Clinical Impact of RANK Signalling in Ovarian Cancer
by
 ,
,
Verena Wieser
1, 
Susanne Sprung
2,
Irina Tsibulak
1,
Johannes Haybaeck
2,
Hubert Hackl
3,
Heidelinde Fiegl
1,
Christian Marth
1 and
Alain Gustave Zeimet
1,* 1
Department of Obstetrics and Gynaecology, Medical University of Innsbruck, 6020 Innsbruck, Austria
2
Institute of Pathology, Medical University Innsbruck, 6020 Innsbruck, Austria
3
Biocenter, Division of Bioinformatics, Medical University Innsbruck, 6020 Innsbruck, Austria
*
Author to whom correspondence should be addressed.
Cancers 2019, 11(6), 791; https://doi.org/10.3390/cancers11060791
Submission received: 11 May 2019
/
Revised: 30 May 2019
/
Accepted: 6 June 2019
/
Published: 8 June 2019
Abstract
:Ovarian cancer (OC) is a gynaecological malignancy with poor clinical outcome and limited treatment options. The receptor activator of nuclear factor-κB (RANK) pathway, activated by RANK ligand (RANKL), critically controls bone metabolism, tumourigenesis and tumour immune responses. Denosumab, a monocloncal RANKL antibody, exerts tumour-suppressive effects in mice and humans. Here, we investigated the relevance of RANK signalling in OC. RANK, RANKL and OPG expression in 192 epithelial OC tissues was compared to expression in 35 non-malignant control tissues and related to clinico-pathological characteristics. Findings were validated in a cohort of 563 OC patients from The Cancer Genome Atlas (TCGA). The expression of RANK, RANKL and OPG was studied in four OC cell lines and the impact of RANK ligation or blockade on OC cell proliferation was determined. RANK, RANKL and OPG were expressed in epithelial and stromal cells in OC. RANKL expression was elevated in OC tissue, particularly in BRCA1/2 mutated tumours. High RANKL expression independently predicted reduced progression-free (PFS, p = 0.017) and overall survival (OS, p = 0.007), which could be validated in the TCGA cohort (PFS, p = 0.022; OS, p = 0.046, respectively). Expression of RANK and OPG in OC cells was induced by inflammatory cytokines IL-1β and TNFα. Neither recombinant RANK ligation nor denosumab treatment affected OC cell proliferation. Our study independently links RANKL expression with poor clinical outcome in two unrelated OC cohorts. These findings implicate RANK signalling in the immunopathogenesis of OC and warrant clinical trials with denosumab in OC.
1. Introduction
Ovarian cancer (OC) is one of the most common cancers amongst women in Europe and the leading cause of death in gynaecological cancers [1]. In recent years, multiple treatment modalities have emerged including surgical therapy, chemotherapy, anti-angiogenic agents, and PARP-inhibitors (PARPis). However, prognosis remains devastating and highlights the necessity for a better knowledge about disease pathogenesis and involved pathways [2].
The interplay of receptor activator of nuclear factor-κB (RANK), its ligand RANKL and Osteoprotegerin (OPG) are established regulators of bone metabolism. Specifically, RANKL expressed on osteoblasts activates RANK signalling and transcriptional activation of osteoclasts which promote osteoclastogenesis and bone resorption [3]. The endogenous OPG functions as a soluble decoy receptor preventing RANKL from activating its receptor RANK [4]. Moreover, the RANK/RANKL/OPG system also plays essential roles in immunity and tumourigenesis [5,6] and RANK/RANKL cancer cell expression correlated with metastasis and tumour progression in human breast cancer (BC) [7]. More specifically, previous studies demonstrated that RANKL mediates progesterone-driven mammary carcinogenesis [8,9,10] and RANK/RANKL signalling controlled BRCA1 mutation-driven mammary tumours [11]. Sigl et al. demonstrated that the genetic and pharmacological inhibition of RANKL in mice abolished the occurrence of Brca1 mutation-driven pre-neoplastic lesions [11]. Further, RANK/RANKL blockade impaired proliferation and expansion of mammary progenitors from human BRCA1 mutation carriers indicating a significant role of RANK/RANKL signalling in inherited BC. Therefore, BRCA-P, an international randomized phase III study (NCT01864798) investigates denosumab for the prevention of BC in BRCA1 mutation carriers. Notably, mutations in the BRCA1 gene are not only associated with inherited BC but also with OC. Although BC and OC present as distinct clinical entities, recent evidence supported a substantial overlap with respect to genetic and epigenetic alterations [12].
Furthermore, the inhibition of RANK signalling was demonstrated to improve the effectiveness of checkpoint blockade in experimental solid tumours, experimental metastasis and malignant melanoma patients [13,14,15]. This effect seems to depend on a functional immune system as the depletion of natural killer cells and T cells abrogates this effect in mice [16]. In line with this, a window of opportunity trial including pre-menopausal women with early BC, RANK pathway inhibition using denosumab resulted in a significant increase in TILs (NCT01864798), however, had less effect on tumour proliferation.
Regarding the potential relevance of RANK/RANKL in hereditary BC and in the immunopathogenesis of experimental tumours and malignant melanoma patients, we hypothesized a differential regulation of this pathway in OC. We, therefore, determined RANK, RANKL and OPG expression in 192 OC tissues and 35 non-malignant control tissues and performed association analysis with clinicopathological characteristics and clinical outcome of OC patients. To specifically understand RANK signalling in BRCA1/2 driven OC, tissue was separately analysed according to BRCA1/2 mutation status determined in OC tissue. To further strengthen our hypothesis, results were validated in a larger TCGA Affymetrix cohort comprising 563 OC patients (ovarian cystadenocarcinomas). Using four OC cell lines, inhibition and, vice versa, activation of the RANK pathway was performed to investigate a direct effect of RANK signalling on tumour cell proliferation.
2. Results
2.1. RANKL Is Highly Expressed in OC and BRCA1/2 Mutated Tumours
To assess a role for the RANK/RANKL/OPG pathway in OC, we analysed the expression in 192 OC samples by qPCR. Transcript levels were compared to 21 non-malignant ovaries and 14 non-malignant fallopian tubes of healthy controls. We found highly elevated RANKL and OPG expression in OC tissue compared to control tissues (Figure 1A,B), which was largely unrelated to histological subtype (Supplementary Materials Table S1). RANK was equally expressed in OC and non-malignant fallopian tubes, but lower expressed in non-malignant ovaries (Figure 1C). Spearman rank association analyses demonstrated a significant positive correlation between RANK, RANKL and OPG expression (RANK and RANKL: rs = 0.164, p = 0.018, Figure S1A; RANKL and OPG: rs = 0.167, p = 0.016, Figure S1B; RANK and OPG: rs = 0.214, p = 0.002, Figure S1C).
In a next step, RANK, RANKL and OPG expression was stratified according to BRCA1/2 mutation status available for 190 patients. In this cohort, 44 patients (22.9%) exhibited a BRCA1 or BRCA2 mutation. Notably, BRCA1/2 mutated cancers exhibited a higher RANKL expression (p = 0.033, Figure 1D), but not increased RANK or OPG expression (Figure S1D,E). More specifically, RANKL expression was significantly higher in BRCA1 mutated tumours (n = 35) compared to BRCA wild-type (wt) tumours and also elevated in BRCA2 mutated tumours (n = 9) which did not reach statistical significance (Figure S1F). Furthermore, we performed Spearman rank analysis for transcriptional levels of BRCA1/2 and RANK/RANKL/OPG. We found a direct correlation between BRCA2 and RANKL expression (rs = 0.309, p < 0.001; Figure S1G) and BRCA2 and OPG expression (rs = 0.230, p = 0.002; Supplementary Materials Figure S1H) but no correlation between BRCA1 and RANK/RANKL/OPG levels.
