Molecular Genetics of Renal Cell Tumors: A Practical Diagnostic Approach


1
Department of Pathology, Faculty of Medicine, University of British Columbia, Royal Columbian Hospital, Vancouver, BC V3E 0G9, Canada
2
Department of Pathology, Institute Nacional de Cancerologia, INCAN, Mexico DF 14080, Mexico
3
Department of Pathology, Centro Hospitalar de Vila Nova de Gaia-Espinho, Vila Nova de Gaia, Cancer Biology and Epigenetics Group (CBEG), IPO Porto Research Center (CI-IPOP), Portuguese Oncology Institute of Porto (IPO Porto) & Porto Comprehensive Cancer Center (P.CCC), 4200-072 Porto, Portugal
4
Department of Microscopy, Institute of Biomedical Sciences Abel Salazar, University of Porto (ICBAS-UP), 4200-072 Porto, Portugal
5
Department of Pathology, Charles University in Prague, Faculty of Medicine in Plzen, 304 60 Pilsen, Czech Republic
*
Author to whom correspondence should be addressed.
Cancers 2020, 12(1), 85; https://doi.org/10.3390/cancers12010085
Submission received: 1 December 2019
/
Revised: 20 December 2019
/
Accepted: 23 December 2019
/
Published: 30 December 2019
(This article belongs to the Special Issue Renal Cell Carcinoma)
Abstract
:Renal epithelial cell tumors are composed of a heterogeneous group of tumors with variable morphologic, immunohistochemical, and molecular features. A “histo-molecular” approach is now an integral part of defining renal tumors, aiming to be clinically and therapeutically pertinent. Most renal epithelial tumors including the new and emerging entities have distinct molecular and genetic features which can be detected using various methods. Most renal epithelial tumors can be diagnosed easily based on pure histologic findings with or without immunohistochemical examination. Furthermore, molecular-genetic testing can be utilized to assist in arriving at an accurate diagnosis. In this review, we presented the most current knowledge concerning molecular-genetic aspects of renal epithelial neoplasms, which potentially can be used in daily diagnostic practice.
1. Introduction
Renal cell tumors are one of the most extensively studied human neoplasms. A number of morphologic, immunohistochemical and molecular genetic features were described during the last 20 years, which have also led to recognition of new entities, expanding our knowledge and understanding of renal tumors.
“The Heidelberg classification of renal cell tumors” published in 1997 was the first classification integrating molecular genetic features as one of the diagnostic tools applicable to renal cell tumors [1]. This classification was further corroborated by the so-called UICC Rochester Classification [2], which later evolved through the 2004 World Health Organization (WHO) tumor classification [3], 2012 Vancouver ISUP (International Society of Urologic Pathology) consensus conference [4], and most recently the 2016 WHO blue book [5]. This “histo-molecular” approach is now an integral part of defining renal tumors and the emerging entities, aiming to be clinically and therapeutically pertinent. A summary of genetic tests and routinely used immunohistochemical examinations in daily practice is shown in Table 1. There have been many studies describing and examining molecular genetic changes of renal tumors. All these studies have shown that the molecular genetic changes are remarkably heterogeneous across the whole spectrum of renal cell carcinomas (RCCs) and other tumors and that molecular-genetic analysis cannot be used as a universal diagnostic tool.
In this review, we present the most current knowledge concerning molecular-genetic aspects of renal epithelial neoplasms, which potentially can be used in daily diagnostic practice. It is important to note that ISUP recommendations for molecular genetic testing of renal cell tumors will be published in the near future.
2. Clear Cell Renal Cell Carcinoma (CCRCC)
Clear cell renal cell carcinoma (CCRCC), the most common RCC, is typically composed of cells with clear cytoplasm and with a rich fine capillary network [5]. CCRCCs can also exhibit with eosinophilic cytoplasm and marked cellular pleomorphism. CCRCC cases mimicking clear cell papillary RCC are not infrequently found [6,7].
Chromosome 3p deletion has been described in CCRCC since the 80s [8], and was recognized as a characteristic genetic feature of this tumor in the Heidelberg classification [1], present in more than 90% of cases [9,10]. In parallel, VHL gene located on chromosome 3p was described as the most frequently mutated gene (50–75%) in CCRCC, and later found to be silenced by promoter methylation in 5–20% of cases [9,10]. Thus, the most frequent genetic alteration in CCRCC involves chromosome 3p deletion, VHL mutation and/or VHL promoter methylation, leading to VHL inactivation, an early and crucial event in sporadic CCRCC and in the familial cancer syndrome von Hippel–Lindau disease [9,11].
In addition to VHL located on chromosome 3p, there are other genes such the component of the SWI/SNF chromatin remodeling complex PBRM1 (26–33%), the histone modifying enzymes SETD2 (4–12%) and BAP1 (10%) being frequently reported in CCRCC [12,13,14].
Application in routine practice:
The presence of VHL mutation, chromosome 3p deletion or VHL promoter methylation is considered useful for the confirmation of CCRCC diagnosis in difficult cases (see following sections).
3. Multilocular Cystic Renal Cell Neoplasm of Low Malignant Potential (MCRCNLMP)
Multilocular cystic renal cell neoplasm of low malignant potential (MCRCNLMP) is a rare (<1%) renal tumor with an excellent prognosis, without recurrence or metastases described for bona fide cases [5]. Careful macroscopic evaluation and sampling are pivotal for the diagnosis, as the presence of solid nodules and/or cell clusters with expansive growth warrants a diagnosis of multicystic CCRCC [5]. MCRCNLMP, a low-grade tumor, had been considered a variant of CCRCC due to morphological similarities and analogous genetic features [15,16,17]. The most frequent genetic alterations in MCRCNLMP are identical to chromosome 3p deletion in 74% (14/19) of cases [17] and VHL mutation in 25% (3/12) of cases [18].
Interestingly, KRAS mutation was not found in small cohort of 12 MCRCNLMP cases, contrarily to codon 12 or codon 13 mutations identified in 12 CCRCC cases [19,20]. Of note, other studies that failed to identify KRAS mutation in CCRCC sequenced only codon 12 [21], codon 2 [22] or codons 1 and 2 [23], or used distinct methodology [24,25], which might have contributed to the conflicting results.
Application in routine practice:
Similar to CCRCC, chromosome 3p deletion and VHL mutation might be found in MCRCNLMP, but no specific genetic alterations have so far been identified. Careful macroscopic and microscopic evaluation is the gold standard for diagnosis.
4. Papillary Renal Cell Carcinoma (PRCC)
Papillary renal cell carcinoma (PRCC) is the second most common type of RCC, traditionally referred as tumor comprising of 15% of all RCCs [26]. According to the latest classification systems (WHO 2004, Vancouver ISUP Classification), it is classified into type 1 and type 2 PRCCs, which is also currently being used in the latest WHO 2016 classification. While PRCC type 1 seems to be a distinct and compact histo-molecular entity, the so-called type 2 appears to be, rather, composed of a group of tumors sharing papillary/tubulopapillary architecture with different molecular and genetic features [27]. In addition, there have recently been a number of subtypes/variants of papillary renal tumors (i.e., fumarate hydratase (FH)-deficient RCC, oncocytic PRCC), expanding the PRCC spectrum [27].
4.1. Type 1 Papillary RCC
The morphology of PRCC type 1 is well defined and in most cases would suffice for an accurate diagnosis in routine practice [5]. These tumors also have a distinct immunohistochemical profile, which can be further utilized in addition to basic hematoxylin and eosin (H&E) staining in the diagnostic workup [5].
The CNV (copy-number variation) pattern is relatively constant demonstrating polysomy or trisomy of chromosomes 7 or 17 as the most frequently referred changes. However, gains of chromosomes 3, 12, 16, and 20 (and less frequently gains of chromosomes 2, 4, 5, 6, 8, 13, and 18) have also been noted in these tumors. Of note, chromosomal losses have also been reported (chromosomes 1, 2, 4, 5, 7, 8, 9, 10, 11, 14, 15, 16, 18, 19, 20, 21, and 22) [28].
4.2. Type 2 Papillary RCC
“Type 2” papillary RCC is considered a controversial entity and currently by most authors deemed rather to represent multiple specific papillary renal neoplasms. Although gains of chromosomes 7 and 17 were reported to be the most frequently listed CNV changes for this subtype, the recent literature show that trisomy/polysomy 7/17 is not commonly associated with type 2 PRCC [28]. Based on a systematic review published recently, gains of chromosomes 12, 16 and 20 are also frequently reported in papillary RCC “Type 2” [28].
There are several genetic-based studies supporting the notion that the so-called “Type 2” PRCC is rather a group of tumors. Such tumors showed CDKN2A silencing, SETD2 mutations, and increased expression of the NRF2 antioxidant response element pathway [27]. Of note, FH-deficient RCCs, a high-grade PRCC which was previously categorized as PRCC “Type 2”, have already been reclassified from Type 2 PRCC, owing to recent molecular and genetic studies on Type 2 PRCCs [27].
4.3. Oncocytic Papillary RCC/Papillary Renal Cell Neoplasm with Reverse Polarity
Oncocytic papillary RCC, the “third” variant/subtype of papillary RCC included in the WHO 2016 blue book [32,33,34,35], is a poorly understood papillary RCC entity composed of oncocytic neoplastic cells [26,36]. CNV pattern in these tumors is highly variable with at least 3 patterns being reported: (1) gains of chromosomes 7 and 17 [33,34,35], (2) gains of chromosomes 3 and 11, and (3) loss of chromosome Y in male patients as well as losses of chromosomes 1, 4, 14 and loss of chromosome X. Some these tumors have shown to have a copy number pattern identical to renal oncocytoma: disomic status of chromosomes 7 and 17, some with deletion of chromosome 14, deletion of 1p (locus 1p36) [37]. Saleeb et al. considered oncocytic PRCC as so-called “type 4” papillary RCC (oncocytic low-grade), [38]. Al-Obaidy et al. have proposed the term papillary renal cell neoplasm with reverse polarity at last for a part of the spectrum of oncocytic RCC with papillary architecture [39]. Interestingly, this tumor is characterized by frequent KRAS mutations [40].
4.4. Papillary RCC NOS: Other Variants
A number of unusual papillary RCC variants have recently been described such as solid, mucin secreting, biphasic squamoid, and Warthin-like, which potentially can create diagnostic challenges in routine practice [41,42,43,44,45,46,47]. It should be noted that all of these variants are defined mostly using morphologic features and that their molecular-genetic features are widely varied, as generally observed in papillary RCCs.
Application in routine practice:
PRCC type 1 is a distinct entity, demonstrating typical CNV of gain of 7, 17 and loss of the Y chromosome in male patients. PRCC type 2 is rather composed of a group of tumors without a consistent CNV pattern. Considering highly variable CNV patterns among PRCCs in general (except for type 1 PRCC), it is almost impossible to diagnose PRCC based on CNV or based on another molecular genetic methods only. In high grade papillary renal tumors, FH-deficient RCC should always be considered and ruled out using a combination of immunohistochemistry and FH mutation/LOH (loss of heterozygosity) analysis.
5. Chromophobe Renal Cell Carcinoma (ChRCC)
Molecular-genetic testing will not be required to make a diagnosis of typical chromophobe RCC (ChRCC) (classic or eosinophilic variants). In addition to classic and eosinophilic ChRCCs, there are several other variants which have been described in the literature including pigmented microcystic adenomatoid, multicystic variant, [48,49,50,51] ChRCC with neuroendocrine differentiation, [52,53,54,55,56] and renal oncocytoma-like variant [57]. With the exception of ChRCC with neuroendocrine features, it seems that such variability has no influence on biological behavior. However, ChRCC with neuroendocrine features is a more aggressive variant [52].
CNV in ChRCC is rather variable and as such would be challenging to utilize in routine practice. ChRCC is usually associated with multiple chromosomal losses including chromosomes Y, 1, 2, 6, 10, 13, 17, 21 [58,59]. However, multiple chromosomal gains (chromosomes 4, 7, 15, 19, and 20), or even diploid pattern have been described in otherwise typical CHRCCs [60,61,62,63].
Testing germline mutations in the novel tumor suppressor gene FLCN (folliculin) can be used to support the diagnosis of Birt–Hogg–Dubé syndrome, which predisposes to the so-called “hybrid” oncocytic/chromophobe tumors.
Application in routine practice:
Molecular genetic ancillary tests are not useful for diagnosing ChRCC in daily practice. However, FLCN gene analysis can be useful in “hybrid” oncocytic/chromophobe tumors in suspected cases.
6. Oncocytoma
Renal oncocytoma (RO) can mostly be diagnosed based on morphology, while in difficult cases immunohistochemical examination can be further utilized. Molecular genetic tests are rarely used to diagnose RO. There are 3 basic genetic patterns in ROs: (1) loss of chromosome 1 (in whole or in part) and loss of chromosome Y, (2) rearrangements of 11q13 (mostly translocation t(5;11)(q35;q13)), chromosome 14 deletion, and (3) a normal karyotype [64,65,66,67,68,69].
These patterns have led some authors to propose two or three dominant subtypes of RO, however the clinical utility of such categorization remains unclear [69,70]. It has recently been recognized that CCND1 (cyclin D1) is located on the 11q13 locus. There are several studies that have attempted to sub-classify ROs according to the CCND1 status [69,70,71]. Nonetheless, all these proposals have shown no clinical usefulness and utility in daily routine and differential diagnostic practice. Similar to ChRCCs, the most commonly used test is the analysis of the FLCN gene in a similar setting, such as in “hybrid” oncocytic/chromophobe tumors.
Application in routine practice:
Similar to ChRCCs, molecular-genetic ancillary tests are not very useful for ROs in daily practice. However, FLCN gene analysis in suspected cases of “hybrid” oncocytic/chromophobe tumors is useful.
7. Clear Cell Papillary Renal Cell Carcinoma (CCPRCC)
The diagnosis of typical clear cell papillary renal cell carcinoma (CCPRCC) is mostly based on the morphology and immunohistochemical profile. In typical cases with characteristic morphology, diffuse CK7 positivity, and strong cup-shaped positivity with CANH 9, molecular genetic testing is not necessary for the diagnosis of CCPRCC [72,73,74]. However, there are some cases of CCPRCCs which show more complex morphologic features and substantial overlap with other RCCs (i.e., CCRCC). Because CCPRCC is an indolent neoplasm (with few extremely rare exceptions), an accurate diagnosis is crucial for further management. We believe that in such instances, further analysis of the VHL gene is the most useful and valuable step in arriving at the correct diagnosis in routine practice [75]. In fact, analysis of 3p25 loss and VHL gene alterations (mutations and methylation status) together with morphology and immunohistochemical profile would allow us to correctly diagnose almost all such cases [75].
It is important to emphasis that CCPRCC has been described in patients with von Hippel–Lindau syndrome. In such cases, VHL germline mutation is an obvious finding and can’t be helpful in differential diagnostic process.
