

Increased Plasmatic Levels of Exosomes Are Significantly Related to Relapse Rate in Patients with Oral Squamous Cell Carcinoma: A Cohort Study
 , ,
, ,  ,
,  , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection and Clinical Data
2.3. Sample Collection and Plasmatic Exosomes Characterization and Quantification
2.4. Statistical Analysis
3. Results
3.1. Sample Description
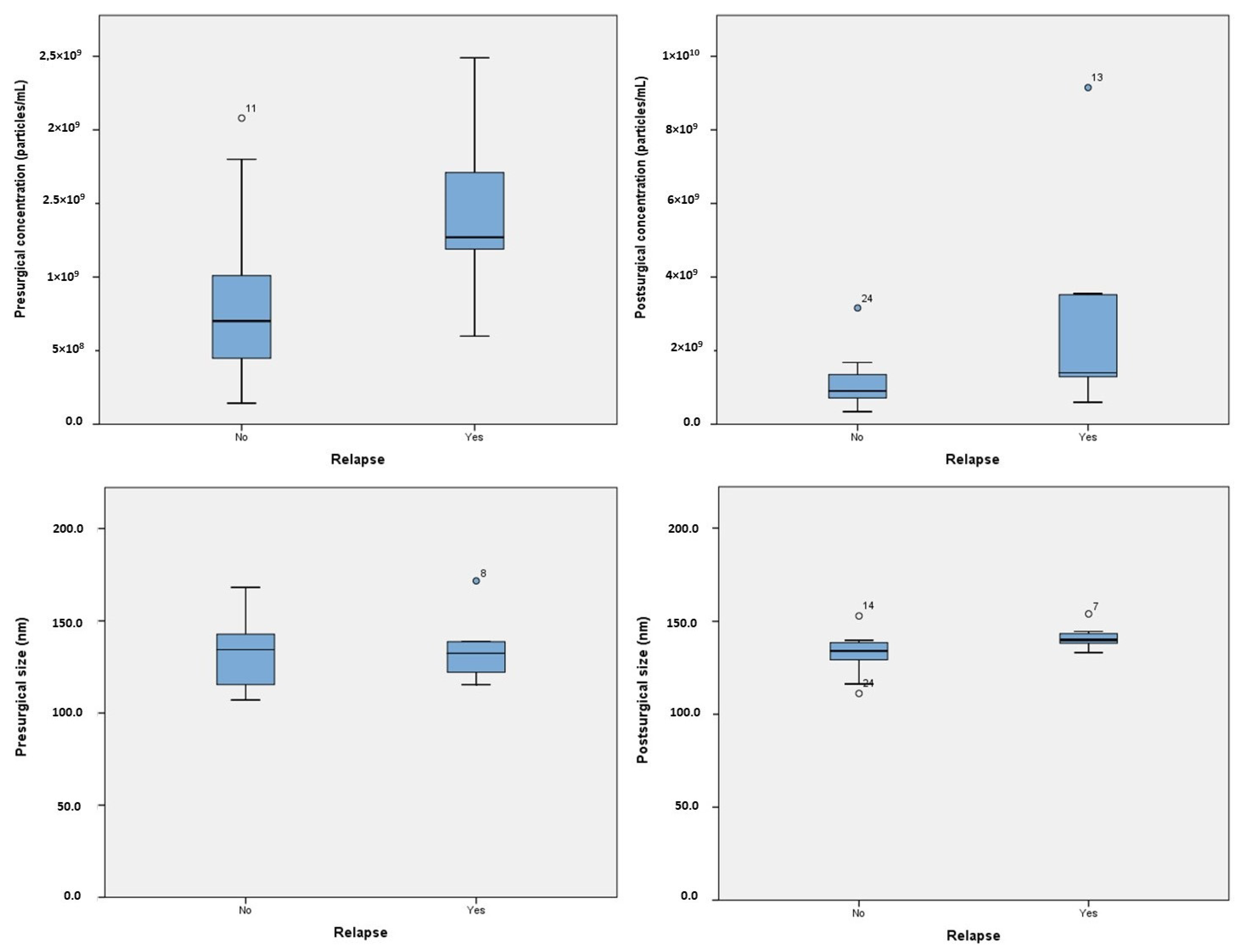
3.2. Concentration and Size Distribution of Plasmatic Exosomes
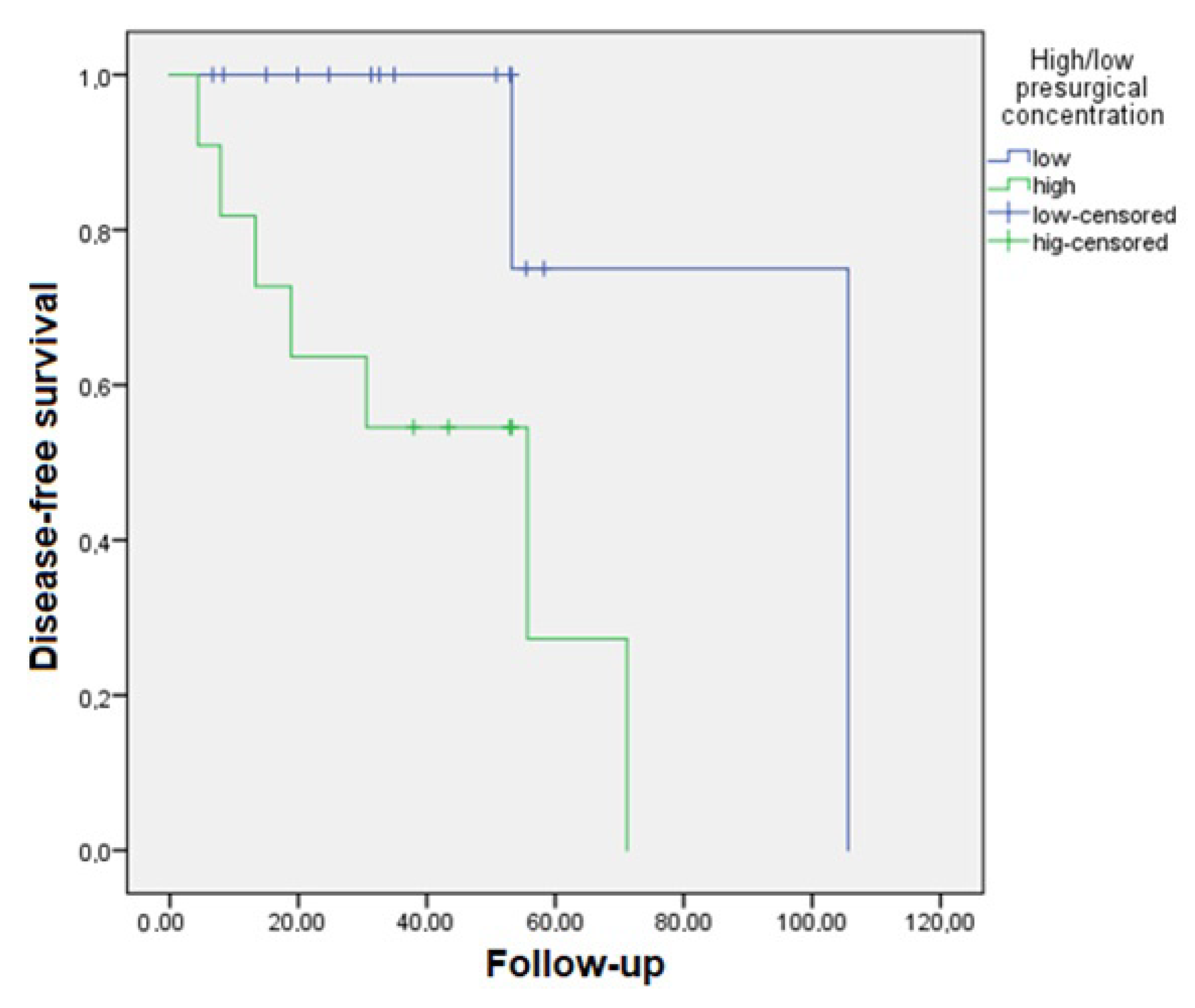
3.3. Survival Analysis
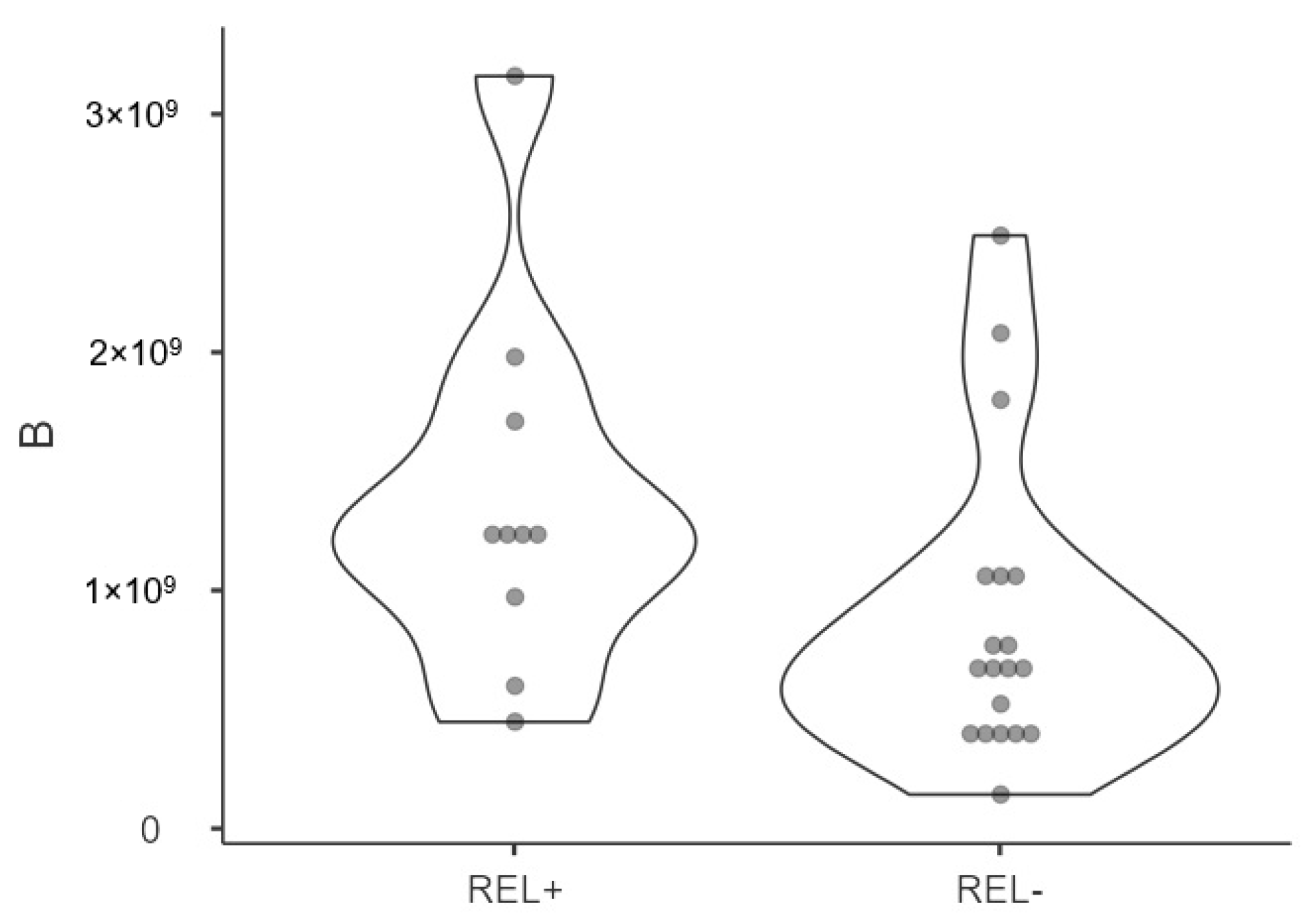
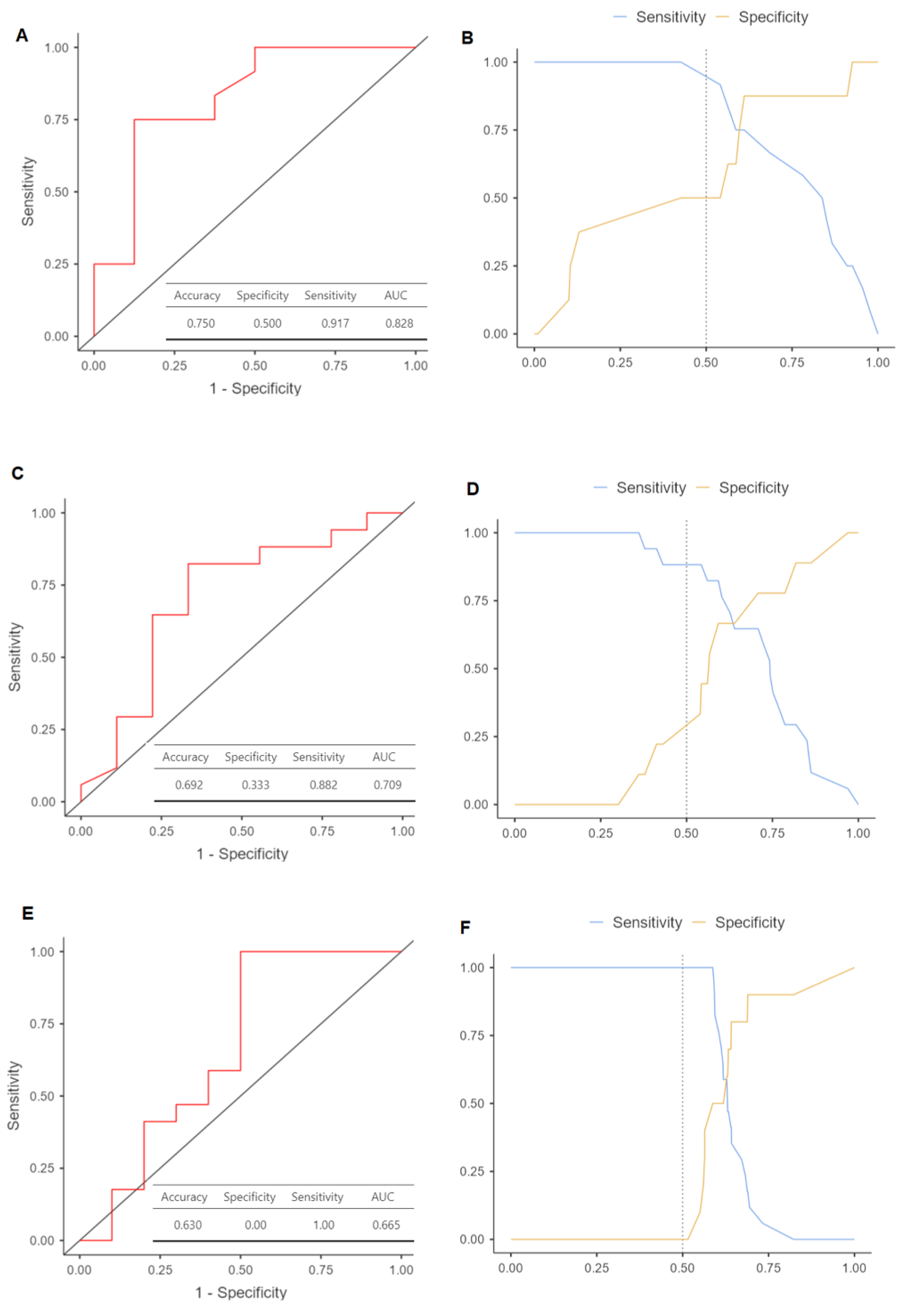
3.4. Relapse Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Boyd, N.M.; Reade, P.C. Mechanisms of carcinogenesis with particular reference to the oral mucosa. J. Oral Pathol. Med. 1988, 17, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Raza, A.; Khan, A.Q.; Inchakalody, V.P.; Mestiri, S.; Yoosuf, Z.S.K.; Bedhiafi, T.; El-Ella, D.M.A.; Taib, N.; Hydrose, S.; Akbar, S. Dynamic liquid biopsy components as predictive and prognostic biomarkers in colorectal cancer. J. Exp. Clin. Cancer Res. 2022, 41, 99. [Google Scholar] [CrossRef]
- Balachander, K.; Roy, A.; Priyadharsini, J.V.; Murugan, S.; Paramasivam, A. Mitochondrial DNA in circulating exosomes: A novel biomarker and potential therapeutic target for oral cancer. Oral Oncol. 2022, 128, 105857. [Google Scholar] [CrossRef]
- Tadimety, A.; Closson, A.; Li, C.; Yi, S.; Shen, T.; Zhang, J.X. Advances in liquid biopsy on-chip for cancer management: Technologies, biomarkers, and clinical analysis. Crit. Rev. Clin. Lab. Sci. 2018, 55, 140–162. [Google Scholar] [CrossRef]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef]
- Jia, S.; Zhang, R.; Li, Z.; Li, J. Clinical and biological significance of circulating tumor cells, circulating tumor DNA, and exosomes as biomarkers in colorectal cancer. Oncotarget 2017, 8, 55632. [Google Scholar] [CrossRef]