2.2. High RANKL mRNA Expression is Associated with Poor Prognosis
Based on the observation that OC patients exhibited increased RANKL expression, we next assessed an impact of RANK, RANKL and OPG expression on the clinical outcome of OC patients. We utilized the Youden Index to dichotomize the OC cohort into “high” and “low” RANK, RANKL and OPG expressing tumours [17]. Univariate survival analysis (Table 1) demonstrated that patients with low RANKL expression (<62nd percentile) in OC tissue exhibited a median progression-free survival (PFS) of 3.6 years (95% confidence interval (CI): 1.8–5.3) whereas patients with high RANKL (>62nd percentile) expression exhibited a median PFS of only 1.7 years (95% CI: 1.2–2.2) (p = 0.010; Figure 2A). There was also a strong association between high RANKL expression in OC tissue and impaired overall survival (OS): Patients with low RANKL expression (<62nd percentile) exhibited a median OS of 8.8 years (95% CI: 6.0–11.6) while patients with high RANKL expression (>62nd percentile) exhibited a median OS of 3.6 years (95% CI: 2.5–4.7), (p = 0.005; Figure 2B). This prognostic impact was unrelated to BRCA1/2 mutation status as we observed comparable results in the subgroup of patients with BRCA1/2 wt tumours (Supplementary Materials Figure S2A,B). BRCA1/2 mutation status, however, was not associated with clinical outcome in our OC cohort. When analysing the subgroup of patients suffering from HGSOC, which represents the majority of OC patients in our cohort, we observed similar results (Supplementary Materials Figure S3A–C).
Similar findings were notable for RANK expression in our cohort (Table 1): Patients with low RANK expression (<25th percentile) in OC tissue exhibited a median PFS of 3.6 years (CI: 0.9–6.2) whereas patients with high RANK expression (>25th percentile) exhibited a median PFS of only 2.0 years (CI: 1.5–2.4) (Figure 2C), however, this did not reach statistical significance (p = 0.117). In contrast, patients with low RANK expression (<25th percentile) in OC tissue exhibited a median OS of 9.3 years (CI: 2.0–16.6) while patients with high RANK expression (>25th percentile) exhibited a median OS of 3.71 years (CI: 1.85–5.57), (p = 0.030; Figure 2D). Importantly, multivariate analyses identified RANKL, but not RANK, as an independent prognostic factor for PFS (HR 1.42, p = 0.017; Table 1) and OS (HR 1.70, p = 0.007; Table 1). OPG expression (optimal cut-off: 92nd percentile) was not of prognostic significance regarding PFS or OS in our cohort (Table 1, Supplementary Materials Figure S4A,B).
2.3. Validation of the Prognostic Impact of RANKL Expression in an Independent Cohort
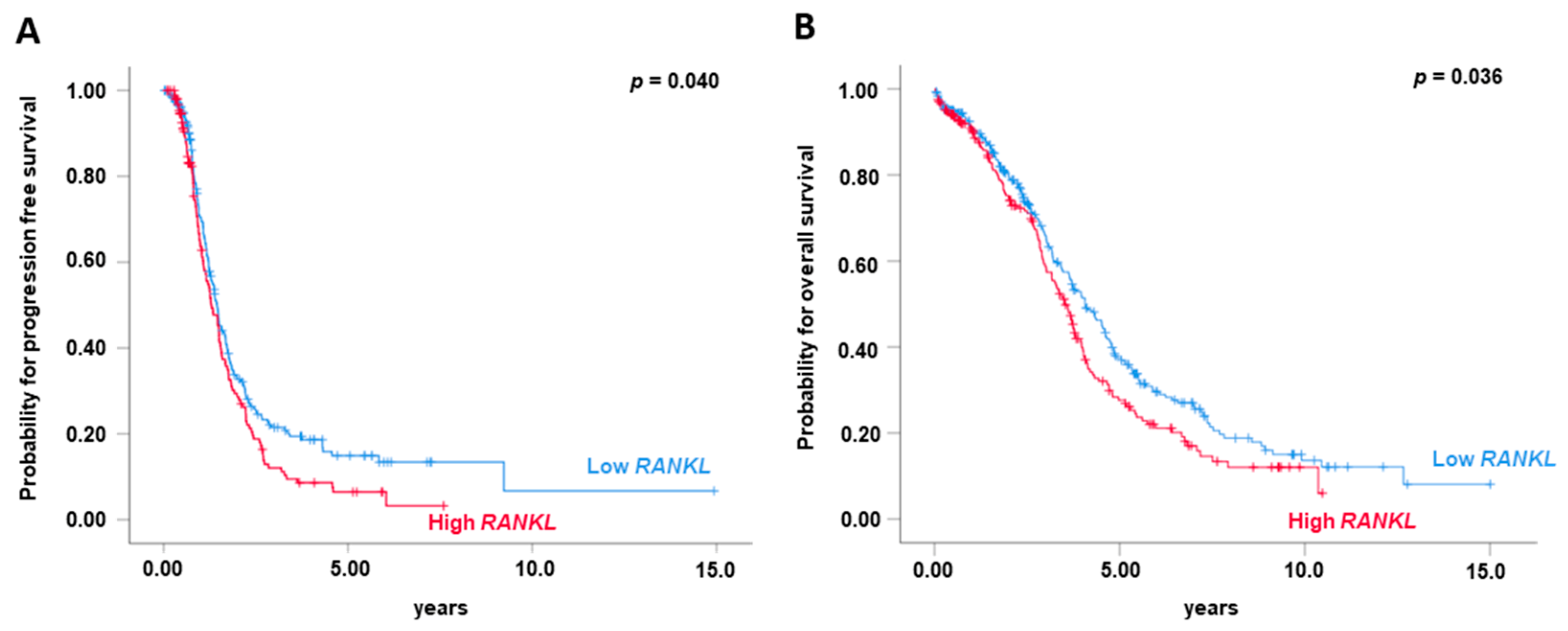
Gene expression datasets from The Cancer Genome Atlas (TCGA) project on primary serous ovarian carcinomas (n = 563) were analysed for the prognostic impact of RANKL expression on PFS and OS. High RANKL expression was associated with decreased PFS (p = 0.040, Figure 3A) and OS (p = 0.036, Figure 3B). Notably, also in the TCGA cohort, multivariate analyses identified RANKL as an independent prognostic factor for PFS (HR 1.32, p = 0.022; Table 2) and OS (HR 1.26, p = 0.046; Table 2). We did not find an impact of RANK or OPG expression on OC prognosis in the TCGA cohort.
We also performed a reverse analysis: We calculated the Youden Index for RANKL, RANK and OPG expression in the TCGA set and then applied this cut-off to the clinical analysis of both cohorts. Indeed, using the cut-off from the TCGA cohort, RANKL expression was associated with worse PFS (p = 0.032; Supplementary Materials Figure S5A) and OS (p = 0.026; Supplementary Materials Figure S5B) in the TCGA cohort, and also in our OC cohort (p = 0.013 and p = 0.007, respectively; Supplementary Materials Figure S5C,D). In contrast, RANK and OPG expression were not associated with worse OS or PFS in the TCGA cohort.