Application in routine practice:
Majority of CCPRCC are diagnosed based on morphology and immunogistochemical profile. In challenging cases where the morphology and/or immunohistochemical profile are not typical of CCPRCC, genetic testing for VHL mutation/methylation and/or chromosome 3p loss are essential for rendering an accurate diagnosis of CCPRCC.
8. MiT Family Translocation-Associated Renal Cell Carcinoma
Renal tumors with TFE3, TFEB, and MiTF rearrangements are “classic” translocation-associated RCCs, being diagnosed based on a combination of morphologic, immunohistochemical, and molecular genetic analyses. RCC with TFE3 rearrangements (Xp11.2) is the most common of all translocation-associated RCCs. Although morphologic features of translocation-associated RCCs are well described in the literature, recent studies have described morphologic variants associated with different fusion partners, which can in itself pose challenges to the diagnostic process. Some of these tumors are surprisingly similar in morphology to clear cell papillary RCC (TFE3-NONO). So far the following fusion partners for TFE3 gene have been described: ASPSCR1, PRCC, NONO, SFPQ, CLTC, PARP14, LUC7L3, KHSRP, DVL2, MED15, NEAT1, RBM10, KAT6A, and GRIPAP1 [76,77,78,79,80,81,82,83,84].
Although TFE3 translocation RCCs can show a diverse morphologic spectrum, certain morphologic features (i.e., high-grade cells with abundant clear/eosinophilic cytoplasm and papillary/nested architecture; psammomatous calcifications) can be suggestive of this entity. Immunohistochemical analysis may not be sufficient to confirm the diagnosis of TFE3 translocation RCC, and that in some cases further molecular genetic testing maybe indicated [85]. Fluorescence in situ hybridization (FISH) testing is usually used to confirm the diagnosis. It should be noted that in some fusion partners, FISH can produce false negative results [85,86]. Thus, NGS is more accurate, namely for cases, where fusion partner is beyond the reaches of probe or staying too close to TFE3.
TFEB or t(6;11) translocation RCC is much less common member of the MiT family RCCs. These tumors exhibit a typical biphasic morphologic feature composed of large epithelioid cells with clear/eosinophilic cytoplasm and a minor population of small eosinophilic cells that form rosette-like structures within basement membrane-like material. Immunohistochemically, these neoplasms express melanocytic markers (HMB45 and/or Melan A). Usually there is a fusion of MALAT1 and TFEB, although other partners such as COL21A1, CADM2, and KHDRBS2 have recently been described [27,87]. However, even in the group of TFEB or t(6;11) translocation RCC, there is morphologic variability and that not all cases follow a “classic“ morphologic pattern with biphasic morphology (Figure 1).
Recent studies have shown that amplification of the TFEB gene in TFEB or t(6;11) translocation RCCs can uncommonly occur and is associated with more aggressive clinical behavior with distant metastases (see RCC with TFEB amplification). It is worth noting that amplification of TFEB gene can rarely be found in various renal tumors, most of which are usually unclassified RCCs or translocation-like RCCs.
Application in routine practice:
Diagnosis of TFE3 translocation RCC should be considered in RCC with a mixture of clear cell and papillary features, psammoma bodies, abnormally voluminous cytoplasm, hyalinized stroma, or in a young/pediatric patient. Although positive immunohistochemical staining for TFE3 or TFEB proteins, melanocytic markers, or cathepsin K can be suggestive, molecular genetic testing is highly recommended for confirming the diagnosis. FISH for TFE3 or TFEB rearrangement is a helpful diagnostic tool; however NGS is recommended in cases where false negative FISH can be expected (namely partners RBM10, RBMX, GRIPAP1, and NONO). In other words, when the morphology and/or immunohistochemical profile is suggestive of TFE3 translocation RCC, NGS analysis is recommended for confirmation. Amplification of TFEB gene seems to be a strong adverse prognostic indicator in TFEB translocation RCCs, however such cases are rare and less frequently encountered comparing with TFEB amplified RCCs (without TFEB break) its occurrence is rather rare.
9. Mucinous Tubular and Spindle Cell Carcinoma (MTSCC)
Mucinous tubular and spindle cell carcinoma (MTSCC) is usually a non-aggressive renal tumor with characteristic morphology. This neoplasm can resemble PRCC with overlapping morphologic and even immunohistochemical features [88,89,90]. In the past, studies reported variable CNV patterns for MTSCC, even sometimes resembling PRCC CNV pattern suggesting MTSCC to be a variant of PRCC type 1 [36,91]. However, recent studies have shown that MTSCCs typically have a CNV pattern with multiple chromosomal losses involving chromosomes 1, 4, 6, 8, 9, 13, 14, 15, and 22, without the gains of chromosomes 7 and 17 [92,93,94,95]. In cases where there is a morphologic overlap with PRCC (mostly type 1), CNV also shows overlapping features with frequent gains of chromosomes 7 and/or 17.
Application in routine practice:
MTSCC is an indolent and rare tumor with characteristic morphologic features that can be used in diagnosis in the vast majority of cases (with or without immunohistochemical studies). In difficult cases, CNV pattern analysis can be helpful. Tumors with features of PRCC, including gain of chromosome 7 or 17, should be classified as PRCC NOS.
10. Tubulocystic Renal Cell Carcinoma (TC-RCC)
Tubulocystic RCC (TC-RCC) is a relative new entity first officially included in the 2012 ISUP Vancouver Classification. Similar to MTSCC, TC-RCC has morphologic and immunohistochemical features that are frequently overlap with PRCC [36,96,97].
The genetic features of these tumors are variable with previous studies suggesting similar CNV patterns to that reported in type 1 PRCC (gain of chromosome 7 or 17 and loss of Y). However, more recent studies showed that gain of chromosomes 7 and 17 is not a typical CNV pattern in cases of TC-RCC where strict histo-diagnostic criteria are applied [96,97,98]. In fact, loss of chromosome 9 has been suggested as a characteristic feature of TC-RCC [99]. It should be noted that TC-RCC is a rare and indolent tumor that should not be confused with fumarate hydratase (FH)-deficient RCC, where the tumor shows a low grade tubulocystic pattern and with abrupt transition to high-grade infiltrative carcinoma. A similar situation exists in tumors with pure tubulocystic pattern and eosinophilic cells but with prominent macronucleoli. Such cases must be considered as potentially FH deficient RCCs and immunohistochemical/molecular-genetic examination of FH should be performed [100,101].
Application in routine practice:
TC-RCC should be diagnosed based on its strict histologic criteria, without mixed areas resembling PRCC. If CNV patterns show gains of chromosome 7 and 17, it is advised to best classify it as PRCC than TC-RCC. RCCs with “Tubulocystic” features and high grade abrupt areas should raise the possibility of FH-deficient RCC and be further genetically tested for FH gene mutation/LOH.
11. Acquired Cystic Kidney Disease (ACD)-Associated Renal Cell Carcinoma
Acquired cystic kidney disease (ACD)-associated RCC is a relatively rare renal tumor. Its morphologic feature is relatively variable, as is its immunohistochemical profile. However several studies described gains of chromosomes 7 and 17, and other showed gain of chromosomes 3, 16, and Y [102,103,104,105,106,107].
Application in routine practice:
Currently there are no specific genetic alterations useful for routine practice in these tumors.
12. Renal Medullary Carcinoma
Renal medullary carcinoma is a rare, aggressive, and high grade renal tumor occurring mostly in African Americans with sickle cell trait or with other hemoglobinopathies. Within the differential diagnosis, collecting duct carcinoma, high-grade urothelial carcinoma and other high-grade RCCs should be always considered. [108] Medullary carcinoma is characterized by loss of the SMARCB1 (INI-1) gene [109,110,111], which can also be detected immunohistochamically (following by positive OCT3/4 staining) [108,112,113,114,115]. In rare cases where alterations of SMARCB1 gene or abnormal negative staining for the protein is documented in the absence of sickle trait, the term “RCC unclassified with medullary phenotype” has been proposed [116,117].
Application in routine practice:
High-grade renal tumors with histologic features suggestive of renal medullary carcinoma should be stained with SMARCB1. For cases with loss of SMARCB1 expression, molecular genetic testing of SMARCB1 is useful. The result of immunohistochemical/genetic testing should be correlated with hematologic findings (i.e., sickle cell trait or other hemoglobinopathy). In situation, when RCCs with SMARCB1 loss is encountered, and sickle trait or other hemoglobinopathies are absent, it is currently recommended to classify them as RCC unclassified with medullary phenotype.
13. Collecting Duct Carcinoma (CDC)
One of the most frequently misclassified renal tumors is still collecting duct carcinoma (CDC). Even nowadays, the diagnosis of CDC remains the diagnosis of exclusion. The following entities should be always be considered and excluded in such scenarios: FH-deficient RCC, high-grade urothelial carcinoma of renal pelvis, renal medullary carcinoma, and metastatic carcinoma from another organ.
Unfortunately, currently there is no characteristic molecular genetic feature or combination of features useful for differential diagnosis. Molecular genetic testing should be considered after excluding other entities in the differential diagnosis (i.e., FH-deficient RCC, renal medullary carcinoma).
Application in routine practice:
There is no specific molecular genetic test which can help to establish the diagnosis of CDC. FH-deficient RCC and renal medullary carcinoma should be always considered and diagnosis can be supported by genetic testing.
14. Succinate Dehydrogenase (SDH)-Deficient Renal Cell Carcinoma
Renal tumors associated with autosomal dominant germline mutations of SDHA, SDHB, SDHC and SDHD have recently been described. Such tumors are part of syndrome characterized by occurrence of renal carcinomas, paragangliomas/pheochromocytomas, gastrointestinal stromal tumors (GIST), and pituitary adenomas [118,119]. The majority of succinate dehydrogenase (SDH)-deficient RCCs demonstrate a characteristic morphology with solid alveolar architecture, eosinophilic cytoplasm with numerous intracytoplasmatic vacuoles (Figure 2). Cases with high grade features and overlapping morphology resembling CCRCC, PRCC or unclassified RCC have also been described. Immunohistochemical staining for SDHB is negative. Antibody against SDHB detects all 4 subgroups (SDHA, SDHB, SDHC and SDHD) deficiencies [118,119]. However, the interpretation of SDHB staining must be done with caution and an internal positive control should be present. SDH deficiency is almost always associated with germline SDH subunit mutation [118,119,120,121].
Application in routine practice:
Suspected cases should be immunohistochemically stained for SDHB. Immunohistochemical staining for SDHB is negative in SDH-deficient cases. The vast majority of SDH-deficient RCCs are associated with germline mutation of the SDHB subunit. Genetic testing of SDH subunit mutation is not necessary, however in cases where the result of immunohistochemical examination is inconclusive, it is highly recommended.
15. Fumarate Hydratase (FH)-Deficient RCC and HLRCC (Hereditary Leiomyomatosis and Renal Cell Carcinoma)
FH-deficient RCC and hereditary leiomyomatosis and renal cell carcinoma associated RCC have been discussed extensively in the recent literature. Initially it was thought that these tumors are hereditary counterparts of the so-called “type 2” PRCC. Histologically, they show marked intratumoral heterogeneity with papillary, tubulocystic, solid or cribriform patterns, and usually the presence of large nuclei with deep red nucleoli (Figure 3A,B). However, no single or a combination of histologic features are diagnostic of FH-deficient RCCs/HLRCCs [101,108,122,123,124,125,126,127,128].
Immunohistochemically, FH-deficient RCCs show loss of staining for fumarate hydratase (FH) (sensitivity 80 to 90%) [101,108,123,124,125,126,127,128,129]. Positive immunohistochemical staining for 2SC (2-Succinocysteine) is supportive feature, however antibody for 2SC is not currently commercially available [123,125,129]. The CNV pattern is heterogeneous, no constant combination of changes has been disclosed so far and it is not possible to use it in differential diagnostic process [124].
Overall, in cases with suspected clinical and morphologic features (high-grade aggressive RCCs in young patients) FH-deficient RCCs/HLRCCs should be considered in the differential diagnostic workup. For screening, immunohistochemical staining with FH is useful, however cases where staining interpretation is not convincing or in suspected clinical settings it would be better to test for FH mutation/LOH.
Application in routine practice:
High-grade RCCs occurring in young patients exhibiting variable growth patterns and morphologic features should prompt the differential diagnosis of FH-deficient RCCs/HLRCCs. Immunohistochemically, FH can be helpful; however, it is not 100% specific, and as such analysis of FH mutation/LOH should be considered.
16. New but Perspective Renal Tumors
As mentioned earlier in the introduction, renal tumors are intensively studied and more new entities and variants are described every year. It is questionable whether all these variants will be regarded as established entities within future classifications or whether they will be reclassified as variants of some “traditional” renal tumors. Some of the published papers are recent without further corroboration by other studies, while others worked with a limited number of cases. More studies examining the ideas and hypotheses would be needed to allow including such entities in the future WHO classifications. In the following section we will briefly introduce such tumors. Majority of new entities will be covered in other reviews in this issue of Cancers.
16.1. Eosinophilic Solid and Cystic (ESC) RCC
Eosinophilic solid and cystic RCC (ESC-RCC) is a recently recognized entity, described in patients with TS (tuberous sclerosis) complex. Subsequently, identical tumors were described in patients without any relation to TS complex, mostly middle aged/elderly women [130,131]. These tumors have solid and cystic architecture, composed of neoplastic cells with voluminous cytoplasm showing basophilic stippling [132]. They are frequently positive for cytokeratin 20, which is highly unusual for any RCCs [132]. Both familiar and sporadic tumors have molecular alterations of TSC1 or TSC2 [133,134,135,136,137].
16.2. RCC with TSC/MTOR Gene Mutations
The molecular genetic revolution in the field of oncopathology has resulted in identifying more entities including a recently described subset of tumors harboring mutations of TSC1, TSC2, or MTOR, being recognized in sporadic patients as well as patients with tuberous sclerosis complex [130,131]. RCC with prominent smooth muscle (or sometimes referred as RCC with angioleiomyoma-like stroma), [130,138,139,140,141,142], tumors with oncocytic features named as HOT (high-grade oncocytic tumor) or descriptively as sporadic RCC with eosinophilic and vacuolated cytoplasm [143,144,145] are best known examples of this group.
16.3. TCEB1-Mutated RCC
These tumors are well-circumscribed, have predominantly tubular and papillary architecture, and have thick intersecting fibromuscular bands superficially resembling a renal angiomyoadenomatous tumor (RAT)-like morphology. They are distinct from both CCRCC and CCPRCC, harboring mutations of TCEB1 but with no VHL gene abnormalities [24,138,140,146,147,148]. Given the limited data available on these tumors, it is rather early to assume concrete conclusions [146].