- Mason, T.E.; Ricks-Santi, L.; Chen, W.; Apprey, V.; Joykutty, J.; Ahaghotu, C.; Kittles, R.; Bonney, G.; Dunston, G.M. Association of CD14 variant with prostate cancer in African American men. Prostate 2010, 70, 262–269. [Google Scholar] [CrossRef]
- Li, Y.; Gao, S.; Hu, Q.; Wu, F. Functional Properties of Cancer Epithelium and Stroma-Derived Exosomes in Head and Neck Squamous Cell Carcinoma. Life 2022, 12, 757. [Google Scholar] [CrossRef]
- Shi, S.; Yu, Z.; Jia, J. The Roles of Exosomes in the Diagnose, Development and Therapeutic Resistance of Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2023, 24, 1968. [Google Scholar] [CrossRef] [PubMed]
- Fais, S.; O’Driscoll, L.; Borras, F.E.; Buzas, E.; Camussi, G.; Cappello, F.; Carvalho, J.; Cordeiro da Silva, A.; Del Portillo, H.; El Andaloussi, S.; et al. Evidence-based clinical use of nanoscale extracellular vesicles in nanomedicine. ACS Nano 2016, 10, 3886–3899. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.; Raposo, G.; Théry, C.; Biology, D. Biogenesis, secretion, and intercellular interactions of exosomes and other extracellular vesicles. Annu. Rev. Cell Dev. Biol. 2014, 30, 255–289. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, Y.; Gong, H.; Luo, S.; Cui, Y. The role of exosomes and their applications in cancer. Int. J. Mol. Sci. 2021, 22, 12204. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.; Tang, J.; Shiau, J.; Yen, C.; Chang, F.; Yang, K.; Hou, M.; Farooqi, A.A.; Chang, H. Modulating Effects of Cancer-Derived Exosomal miRNAs and Exosomal Processing by Natural Products. Cancers 2023, 15, 318. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Guo, J.; Fan, Z.; Yang, S.; Zhang, C.; Cheng, B.; Xia, J. Exosomal miR-146b-5p derived from cancer-associated fibroblasts promotes progression of oral squamous cell carcinoma by downregulating HIPK3. Cell. Signal. 2023, 106, 110635. [Google Scholar] [CrossRef]