2.4. RANK, RANKL and OPG Are Expressed on Tumour Cells and in the Tumour Microenvironment
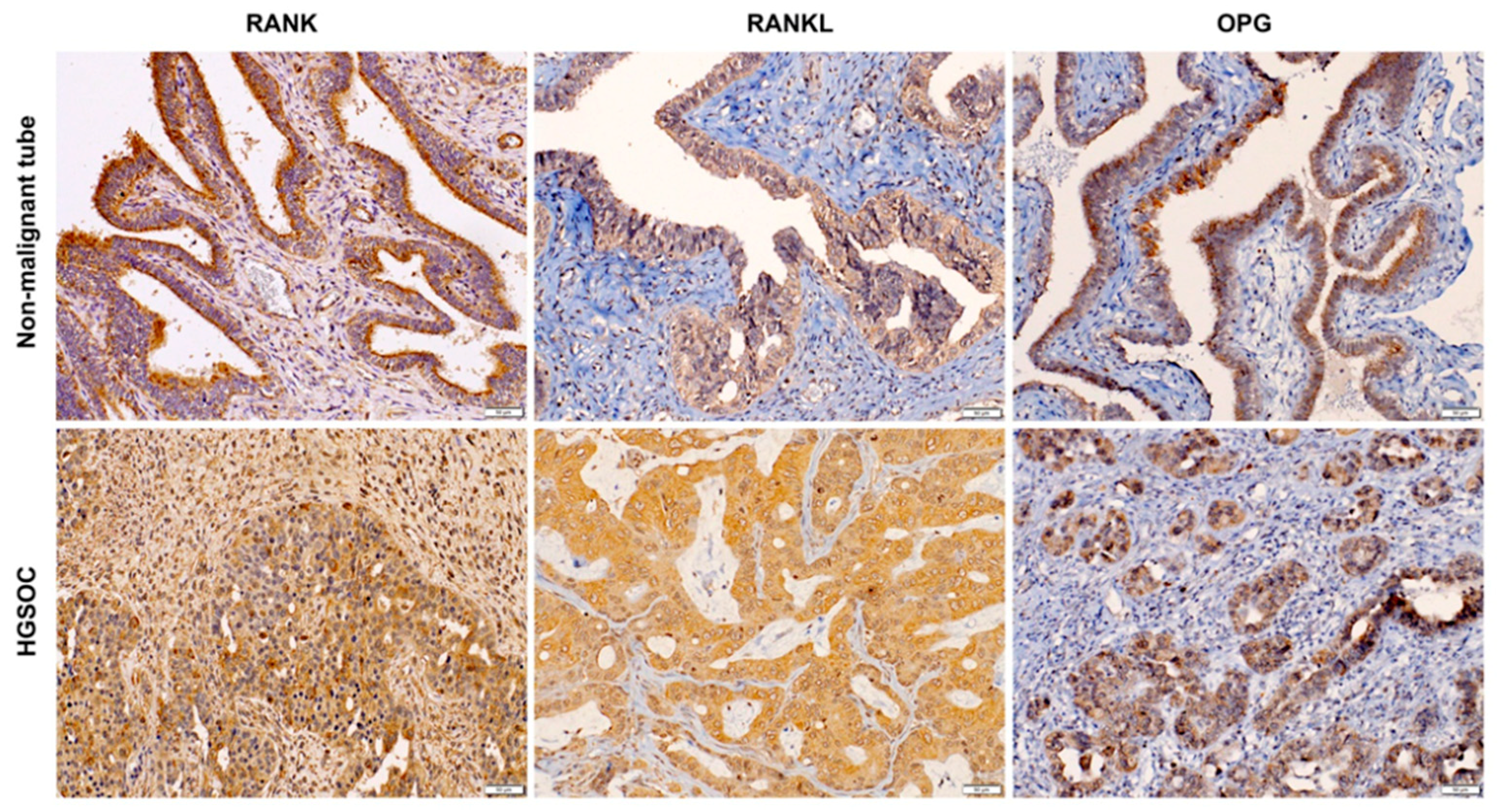
To elucidate the intratumour distribution of RANK, RANKL and OPG we randomly selected 20 OC tissues for immunohistochemistry. Epithelial cells and, to some extent, stromal cells expressed RANK, RANKL and OPG in healthy and diseased tissue (Figure 4, Supplementary Materials Table S2). Notably, non-malignant fallopian tubes expressed RANK, RANKL and OPG, which was pronounced in OC tissue (Figure 4). We did not find an association for semi-quantitative immunohistochemical RANK, RANKL and OPG expression patterns and clinicopathological characteristics and also tumour grade or histological subtype were not associated with a specific distribution pattern of RANK, RANKL or OPG expression. Additional representative images of IHC are shown in Supplementary Materials Figure S6.
2.5. Neither Stimulation with RANKL Nor Treatment with Denosmuab Affects OC Cell Proliferation
Similar to OC tissue, OC cell lines SKOV6, HOC7, HTB77, and OVCAR3 exhibited RANK, RANKL and OPG expression at baseline (Supplementary Materials Figure S7A–C). Expression of both, RANK and OPG, was induced in SKOV6 cells by inflammatory mediators such as IL-1β or TNFα but not mitogenic mediators such as IL-6 or LPA (Supplementary Materials Figure S7D,E). In contrast, RANKL expression was largely unaffected by cytokine stimulation (Supplementary Materials Figure S7F). Notably, progesterone did not impact on RANKL expression (Supplementary Materials Figure S7F), as previously demonstrated for breast cancer cells [18].
Considering the known effect of denosumab on cell proliferation in vitro [18,19] we next assessed whether pharmacological RANKL inhibition or stimulation with recombinant RANKL could directly influence cell proliferation of OC cells. Therefore, we treated OC cell lines with increasing concentrations of denosumab with or without cisplatin co-treatment. Denosumab did not affect the proliferation of OC cell lines OVCAR3 (Supplementary Materials Figure S8A–C), SKOV6 (Supplementary Materials Figure S8D–F) or HTB77 (Supplementary Materials Figure S8G–I) evaluated by MTT assays and by expression analyses of cell the cycle proteins G1/S-specific cyclin-E (CCNE) and transcription factor E2F3a (E2F3A). Furthermore, denosumab in combination with cisplatin did not have an additional effect on platinum-induced cytotoxicity in OVCAR3 (Supplementary Materials Figure S9A), SKOV6 (Supplementary Materials Figure S9B) and HTB77 cells (Supplementary Materials Figure S9C). Despite expression of RANK in OC cells, stimulation with recombinant RANKL did not affect cell proliferation (Supplementary Materials Figure S10A–D).
2.6. High CCND1 mRNA Expression is Associated with Poor Prognosis
To further investigate downstream signalling of RANK activation we performed correlation analysis between RANK and RANKL and mediators of either the NFκB pathway (CCND1) or the ID2 pathway (P21) [20] in the TCGA cohort. As we found a correlation between both RANK and RANKL, and CCND1 (Figure 5A,B) we performed Kaplan—Meier survival analysis according to high (>64th percentile) and low CCND1 (<64th percentile) expressions and demonstrate that high CCND1 is associated with reduced PFS (p = 0.208; Figure 5C) and OS (p = 0.013; Figure 5D). In contrast, we did not find a correlation between RANK/RANKL and P21 expression These data suggest that downstream RANKL mediator(s), specifically CCND1, contribute to poor clinical outcome in OC.
3. Discussion
In this study, we investigated the RANK/RANKL/OPG pathway in OC and its impact on clinical outcome in two unrelated OC cohorts. We found that RANK, RANKL and OPG were highly expressed in OC tissue which localized to tumour epithelium and to tumour stromal cells. Previous studies demonstrated that a high percentage of tumours such as breast, cervical, endometrial, colorectal, prostate cancer and malignant melanoma express RANK, and some of them also express RANKL [6,21,22,23].
As little is known about the prognostic impact of RANK and RANKL expression in OC, we analysed our cohort of 192 OC patients including various histologic types and validated our findings in an independent TCGA cohort comprising serous ovarian carcinomas. These studies demonstrate that high RANKL expression independently predicted poor clinical outcome defined by a shorter PFS and OS in a multivariate analysis. Considering different histologic subtypes included in our and the TCGA cohort, a subgroup analysis of HGSOC patients (n = 122) in our cohort revealed similar results (Figure S3) compared to the entire cohort including various histological subtypes. RANK and/or RANKL expression previously associated with poor clinical outcome in gastric cancer [24], acute myeloid leukaemia [25], breast cancer [26,27], (clear-cell) renal cell carcinoma [28,29], prostate cancer [30] and osteosarcoma [31].
RANK signalling is critically involved in BRCA-driven tumourigenesis in BC [11] and previous studies demonstrated that RANKL mediates proliferation of the mammary epithelium in mice [32] and humans [10]. Treatment of non-malignant human breast epithelial cells with denosumab significantly decreased the frequency of colony formation [19]. In line with previous findings in BC [11], we noted that RANKL expression was particularly elevated in BRCA1/2 mutated OC as compared to BRCA1/2 wild-type (wt) tumours. Future studies should investigate a functional role for RANK/RANKL/OPG signalling in DNA repair mechanisms to foster our biological understanding how RANK signalling impacts on the course of OC [33]. In this regard, we did not note that modulation of RANK signalling (by denosumab or recombinant RANK ligand) affect OC cell proliferation in four OC cell lines. As such, we speculate that OC-derived RANKL may modulate the tumour microenvironment and particularly tumour immune responses [7] which could involve stromal cells or infiltrating immune cells and an inflammatory OC environment [34,35,36].
In line with this, pro-inflammatory mediators such as IL-1β and TNFα induced RANK, and OPG expression in OC cell lines. As we observed a correlation between CCND1 and both, RANK and RANKL expression in the TCGA cohort and we noted an association between CCND1 and reduced OS, we speculate that NFkB activation may be a critical event downstream of RANK activation in OC. Moreover, RANKL acts as a chemoattractant to M2 macrophages and tumour cells [6,37] and the RANK pathway is involved in epithelial–mesenchymal transition (EMT) and stemness, and facilitates tumour growth and metastasis by modulating immune and vascular niches [38]. RANKL also up-regulates the angiogenic process by stimulating the proliferation and survival of endothelial cells [39,40] and may promote extravasation/intravasation of RANK-expressing cancer cells, as well as their migration to distant organs [38]. More recently, Khan et al. demonstrated that RANKL blockade can rescue melanoma-specific T cells from thymic deletion and, therefore, increases the anti-tumour immune response in melanoma [41]. These data suggest also a potential role of the RANK pathway in immune escape and immunotherapy which may become relevant in OC [42,43].