16.4. RCC with TFEB/6p21/VEGFA Amplification
RCC with TFEB rearrangement is a poorly understood entity, although such tumors have been described or briefly mentioned in several papers. The first systematic study summarizing knowledge about this group of tumors was published by Williamson at al. [149] in 2017. It appears that tumors from this group show amplification of chromosome 6p21 with changes in TFEB and VEGFA [149,150,151,152,153,154,155,156]. So far the described cases show variable morphology with shared positivity for melan-A and/or HMB45. Cathepsin K is usually positive [149,150]. RCC with TFEB/6p21/VEGFA amplification exhibit papillary architecture, however tumors resembling CCRCC or ChRCC were also documented. Molecular genetics usually disclose amplification of TFEB/6p21/VEGFA, while rearrangement of TFEB is usually not present. However, in one of the first cases authors pointed out that amplification of TFEB gene might be a marker of aggressive behavior showed both rearrangement and amplification [152] (Figure 4). Recent work shows that TFEB gene expression is increased in these tumors, although not as much as in TFEB translocation tumors, raising the possibility that other genes at the 6p21 locus, such as VEGFA or CCND3 or other genes may be responsible for aggressive behavior [155].
16.5. ALK-Rearranged RCC
Rearrangement of ALK has been described in various tumors, mostly in lymphomas, lung carcinomas, and thyroid carcinomas. In kidney, renal tumors with ALK rearrangement have also been rarely reported [157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174]. Histologically, they show a tubulopapillary or cribriform pattern with rhabdoid-like cell morphology in a myxoid/mucinous background (mostly interstitium). Fusion partners that have been identified in ALK-rearranged RCC are TPM3, STRN, VCL, HOOK1, CLIP1, and KIF5B. Some cases demonstrated highly surprising morphology, identical to metanephric adenoma or MTSCC [166].
17. Discussion
It is well-known that renal tumors are characterized by marked both intertumoral and intratumoral heterogeneity, which can play role in tumor evolution and hamper personalized therapeutic strategies. Molecular characterization of renal cell neoplasms has led to the identification of driver genes and specific molecular pathways. This comprehension along with the traditional histo-morphologic features has revolutionized the treatment approach and modalities in these tumors.
Imaging genomics, an emerging research field, has also created new opportunities for the diagnosis and prognosis of renal tumors. Of note, Cheng et al. [175] developed and examined an integrative genomics framework for constructing a prognostic model for clear cell renal cell carcinomas using both histopathologic images and genomic signatures. Similarly, Shao et al. [176] introduced ordinal multi-modal feature selection framework that simultaneously identified important features from both pathological images and multi-modal genomic data for the prognosis. It appears that such an integrative pathologic-genomics approach can help to better understand prognostic and hopefully therapeutic aspects of various renal tumors.
It should be noted that one of the main challenges in assessing the current literature on molecular-genetic characteristics of renal tumor is related to the heterogeneity of methodologies and definitions used in various studies. This is mainly due to the fact that our understating of renal neoplasms is evolving as the new molecular and technological advances are emerging such as NGS. Despite the limitations of the current literature, we are still able to draw the landscape of uniform histo-molecular renal entities.
18. Conclusions
Overall, most renal tumors can easily be diagnosed based on pure histologic findings with or without immunohistochemical examination. However, in selected cases, molecular-genetic testing can be utilized to assist in arriving at an accurate diagnosis.
Author Contributions
R.A.: literature search, first author D.P.M.: literature search, Table, A.S.L.: literature search, clear cell RCC and Multiloculasr Cystic Renal Cell Neoplasm of Low Malignant Potential section, O.H.: literature search, review design, photos. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Charles University Research Fund (project number Q39) and by the grant of Ministry of Health of the Czech republic-Conceptual Development of Research Organization (Faculty Hospital in Plzen- FNPl 00669806).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kovacs, G.; Akhtar, M.; Beckwith, B.J.; Bugert, P.; Cooper, C.S.; Delahunt, B.; Eble, J.N.; Fleming, S.; Ljungberg, B.; Medeiros, L.J.; et al. The Heidelberg classification of renal cell tumours. J Pathol 1997, 183, 131–133. [Google Scholar] [CrossRef]
- Storkel, S.; Eble, J.N.; Adlakha, K.; Amin, M.; Blute, M.L.; Bostwick, D.G.; Darson, M.; Delahunt, B.; Iczkowski, K. Classification of renal cell carcinoma: Workgroup No. 1. Union Internationale Contre le Cancer (UICC) and the American Joint Committee on Cancer (AJCC). Cancer 1997, 80, 987–989. [Google Scholar] [CrossRef]
- Eble, J.N.; Sauter, G.; Epstein, J.; Sesterhenn, I. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs, WHO Classification of Tumours, 3rd ed.; WHO: Geneva, Switzerland; IARC Press: Lyon, Switzerland, 2004; Volume 7. [Google Scholar]
- Delahunt, B.; Srigley, J.R.; Montironi, R.; Egevad, L. Advances in renal neoplasia: Recommendations from the 2012 International Society of Urological Pathology Consensus Conference. Urology 2014, 83, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V.E. WHO Classification of Tumours of the Urinary System and Male Genital Organs—WHO Classification of Tumours, 4th ed.; WHO: Geneva, Switzerland; IARC Press: Lyon, Switzerland, 2016; Volume 8. [Google Scholar]
- Petersson, F.; Grossmann, P.; Hora, M.; Sperga, M.; Montiel, D.P.; Martinek, P.; Gutierrez, M.E.; Bulimbasic, S.; Michal, M.; Branzovsky, J.; et al. Renal cell carcinoma with areas mimicking renal angiomyoadenomatous tumor/clear cell papillary renal cell carcinoma. Hum. Pathol. 2013, 44, 1412–1420. [Google Scholar] [CrossRef] [PubMed]
- Somoracz, A.; Kuthi, L.; Micsik, T.; Jenei, A.; Hajdu, A.; Vrabely, B.; Raso, E.; Sapi, Z.; Bajory, Z.; Kulka, J.; et al. Renal Cell Carcinoma with Clear Cell Papillary Features: Perspectives of a Differential Diagnosis. Pathol. Oncol. Res. 2019. [Google Scholar] [CrossRef] [Green Version]
- Carroll, P.R.; Murty, V.V.; Reuter, V.; Jhanwar, S.; Fair, W.R.; Whitmore, W.F.; Chaganti, R.S. Abnormalities at chromosome region 3p12-14 characterize clear cell renal carcinoma. Cancer Genet. Cytogenet. 1987, 26, 253–259. [Google Scholar] [CrossRef]
- Smits, K.M.; Schouten, L.J.; van Dijk, B.A.; Hulsbergen-van de Kaa, C.A.; Wouters, K.A.; Oosterwijk, E.; van Engeland, M.; van den Brandt, P.A. Genetic and epigenetic alterations in the von hippel-lindau gene: The influence on renal cancer prognosis. Clin. Cancer Res. 2008, 14, 782–787. [Google Scholar] [CrossRef] [Green Version]
- Banks, R.E.; Tirukonda, P.; Taylor, C.; Hornigold, N.; Astuti, D.; Cohen, D.; Maher, E.R.; Stanley, A.J.; Harnden, P.; Joyce, A.; et al. Genetic and epigenetic analysis of von Hippel-Lindau (VHL) gene alterations and relationship with clinical variables in sporadic renal cancer. Cancer Res. 2006, 66, 2000–2011. [Google Scholar] [CrossRef] [Green Version]
- Latif, F.; Tory, K.; Gnarra, J.; Yao, M.; Duh, F.M.; Orcutt, M.L.; Stackhouse, T.; Kuzmin, I.; Modi, W.; Geil, L.; et al. Identification of the von Hippel-Lindau disease tumor suppressor gene. Science 1993, 260, 1317–1320. [Google Scholar] [CrossRef]
- Dalgliesh, G.L.; Furge, K.; Greenman, C.; Chen, L.; Bignell, G.; Butler, A.; Davies, H.; Edkins, S.; Hardy, C.; Latimer, C.; et al. Systematic sequencing of renal carcinoma reveals inactivation of histone modifying genes. Nature 2010, 463, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Guo, G.; Gui, Y.; Gao, S.; Tang, A.; Hu, X.; Huang, Y.; Jia, W.; Li, Z.; He, M.; Sun, L.; et al. Frequent mutations of genes encoding ubiquitin-mediated proteolysis pathway components in clear cell renal cell carcinoma. Nat. Genet. 2011, 44, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Varela, I.; Tarpey, P.; Raine, K.; Huang, D.; Ong, C.K.; Stephens, P.; Davies, H.; Jones, D.; Lin, M.L.; Teague, J.; et al. Exome sequencing identifies frequent mutation of the SWI/SNF complex gene PBRM1 in renal carcinoma. Nature 2011, 469, 539–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzigan, S.; Lopez-Beltran, A.; Montironi, R.; Drut, R.; Romero, A.; Hayashi, T.; Gentili, A.L.; Fonseca, P.S.; deTorres, I.; Billis, A.; et al. Multilocular cystic renal cell carcinoma: A report of 45 cases of a kidney tumor of low malignant potential. Am. J. Clin. Pathol. 2006, 125, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Williamson, S.R.; Halat, S.; Eble, J.N.; Grignon, D.J.; Lopez-Beltran, A.; Montironi, R.; Tan, P.H.; Wang, M.; Zhang, S.; Maclennan, G.T.; et al. Multilocular cystic renal cell carcinoma: Similarities and differences in immunoprofile compared with clear cell renal cell carcinoma. Am. J. Surg. Pathol. 2012, 36, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Halat, S.; Eble, J.N.; Grignon, D.J.; Lopez-Beltran, A.; Montironi, R.; Tan, P.H.; Wang, M.; Zhang, S.; MacLennan, G.T.; Cheng, L. Multilocular cystic renal cell carcinoma is a subtype of clear cell renal cell carcinoma. Mod. Pathol. 2010, 23, 931–936. [Google Scholar] [CrossRef] [PubMed]
- von Teichman, A.; Comperat, E.; Behnke, S.; Storz, M.; Moch, H.; Schraml, P. VHL mutations and dysregulation of pVHL- and PTEN-controlled pathways in multilocular cystic renal cell carcinoma. Mod. Pathol. 2011, 24, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Raspollini, M.R.; Castiglione, F.; Martignoni, G.; Cheng, L.; Montironi, R.; Lopez-Beltran, A. Unlike in clear cell renal cell carcinoma, KRAS is not mutated in multilocular cystic clear cell renal cell neoplasm of low potential. Virchows Arch. 2015, 467, 687–693. [Google Scholar] [CrossRef]
- Raspollini, M.R.; Castiglione, F.; Cheng, L.; Montironi, R.; Lopez-Beltran, A. Synchronous clear cell renal cell carcinoma and multilocular cystic renal cell neoplasia of low malignant potential: A clinico-pathologic and molecular study. Pathol. Res. Pr. 2016, 212, 471–474. [Google Scholar] [CrossRef]
- Szymanska, K.; Moore, L.E.; Rothman, N.; Chow, W.H.; Waldman, F.; Jaeger, E.; Waterboer, T.; Foretova, L.; Navratilova, M.; Janout, V.; et al. TP53, EGFR, and KRAS mutations in relation to VHL inactivation and lifestyle risk factors in renal-cell carcinoma from central and eastern Europe. Cancer Lett. 2010, 293, 92–98. [Google Scholar] [CrossRef]
- Gattenlohner, S.; Etschmann, B.; Riedmiller, H.; Muller-Hermelink, H.K. Lack of KRAS and BRAF mutation in renal cell carcinoma. Eur. Urol. 2009, 55, 1490–1491. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, O.; Sen, H.; Bulut, E.; Cengiz, B.; Karakok, M.; Erturhan, S.; Seckiner, I. Evaluation of EGFR, KRAS and BRAF gene mutations in renal cell carcinoma. J. Kidney Cancer VHL 2014, 1, 40–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, Y.; Yoshizato, T.; Shiraishi, Y.; Maekawa, S.; Okuno, Y.; Kamura, T.; Shimamura, T.; Sato-Otsubo, A.; Nagae, G.; Suzuki, H.; et al. Integrated molecular analysis of clear-cell renal cell carcinoma. Nat. Genet. 2013, 45, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research, N. Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature 2013, 499, 43–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delahunt, B.; Algaba, F.; Eble, J.; Cheville, J.; Amin, M.B.; Argani, P.; Martignoni, G.; Moch, H.; Srigley, J.R.; Tan, P.H.; et al. Papillary renal cell carcinoma. In WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; Moch, H., Humphrey, P.A., Ulbright, T.M., Reuter, V.E., Eds.; International Agency for Research on Cancer: Lyon, France, 2016; Volume 8, pp. 23–25. [Google Scholar]