- Yuan, Y.; Jiao, P.; Wang, Z.; Chen, M.; Du, H.; Xu, L.; Xu, J.; Dai, Y.; Wu, F.; Zhang, Y. Endoplasmic reticulum stress promotes the release of exosomal PD-L1 from head and neck cancer cells and facilitates M2 macrophage polarization. Cell Commun. Signal. 2022, 20, 12. [Google Scholar] [CrossRef]
- Rodríguez Zorrilla, S.; Pérez-Sayans, M.; Fais, S.; Logozzi, M.; Gallas Torreira, M.; García García, A. A pilot clinical study on the prognostic relevance of plasmatic exosomes levels in oral squamous cell carcinoma patients. Cancers 2019, 11, 429. [Google Scholar] [CrossRef] [PubMed]
- Devarajan, P. Neutrophil gelatinase-associated lipocalin: A promising biomarker for human acute kidney injury. Biomark. Med. 2010, 4, 265–280. [Google Scholar] [CrossRef]
- Logozzi, M.; De Milito, A.; Lugini, L.; Borghi, M.; Calabrò, L.; Spada, M.; Perdicchio, M.; Marino, M.L.; Federici, C.; Iessi, E.; et al. High levels of exosomes expressing CD63 and caveolin-1 in plasma of melanoma patients. PLoS ONE 2009, 4, e5219. [Google Scholar] [CrossRef] [PubMed]
- Logozzi, M.; Mizzoni, D.; Di Raimo, R.; Giuliani, A.; Maggi, M.; Sciarra, A.; Fais, S. Plasmatic exosome number and size distinguish prostate cancer patients from healthy individuals: A prospective clinical study. Front. Oncol. 2021, 11, 4258. [Google Scholar] [CrossRef] [PubMed]
- Cappello, F.; Fais, S. Extracellular vesicles in cancer pros and cons: The importance of the evidence-based medicine. Semin. Cancer Biol. 2022, 86, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, A.; Costa-Silva, B.; Shen, T.; Rodrigues, G.; Hashimoto, A.; Tesic Mark, M.; Molina, H.; Kohsaka, S.; Di Giannatale, A.; Ceder, S.; et al. Tumour exosome integrins determine organotropic metastasis. Nature 2015, 527, 329–335. [Google Scholar] [CrossRef]
- Steinbichler, T.B.; Dudás, J.; Riechelmann, H.; Skvortsova, I. The role of exosomes in cancer metastasis. Semin. Cancer Biol. 2017, 44, 170–181. [Google Scholar] [CrossRef]
- Federici, C.; Petrucci, F.; Caimi, S.; Cesolini, A.; Logozzi, M.; Borghi, M.; D’Ilio, S.; Lugini, L.; Violante, N.; Azzarito, T. Exosome release and low pH belong to a framework of resistance of human melanoma cells to cisplatin. PLoS ONE 2014, 9, e88193. [Google Scholar] [CrossRef]