More precisely, immunotherapy for the treatment of OC is promising as previous studies demonstrated that the presence of tumour infiltrating lymphocytes (TILs) is associated with improved clinical outcome in OC patients [44,45]. Therapies targeting TILs in OC include immune checkpoint blockade, cancer vaccines, and adoptive cell therapy [43]. However, there are currently no approved immunotherapies for OC. Interestingly, short course of denosumab in the D-BEYOND study including premenopausal women with early BC significantly increased stromal TILs without reducing tumour proliferation rate (NCT01864798). These data are in line with our hypothesis that the RANK pathway may influence OC biology via immunomodulation. Notably, latest studies demonstrate that RANK signalling inhibition may improve the effectiveness of checkpoint blockade in cancer treatment [15]. Ahern et al. demonstrated that RANKL blockade improved the efficacy of anti-CTLA4 monoclonal antibodies against experimental solid tumours and experimental metastases [13]. Furthermore, Smyth et al. demonstrated that that a combination of natural killer cells and T cells are required for the antitumour activity of anti-CTLA-4 and anti-RANKL in mice [16]. A retrospective review by Afzal et al. demonstrated that the combination of immune checkpoint inhibitors and denosumab improved median PFS and OS malignant melanoma patients compared to checkpoint inhibitors alone [14]. In OC, checkpoint inhibitors have not been convincing as the observed response rates were low, however, improvements in therapeutic efficacy have been proposed through combination with PARPis and other immunostimulatory compounds. Considering that RANK inhibition was demonstrated to improve immune responses the combination of RANK inhibitors, e.g., denosumab, with checkpoint inhibitors may be worth to assess in clinical trials of OC and other gynaecological malignancies, such as cervical cancer, which was shown also to be of high expression of RANK and RANKL [46].
In BC, on the one hand RANK signalling (driven by progesterone) controls the onset of hormone-induced BC through the expansion of mammary progenitor cells and on the other hand, RANK and RANKL also critically regulate BRCA1-mutation-driven BC. The latter could be explained by the fact that common variations in the RANK gene modify the risk of developing BC in BRCA1-mutation carriers. Further, women carrying a germline BRCA1 mutation show high levels of progesterone and oestrogen during the luteal linking BRCA1 associated tumourigenesis to female sex hormones [20]. Considering that progesterone triggers massive induction of RANKL in mammary-gland epithelial cells, genetic inactivation of RANK prevents progestin-driven epithelial proliferation [10,32,47] and we detected progesterone receptors in our OC cohort (0–90% PR positive for IHC), we tested the “in vitro” impact of progesterone on RANKL expression in OC cell lines. However, progesterone treatment did not induce expression of RANKL/RANK/OPG. This is in contrast to findings in BC cells [10,32,47] and appears uncoupled from the observation that progesterone protects against OC [48].
OC is a clinically challenging cancer entity that requires intensive treatment combining surgery, chemotherapy and angiogenic inhibitors [49]. However, prognosis of OC patients remains devastating, which is why novel therapeutic options are eagerly awaited [2]. Denosumab is a neutralizing RANKL antibody that has been approved by the FDA for the treatment of osteoporosis. Moreover, denosumab is currently used to treat bone fractures of metastatic disease and RANKL inhibition has been extensively studied in preclinical tumour models [47] and is now proven as a preventive strategy for women carrying BRCA1 mutations and high risk of BC [20].
4. Materials and Methods
4.1. Patients and Samples
Ovarian tissue samples from 192 patients with OC obtained at primary debulking (patients were 24 to 90 years old; median age at diagnosis was 59.7 years) and control tissues from 35 patients obtained by elective salpingectomy or elective oophorectomy for benign conditions (i.e., salpingectomy for sterilization or contralateral salpingo-oophorectomy as part of surgery for benign cysts) (patients were 30.4 to 74.3 years old, median age: 51.0 years) were collected and processed at the Department of Obstetrics and Gynaecology of the Medical University of Innsbruck, Austria between 1989 and 2010 as described recently [42]. Written informed consent was obtained from all patients before enrolment. The study was reviewed and approved by the Ethics committee of the Medical University of Innsbruck (reference number: 1157/2018) and conducted in accordance with the Declaration of Helsinki. All samples were anonymized before the commencement of the analysis. All patients were monitored within the outpatient follow-up program of our department. Tumour specimens were analysed for somatic BRCA1/2 mutations as previously described [50]. The median observation period was 1.6 years (0.03–22 years) regarding PFS and 3.6 years (0.09–26.1 years) concerning the OS. All patients were of Caucasian ethnicity. Clinicopathological features are shown in Table 1.
4.2. RNA Isolation and Reverse Transcription
Total cellular RNA extraction from tissue samples and in vitro experiments and reverse transcription were performed as previously described [42]. Histologically, ~75% of the analysed tissue samples consisted of cancer cells (Table S2) did not correlate with RANK, RANKL and OPG expression (Table S3).
4.3. Quantitative Real Time PCR
Primers and probes for the TATA box-binding protein (TBP; endogenous RNA-control) were used according to Bieche et al. [51]. Primers and probes for RANK, RANKL and OPG were purchased from Applied Biosystems (Hs00921372_m1, Hs00243522_m1, Hs00900358_m1, Foster City, CA, USA). The following primer sequences were used for CCNE: for 5′ ACT TAA GGG CCT TCA TAA TCA TTA ATT C 3′, rev 5′ GCA GCC AAA CTT GAG GAA ATC TAT 3′, probe 5′ FAM-AGA ATT TCA TCT CCT GAA CAA GCT CCA TCT GTC-TAMRA 3′; and E2F3A: for 5′ TTT AAA CCA TCT GAG AGG TAC TGA TGA 3′, rev 5′ CGG CCC TCC GGC AA 3′, probe 5′ FAM-CGC TTT CTC CTA GCT CCA GCC TTC G_TAMRA 3′. PCR reactions were performed as previously described [42]. BRCA1 and BRCA2 mRNA expression was determined as previously described [50].
4.4. TCGA Cohort
Analyses were performed on The Cancer Genome Atlas (TCGA, National Cancer Institute, Bethesda, MD, USA) publicly available dataset. Eligible patients were those who were defined as having serous ovarian cystadenocarcinoma in the TCGA dataset and who had complete information on age at OC diagnosis, tumour grade, FIGO stage, survival, and had gene expression analyses available.
4.5. Immunohistochemistry
Immunohistochemistry was performed using an automated immunostainer (BenchMark ULTRA, Ventana Medical Systems, Tucson, AZ, USA). In short, formalin-fixed, paraffin-embedded (FFPE) tissue sections were prepared with cell conditioning reagent for antigen retrieval. Anti-SPATA2 antibody (Sigma-Aldrich, HPA048581, St. Louis, MO,) was incubated for 30 min at 37 °C and for visualization the Ultra View DAB Detection Kit (Ventana Medical Systems, Oro Valley, AZ, USA) was used as recommended. Slides were counterstained with haematoxylin and bluing reagent. Images were acquired with a Zeiss AxioCam (Oberkochen, Germany).
4.6. Culture and Treatment of OC Cells
OVCAR3, HOC7, SKOV6 and HTB77 human ovarian cancer cells were purchased from ATCC (Middlesex, UK) and cultured in RPMI supplemented with 10% foetal bovine serum and penicillin/streptomycin. We have performed the STR profiling in our lab in February 2018 before performing in vitro experiments and regularly performed Mycoplasma testing. Cells were treated with recombinant human IL-1β (10 ng/mL; Invivogen, San Diego, CA, USA), TNFα (25 ng/mL; Peprotech, Rocky Hill, NJ, USA), IL-6 (10 ng/mL; Peprotech, Rocky Hill, NJ, USA), LPA (20 μM; Sigma-Aldrich, St. Louis, MO, USA), progesterone (1 mg/mL; Proluton®, Sandoz, Holzkirchen, Germany), Denosumab (X-Geva®; Amgen, Thousand Oaks, CA, USA; 3 µg/mL, 30 µg/mL, 300 µg/mL), cisplatin (1–5 µg/mL, Sandoz, Holzkirchen, Germany), recombinant Human sRANK Ligand (Escherichia coli-derived; Peprotech, Rocky Hill, NJ, USA) for indicated time points.