- Cancer Genome Atlas Research, N.; Linehan, W.M.; Spellman, P.T.; Ricketts, C.J.; Creighton, C.J.; Fei, S.S.; Davis, C.; Wheeler, D.A.; Murray, B.A.; Schmidt, L.; et al. Comprehensive Molecular Characterization of Papillary Renal-Cell Carcinoma. N. Engl. J. Med. 2016, 374, 135–145. [Google Scholar] [CrossRef]
- Pitra, T.; Pivovarcikova, K.; Alaghehbandan, R.; Hes, O. Chromosomal numerical aberration pattern in papillary renal cell carcinoma: Review article. Ann. Diagn. Pathol. 2019, 40, 189–199. [Google Scholar] [CrossRef]
- Zbar, B.; Tory, K.; Merino, M.; Schmidt, L.; Glenn, G.; Choyke, P.; Walther, M.M.; Lerman, M.; Linehan, W.M. Hereditary papillary renal cell carcinoma. J. Urol. 1994, 151, 561–566. [Google Scholar] [CrossRef]
- Schmidt, L.; Duh, F.M.; Chen, F.; Kishida, T.; Glenn, G.; Choyke, P.; Scherer, S.W.; Zhuang, Z.; Lubensky, I.; Dean, M.; et al. Germline and somatic mutations in the tyrosine kinase domain of the MET proto-oncogene in papillary renal carcinomas. Nat. Genet. 1997, 16, 68–73. [Google Scholar] [CrossRef]
- Dharmawardana, P.G.; Giubellino, A.; Bottaro, D.P. Hereditary papillary renal carcinoma type I. Curr. Mol. Med. 2004, 4, 855–868. [Google Scholar] [CrossRef]
- Lefevre, M.; Couturier, J.; Sibony, M.; Bazille, C.; Boyer, K.; Callard, P.; Vieillefond, A.; Allory, Y. Adult papillary renal tumor with oncocytic cells: Clinicopathologic, immunohistochemical, and cytogenetic features of 10 cases. Am. J. Surg. Pathol. 2005, 29, 1576–1581. [Google Scholar] [CrossRef]
- Han, G.; Yu, W.; Chu, J.; Liu, Y.; Jiang, Y.; Li, Y.; Zhang, W. Oncocytic papillary renal cell carcinoma: A clinicopathological and genetic analysis and indolent clinical course in 14 cases. Pathol. Res. Pr. 2017, 213, 1–6. [Google Scholar] [CrossRef]
- Kunju, L.P.; Wojno, K.; Wolf, J.S., Jr.; Cheng, L.; Shah, R.B. Papillary renal cell carcinoma with oncocytic cells and nonoverlapping low grade nuclei: Expanding the morphologic spectrum with emphasis on clinicopathologic, immunohistochemical and molecular features. Hum. Pathol. 2008, 39, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Hes, O.; Brunelli, M.; Michal, M.; Cossu Rocca, P.; Hora, M.; Chilosi, M.; Mina, M.; Boudova, L.; Menestrina, F.; Martignoni, G. Oncocytic papillary renal cell carcinoma: A clinicopathologic, immunohistochemical, ultrastructural, and interphase cytogenetic study of 12 cases. Ann. Diagn. Pathol. 2006, 10, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Srigley, J.R.; Delahunt, B.; Eble, J.N.; Egevad, L.; Epstein, J.I.; Grignon, D.; Hes, O.; Moch, H.; Montironi, R.; Tickoo, S.K.; et al. The International Society of Urological Pathology (ISUP) Vancouver classification of renal neoplasia. Am. J. Surg. Pathol. 2013, 37, 1469–1489. [Google Scholar] [CrossRef] [PubMed]
- Michalova, K.; Steiner, P.; Alaghehbandan, R.; Trpkov, K.; Martinek, P.; Grossmann, P.; Montiel, D.P.; Sperga, M.; Straka, L.; Prochazkova, K.; et al. Papillary renal cell carcinoma with cytologic and molecular genetic features overlapping with renal oncocytoma: Analysis of 10 cases. Ann. Diagn. Pathol. 2018, 35, 1–6. [Google Scholar] [CrossRef]
- Saleeb, R.M.; Brimo, F.; Farag, M.; Rompre-Brodeur, A.; Rotondo, F.; Beharry, V.; Wala, S.; Plant, P.; Downes, M.R.; Pace, K.; et al. Toward Biological Subtyping of Papillary Renal Cell Carcinoma With Clinical Implications Through Histologic, Immunohistochemical, and Molecular Analysis. Am. J. Surg. Pathol. 2017, 41, 1618–1629. [Google Scholar] [CrossRef]
- Al-Obaidy, K.I.; Eble, J.N.; Cheng, L.; Williamson, S.R.; Sakr, W.A.; Gupta, N.; Idrees, M.T.; Grignon, D.J. Papillary Renal Neoplasm with Reverse Polarity: A Morphologic, Immunohistochemical, and Molecular Study. Am. J. Surg. Pathol. 2019, 43, 1099–1111. [Google Scholar] [CrossRef]
- Al-Obaidy, K.I.; Eble, J.N.; Nassiri, M.; Cheng, L.; Eldomery, M.K.; Williamson, S.R.; Sakr, W.A.; Gupta, N.; Hassan, O.; Idrees, M.T.; et al. Recurrent KRAS mutations in papillary renal neoplasm with reverse polarity. Mod. Pathol. 2019. [Google Scholar] [CrossRef]
- Marsaud, A.; Dadone, B.; Ambrosetti, D.; Baudoin, C.; Chamorey, E.; Rouleau, E.; Lefol, C.; Roussel, J.F.; Fabas, T.; Cristofari, G.; et al. Dismantling papillary renal cell carcinoma classification: The heterogeneity of genetic profiles suggests several independent diseases. Genes Chromosomes Cancer 2015, 54, 369–382. [Google Scholar] [CrossRef]
- Pivovarcikova, K.; Peckova, K.; Martinek, P.; Montiel, D.P.; Kalusova, K.; Pitra, T.; Hora, M.; Skenderi, F.; Ulamec, M.; Daum, O.; et al. “Mucin”-secreting papillary renal cell carcinoma: Clinicopathological, immunohistochemical, and molecular genetic analysis of seven cases. Virchows Arch. 2016, 469, 71–80. [Google Scholar] [CrossRef]
- Peckova, K.; Martinek, P.; Pivovarcikova, K.; Vanecek, T.; Alaghehbandan, R.; Prochazkova, K.; Montiel, D.P.; Hora, M.; Skenderi, F.; Ulamec, M.; et al. Cystic and necrotic papillary renal cell carcinoma: Prognosis, morphology, immunohistochemical, and molecular-genetic profile of 10 cases. Ann. Diagn Pathol. 2017, 26, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Ulamec, M.; Skenderi, F.; Trpkov, K.; Kruslin, B.; Vranic, S.; Bulimbasic, S.; Trivunic, S.; Montiel, D.P.; Peckova, K.; Pivovarcikova, K.; et al. Solid papillary renal cell carcinoma: Clinicopathologic, morphologic, and immunohistochemical analysis of 10 cases and review of the literature. Ann. Diagn. Pathol. 2016, 23, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Hes, O.; Condom Mundo, E.; Peckova, K.; Lopez, J.I.; Martinek, P.; Vanecek, T.; Falconieri, G.; Agaimy, A.; Davidson, W.; Petersson, F.; et al. Biphasic Squamoid Alveolar Renal Cell Carcinoma: A Distinctive Subtype of Papillary Renal Cell Carcinoma? Am. J. Surg. Pathol. 2016, 40, 664–675. [Google Scholar] [CrossRef] [PubMed]
- Trpkov, K.; Athanazio, D.; Magi-Galluzzi, C.; Yilmaz, H.; Clouston, D.; Agaimy, A.; Williamson, S.R.; Brimo, F.; Lopez, J.I.; Ulamec, M.; et al. Biphasic papillary renal cell carcinoma is a rare morphological variant with frequent multifocality: A study of 28 cases. Histopathology 2018, 72, 777–785. [Google Scholar] [CrossRef]
- Skenderi, F.; Ulamec, M.; Vanecek, T.; Martinek, P.; Alaghehbandan, R.; Foix, M.P.; Babankova, I.; Montiel, D.P.; Alvarado-Cabrero, I.; Svajdler, M.; et al. Warthin-like papillary renal cell carcinoma: Clinicopathologic, morphologic, immunohistochemical and molecular genetic analysis of 11 cases. Ann. Diagn. Pathol. 2017, 27, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Hes, O.; Vanecek, T.; Perez-Montiel, D.M.; Alvarado Cabrero, I.; Hora, M.; Suster, S.; Lamovec, J.; Curik, R.; Mandys, V.; Michal, M. Chromophobe renal cell carcinoma with microcystic and adenomatous arrangement and pigmentation--a diagnostic pitfall. Morphological, immunohistochemical, ultrastructural and molecular genetic report of 20 cases. Virchows Arch. 2005, 446, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Michal, M.; Hes, O.; Svec, A.; Ludvikova, M. Pigmented microcystic chromophobe cell carcinoma: A unique variant of renal cell carcinoma. Ann. Diagn. Pathol. 1998, 2, 149–153. [Google Scholar] [CrossRef]
- Dundr, P.; Pesl, M.; Povysil, C.; Tvrdik, D.; Pavlik, I.; Soukup, V.; Dvoracek, J. Pigmented microcystic chromophobe renal cell carcinoma. Pathol. Res. Pr. 2007, 203, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Foix, M.P.; Dunatov, A.; Martinek, P.; Mundo, E.C.; Suster, S.; Sperga, M.; Lopez, J.I.; Ulamec, M.; Bulimbasic, S.; Montiel, D.P.; et al. Morphological, immunohistochemical, and chromosomal analysis of multicystic chromophobe renal cell carcinoma, an architecturally unusual challenging variant. Virchows Arch. 2016, 469, 669–678. [Google Scholar] [CrossRef]
- Peckova, K.; Martinek, P.; Ohe, C.; Kuroda, N.; Bulimbasic, S.; Condom Mundo, E.; Perez Montiel, D.; Lopez, J.I.; Daum, O.; Rotterova, P.; et al. Chromophobe renal cell carcinoma with neuroendocrine and neuroendocrine-like features. Morphologic, immunohistochemical, ultrastructural, and array comparative genomic hybridization analysis of 18 cases and review of the literature. Ann. Diagn. Pathol. 2015, 19, 261–268. [Google Scholar] [CrossRef]
- Parada, D.D.; Pena, K.B. Chromophobe renal cell carcinoma with neuroendocrine differentiation. APMIS 2008, 116, 859–865. [Google Scholar] [CrossRef]
- Kuroda, N.; Tamura, M.; Hes, O.; Michal, M.; Gatalica, Z. Chromophobe renal cell carcinoma with neuroendocrine differentiation and sarcomatoid change. Pathol. Int. 2011, 61, 552–554. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, G.A.; Al-Zahrani, R. Chromophobe renal cell carcinoma of the kidney with neuroendocrine differentiation: A case report with review of literature. Urol. Ann. 2015, 7, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Ohe, C.; Kuroda, N.; Matsuura, K.; Kai, T.; Moriyama, M.; Sugiguchi, S.; Terahata, S.; Hosaka, N.; Hes, O.; Michal, M.; et al. Chromophobe renal cell carcinoma with neuroendocrine differentiation/morphology: A clinicopathological and genetic study of three cases. Hum. Pathol. Case Rep. 2014, 1, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Kuroda, N.; Tanaka, A.; Yamaguchi, T.; Kasahara, K.; Naruse, K.; Yamada, Y.; Hatanaka, K.; Shinohara, N.; Nagashima, Y.; Mikami, S.; et al. Chromophobe renal cell carcinoma, oncocytic variant: A proposal of a new variant giving a critical diagnostic pitfall in diagnosing renal oncocytic tumors. Med. Mol. Morphol. 2013, 46, 49–55. [Google Scholar] [CrossRef]
- Speicher, M.R.; Schoell, B.; du Manoir, S.; Schrock, E.; Ried, T.; Cremer, T.; Storkel, S.; Kovacs, A.; Kovacs, G. Specific loss of chromosomes 1, 2, 6, 10, 13, 17, and 21 in chromophobe renal cell carcinomas revealed by comparative genomic hybridization. Am. J. Pathol. 1994, 145, 356–364. [Google Scholar]
- Paner, G.; Amin, M.B.; Moch, H.; Störkel, S. Chromophobe renal cell carcinoma. In WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; Moch, H., Humphrey, P.A., Ulbright, T.M., Reuter, V.E., Eds.; International Agency for Research on Cancer: Lyon, France, 2016; Volume 8, pp. 27–28. [Google Scholar]
- Davis, C.F.; Ricketts, C.J.; Wang, M.; Yang, L.; Cherniack, A.D.; Shen, H.; Buhay, C.; Kang, H.; Kim, S.C.; Fahey, C.C.; et al. The somatic genomic landscape of chromophobe renal cell carcinoma. Cancer Cell 2014, 26, 319–330. [Google Scholar] [CrossRef] [Green Version]
- Vieira, J.; Henrique, R.; Ribeiro, F.R.; Barros-Silva, J.D.; Peixoto, A.; Santos, C.; Pinheiro, M.; Costa, V.L.; Soares, M.J.; Oliveira, J.; et al. Feasibility of differential diagnosis of kidney tumors by comparative genomic hybridization of fine needle aspiration biopsies. Genes Chromosomes Cancer 2010, 49, 935–947. [Google Scholar] [CrossRef]
- Sperga, M.; Martinek, P.; Vanecek, T.; Grossmann, P.; Bauleth, K.; Perez-Montiel, D.; Alvarado-Cabrero, I.; Nevidovska, K.; Lietuvietis, V.; Hora, M.; et al. Chromophobe renal cell carcinoma--chromosomal aberration variability and its relation to Paner grading system: An array CGH and FISH analysis of 37 cases. Virchows Arch. 2013, 463, 563–573. [Google Scholar] [CrossRef]
- Tan, M.H.; Wong, C.F.; Tan, H.L.; Yang, X.J.; Ditlev, J.; Matsuda, D.; Khoo, S.K.; Sugimura, J.; Fujioka, T.; Furge, K.A.; et al. Genomic expression and single-nucleotide polymorphism profiling discriminates chromophobe renal cell carcinoma and oncocytoma. BMC Cancer 2010, 10, 196. [Google Scholar] [CrossRef]