- Słomka, A.; Kornek, M.; Cho, W.C. Small Extracellular Vesicles and Their Involvement in Cancer Resistance: An Up-to-Date Review. Cells 2022, 11, 2913. [Google Scholar] [CrossRef]
- Khan, M.I.; Alsayed, R.K.; Choudhry, H.; Ahmad, A. Exosome-mediated response to cancer therapy: Modulation of epigenetic machinery. Int. J. Mol. Sci. 2022, 23, 6222. [Google Scholar] [CrossRef]
- Syn, N.; Wang, L.; Sethi, G.; Thiery, J.; Goh, B. Exosome-mediated metastasis: From epithelial–mesenchymal transition to escape from immunosurveillance. Trends Pharmacol. Sci. 2016, 37, 606–617. [Google Scholar] [CrossRef]
- Aqil, F.; Gupta, R.C. Exosomes in cancer therapy. Cancers 2022, 14, 500. [Google Scholar] [CrossRef]
- Xiang, X.; Poliakov, A.; Liu, C.; Liu, Y.; Deng, Z.; Wang, J.; Cheng, Z.; Shah, S.V.; Wang, G.; Zhang, L.; et al. Induction of myeloid-derived suppressor cells by tumor exosomes. Int. J. Cancer 2009, 124, 2621–2633. [Google Scholar] [CrossRef]
- Lugini, L.; Sciamanna, I.; Federici, C.; Iessi, E.; Spugnini, E.P.; Fais, S. Antitumor effect of combination of the inhibitors of two new oncotargets: Proton pumps and reverse transcriptase. Oncotarget 2017, 8, 4147. [Google Scholar] [CrossRef]
- Lin, Z.; Wu, Y.; Xu, Y.; Li, G.; Li, Z.; Liu, T. Mesenchymal stem cell-derived exosomes in cancer therapy resistance: Recent advances and therapeutic potential. Mol. Cancer 2022, 21, 179. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Zhang, X.; Li, X. Exosomes derived from mesenchymal stem cells. Int. J. Mol. Sci. 2014, 15, 4142–4157. [Google Scholar] [CrossRef]
- Logozzi, M.; Angelini, D.F.; Iessi, E.; Mizzoni, D.; Di Raimo, R.; Federici, C.; Lugini, L.; Borsellino, G.; Gentilucci, A.; Pierella, F.; et al. Increased PSA expression on prostate cancer exosomes in in vitro condition and in cancer patients. Cancer Lett. 2017, 403, 318–329. [Google Scholar] [CrossRef] [PubMed]