4.7. MTT Assay
MTT assay was performed as previously described [52]. In short, MTT (10 mL/well, Sigma-Aldrich, St. Louis, MO, USA) was added to cell culture in 96 well plates after indicated timepoints and incubated for another 5 h. After the addition of 100 mL DMSO (Sigma-Aldrich, St. Louis, MO, USA), the extinction was measured photometrically (wavelength 550 nm).
4.8. Statistical Analysis
The non-parametric Mann–Whitney U test or Kruskal–Wallis test were applied to test for statistical significance between two groups or more than two groups, respectively. The correlations between RANK, RANKL, OPG, BRCA1 and BRCA2 mRNA expression were assessed by Spearman rank correlation analyses. PFS was defined as the time from diagnosis of the primary of tumour to the histopathological confirmation of recurrence or metastases or death from any cause and OS as the time from diagnosis of the primary of tumour to death from any cause. Patients were censored at the date of their last personal contact. Univariate Kaplan—Meier analyses and multivariable Cox survival analyses were used to explore the association of RANK, RANKL and OPG expression with PFS and OS (the p-value cut-off for inclusion to the multivariable Cox analysis was 0.2). For survival analyses, patients were dichotomized into low and high mRNA expression level groups by the optimal cut-off expression value calculated by the Youden Index [17]. Thereby, the cut-off was set at the 25th percentile for RANK, the 92nd percentile for OPG, and the 62nd percentile for RANKL which was further applied for the TCGA cohort. Experiments with more than two comparisons were tested for statistical significance by one-way ANOVA. p-values less than 0.05 were considered as statistically significant. Statistical analysis was performed using SPSS statistical software (version 20.0.0; SPSS Inc., Chicago, IL, USA).
5. Conclusions
RANKL expression is elevated in OC and independently predicts poor clinical outcome in two unrelated cohorts proposing a significant role of RANK signalling in the immunopathogenesis of OC. This clinical observation suggests that denosumab may be of therapeutic use in OC, although we acknowledge that further mechanistic studies about the role of RANK signalling in OC are warranted.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6694/11/6/791/s1; Table S1: Association of RANK, RANKL and OPG mRNA expression with clinicopathological features in OC patients, Table S2: IHC scoring of RANKL, RANK and OPG regarding their distribution to intra-tumour epithelial and stromal cells, Table S3: Spearman correlation analysis of tumour purity on IHC samples and RNA expression of RANK, RANKL and OPG (n = 20), Figure S1: RANK, RANKL and OPG mRNA expression levels in OC, BRCA1/2 mutated OC and correlation analyses, Figure S2: High RANKL mRNA expressions are associated with worse PFS and OS in the subgroup of patients with BRCA1/2 wildtype tumours (n = 146), Figure S3: RANKL expressions are elevated in HGSOC compared to non-malignant ovaries and Fallopian tubes and associated with worse PFS and OS in the subgroup of HGSOC patients, Figure S4: Kaplan—Meier survival analyses of OPG mRNA-expression in OC patients, Figure S5: Kaplan—Meier survival analyses of RANKL mRNA-expression with optimal cut-offs determined in the TCGA cohort, Figure S6: RANK, RANKL and OPG localize to cancer cells and tumour microenvironment in OC; Figure S7: RANK/RANKL/OPG are expressed in the human OC cell lines HOC7, SKOV6, HTB77 and OVCAR3 whereas RANK and OPG can be induced by inflammatory stimuli in OC cell lines, Figure S8: Blocking RANK/RANKL signalling using denosumab influenced neither OC cell viability nor cell cycle regulation, Figure S9: Blocking RANK/RANKL signalling using denosumab did not influence platinum-induced OC cell toxicity; Figure S10: Recombinant RANKL did not influence platinum-induced OC viability.
Author Contributions
Conceptualization: V.W.; data curation: V.W., S.S., I.T. and H.H.; formal analysis: V.W., S.S., I.T. and H.H.; funding acquisition: C.M. and A.G.Z.; investigation: V.W., S.S. and I.T.; methodology: V.W., S.S. and H.F.; project administration: V.W. and A.G.Z.; resources: J.H., H.H., H.F., C.M. and A.G.Z.; software: V.W., H.H. and H.F.; supervision: H.F., C.M. and A.G.Z.; validation: H.F.; visualization: V.W. and S.S.; writing—original draft: V.W.; writing—review and editing: S.S., I.T., J.H., H.F., C.M. and A.G.Z.
Funding
The project was supported by the Verein zur Krebsforschung in der Frauenheilkunde, an association which is exclusively financed by donation funds for cancer research in female malignancies.
Acknowledgments
We thank Christian Höpperger (Institute of Pathology, Medical University of Innsbruck) for his excellent technical assistance and Georg Goebel (Department of Medical Statistics, Informatics and Health Economics, Medical University of Innsbruck) for his statistical support.
Conflicts of Interest
The authors declare no potential conflicts of interest.
References
- Cannistra, S.A. Cancer of the ovary. N. Engl. J. Med. 2004, 351, 2519–2529. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, L.A.; Huang, B.; Miller, R.W.; Tucker, T.; Goodrich, S.T.; Podzielinski, I.; DeSimone, C.P.; Ueland, F.R.; van Nagell, J.R.; Seamon, L.G. Ten-year relative survival for epithelial ovarian cancer. Obstet. Gynecol. 2012, 120, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Nakashima, T.; Hiroshi, N.; Penninger, J.M. RANKL-RANK signaling in osteoclastogenesis and bone disease. Trends Mol. Med. 2006, 12, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Simonet, W.S.; Lacey, D.L.; Dunstan, C.R.; Kelley, M.; Chang, M.S.; Luthy, R.; Nguyen, H.Q.; Wooden, S.; Bennett, L.; Boone, T.; et al. Osteoprotegerin: a novel secreted protein involved in the regulation of bone density. Cell 1997, 89, 309–319. [Google Scholar] [CrossRef]
- Walsh, M.C.; Choi, Y. Biology of the RANKL-RANK-OPG System in Immunity, Bone, and Beyond. Front. Immunol. 2014, 5, 511. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.H.; Nakashima, T.; Sanchez, O.H.; Kozieradzki, I.; Komarova, S.V.; Sarosi, I.; Morony, S.; Rubin, E.; Sarao, R.; Hojilla, C.V.; et al. Regulation of cancer cell migration and bone metastasis by RANKL. Nature 2006, 440, 692–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, M.L.; Fong, L. Effects of RANKL-Targeted Therapy in Immunity and Cancer. Front. Oncol. 2014, 3, 329. [Google Scholar] [CrossRef] [PubMed]
- Eghbali-Fatourechi, G.; Khosla, S.; Sanyal, A.; Boyle, W.J.; Lacey, D.L.; Riggs, B.L. Role of RANK ligand in mediating increased bone resorption in early postmenopausal women. J. Clin. Invest. 2003, 111, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Wang, J.; Gupta, A.; Shidfar, A.; Branstetter, D.; Lee, O.; Ivancic, D.; Sullivan, M.; Chatterton, R.T., Jr.; Dougall, W.C.; et al. RANKL expression in normal and malignant breast tissue responds to progesterone and is up-regulated during the luteal phase. Breast Cancer Res. Treat. 2014, 146, 515–523. [Google Scholar] [CrossRef]