- Crotty, T.B.; Lawrence, K.M.; Moertel, C.A.; Bartelt, D.H., Jr.; Batts, K.P.; Dewald, G.W.; Farrow, G.M.; Jenkins, R.B. Cytogenetic analysis of six renal oncocytomas and a chromophobe cell renal carcinoma. Evidence that -Y, -1 may be a characteristic anomaly in renal oncocytomas. Cancer Genet Cytogenet. 1992, 61, 61–66. [Google Scholar] [CrossRef]
- Fuzesi, L.; Gunawan, B.; Braun, S.; Boeckmann, W. Renal oncocytoma with a translocation t(9;11)(p23;q13). J. Urol. 1994, 152, 471–472. [Google Scholar] [CrossRef]
- Paner, G.P.; Lindgren, V.; Jacobson, K.; Harrison, K.; Cao, Y.; Campbell, S.C.; Flanigan, R.C.; Picken, M.M. High incidence of chromosome 1 abnormalities in a series of 27 renal oncocytomas: Cytogenetic and fluorescence in situ hybridization studies. Arch. Pathol. Lab. Med. 2007, 131, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, V.; Paner, G.P.; Omeroglu, A.; Campbell, S.C.; Waters, W.B.; Flanigan, R.C.; Picken, M.M. Cytogenetic analysis of a series of 13 renal oncocytomas. J. Urol. 2004, 171, 602–604. [Google Scholar] [CrossRef] [PubMed]
- Picken, M.M.; Chyna, B.; Flanigan, R.C.; Lee, J.M. Analysis of chromosome 1p abnormalities in renal oncocytomas by loss of heterozygosity studies: Correlation with conventional cytogenetics and fluorescence in situ hybridization. Am. J. Clin. Pathol. 2008, 129, 377–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, C.B.; Lipsky, M.; Nandula, S.V.; Freeman, C.E.; Matthews, T.; Walsh, C.E.; Li, G.; Szabolcs, M.; Mansukhani, M.M.; McKiernan, J.M.; et al. Cytogenetic analysis of 130 renal oncocytomas identify three distinct and mutually exclusive diagnostic classes of chromosome aberrations. Genes Chromosomes Cancer 2019. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Tolkunov, D.; Aviv, H.; Hakimi, A.A.; Yao, M.; Hsieh, J.J.; Ganesan, S.; Chan, C.S.; White, E. The Genomic Landscape of Renal Oncocytoma Identifies a Metabolic Barrier to Tumorigenesis. Cell Rep. 2015, 13, 1895–1908. [Google Scholar] [CrossRef] [Green Version]
- Sukov, W.R.; Ketterling, R.P.; Lager, D.J.; Carlson, A.W.; Sinnwell, J.P.; Chow, G.K.; Jenkins, R.B.; Cheville, J.C. CCND1 rearrangements and cyclin D1 overexpression in renal oncocytomas: Frequency, clinicopathologic features, and utility in differentiation from chromophobe renal cell carcinoma. Hum. Pathol. 2009, 40, 1296–1303. [Google Scholar] [CrossRef]
- Williamson, S.R.; Eble, J.N.; Cheng, L.; Grignon, D.J. Clear cell papillary renal cell carcinoma: Differential diagnosis and extended immunohistochemical profile. Mod. Pathol. 2013, 26, 697–708. [Google Scholar] [CrossRef] [Green Version]
- Mantilla, J.G.; Antic, T.; Tretiakova, M.S. GATA-3 Is a Specific Marker for Clear Cell Papillary Renal Cell Carcinoma. Mod. Pathol. 2017, 30, 241A. [Google Scholar]
- Martignoni, G.; Brunelli, M.; Segala, D.; Munari, E.; Gobbo, S.; Cima, L.; Borze, I.; Wirtanen, T.; Sarhadi, V.K.; Atanesyan, L.; et al. Validation of 34betaE12 immunoexpression in clear cell papillary renal cell carcinoma as a sensitive biomarker. Pathology 2017, 49, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Hes, O.; Comperat, E.M.; Rioux-Leclercq, N. Clear cell papillary renal cell carcinoma, renal angiomyoadenomatous tumor, and renal cell carcinoma with leiomyomatous stroma relationship of 3 types of renal tumors: A review. Ann. Diagn. Pathol. 2016, 21, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, J.S.; Malik, F.; Amin, M.B.; Argani, P.; Bahrami, A. MiT family translocation renal cell carcinomas: A 15th anniversary update. Histol. Histopathol. 2019, 18159. [Google Scholar] [CrossRef]
- Argani, P.; Antonescu, C.R.; Illei, P.B.; Lui, M.Y.; Timmons, C.F.; Newbury, R.; Reuter, V.E.; Garvin, A.J.; Perez-Atayde, A.R.; Fletcher, J.A.; et al. Primary renal neoplasms with the ASPL-TFE3 gene fusion of alveolar soft part sarcoma: A distinctive tumor entity previously included among renal cell carcinomas of children and adolescents. Am. J. Pathol. 2001, 159, 179–192. [Google Scholar] [CrossRef]
- Argani, P.; Lui, M.Y.; Couturier, J.; Bouvier, R.; Fournet, J.C.; Ladanyi, M. A novel CLTC-TFE3 gene fusion in pediatric renal adenocarcinoma with t(X;17)(p11.2;q23). Oncogene 2003, 22, 5374–5378. [Google Scholar] [CrossRef] [PubMed]
- Argani, P.; Ladanyi, M. Renal carcinomas associated with Xp11.2 translocations / TFE3 gene fusions. In Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs, 1st ed.; Eble, J.N., Sauter, G., Epstein, J.I., Sesterhenn, I.A., Eds.; IARC Press: Lyon, France, 2004; pp. 37–38. [Google Scholar]
- Argani, P.; Olgac, S.; Tickoo, S.K.; Goldfischer, M.; Moch, H.; Chan, D.Y.; Eble, J.N.; Bonsib, S.M.; Jimeno, M.; Lloreta, J.; et al. Xp11 translocation renal cell carcinoma in adults: Expanded clinical, pathologic, and genetic spectrum. Am. J. Surg. Pathol. 2007, 31, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Argani, P.; Hicks, J.; De Marzo, A.M.; Albadine, R.; Illei, P.B.; Ladanyi, M.; Reuter, V.E.; Netto, G.J. Xp11 translocation renal cell carcinoma (RCC): Extended immunohistochemical profile emphasizing novel RCC markers. Am. J. Surg. Pathol. 2010, 34, 1295–1303. [Google Scholar] [CrossRef] [Green Version]
- Ellis, C.L.; Eble, J.N.; Subhawong, A.P.; Martignoni, G.; Zhong, M.; Ladanyi, M.; Epstein, J.I.; Netto, G.J.; Argani, P. Clinical heterogeneity of Xp11 translocation renal cell carcinoma: Impact of fusion subtype, age, and stage. Mod. Pathol. 2014, 27, 875–886. [Google Scholar] [CrossRef] [Green Version]
- Argani, P. MiT family translocation renal cell carcinoma. Semin. Diagn. Pathol. 2015, 32, 103–113. [Google Scholar] [CrossRef]
- Argani, P.; Zhong, M.; Reuter, V.E.; Fallon, J.T.; Epstein, J.I.; Netto, G.J.; Antonescu, C.R. TFE3-Fusion Variant Analysis Defines Specific Clinicopathologic Associations Among Xp11 Translocation Cancers. Am. J. Surg. Pathol. 2016, 40, 723–737. [Google Scholar] [CrossRef] [Green Version]
- Hayes, M.; Peckova, K.; Martinek, P.; Hora, M.; Kalusova, K.; Straka, L.; Daum, O.; Kokoskova, B.; Rotterova, P.; Pivovarcikova, K.; et al. Molecular-genetic analysis is essential for accurate classification of renal carcinoma resembling Xp11.2 translocation carcinoma. Virchows Arch. 2015, 466, 313–322. [Google Scholar] [CrossRef]
- Kato, I.; Furuya, M.; Baba, M.; Kameda, Y.; Yasuda, M.; Nishimoto, K.; Oyama, M.; Yamasaki, T.; Ogawa, O.; Niino, H.; et al. RBM10-TFE3 renal cell carcinoma characterised by paracentric inversion with consistent closely split signals in break-apart fluorescence in-situ hybridisation: Study of 10 cases and a literature review. Histopathology 2019, 75, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Malouf, G.G.; Su, X.; Yao, H.; Gao, J.; Xiong, L.; He, Q.; Comperat, E.; Couturier, J.; Molinie, V.; Escudier, B.; et al. Next-generation sequencing of translocation renal cell carcinoma reveals novel RNA splicing partners and frequent mutations of chromatin-remodeling genes. Clin. Cancer Res. 2014, 20, 4129–4140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thway, K.; du Parcq, J.; Larkin, J.M.; Fisher, C.; Livni, N. Metastatic renal mucinous tubular and spindle cell carcinoma. Atypical behavior of a rare, morphologically bland tumor. Ann. Diagn. Pathol. 2012, 16, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, J.; Amin, M.B.; Selbs, E.; Turi, G.K.; Paner, G.P.; Reuter, V.E. Mucinous tubular and spindle cell carcinoma of the kidney with sarcomatoid change. Am. J. Surg. Pathol. 2009, 33, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Bulimbasic, S.; Ljubanovic, D.; Sima, R.; Michal, M.; Hes, O.; Kuroda, N.; Persec, Z. Aggressive high-grade mucinous tubular and spindle cell carcinoma. Hum. Pathol. 2009, 40, 906–907. [Google Scholar] [CrossRef] [PubMed]
- Paner, G.P.; Srigley, J.R.; Radhakrishnan, A.; Cohen, C.; Skinnider, B.F.; Tickoo, S.K.; Young, A.N.; Amin, M.B. Immunohistochemical analysis of mucinous tubular and spindle cell carcinoma and papillary renal cell carcinoma of the kidney: Significant immunophenotypic overlap warrants diagnostic caution. Am J Surg. Pathol. 2006, 30, 13–19. [Google Scholar] [CrossRef]
- Ren, Q.; Wang, L.; Al-Ahmadie, H.A.; Fine, S.W.; Gopalan, A.; Sirintrapun, S.J.; Tickoo, S.K.; Reuter, V.E.; Chen, Y.B. Distinct Genomic Copy Number Alterations Distinguish Mucinous Tubular and Spindle Cell Carcinoma of the Kidney From Papillary Renal Cell Carcinoma With Overlapping Histologic Features. Am. J. Surg. Pathol. 2018, 42, 767–777. [Google Scholar] [CrossRef]
- Peckova, K.; Martinek, P.; Sperga, M.; Montiel, D.P.; Daum, O.; Rotterova, P.; Kalusova, K.; Hora, M.; Pivovarcikova, K.; Rychly, B.; et al. Mucinous spindle and tubular renal cell carcinoma: Analysis of chromosomal aberration pattern of low-grade, high-grade, and overlapping morphologic variant with papillary renal cell carcinoma. Ann. Diagn. Pathol. 2015, 19, 226–231. [Google Scholar] [CrossRef]
- Sadimin, E.T.; Chen, Y.B.; Wang, L.; Argani, P.; Epstein, J.I. Chromosomal abnormalities of high-grade mucinous tubular and spindle cell carcinoma of the kidney. Histopathology 2017, 71, 719–724. [Google Scholar] [CrossRef]
- Cossu-Rocca, P.; Eble, J.N.; Delahunt, B.; Zhang, S.; Martignoni, G.; Brunelli, M.; Cheng, L. Renal mucinous tubular and spindle carcinoma lacks the gains of chromosomes 7 and 17 and losses of chromosome Y that are prevalent in papillary renal cell carcinoma. Mod. Pathol. 2006, 19, 488–493. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Yang, X.J.; Lopez, J.I.; Shah, R.B.; Hes, O.; Shen, S.S.; Li, R.; Yang, Y.; Lin, F.; Elson, P.; et al. Renal tubulocystic carcinoma is closely related to papillary renal cell carcinoma: Implications for pathologic classification. Am. J. Surg. Pathol. 2009, 33, 1840–1849. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.; Jones, C.L.; Williamson, S.R.; Eble, J.N.; Grignon, D.J.; Zhang, S.; Wang, M.; Baldridge, L.A.; Wang, L.; Montironi, R.; et al. Tubulocystic renal cell carcinoma is an entity that is immunohistochemically and genetically distinct from papillary renal cell carcinoma. Histopathology 2016, 68, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.J.; Zhou, M.; Hes, O.; Shen, S.; Li, R.; Lopez, J.; Shah, R.B.; Yang, Y.; Chuang, S.T.; Lin, F.; et al. Tubulocystic carcinoma of the kidney: Clinicopathologic and molecular characterization. Am. J. Surg. Pathol. 2008, 32, 177–187. [Google Scholar] [CrossRef]
- Sarungbam, J.; Mehra, R.; Tomlins, S.A.; Smith, S.C.; Jayakumaran, G.; Al-Ahmadie, H.; Gopalan, A.; Sirintrapun, S.J.; Fine, S.W.; Zhang, Y.; et al. Tubulocystic renal cell carcinoma: A distinct clinicopathologic entity with a characteristic genomic profile. Mod. Pathol. 2019, 32, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Al-Hussain, T.O.; Cheng, L.; Zhang, S.; Epstein, J.I. Tubulocystic carcinoma of the kidney with poorly differentiated foci: A series of 3 cases with fluorescence in situ hybridization analysis. Hum. Pathol. 2013, 44, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C.; Trpkov, K.; Chen, Y.B.; Mehra, R.; Sirohi, D.; Ohe, C.; Cani, A.K.; Hovelson, D.H.; Omata, K.; McHugh, J.B.; et al. Tubulocystic Carcinoma of the Kidney With Poorly Differentiated Foci: A Frequent Morphologic Pattern of Fumarate Hydratase-deficient Renal Cell Carcinoma. Am. J. Surg. Pathol. 2016, 40, 1457–1472. [Google Scholar] [CrossRef]
- Kuroda, N.; Ohe, C.; Mikami, S.; Hes, O.; Michal, M.; Brunelli, M.; Martignoni, G.; Sato, Y.; Yoshino, T.; Kakehi, Y.; et al. Review of acquired cystic disease-associated renal cell carcinoma with focus on pathobiological aspects. Histol. Histopathol. 2011, 26, 1215–1218. [Google Scholar] [CrossRef]