- Logozzi, M.; Di Raimo, R.; Mizzoni, D.; Fais, S. Immunocapture-based ELISA to characterize and quantify exosomes in both cell culture supernatants and body fluids. Meth Enzymol. 2020, 645, 155–180. [Google Scholar]
- Orefice, N.S.; Di Raimo, R.; Mizzoni, D.; Logozzi, M.; Fais, S. Purposing plant-derived exosomes-like nanovesicles for drug delivery: Patents and literature review. Expert Opin. Ther. Pat. 2023, 33, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Castelli, G.; Logozzi, M.; Mizzoni, D.; Di Raimo, R.; Cerio, A.; Dolo, V.; Pasquini, L.; Screnci, M.; Ottone, T.; Testa, U.; et al. Ex Vivo Anti-Leukemic Effect of Exosome-like Grapefruit-Derived Nanovesicles from Organic Farming-The Potential Role of Ascorbic Acid. Int. J. Mol. Sci. 2023, 24, 15663. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strobe Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Ajuria, M.; García-García, A.; Suárez-Peñaranda, J.M.; Garrido-Pumar, M.; Chamorro-Petronacci, C.M.; Somoza-Martín, J.M.; Pérez-Sayáns, M. Analysis of the Efficiency and Prognostic Value of the Sentinel Node Technique in Oral Squamous Cell Carcinoma after Seven Years. Medicina 2021, 57, 1092. [Google Scholar] [CrossRef] [PubMed]
- An, H.J.; Kim, M.H.; Kim, S.H.; Lee, G.; Song, D.H. Prognostic role of extracellular vesicles in squamous cell carcinoma of the lung. Thorac. Cancer 2020, 11, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Heckler, C.E. Applied Multivariate Statistical Analysis. Technometrics 2005, 47, 517. [Google Scholar] [CrossRef]
- Mascitti, M.; Rubini, C.; De Michele, F.; Balercia, P.; Girotto, R.; Troiano, G.; Muzio, L.L.; Santarelli, A. American Joint Committee on Cancer staging system 7th edition versus 8th edition: Any improvement for patients with squamous cell carcinoma of the tongue? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Pollaers, K.; Hinton-Bayre, A.; Friedland, P.L.; Farah, C.S. AJCC 8th Edition oral cavity squamous cell carcinoma staging–Is it an improvement on the AJCC 7th Edition? Oral Oncol. 2018, 82, 23–28. [Google Scholar] [CrossRef]