- Tanos, T.; Sflomos, G.; Echeverria, P.C.; Ayyanan, A.; Gutierrez, M.; Delaloye, J.F.; Raffoul, W.; Fiche, M.; Dougall, W.; Schneider, P.; et al. Progesterone/RANKL is a major regulatory axis in the human breast. Sci. Transl. Med. 2013, 5, 182ra155. [Google Scholar] [CrossRef]
- Sigl, V.; Owusu-Boaitey, K.; Joshi, P.A.; Kavirayani, A.; Wirnsberger, G.; Novatchkova, M.; Kozieradzki, I.; Schramek, D.; Edokobi, N.; Hersl, J.; et al. RANKL/RANK control Brca1 mutation. Cell Res. 2016, 26, 761–774. [Google Scholar] [CrossRef] [PubMed]
- Longacre, M.; Snyder, N.A.; Housman, G.; Leary, M.; Lapinska, K.; Heerboth, S.; Willbanks, A.; Sarkar, S. A Comparative Analysis of Genetic and Epigenetic Events of Breast and Ovarian Cancer Related to Tumorigenesis. Int. J. Mol. Sci. 2016, 17, 759. [Google Scholar] [CrossRef] [PubMed]
- Ahern, E.; Harjunpaa, H.; Barkauskas, D.; Allen, S.; Takeda, K.; Yagita, H.; Wyld, D.; Dougall, W.C.; Teng, M.W.L.; Smyth, M.J. Co-administration of RANKL and CTLA4 Antibodies Enhances Lymphocyte-Mediated Antitumor Immunity in Mice. Clin. Cancer. Res. 2017, 23, 5789–5801. [Google Scholar] [CrossRef] [PubMed]
- Afzal, M.Z.; Shirai, K. Immune checkpoint inhibitor (anti-CTLA-4, anti-PD-1) therapy alone versus immune checkpoint inhibitor (anti-CTLA-4, anti-PD-1) therapy in combination with anti-RANKL denosumuab in malignant melanoma: a retrospective analysis at a tertiary care center. Melanoma Res. 2018, 28, 341–347. [Google Scholar] [CrossRef] [PubMed]
- van Dam, P.A.; Verhoeven, Y.; Trinh, X.B.; Wouters, A.; Lardon, F.; Prenen, H.; Smits, E.; Baldewijns, M.; Lammens, M. RANK/RANKL signaling inhibition may improve the effectiveness of checkpoint blockade in cancer treatment. Crit. Rev. Oncol. Hematol. 2019, 133, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Smyth, M.J.; Yagita, H.; McArthur, G.A. Combination Anti-CTLA-4 and Anti-RANKL in Metastatic Melanoma. J. Clin. Oncol. 2016, 34, e104–e106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Schramek, D.; Leibbrandt, A.; Sigl, V.; Kenner, L.; Pospisilik, J.A.; Lee, H.J.; Hanada, R.; Joshi, P.A.; Aliprantis, A.; Glimcher, L.; et al. Osteoclast differentiation factor RANKL controls development of progestin-driven mammary cancer. Nature 2010, 468, 98–102. [Google Scholar] [CrossRef] [Green Version]
- Kondegowda, N.G.; Fenutria, R.; Pollack, I.R.; Orthofer, M.; Garcia-Ocana, A.; Penninger, J.M.; Vasavada, R.C. Osteoprotegerin and Denosumab Stimulate Human Beta Cell Proliferation through Inhibition of the Receptor Activator of NF-kappaB Ligand Pathway. Cell Metab. 2015, 22, 77–85. [Google Scholar] [CrossRef]
- Sigl, V.; Jones, L.P.; Penninger, J.M. RANKL/RANK: from bone loss to the prevention of breast cancer. Open Biol. 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Santini, D.; Perrone, G.; Roato, I.; Godio, L.; Pantano, F.; Grasso, D.; Russo, A.; Vincenzi, B.; Fratto, M.E.; Sabbatini, R.; et al. Expression pattern of receptor activator of NFkappaB (RANK) in a series of primary solid tumors and related bone metastases. J. Cell. Physiol. 2011, 226, 780–784. [Google Scholar] [CrossRef]
- Santini, D.; Schiavon, G.; Vincenzi, B.; Gaeta, L.; Pantano, F.; Russo, A.; Ortega, C.; Porta, C.; Galluzzo, S.; Armento, G.; et al. Receptor activator of NF-kB (RANK) expression in primary tumors associates with bone metastasis occurrence in breast cancer patients. PLoS ONE 2011, 6, e19234. [Google Scholar] [CrossRef]
- Bhatia, P.; Sanders, M.M.; Hansen, M.F. Expression of receptor activator of nuclear factor-kappaB is inversely correlated with metastatic phenotype in breast carcinoma. Clin. Cancer Res. 2005, 11, 162–165. [Google Scholar]
- Zhang, X.; Song, Y.; Song, N.; Zhang, L.; Wang, Y.; Li, D.; Wang, Z.; Qu, X.; Liu, Y. Rankl expression predicts poor prognosis in gastric cancer patients: results from a retrospective and single-center analysis. Braz. J. Med. Biol. Res. 2018, 51, e6265. [Google Scholar] [CrossRef] [Green Version]
- Schmohl, J.U.; Nuebling, T.; Wild, J.; Kroell, T.; Kanz, L.; Salih, H.R.; Schmetzer, H. Expression of RANK-L and in part of PD-1 on blasts in patients with acute myeloid leukemia correlates with prognosis. Eur. J. Haematol. 2016, 97, 517–527. [Google Scholar] [CrossRef]
- Vidula, N.; Yau, C.; Li, J.; Esserman, L.J.; Rugo, H.S. Receptor activator of nuclear factor kappa B (RANK) expression in primary breast cancer correlates with recurrence-free survival and development of bone metastases in I-SPY1 (CALGB 150007/150012; ACRIN 6657). Breast Cancer Res. Treat. 2017, 165, 129–138. [Google Scholar] [CrossRef]
- Pfitzner, B.M.; Branstetter, D.; Loibl, S.; Denkert, C.; Lederer, B.; Schmitt, W.D.; Dombrowski, F.; Werner, M.; Rudiger, T.; Dougall, W.C.; et al. RANK expression as a prognostic and predictive marker in breast cancer. Breast Cancer Res. Treat. 2014, 145, 307–315. [Google Scholar] [CrossRef]
- Beuselinck, B.; Jean-Baptiste, J.; Couchy, G.; Job, S.; De Reynies, A.; Wolter, P.; Theodore, C.; Gravis, G.; Rousseau, B.; Albiges, L.; et al. RANK/OPG ratio of expression in primary clear-cell renal cell carcinoma is associated with bone metastasis and prognosis in patients treated with anti-VEGFR-TKIs. Br. J. Cancer 2015, 113, 1313–1322. [Google Scholar] [CrossRef] [Green Version]
- Mikami, S.; Katsube, K.; Oya, M.; Ishida, M.; Kosaka, T.; Mizuno, R.; Mochizuki, S.; Ikeda, T.; Mukai, M.; Okada, Y. Increased RANKL expression is related to tumour migration and metastasis of renal cell carcinomas. J. Pathol. 2009, 218, 530–539. [Google Scholar] [CrossRef]
- Chen, G.; Sircar, K.; Aprikian, A.; Potti, A.; Goltzman, D.; Rabbani, S.A. Expression of RANKL/RANK/OPG in primary and metastatic human prostate cancer as markers of disease stage and functional regulation. Cancer 2006, 107, 289–298. [Google Scholar] [CrossRef]
- Bago-Horvath, Z.; Schmid, K.; Rossler, F.; Nagy-Bojarszky, K.; Funovics, P.; Sulzbacher, I. Impact of RANK signalling on survival and chemotherapy response in osteosarcoma. Pathology 2014, 46, 411–415. [Google Scholar] [CrossRef]
- Beleut, M.; Rajaram, R.D.; Caikovski, M.; Ayyanan, A.; Germano, D.; Choi, Y.; Schneider, P.; Brisken, C. Two distinct mechanisms underlie progesterone-induced proliferation in the mammary gland. Proc. Natl. Acad Sci. USA 2010, 107, 2989–2994. [Google Scholar] [CrossRef] [Green Version]
- Moynahan, M.E.; Pierce, A.J.; Jasin, M. BRCA2 is required for homology-directed repair of chromosomal breaks. Mol. Cell. 2001, 7, 263–272. [Google Scholar] [CrossRef]