- Kuroda, N.; Shiotsu, T.; Hes, O.; Michal, M.; Shuin, T.; Lee, G.H. Acquired cystic disease-associated renal cell carcinoma with gain of chromosomes 3, 7, and 16, gain of chromosome X, and loss of chromosome Y. Med. Mol. Morphol. 2010, 43, 231–234. [Google Scholar] [CrossRef]
- Kuroda, N.; Tamura, M.; Hamaguchi, N.; Mikami, S.; Pan, C.C.; Brunelli, M.; Martignoni, G.; Hes, O.; Michal, M.; Lee, G.H. Acquired cystic disease-associated renal cell carcinoma with sarcomatoid change and rhabdoid features. Ann. Diagn. Pathol. 2011, 15, 462–466. [Google Scholar] [CrossRef]
- Kuroda, N.; Yamashita, M.; Kakehi, Y.; Hes, O.; Michal, M.; Lee, G.H. Acquired cystic disease-associated renal cell carcinoma: An immunohistochemical and fluorescence in situ hybridization study. Med. Mol. Morphol. 2011, 44, 228–232. [Google Scholar] [CrossRef]
- Cossu-Rocca, P.; Eble, J.N.; Zhang, S.; Martignoni, G.; Brunelli, M.; Cheng, L. Acquired cystic disease-associated renal tumors: An immunohistochemical and fluorescence in situ hybridization study. Mod. Pathol. 2006, 19, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, E.; Yusenko, M.V.; Nagy, A.; Kovacs, G. Oligoarray comparative genomic hybridization of renal cell tumors that developed in patients with acquired cystic renal disease. Hum. Pathol. 2010, 41, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Ohe, C.; Smith, S.C.; Sirohi, D.; Divatia, M.; de Peralta-Venturina, M.; Paner, G.P.; Agaimy, A.; Amin, M.B.; Argani, P.; Chen, Y.B.; et al. Reappraisal of Morphologic Differences Between Renal Medullary Carcinoma, Collecting Duct Carcinoma, and Fumarate Hydratase-deficient Renal Cell Carcinoma. Am. J. Surg. Pathol. 2018, 42, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Carlo, M.I.; Khan, H.; Nanjangud, G.J.; Rana, S.; Cimera, R.; Zhang, Y.; Hakimi, A.A.; Verma, A.K.; Al-Ahmadie, H.A.; et al. Distinctive mechanisms underlie the loss of SMARCB1 protein expression in renal medullary carcinoma: Morphologic and molecular analysis of 20 cases. Mod. Pathol. 2019, 32, 1329–1343. [Google Scholar] [CrossRef]
- Calderaro, J.; Masliah-Planchon, J.; Richer, W.; Maillot, L.; Maille, P.; Mansuy, L.; Bastien, C.; de la Taille, A.; Boussion, H.; Charpy, C.; et al. Balanced Translocations Disrupting SMARCB1 Are Hallmark Recurrent Genetic Alterations in Renal Medullary Carcinomas. Eur. Urol. 2016, 69, 1055–1061. [Google Scholar] [CrossRef]
- Carlo, M.I.; Chaim, J.; Patil, S.; Kemel, Y.; Schram, A.M.; Woo, K.; Coskey, D.; Nanjangud, G.J.; Voss, M.H.; Feldman, D.R.; et al. Genomic Characterization of Renal Medullary Carcinoma and Treatment Outcomes. Clin. Genitourin. Cancer 2017, 15, e987–e994. [Google Scholar] [CrossRef]
- Calderaro, J.; Moroch, J.; Pierron, G.; Pedeutour, F.; Grison, C.; Maille, P.; Soyeux, P.; de la Taille, A.; Couturier, J.; Vieillefond, A.; et al. SMARCB1/INI1 inactivation in renal medullary carcinoma. Histopathology 2012, 61, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Galli, S.; Srinivasan, R.; Linehan, W.M.; Tsokos, M.; Merino, M.J. Renal medullary carcinoma: Molecular, immunohistochemistry, and morphologic correlation. Am. J. Surg. Pathol. 2013, 37, 368–374. [Google Scholar] [CrossRef]
- Cheng, J.X.; Tretiakova, M.; Gong, C.; Mandal, S.; Krausz, T.; Taxy, J.B. Renal medullary carcinoma: Rhabdoid features and the absence of INI1 expression as markers of aggressive behavior. Mod. Pathol. 2008, 21, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.; Tannir, N.M.; Tamboli, P. Expression of OCT3/4 in renal medullary carcinoma represents a potential diagnostic pitfall. Am. J. Surg. Pathol. 2012, 36, 583–588. [Google Scholar] [CrossRef]
- Sirohi, D.; Smith, S.C.; Ohe, C.; Colombo, P.; Divatia, M.; Dragoescu, E.; Rao, P.; Hirsch, M.S.; Chen, Y.B.; Mehra, R.; et al. Renal cell carcinoma, unclassified with medullary phenotype: Poorly differentiated adenocarcinomas overlapping with renal medullary carcinoma. Hum. Pathol. 2017, 67, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Smith, S.C.; Agaimy, A.; Argani, P.; Comperat, E.M.; Delahunt, B.; Epstein, J.I.; Eble, J.N.; Grignon, D.J.; Hartmann, A.; et al. Collecting duct carcinoma versus renal medullary carcinoma: An appeal for nosologic and biological clarity. Am. J. Surg. Pathol. 2014, 38, 871–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, A.J. Succinate dehydrogenase (SDH) and mitochondrial driven neoplasia. Pathology 2012, 44, 285–292. [Google Scholar] [CrossRef]
- Gill, A.J. Succinate dehydrogenase (SDH)-deficient neoplasia. Histopathology 2018, 72, 106–116. [Google Scholar] [CrossRef]
- Gill, A.J.; Benn, D.E.; Chou, A.; Clarkson, A.; Muljono, A.; Meyer-Rochow, G.Y.; Richardson, A.L.; Sidhu, S.B.; Robinson, B.G.; Clifton-Bligh, R.J. Immunohistochemistry for SDHB triages genetic testing of SDHB, SDHC, and SDHD in paraganglioma-pheochromocytoma syndromes. Hum. Pathol. 2010, 41, 805–814. [Google Scholar] [CrossRef] [PubMed]
- van Nederveen, F.H.; Gaal, J.; Favier, J.; Korpershoek, E.; Oldenburg, R.A.; de Bruyn, E.M.; Sleddens, H.F.; Derkx, P.; Riviere, J.; Dannenberg, H.; et al. An immunohistochemical procedure to detect patients with paraganglioma and phaeochromocytoma with germline SDHB, SDHC, or SDHD gene mutations: A retrospective and prospective analysis. Lancet Oncol. 2009, 10, 764–771. [Google Scholar] [CrossRef] [Green Version]
- Merino, M.J.; Linehan, W.M. Hereditary leiomyomatosis and renal cell carcinoma (HLRCC)-associated renal cell carcinoma. In WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; Moch, H., Humphrey, P.A., Ulbright, T.M., Reuter, V.E., Eds.; International Agency for Research on Cancer: Lyon, France, 2016; Volume 8, pp. 25–26. [Google Scholar]
- Trpkov, K.; Hes, O.; Agaimy, A.; Bonert, M.; Martinek, P.; Magi-Galluzzi, C.; Kristiansen, G.; Luders, C.; Nesi, G.; Comperat, E.; et al. Fumarate Hydratase-deficient Renal Cell Carcinoma Is Strongly Correlated With Fumarate Hydratase Mutation and Hereditary Leiomyomatosis and Renal Cell Carcinoma Syndrome. Am. J. Surg. Pathol. 2016, 40, 865–875. [Google Scholar] [CrossRef]
- Pivovarcikova, K.; Martinek, P.; Grossmann, P.; Trpkov, K.; Alaghehbandan, R.; Magi-Galluzzi, C.; Pane Foix, M.; Condom Mundo, E.; Berney, D.; Gill, A.; et al. Fumarate hydratase deficient renal cell carcinoma: Chromosomal numerical aberration analysis of 12 cases. Ann. Diagn. Pathol. 2019, 39, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.D.; Chan, E.; Fan, A.C.; Kunder, C.A.; Williamson, S.R.; Zhou, M.; Idrees, M.T.; Maclean, F.M.; Gill, A.J.; Kao, C.S. A Clinicopathologic and Molecular Analysis of Fumarate Hydratase-Deficient Renal Cell Carcinoma in 32 Patients. Am. J. Surg. Pathol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Shyu, I.; Mirsadraei, L.; Wang, X.; Robila, V.; Mehra, R.; McHugh, J.B.; Chen, Y.B.; Udager, A.M.; Gill, A.J.; Cheng, L.; et al. Clues to recognition of fumarate hydratase-deficient renal cell carcinoma: Findings from cytologic and limited biopsy samples. Cancer Cytopathol. 2018. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.B.; Brannon, A.R.; Toubaji, A.; Dudas, M.E.; Won, H.H.; Al-Ahmadie, H.A.; Fine, S.W.; Gopalan, A.; Frizzell, N.; Voss, M.H.; et al. Hereditary leiomyomatosis and renal cell carcinoma syndrome-associated renal cancer: Recognition of the syndrome by pathologic features and the utility of detecting aberrant succination by immunohistochemistry. Am. J. Surg. Pathol. 2014, 38, 627–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, M.; Guillaud-Bataille, M.; Salleron, J.; Genestie, C.; Deveaux, S.; Slama, A.; de Paillerets, B.B.; Richard, S.; Benusiglio, P.R.; Ferlicot, S. Pattern multiplicity and fumarate hydratase (FH)/S-(2-succino)-cysteine (2SC) staining but not eosinophilic nucleoli with perinucleolar halos differentiate hereditary leiomyomatosis and renal cell carcinoma-associated renal cell carcinomas from kidney tumors without FH gene alteration. Mod. Pathol. 2018, 31, 974–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, W.J.; Andrici, J.; Maclean, F.; Madadi-Ghahan, R.; Farzin, M.; Sioson, L.; Toon, C.W.; Clarkson, A.; Watson, N.; Pickett, J.; et al. Fumarate Hydratase-deficient Uterine Leiomyomas Occur in Both the Syndromic and Sporadic Settings. Am. J. Surg. Pathol. 2016, 40, 599–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, J.; Tretiakova, M.S.; Troxell, M.L.; Osunkoya, A.O.; Fadare, O.; Sangoi, A.R.; Shen, S.S.; Lopez-Beltran, A.; Mehra, R.; Heider, A.; et al. Tuberous sclerosis-associated renal cell carcinoma: A clinicopathologic study of 57 separate carcinomas in 18 patients. Am. J. Surg. Pathol. 2014, 38, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Cornejo, K.M.; Sadow, P.M.; Cheng, L.; Wang, M.; Xiao, Y.; Jiang, Z.; Oliva, E.; Jozwiak, S.; Nussbaum, R.L.; et al. Renal cell carcinoma in tuberous sclerosis complex. Am. J. Surg. Pathol. 2014, 38, 895–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trpkov, K.; Hes, O.; Bonert, M.; Lopez, J.I.; Bonsib, S.M.; Nesi, G.; Comperat, E.; Sibony, M.; Berney, D.M.; Martinek, P.; et al. Eosinophilic, Solid, and Cystic Renal Cell Carcinoma: Clinicopathologic Study of 16 Unique, Sporadic Neoplasms Occurring in Women. Am. J. Surg. Pathol. 2016, 40, 60–71. [Google Scholar] [CrossRef]
- Mehra, R.; Vats, P.; Cao, X.; Su, F.; Lee, N.D.; Lonigro, R.; Premkumar, K.; Trpkov, K.; McKenney, J.K.; Dhanasekaran, S.M.; et al. Somatic Bi-allelic Loss of TSC Genes in Eosinophilic Solid and Cystic Renal Cell Carcinoma. Eur. Urol. 2018, 74, 483–486. [Google Scholar] [CrossRef]
- Palsgrove, D.N.; Li, Y.; Pratilas, C.A.; Lin, M.T.; Pallavajjalla, A.; Gocke, C.; De Marzo, A.M.; Matoso, A.; Netto, G.J.; Epstein, J.I.; et al. Eosinophilic Solid and Cystic (ESC) Renal Cell Carcinomas Harbor TSC Mutations: Molecular Analysis Supports an Expanding Clinicopathologic Spectrum. Am. J. Surg. Pathol. 2018, 42, 1166–1181. [Google Scholar] [CrossRef]
- Parilla, M.; Kadri, S.; Patil, S.A.; Ritterhouse, L.; Segal, J.; Henriksen, K.J.; Antic, T. Are Sporadic Eosinophilic Solid and Cystic Renal Cell Carcinomas Characterized by Somatic Tuberous Sclerosis Gene Mutations? Am. J. Surg. Pathol. 2018, 42, 911–917. [Google Scholar] [CrossRef]
- Tretiakova, M.S. Eosinophilic solid and cystic renal cell carcinoma mimicking epithelioid angiomyolipoma: Series of 4 primary tumors and 2 metastases. Hum. Pathol. 2018, 80, 65–75. [Google Scholar] [CrossRef]
- Li, Y.; Reuter, V.E.; Matoso, A.; Netto, G.J.; Epstein, J.I.; Argani, P. Re-evaluation of 33 ‘unclassified’ eosinophilic renal cell carcinomas in young patients. Histopathology 2018, 72, 588–600. [Google Scholar] [CrossRef] [PubMed]
- Williamson, S.R. Renal cell carcinomas with a mesenchymal stromal component: What do we know so far? Pathology 2019, 51, 453–462. [Google Scholar] [CrossRef]
- Williamson, S.R.; Hornick, J.L.; Eble, J.N.; Gupta, N.S.; Rogers, C.G.; True, L.; Grignon, D.J.; Cheng, L. Renal cell carcinoma with angioleiomyoma-like stroma and clear cell papillary renal cell carcinoma: Exploring SDHB protein immunohistochemistry and the relationship to tuberous sclerosis complex. Hum. Pathol. 2018, 75, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Parilla, M.; Alikhan, M.; Al-Kawaaz, M.; Patil, S.; Kadri, S.; Ritterhouse, L.L.; Segal, J.; Fitzpatrick, C.; Antic, T. Genetic Underpinnings of Renal Cell Carcinoma With Leiomyomatous Stroma. Am. J. Surg. Pathol. 2019, 43, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Verkarre, V.; Mensah, A.; Leroy, X.; Sibony, M.; Vasiliu, V.; Comperat, E.; Richard, S.; Mejean, A. A Clinico-Pathologic Study of 17 Patients with Renal Cell Carcinoma Associated With Leiomyomatous Stroma Identifies a Strong Association With Tuberous Sclerosis. Lab. Invest 2015, 95, 266A. [Google Scholar]