- Farah, C.S. Molecular landscape of head and neck cancer and implications for therapy. Ann. Transl. Med. 2021, 9, 915. [Google Scholar] [CrossRef]
- Rivera, C.; Oliveira, A.K.; Costa, R.A.P.; De Rossi, T.; Leme, A.F.P. Prognostic biomarkers in oral squamous cell carcinoma: A systematic review. Oral Oncol. 2017, 72, 38–47. [Google Scholar] [CrossRef]
- Gleber-Netto, F.O.; Braakhuis, B.J.; Triantafyllou, A.; Takes, R.P.; Kelner, N.; Rodrigo, J.P.; Strojan, P.; Vander Poorten, V.; Rapidis, A.D.; Rinaldo, A. Molecular events in relapsed oral squamous cell carcinoma: Recurrence vs secondary primary tumor. Oral Oncol. 2015, 51, 738–744. [Google Scholar] [CrossRef]
- González-Moles, M.Á.; Warnakulasuriya, S.; López-Ansio, M.; Ramos-García, P. Hallmarks of Cancer Applied to Oral and Oropharyngeal Carcinogenesis: A Scoping Review of the Evidence Gaps Found in Published Systematic Reviews. Cancers 2022, 14, 3834. [Google Scholar] [CrossRef]
- Søland, T.M.; Brusevold, I.J. Prognostic molecular markers in cancer–quo vadis? Histopathology 2013, 63, 297–308. [Google Scholar] [CrossRef]
- Peterson, E.B.; Chou, W.S.; Gaysynsky, A.; Krakow, M.; Elrick, A.; Khoury, M.J.; Kaphingst, K.A. Communication of cancer-related genetic and genomic information: A landscape analysis of reviews. Transl. Behav. Med. 2018, 8, 59–70. [Google Scholar] [CrossRef]
- Bano, A.; Vats, R.; Yadav, P.; Bhardwaj, R. Exosomics in Oral Cancer Diagnosis, Prognosis, and Therapeutics-An emergent and imperative non-invasive natural nanoparticle-based approach. Crit. Rev. Oncol. 2022, 178, 103799. [Google Scholar] [CrossRef]
- Li, S.; Man, Q.; Gao, X.; Lin, H.; Wang, J.; Su, F.; Wang, H.; Bu, L.; Liu, B.; Chen, G. Tissue-derived extracellular vesicles in cancers and non-cancer diseases: Present and future. J. Extracell. Vesicles 2021, 10, e12175. [Google Scholar] [CrossRef] [PubMed]