- Maccio, A.; Madeddu, C. Inflammation and ovarian cancer. Cytokine 2012, 58, 133–147. [Google Scholar] [CrossRef] [Green Version]
- Volgger, B.M.; Windbichler, G.H.; Zeimet, A.G.; Graf, A.H.; Bogner, G.; Angleitner-Boubenizek, L.; Rohde, M.; Denison, U.; Sliutz, G.; Fuith, L.C.; et al. Long-term significance of urinary neopterin in ovarian cancer: a study by the Austrian Association for Gynecologic Oncology (AGO). Ann. Oncol. 2016, 27, 1740–1746. [Google Scholar] [CrossRef]
- White, K.L.; Schildkraut, J.M.; Palmieri, R.T.; Iversen, E.S., Jr.; Berchuck, A.; Vierkant, R.A.; Rider, D.N.; Charbonneau, B.; Cicek, M.S.; Sutphen, R.; et al. Ovarian cancer risk associated with inherited inflammation-related variants. Cancer Res. 2012, 72, 1064–1069. [Google Scholar] [CrossRef]
- Chawla, S.; Henshaw, R.; Seeger, L.; Choy, E.; Blay, J.Y.; Ferrari, S.; Kroep, J.; Grimer, R.; Reichardt, P.; Rutkowski, P.; et al. Safety and efficacy of denosumab for adults and skeletally mature adolescents with giant cell tumour of bone: interim analysis of an open-label, parallel-group, phase 2 study. Lancet Oncol. 2013, 14, 901–908. [Google Scholar] [CrossRef]
- Palafox, M.; Ferrer, I.; Pellegrini, P.; Vila, S.; Hernandez-Ortega, S.; Urruticoechea, A.; Climent, F.; Soler, M.T.; Munoz, P.; Vinals, F.; et al. RANK induces epithelial-mesenchymal transition and stemness in human mammary epithelial cells and promotes tumorigenesis and metastasis. Cancer Res. 2012, 72, 2879–2888. [Google Scholar] [CrossRef]
- Min, J.K.; Kim, Y.M.; Kim, Y.M.; Kim, E.C.; Gho, Y.S.; Kang, I.J.; Lee, S.Y.; Kong, Y.Y.; Kwon, Y.G. Vascular endothelial growth factor up-regulates expression of receptor activator of NF-kappa B (RANK) in endothelial cells. Concomitant increase of angiogenic responses to RANK ligand. J. Biol. Chem. 2003, 278, 39548–39557. [Google Scholar] [CrossRef]
- Kim, H.H.; Shin, H.S.; Kwak, H.J.; Ahn, K.Y.; Kim, J.H.; Lee, H.J.; Lee, M.S.; Lee, Z.H.; Koh, G.Y. RANKL regulates endothelial cell survival through the phosphatidylinositol 3′-kinase/Akt signal transduction pathway. FASEB J. 2003, 17, 2163–2165. [Google Scholar] [CrossRef]
- Khan, I.S.; Mouchess, M.L.; Zhu, M.L.; Conley, B.; Fasano, K.J.; Hou, Y.; Fong, L.; Su, M.A.; Anderson, M.S. Enhancement of an anti-tumor immune response by transient blockade of central T cell tolerance. J. Exp. Med. 2014, 211, 761–768. [Google Scholar] [CrossRef]
- Wieser, V.; Gaugg, I.; Fleischer, M.; Shivalingaiah, G.; Wenzel, S.; Sprung, S.; Lax, S.F.; Zeimet, A.G.; Fiegl, H.; Marth, C. BRCA1/2 and TP53 mutation status associates with PD-1 and PD-L1 expression in ovarian cancer. Oncotarget 2018, 9, 17501–17511. [Google Scholar] [CrossRef]
- Marth, C.; Wieser, V.; Tsibulak, I.; Zeimet, A.G. Immunotherapy in ovarian cancer: fake news or the real deal? Int. J. Gynecol. Cancer 2019, 29, 201–211. [Google Scholar] [CrossRef]
- Odunsi, K. Immunotherapy in ovarian cancer. Ann. Oncol. 2017, 28, viii1–viii7. [Google Scholar] [CrossRef]
- Sato, E.; Olson, S.H.; Ahn, J.; Bundy, B.; Nishikawa, H.; Qian, F.; Jungbluth, A.A.; Frosina, D.; Gnjatic, S.; Ambrosone, C.; et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc. Natl. Acad. Sci. USA. 2005, 102, 18538–18543. [Google Scholar] [CrossRef]
- van Dam, P.A.; Verhoeven, Y.; Jacobs, J.; Wouters, A.; Tjalma, W.; Lardon, F.; Van den Wyngaert, T.; Dewulf, J.; Smits, E.; Colpaert, C.; et al. RANK-RANKL Signaling in Cancer of the Uterine Cervix: A Review. Int. J. Mol. Sci. 2019, 20, 2183. [Google Scholar] [CrossRef]
- de Groot, A.F.; Appelman-Dijkstra, N.M.; van der Burg, S.H.; Kroep, J.R. The anti-tumor effect of RANKL inhibition in malignant solid tumors-A systematic review. Cancer Treat. Rev. 2018, 62, 18–28. [Google Scholar] [CrossRef]
- Wu, N.Y.; Huang, H.S.; Chao, T.H.; Chou, H.M.; Fang, C.; Qin, C.Z.; Lin, C.Y.; Chu, T.Y.; Zhou, H.H. Progesterone Prevents High-Grade Serous Ovarian Cancer by Inducing Necroptosis of p53-Defective Fallopian Tube Epithelial Cells. Cell Rep. 2017, 18, 2557–2565. [Google Scholar] [CrossRef]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef]
- Tsibulak, I.; Wieser, V.; Degasper, C.; Shivalingaiah, G.; Wenzel, S.; Sprung, S.; Lax, S.F.; Marth, C.; Fiegl, H.; Zeimet, A.G. BRCA1 and BRCA2 mRNA-expression prove to be of clinical impact in ovarian cancer. Br. J. Cancer 2018, 119, 683–692. [Google Scholar] [CrossRef] [Green Version]
- Bieche, I.; Franc, B.; Vidaud, D.; Vidaud, M.; Lidereau, R. Analyses of MYC, ERBB2, and CCND1 genes in benign and malignant thyroid follicular cell tumors by real-time polymerase chain reaction. Thyroid 2001, 11, 147–152. [Google Scholar] [CrossRef]
- Wieser, V.; Adolph, T.E.; Enrich, B.; Kuliopulos, A.; Kaser, A.; Tilg, H.; Kaneider, N.C. Reversal of murine alcoholic steatohepatitis by pepducin-based functional blockade of interleukin-8 receptors. Gut 2017, 66, 930–938. [Google Scholar] [CrossRef]
Figure 1.
RANK, RANKL and OPG mRNA expressions are elevated in OC tissue, particularly in BRCA1/2 mutated OC. (A) RANKL, (B) OPG and (C) RANK expression in non-malignant ovaries (n = 21), non-malignant fallopian tubes (n = 14) and OC (n = 192). (D) RANKL mRNA expression in BRCA1/2 mutated (mut) OC (n = 44) compared to BRCA1/2 wild-type (wt) tumours (n = 146). RANK, RANKL and OPG mRNA expression values were normalized to TBP expression, n.s., not significant.
Figure 1.
RANK, RANKL and OPG mRNA expressions are elevated in OC tissue, particularly in BRCA1/2 mutated OC. (A) RANKL, (B) OPG and (C) RANK expression in non-malignant ovaries (n = 21), non-malignant fallopian tubes (n = 14) and OC (n = 192). (D) RANKL mRNA expression in BRCA1/2 mutated (mut) OC (n = 44) compared to BRCA1/2 wild-type (wt) tumours (n = 146). RANK, RANKL and OPG mRNA expression values were normalized to TBP expression, n.s., not significant.

Figure 2.
High RANK and RANKL mRNA expressions are associated with worse PFS and OS in OC. RANKL mRNA expression (n = 192) and (A) progression free survival and (B) overall survival. RANK mRNA expression (n = 192) and (C) progression free survival and (D) overall survival. RANK and RANKL mRNA expression values were normalized to TBP expression.
Figure 2.
High RANK and RANKL mRNA expressions are associated with worse PFS and OS in OC. RANKL mRNA expression (n = 192) and (A) progression free survival and (B) overall survival. RANK mRNA expression (n = 192) and (C) progression free survival and (D) overall survival. RANK and RANKL mRNA expression values were normalized to TBP expression.

Figure 3.
Validation of the prognostic impact of RANKL in the TCGA dataset. RANKL mRNA expression (n = 563) and (A) progression free survival and (B) overall survival.
Figure 3.
Validation of the prognostic impact of RANKL in the TCGA dataset. RANKL mRNA expression (n = 563) and (A) progression free survival and (B) overall survival.

Figure 4.