- Jia, L.; Jayakumaran, G.; Al-Ahmadie, H.; Fine, S.W.; Gopalan, A.; Sirintrapun, S.J.; Tickoo, S.; Reuter, V.; Cheng, Y.B. Expanding the Morphologic Spectrum of Sporadic Renal Cell Carcinoma (RCC) Harboring Somatic TSC or MTOR Alterations: Analysis of 8 Cases with Clear Cytoplasm and Leiomyomatous Stroma. Mod. Pathol. 2019, 32, 78–79. [Google Scholar]
- Chen, Y.B.; Mirsadraei, L.; Jayakumaran, G.; Al-Ahmadie, H.A.; Fine, S.W.; Gopalan, A.; Sirintrapun, S.J.; Tickoo, S.K.; Reuter, V.E. Somatic Mutations of TSC2 or MTOR Characterize a Morphologically Distinct Subset of Sporadic Renal Cell Carcinoma with Eosinophilic and Vacuolated Cytoplasm. Am. J. Surg. Pathol. 2019, 43, 121–131. [Google Scholar] [CrossRef]
- He, H.; Trpkov, K.; Martinek, P.; Isikci, O.T.; Maggi-Galuzzi, C.; Alaghehbandan, R.; Gill, A.J.; Tretiakova, M.; Lopez, J.I.; Williamson, S.R.; et al. “High-grade oncocytic renal tumor”: Morphologic, immunohistochemical, and molecular genetic study of 14 cases. Virchows Arch. 2018, 473, 725–738. [Google Scholar] [CrossRef]
- Trpkov, K.; Bonert, M.; Gao, Y.; Kapoor, A.; He, H.; Yilmaz, A.; Gill, A.J.; Williamson, S.R.; Comperat, E.; Tretiakova, M.; et al. High-grade oncocytic tumour (HOT) of kidney in a patient with tuberous sclerosis complex. Histopathology 2019, 75, 440–442. [Google Scholar] [CrossRef]
- Hakimi, A.A.; Tickoo, S.K.; Jacobsen, A.; Sarungbam, J.; Sfakianos, J.P.; Sato, Y.; Morikawa, T.; Kume, H.; Fukayama, M.; Homma, Y.; et al. TCEB1-mutated renal cell carcinoma: A distinct genomic and morphological subtype. Mod. Pathol. 2015, 28, 845–853. [Google Scholar] [CrossRef] [Green Version]
- Favazza, L.; Chitale, D.A.; Barod, R.; Rogers, C.G.; Kalyana-Sundaram, S.; Palanisamy, N.; Gupta, N.S.; Williamson, S.R. Renal cell tumors with clear cell histology and intact VHL and chromosome 3p: A histological review of tumors from the Cancer Genome Atlas database. Mod. Pathol. 2017, 30, 1603–1612. [Google Scholar] [CrossRef]
- Hirsch, M.S.; Barletta, J.A.; Gorman, M.; Dal Cin, P. Renal Cell Carcinoma With Monosomy 8 and CAIX Expression: A Distinct Entity or Another Member or the Clear Cell Tubulopapillary RCC/RAT Family? Mod. Pathol. 2015, 28, 229A. [Google Scholar]
- Williamson, S.R.; Grignon, D.J.; Cheng, L.; Favazza, L.; Gondim, D.D.; Carskadon, S.; Gupta, N.S.; Chitale, D.A.; Kalyana-Sundaram, S.; Palanisamy, N. Renal Cell Carcinoma With Chromosome 6p Amplification Including the TFEB Gene: A Novel Mechanism of Tumor Pathogenesis? Am. J. Surg. Pathol. 2017, 41, 287–298. [Google Scholar] [CrossRef]
- Argani, P.; Reuter, V.E.; Zhang, L.; Sung, Y.S.; Ning, Y.; Epstein, J.I.; Netto, G.J.; Antonescu, C.R. TFEB-amplified Renal Cell Carcinomas: An Aggressive Molecular Subset Demonstrating Variable Melanocytic Marker Expression and Morphologic Heterogeneity. Am. J. Surg. Pathol. 2016, 40, 1484–1495. [Google Scholar] [CrossRef]
- Gupta, S.; Johnson, S.H.; Vasmatzis, G.; Porath, B.; Rustin, J.G.; Rao, P.; Costello, B.A.; Leibovich, B.C.; Thompson, R.H.; Cheville, J.C.; et al. TFEB-VEGFA (6p21.1) co-amplified renal cell carcinoma: A distinct entity with potential implications for clinical management. Mod. Pathol. 2017, 30, 998–1012. [Google Scholar] [CrossRef] [Green Version]
- Peckova, K.; Vanecek, T.; Martinek, P.; Spagnolo, D.; Kuroda, N.; Brunelli, M.; Vranic, S.; Djuricic, S.; Rotterova, P.; Daum, O.; et al. Aggressive and nonaggressive translocation t(6;11) renal cell carcinoma: Comparative study of 6 cases and review of the literature. Ann. Diagn. Pathol. 2014, 18, 351–357. [Google Scholar] [CrossRef]
- Skala, S.L.; Xiao, H.; Udager, A.M.; Dhanasekaran, S.M.; Shukla, S.; Zhang, Y.; Landau, C.; Shao, L.; Roulston, D.; Wang, L.; et al. Detection of 6 TFEB-amplified renal cell carcinomas and 25 renal cell carcinomas with MITF translocations: Systematic morphologic analysis of 85 cases evaluated by clinical TFE3 and TFEB FISH assays. Mod. Pathol. 2018, 31, 179–197. [Google Scholar] [CrossRef]
- Durinck, S.; Stawiski, E.W.; Pavia-Jimenez, A.; Modrusan, Z.; Kapur, P.; Jaiswal, B.S.; Zhang, N.; Toffessi-Tcheuyap, V.; Nguyen, T.T.; Pahuja, K.B.; et al. Spectrum of diverse genomic alterations define non-clear cell renal carcinoma subtypes. Nat. Genet. 2015, 47, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Argani, P.; Jungbluth, A.A.; Chen, Y.B.; Tickoo, S.K.; Fine, S.W.; Gopalan, A.; Al-Ahmadie, H.A.; Sirintrapun, S.J.; Sanchez, A.; et al. TFEB Expression Profiling in Renal Cell Carcinomas: Clinicopathologic Correlations. Am. J. Surg. Pathol. 2019, 43, 1445–1461. [Google Scholar] [CrossRef]
- Andeen, N.K.; Qu, X.; Antic, T.; Tykodi, S.S.; Fang, M.; Tretiakova, M.S. Clinical Utility of Chromosome Genomic Array Testing for Unclassified and Advanced-Stage Renal Cell Carcinomas. Arch. Pathol. Lab. Med. 2019, 143, 494–504. [Google Scholar] [CrossRef]
- Moch, H.; Amin, M.; Argani, P.; Cheville, J.; Delahunt, B.; Martignoni, G.; Srigley, J.; Tan, P.; Tickoo, S. Renal cell tumors. In WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; Moch, H., Humphrey, P.A., Ulbright, T.M., Reuter, V.E., Eds.; International Agency for Research on Cancer: Lyon, France, 2016; pp. 14–17. [Google Scholar]
- Debelenko, L.V.; Raimondi, S.C.; Daw, N.; Shivakumar, B.R.; Huang, D.; Nelson, M.; Bridge, J.A. Renal cell carcinoma with novel VCL-ALK fusion: New representative of ALK-associated tumor spectrum. Mod. Pathol. 2011, 24, 430–442. [Google Scholar] [CrossRef] [Green Version]
- Sugawara, E.; Togashi, Y.; Kuroda, N.; Sakata, S.; Hatano, S.; Asaka, R.; Yuasa, T.; Yonese, J.; Kitagawa, M.; Mano, H.; et al. Identification of anaplastic lymphoma kinase fusions in renal cancer: Large-scale immunohistochemical screening by the intercalated antibody-enhanced polymer method. Cancer 2012, 118, 4427–4436. [Google Scholar] [CrossRef]
- Sukov, W.R.; Hodge, J.C.; Lohse, C.M.; Akre, M.K.; Leibovich, B.C.; Thompson, R.H.; Cheville, J.C. ALK alterations in adult renal cell carcinoma: Frequency, clinicopathologic features and outcome in a large series of consecutively treated patients. Mod. Pathol. 2012, 25, 1516–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodokh, Y.; Ambrosetti, D.; Kubiniek, V.; Tibi, B.; Durand, M.; Amiel, J.; Pertuit, M.; Barlier, A.; Pedeutour, F. ALK-TPM3 rearrangement in adult renal cell carcinoma: Report of a new case showing loss of chromosome 3 and literature review. Cancer Genet. 2018, 221, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Cajaiba, M.M.; Jennings, L.J.; George, D.; Perlman, E.J. Expanding the spectrum of ALK-rearranged renal cell carcinomas in children: Identification of a novel HOOK1-ALK fusion transcript. Genes Chromosomes Cancer 2016, 55, 814–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cajaiba, M.M.; Jennings, L.J.; Rohan, S.M.; Perez-Atayde, A.R.; Marino-Enriquez, A.; Fletcher, J.A.; Geller, J.I.; Leuer, K.M.; Bridge, J.A.; Perlman, E.J. ALK-rearranged renal cell carcinomas in children. Genes Chromosomes Cancer 2016, 55, 442–451. [Google Scholar] [CrossRef]
- Hodge, J.C.; Pearce, K.E.; Sukov, W.R. Distinct ALK-rearranged and VCL-negative papillary renal cell carcinoma variant in two adults without sickle cell trait. Mod. Pathol. 2013, 26, 604–605. [Google Scholar] [CrossRef] [Green Version]
- Jeanneau, M.; Gregoire, V.; Desplechain, C.; Escande, F.; Tica, D.P.; Aubert, S.; Leroy, X. ALK rearrangements-associated renal cell carcinoma (RCC) with unique pathological features in an adult. Pathol. Res. Pr. 2016, 212, 1064–1066. [Google Scholar] [CrossRef]
- Kuroda, N.; Liu, Y.; Tretiakova, M.; Ulamec, M.; Takeuchi, K.; Przybycin, C.; Magi-Galluzzi, C.; Agaimy, A.; Yilmaz, A.; Trpkov, K.; et al. Clinicopathological Study of Seven Cases of ALK-positive Renal Tumor Identification of New Fusion Partners including CLIP1 and KIF5B Genes. Mod. Pathol. 2019, 32, 85. [Google Scholar]
- Kuroda, N.; Sugawara, E.; Kusano, H.; Yuba, Y.; Yorita, K.; Takeuchi, K. A review of ALK-rearranged renal cell carcinomas with a focus on clinical and pathobiological aspects. Pol. J. Pathol. 2018, 69, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Kusano, H.; Togashi, Y.; Akiba, J.; Moriya, F.; Baba, K.; Matsuzaki, N.; Yuba, Y.; Shiraishi, Y.; Kanamaru, H.; Kuroda, N.; et al. Two Cases of Renal Cell Carcinoma Harboring a Novel STRN-ALK Fusion Gene. Am. J. Surg. Pathol. 2016, 40, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Park, J.W.; Suh, J.H.; Nam, K.H.; Moon, K.C. ALK-Positive Renal Cell Carcinoma in a Large Series of Consecutively Resected Korean Renal Cell Carcinoma Patients. Korean J. Pathol. 2013, 47, 452–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino-Enriquez, A.; Ou, W.B.; Weldon, C.B.; Fletcher, J.A.; Perez-Atayde, A.R. ALK rearrangement in sickle cell trait-associated renal medullary carcinoma. Genes Chromosomes Cancer 2011, 50, 146–153. [Google Scholar] [CrossRef]
- Pal, S.K.; Bergerot, P.; Dizman, N.; Bergerot, C.; Adashek, J.; Madison, R.; Chung, J.H.; Ali, S.M.; Jones, J.O.; Salgia, R. Responses to Alectinib in ALK-rearranged Papillary Renal Cell Carcinoma. Eur. Urol. 2018, 74, 124–128. [Google Scholar] [CrossRef]
- Smith, N.E.; Deyrup, A.T.; Marino-Enriquez, A.; Fletcher, J.A.; Bridge, J.A.; Illei, P.B.; Netto, G.J.; Argani, P. VCL-ALK renal cell carcinoma in children with sickle-cell trait: The eighth sickle-cell nephropathy? Am. J. Surg. Pathol. 2014, 38, 858–863. [Google Scholar] [CrossRef] [Green Version]
- Thorner, P.S.; Shago, M.; Marrano, P.; Shaikh, F.; Somers, G.R. TFE3-positive renal cell carcinomas are not always Xp11 translocation carcinomas: Report of a case with a TPM3-ALK translocation. Pathol. Res. Pr. 2016, 212, 937–942. [Google Scholar] [CrossRef]
- Yu, W.; Wang, Y.; Jiang, Y.; Zhang, W.; Li, Y. Genetic analysis and clinicopathological features of ALK-rearranged renal cell carcinoma in a large series of resected Chinese renal cell carcinoma patients and literature review. Histopathology 2017, 71, 53–62. [Google Scholar] [CrossRef]
- Cheng, J.; Zhang, J.; Han, Y.; Wang, X.; Ye, X.; Meng, Y.; Parwani, A.; Han, Z.; Feng, Q.; Huang, K. Integrative Analysis of Histopathological Images and Genomic Data Predicts Clear Cell Renal Cell Carcinoma Prognosis. Cancer Res. 2017, 77, e91–e100. [Google Scholar] [CrossRef] [Green Version]
- Shao, W.; Han, Z.; Cheng, J.; Cheng, L.; Wang, T.; Sun, L.; Lu, Z.; Zhang, J.; Zhang, D.; Huang, K. Integrative analysis of pathological images and multi-dimensional genomic data for early-stage cancer prognosis. Ieee Trans. Med. Imaging 2019. [Google Scholar] [CrossRef]
Figure 1.
Some renal cell carcinomas (RCCs) with TFEB translocation lack typical morphology with pseudorosettes and rather show solid architecture. 4× magnification.
Figure 1.
Some renal cell carcinomas (RCCs) with TFEB translocation lack typical morphology with pseudorosettes and rather show solid architecture. 4× magnification.

Figure 2.
SDHB-deficient RCC with typical morphology-eosinophilic renal tumor with numerous vacuoles resembling texture of bubble wrap. 10× magnification.
Figure 2.
SDHB-deficient RCC with typical morphology-eosinophilic renal tumor with numerous vacuoles resembling texture of bubble wrap. 10× magnification.

Figure 3.
FH-deficient RCC: deep red macronucleoli can be prominent (A), however in some cases it is not easy to detect them (B). 4× magnification.
Figure 3.
FH-deficient RCC: deep red macronucleoli can be prominent (A), however in some cases it is not easy to detect them (B). 4× magnification.


Figure 4.
RCC with TFEB break and TFEB amplification. 4× magnification.