- Urabe, F.; Patil, K.; Ramm, G.A.; Ochiya, T.; Soekmadji, C. Extracellular vesicles in the development of organ-specific metastasis. J. Extracell. Vesicles 2021, 10, e12125. [Google Scholar] [CrossRef] [PubMed]
- Andreola, G.; Rivoltini, L.; Castelli, C.; Huber, V.; Perego, P.; Deho, P.; Squarcina, P.; Accornero, P.; Lozupone, F.; Lugini, L. Induction of lymphocyte apoptosis by tumor cell secretion of FasL-bearing microvesicles. J. Exp. Med. 2002, 195, 1303–1316. [Google Scholar] [CrossRef] [PubMed]
- Huber, V.; Fais, S.; Iero, M.; Lugini, L.; Canese, P.; Squarcina, P.; Zaccheddu, A.; Colone, M.; Arancia, G.; Gentile, M. Human colorectal cancer cells induce T-cell death through release of proapoptotic microvesicles: Role in immune escape. Gastroenterology 2005, 128, 1796–1804. [Google Scholar] [CrossRef]
- Bergmann, C.; Strauss, L.; Wieckowski, E.; Czystowska, M.; Albers, A.; Wang, Y.; Zeidler, R.; Lang, S.; Whiteside, T.L. Tumor-derived microvesicles in sera of patients with head and neck cancer and their role in tumor progression. Head Neck 2009, 31, 371–380. [Google Scholar] [CrossRef]
- LeBleu, V.S.; Kalluri, R. Exosomes as a multicomponent biomarker platform in cancer. Trends Cancer 2020, 6, 767–774. [Google Scholar] [CrossRef]
- Ye, B.; Duan, Y.; Zhou, M.; Wang, Y.; Lai, Q.; Yue, K.; Cao, J.; Wu, Y.; Wang, X.; Jing, C. Hypoxic tumor-derived exosomal miR-21 induces cancer-associated fibroblast activation to promote head and neck squamous cell carcinoma metastasis. Cell. Signal. 2023, 108, 110725. [Google Scholar] [CrossRef]
- Xiao, C.; Song, F.; Zheng, Y.L.; Lv, J.; Wang, Q.F.; Xu, N. Exosomes in Head and Neck Squamous Cell Carcinoma. Front. Oncol. 2019, 9, 894. [Google Scholar] [CrossRef] [PubMed]
- Todorova, D.; Simoncini, S.; Lacroix, R.; Sabatier, F.; Dignat-George, F. Extracellular Vesicles in Angiogenesis. Circ. Res. 2017, 120, 1658–1673. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, L.; Medyany, V.; Ezić, J.; Lotfi, R.; Niesler, B.; Röth, R.; Engelhardt, D.; Laban, S.; Schuler, P.J.; Hoffmann, T.K.; et al. Cargo and Functional Profile of Saliva-Derived Exosomes Reveal Biomarkers Specific for Head and Neck Cancer. Front. Med. 2022, 9, 2030. [Google Scholar] [CrossRef]
