Genes Refine the Intermediate-Risk Cytogenetic Classification of Acute Myeloid Leukemia. Cancers 2018, 10, 436. https://doi.org/10.3390/cancers10110436
Pallarès V, Hoyos M, Chillón MC, Barragán E, Prieto Conde MI, Llop M, Falgàs A, Céspedes MV, Montesinos P, Nomdedeu JF, et al. Focal Adhesion Genes Refine the Intermediate-Risk Cytogenetic Classification of Acute Myeloid Leukemia. Cancers. 2018; 10(11):436. https://doi.org/10.3390/cancers10110436
Chicago/Turabian StylePallarès, Victor, Montserrat Hoyos, M. Carmen Chillón, Eva Barragán, M. Isabel Prieto Conde, Marta Llop, Aïda Falgàs, María Virtudes Céspedes, Pau Montesinos, Josep F. Nomdedeu, and et al. 2018. "Focal Adhesion Genes Refine the Intermediate-Risk Cytogenetic Classification of Acute Myeloid Leukemia" Cancers 10, no. 11: 436. https://doi.org/10.3390/cancers10110436