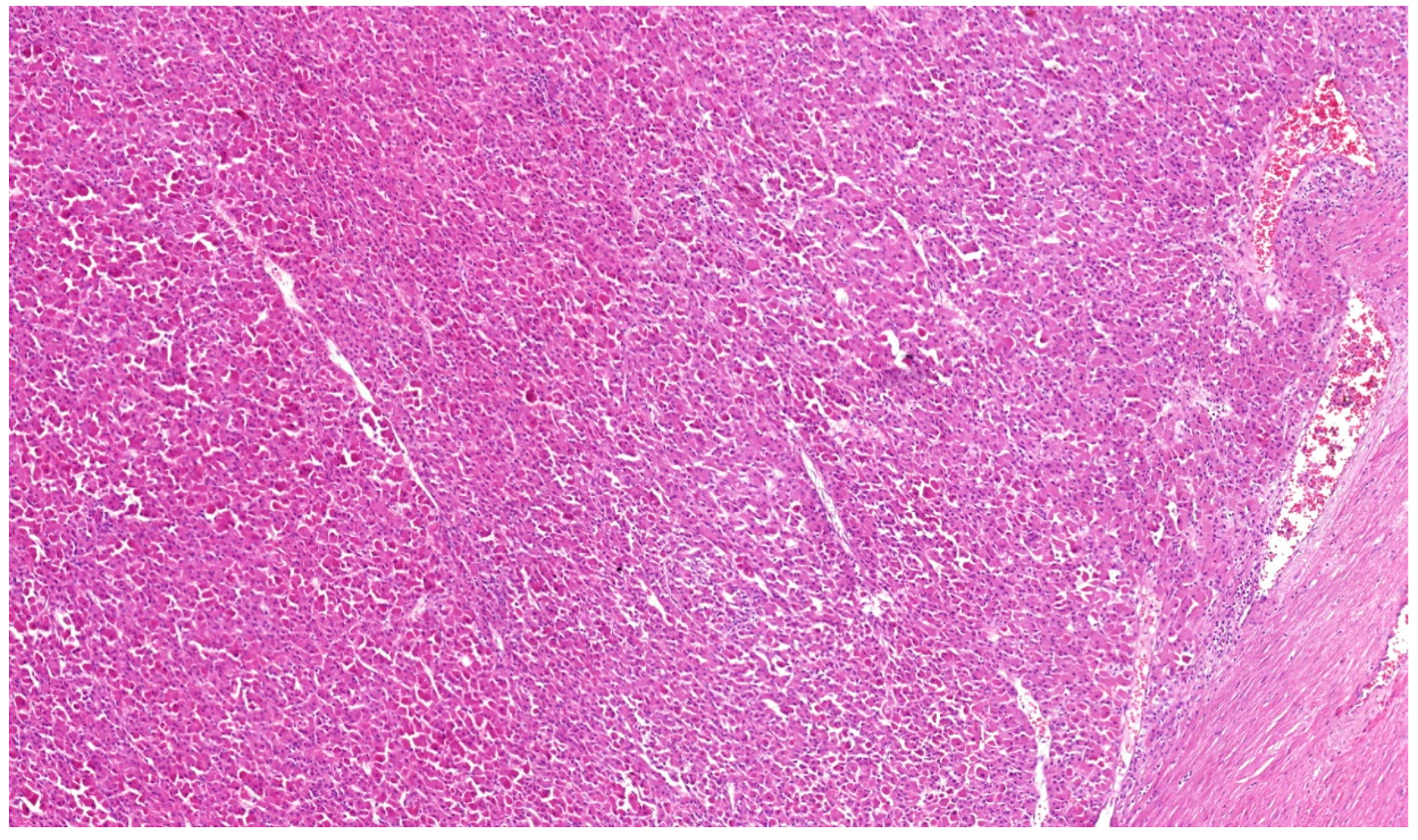{kind=link}
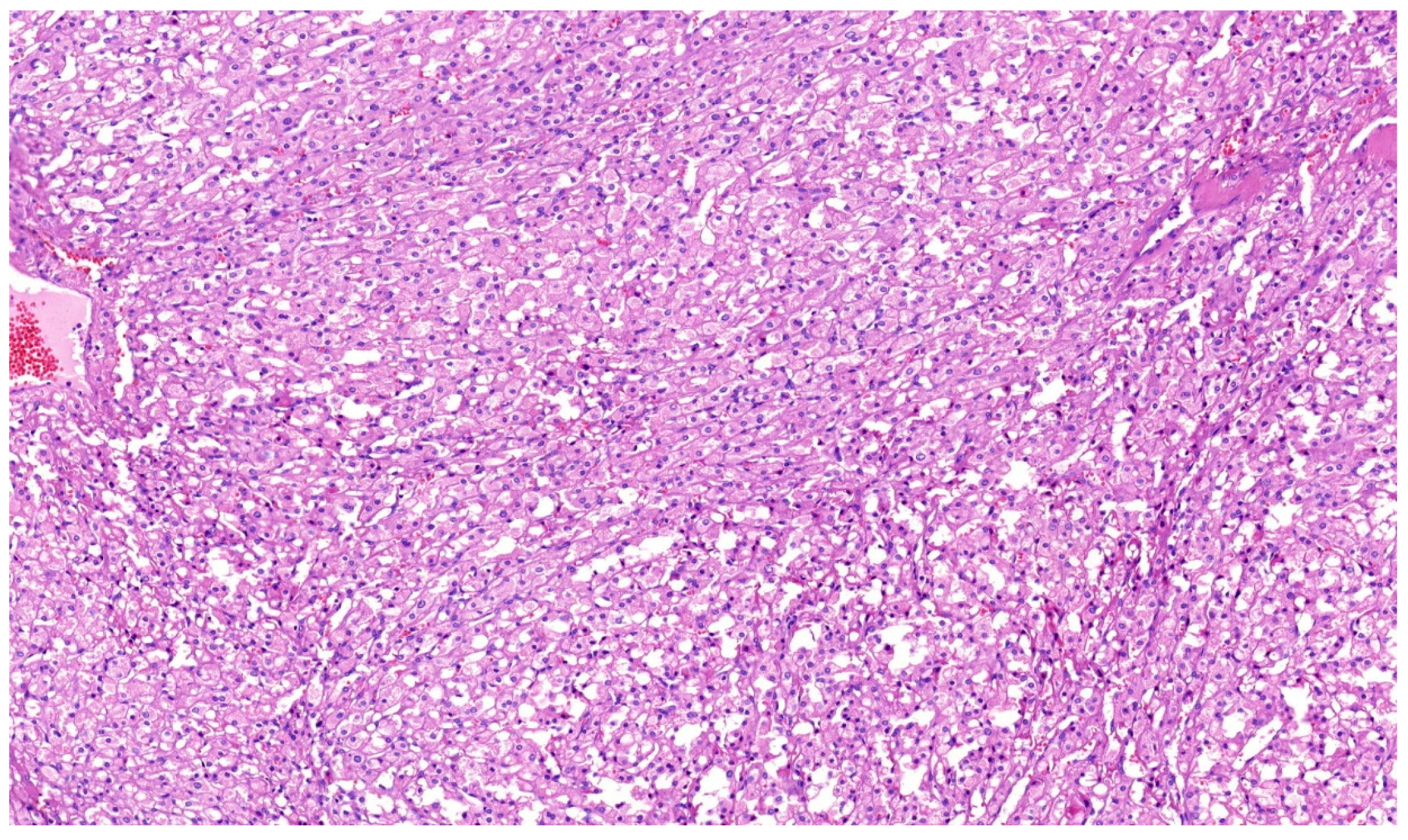{kind=link}
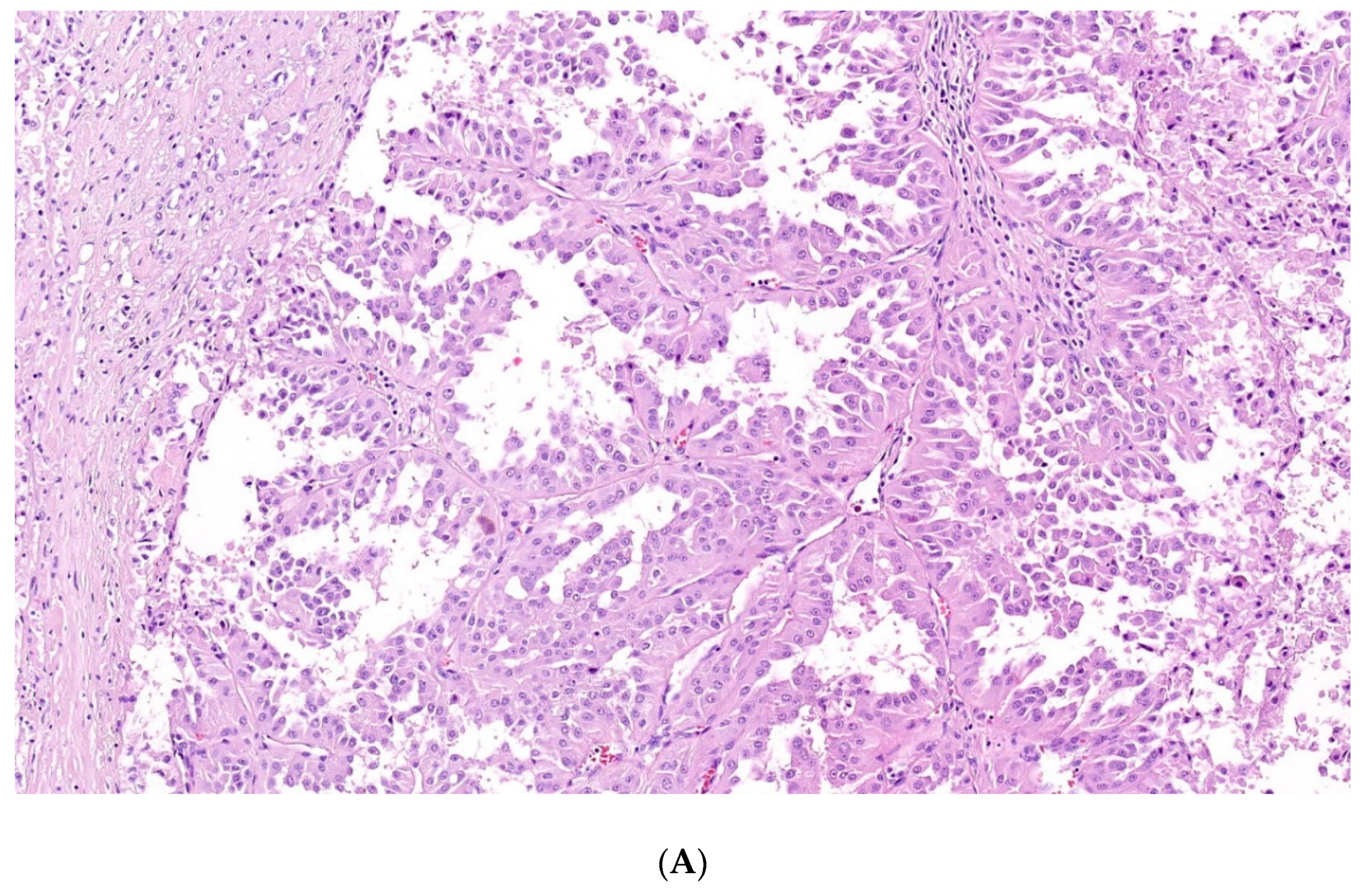{kind=link}
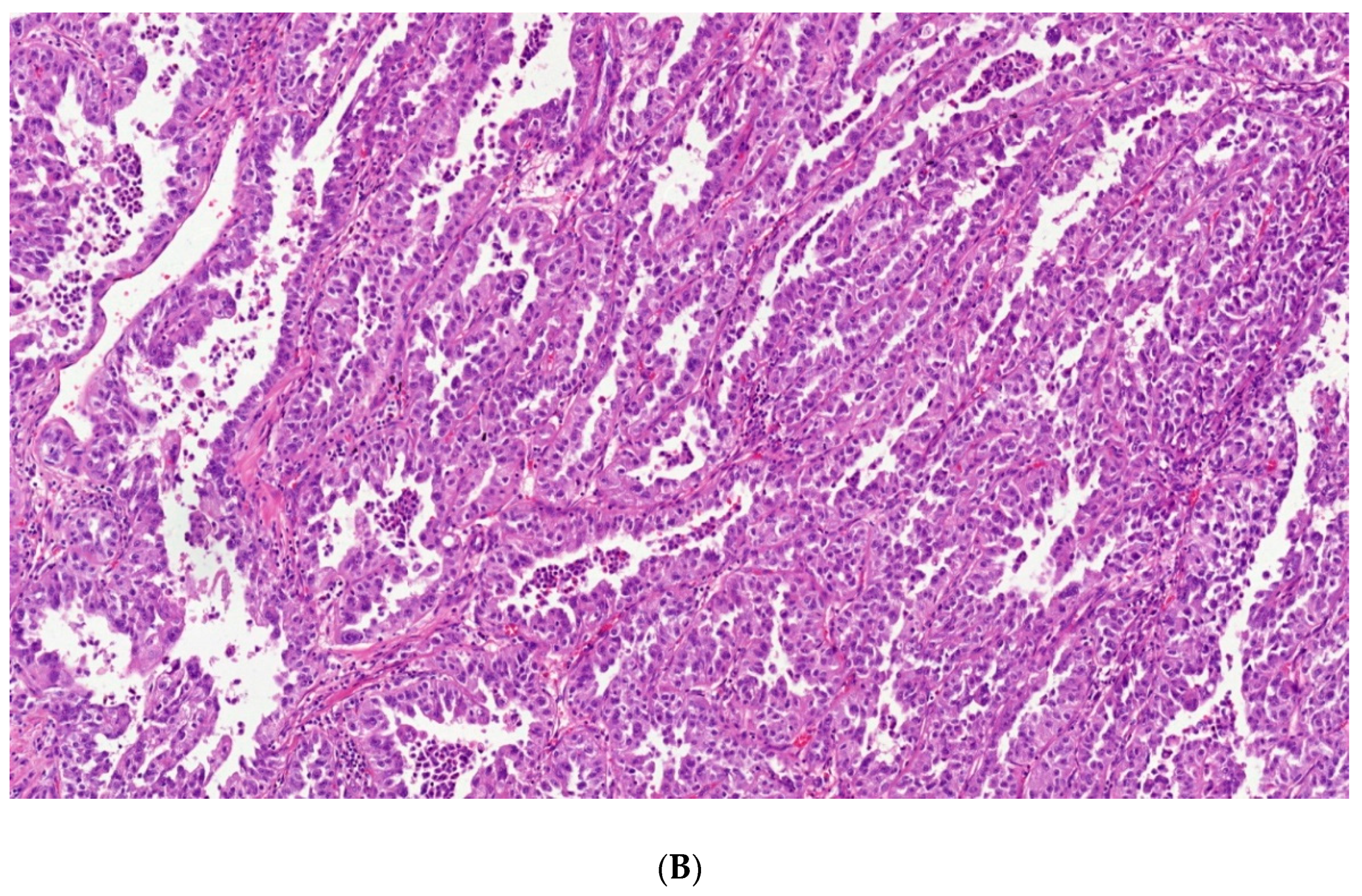{kind=link}
{kind=link}
Table 1.
Genetic tests and routinely used immunohistochemical examinations in renal cell tumors
| Tumor Type | IHC | Mutation | Method |
|---|---|---|---|
| CCRCC | Carbonic Anhydrase (CA) IX, Vimentin | VHL (von Hippel Lindau) inactivation | Sequencing (NGS/classical)/methylation specific PCR (polymerase chain reaction) |
| MCRCNLMP | NS | VHL | NR |
| PRCC type 1 hereditary syndrome | CK7, AMACR | MET | Sequencing (NGS/classical) |
| PRCC type 1 conventional type | CK7, AMACR | Gain of 7,17 | aCGH/FISH |
| PRCC type 2 | NS | NS | |
| OPRCC | AMACR, Vimentin | KRAS | Sequencing (NGS/classical) |
| FH-deficient RCC | FH, 2SC | FH mutation/LOH analysis | Sequencing (NGS/classical)/fragment analysis |
| ChRCCC | CK7, CD117 | NS | |
| “Hybrid” On/Ch tumors | NS | FLCN ** | Sequencing (NGS/classical) |
| Oncocytoma | CK7, CD117 | NS | |
| Clear cell PRCC | CK7, AMACR | VHL | Sequencing (NGS/classical) |
| MiT RCC | TFE3, Cathepsin K | TFE3, TFEB | FISH/NGS |
| MTSCC | AMACR, EMA | CNV pattern analysis | aCGH |
| TC-RCC | CK7, AMACR | CNV pattern analysis | aCGH |
| ACD-associated RCC | CK7, AMACR | NS | |
| RMC | INI1 | SMARCB1 | Sequencing (NGS/classical) |
| CDC | 34betaE12, Ck7 | NS | |
| SDH-deficient renal cell carcinoma | SDHB | SDHB | Sequencing (NGS, classical)/IHC |
Clear cell renal cell carcinoma (CCRCC). Multilocular cystic renal cell neoplasm of low malignant potential (MCRCNLMP). Papillary RCC (PRCC). Oncocytic papillary RCC (OPRCC). “Hybrid” oncocytic/chromophobe tumors (Hybrid” On/Ch tumors). ** Diagnosis of Birt–Hogg–Dubé syndrome. (MTSCC) Mucinous tubular and spindle cell carcinoma. CNV (copy-number variation) Tubulocystic RCC (TC-RCC) Renal medullary carcinoma (RMC). Fluorescence in situ hybridization (FISH). Next-generation sequencing (NGS). Array comparative genome hybridization (aCGH). Not specific (NS). Immunohistochemistry (IHC). Not recommended (NR).
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alaghehbandan, R.; Perez Montiel, D.; Luis, A.S.; Hes, O. Molecular Genetics of Renal Cell Tumors: A Practical Diagnostic Approach. Cancers 2020, 12, 85. https://doi.org/10.3390/cancers12010085
AMA Style
Alaghehbandan R, Perez Montiel D, Luis AS, Hes O. Molecular Genetics of Renal Cell Tumors: A Practical Diagnostic Approach. Cancers. 2020; 12(1):85. https://doi.org/10.3390/cancers12010085
Chicago/Turabian StyleAlaghehbandan, Reza, Delia Perez Montiel, Ana Silvia Luis, and Ondrej Hes. 2020. "Molecular Genetics of Renal Cell Tumors: A Practical Diagnostic Approach" Cancers 12, no. 1: 85. https://doi.org/10.3390/cancers12010085
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.