RANK, RANKL and OPG localize to cancer cells and tumour microenvironment in OC. Representative RANK, RANKL and OPG immunohistochemistry on FFPE sections from non-malignant tubes and HGSOC. n = 8–10 (per target); Scale bars indicate 50 µm.
Figure 4.
RANK, RANKL and OPG localize to cancer cells and tumour microenvironment in OC. Representative RANK, RANKL and OPG immunohistochemistry on FFPE sections from non-malignant tubes and HGSOC. n = 8–10 (per target); Scale bars indicate 50 µm.

Figure 5.
RANK/RANKL correlate with CCND1 which is associated with clinical outcome in the TCGA cohort. Linear regression analysis of (A) RANKL and CCND1, (B) RANK and CCND1 in tumour tissue of OC patients (n = 563). CCND1 (n = 563) and (C) progression free survival and (D) overall survival.
Figure 5.
RANK/RANKL correlate with CCND1 which is associated with clinical outcome in the TCGA cohort. Linear regression analysis of (A) RANKL and CCND1, (B) RANK and CCND1 in tumour tissue of OC patients (n = 563). CCND1 (n = 563) and (C) progression free survival and (D) overall survival.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Univariate and multivariate survival analysis in 192 ovarian cancer patients. RANK/RANKL/OPG cut-off was determined by the Youden Index.
Table 1.
Univariate and multivariate survival analysis in 192 ovarian cancer patients. RANK/RANKL/OPG cut-off was determined by the Youden Index.
| Univariate Survival Analysis in 192 Ovarian Cancer Patients | |||||||
| Variable | Progression Free Survival | Overall Survival | |||||
| No. Patients | Median, Years | p Value | No. Patients | Median, Years | p Value | ||
| (Relapsed/Total) | (95% CI) | (Died/Total) | (95% CI) | ||||
| Age (median) | ≤50.0 yrs. | 21/32 | 2.13 (4.03–9.17) | 0.762 | 15/32 | 9.15 (9.49–17.69) | 0.019 |
| >50.0 yrs. | 92/160 | 2.00 (6.71–10.11) | 105/160 | 3.9 (7.00–10.04) | |||
| FIGO stage | I/II | 10/50 | n.r. (13.63–18.83) | <0.001 | 18/50 | n.r. (12.23–18.08) | <0.001 |
| III/IV | 103/142 | 1.47 (4.03–6.95) | 102/142 | 3.80 (6.07–9.26) | |||
| Tumour grade | 1–2 | 54/99 | 2.06 (6.98–11.34) | 0.249 | 57/99 | 6.76 (9.09–13.78) | 0.07 |
| 3 | 57/91 | 1.98 (5.14–9.00) | 61/91 | 3.71 (5.57–8.92) | |||
| Residual disease after surgery | no | 38/96 | n.r. (10.54–15.10) | <0.001 | 35/96 | n.r. (11.98–16.49) | <0.001 |
| yes | 71/90 | 1.25 (2.25–5.02) | 81/90 | 2.55 (3.74–6.62) | |||
| Histology | HGSOC | 81/122 | 1.81 (4.28–7.41) | 0.003 | 88/122 | 3.70 (6.04–9.57) | 0.001 |
| others | 30/66 | 5.98 (9.31–14.68) | 29/66 | 11.06 (10.31–15.68) | |||
| RANKL mRNA expression | low | 58/115 | 3.56 (1.81–5.31) | 0.01 | 62/115 | 8.76 (5.98–11.55) | 0.005 |
| high | 55/77 | 1.68 (1.21–2.16) | 58/77 | 3.62 (2.51–4.74) | |||
| RANK mRNA expression | low | 24/48 | 3.56 (0.89–6.24) | 0.117 | 26/48 | 9.27 (1.97–16.56) | 0.03 |
| high | 89/144 | 1.97 (1.54–2.40 | 94/144 | 3.71 (1.85–5.57) | |||
| OPG mRNA expression | low | 101/177 | 2.06 (1.33–2.80) | 0.135 | 107/177 | 5.80 (3.94–7.66) | 0.154 |
| high | 12/15 | 1.46 (1.16–1.76) | 13/15 | 3.29 (1.87–4.70) | |||
| Note: The significance level (p) was determined by log-rank test. RANK/RANKL/OPG cut-off was determined by the Youden Index. Abbreviations: CI, confidence interval; HGSOC, high grade serous ovarian cancer; n.r., not reached. | |||||||
| Multivariate Survival Analysis in 192 Ovarian Cancer Patients | |||||||
| Variable | Progression Free Survival | Overall Survival | |||||
| RR | (95 CI) | p Value | RR | (95 CI) | p Value | ||
| Age | ≤50.0 yrs > | 1.19 | (0.73–1.96) | 0.489 | 1.54 | (0.87–2.75) | 0.134 |
| FIGO stage | I/II vs. III/IV | 3.57 | (1.76–7.27) | <0.001 | 1.05 | (0.58–1.90) | 0.872 |
| Tumour grade | 1/2 vs. 3 | 1.09 | (0.73–1.62) | 0.682 | 1.08 | (0.73–1.58) | 0.705 |
| Residual disease after surgery | no vs. Yes | 2.01 | (1.28–3.17) | 0.003 | 4.96 | (1.78–4.62) | <0.001 |
| Histology | HGSOC vs. others | 0.87 | (0.55–1.36) | 0.533 | 0.72 | (0.46–1.12) | 0.14 |
| RANKL mRNA expression | low vs. high | 1.42 | (0.97–2.10) | 0.017 | 1.7 | (1.16–2.50) | 0.007 |
| RANK mRNA expression | low vs. high | 1.19 | (0.72–1.96) | 0.502 | 1.36 | (0.85–2.19) | 0.202 |
| OPG mRNA expression | low vs. high | 1.11 | (0.59–2.07) | 0.749 | 1.25 | (0.68–2.29) | 0.466 |
| Note: The significance level (p) was determined by Cox regression. RANK/RANKL/OPG cut-off was determined by the Youden Index. Abbreviations: CI, confidence interval; HGSOC, high grade serous ovarian cancer; RR, relative risk. | |||||||
Table 2.
Multivariate survival analysis in 514 ovarian cancer patients from the TCGA Affymetrix dataset.
Table 2.
Multivariate survival analysis in 514 ovarian cancer patients from the TCGA Affymetrix dataset.
| Variable | Progression Free Survival | Overall Survival | |||||
|---|---|---|---|---|---|---|---|
| RR | (95 CI) | p Value | RR | (95 CI) | p Value | ||
| Age | ≤ 50.0 yrs > | 0.93 | (0.83–1.05) | 0.252 | 1.02 | (0.95–1.11) | 0.541 |
| FIGO stage | I/II vs. III/IV | 2.02 | (1.38–2.97) | <0.001 | 1.14 | (0.10–1.31) | 0.060 |
| Tumour grade | 1/2 vs. 3 | 0.98 | (0.89–1.09) | 0.755 | 1.02 | (0.94–1.11) | 0.621 |
| Residual disease after surgery | no vs. Yes | 1.07 | (0.96–1.20) | 0.204 | 1.02 | (0.92–1.14) | 0.710 |
| RANKL mRNA expression | low vs. high | 1.32 | (1.04–1.68) | 0.022 | 1.26 | (1.00–1.57) | 0.046 |
| Note: The significance level (p) was determined by Cox regression. Abbreviations: CI, confidence interval; RR, relative risk. | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wieser, V.; Sprung, S.; Tsibulak, I.; Haybaeck, J.; Hackl, H.; Fiegl, H.; Marth, C.; Zeimet, A.G. Clinical Impact of RANK Signalling in Ovarian Cancer. Cancers 2019, 11, 791. https://doi.org/10.3390/cancers11060791
AMA Style
Wieser V, Sprung S, Tsibulak I, Haybaeck J, Hackl H, Fiegl H, Marth C, Zeimet AG. Clinical Impact of RANK Signalling in Ovarian Cancer. Cancers. 2019; 11(6):791. https://doi.org/10.3390/cancers11060791
Chicago/Turabian StyleWieser, Verena, Susanne Sprung, Irina Tsibulak, Johannes Haybaeck, Hubert Hackl, Heidelinde Fiegl, Christian Marth, and Alain Gustave Zeimet. 2019. "Clinical Impact of RANK Signalling in Ovarian Cancer" Cancers 11, no. 6: 791. https://doi.org/10.3390/cancers11060791
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.