- Lou, C.; Shi, J.; Xu, Q. Exosomal miR-626 promotes the malignant behavior of oral cancer cells by targeting NFIB. Mol. Biol. Rep. 2022, 49, 4829–4840. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.; Oliveira, C.; Dourado, M.; Macedo, C.; Winck, F.; Paes Leme, A.; Salo, T.; Coletta, R.; Almeida Freitas, R.; Galvão, H. Extracellular vesicles from oral squamous carcinoma cells display pro- and anti-angiogenic properties. Oral Dis. 2018, 24, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wu, H.; Zhu, Y.; Chen, X.; Chen, Y. Plasma exosomal caveolin-1 predicts Poor Prognosis in Ovarian Cancer. J. Cancer 2021, 12, 5005–5012. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Wu, S.; Hu, C. A narrative review of the role of exosomes and caveolin-1 in liver diseases and cancer. Int. Immunopharmacol. 2023, 120, 110284. [Google Scholar] [CrossRef]
- Fu, P.; Chen, F.; Pan, Q.; Zhao, X.; Zhao, C.; Cho, W.C.; Chen, H. The different functions and clinical significances of caveolin-1 in human adenocarcinoma and squamous cell carcinoma. Onco Targets Ther. 2017, 10, 819–835. [Google Scholar] [CrossRef]
- Xue, J.; Chen, H.; Diao, L.; Chen, X.; Xia, D. Expression of caveolin-1 in tongue squamous cell carcinoma by quantum dots. Eur. J. Histochem. 2010, 54, e20. [Google Scholar] [CrossRef]
- He, T.; Guo, X.; Li, X.; Liao, C.; Wang, X.; He, K. Plasma-Derived Exosomal microRNA-130a Serves as a Noninvasive Biomarker for Diagnosis and Prognosis of Oral Squamous Cell Carcinoma. J. Oncol. 2021, 2021, 5547911. [Google Scholar] [CrossRef]
- Deng, Q.; Chen, Y.; Lin, L.; Lin, J.; Wang, H.; Qiu, Y.; Pan, L.; Zheng, X.; Wei, L.; Wang, J. Exosomal hsa_circRNA_047733 integrated with clinical features for preoperative prediction of lymph node metastasis risk in oral squamous cell carcinoma. J. Oral Pathol. Med. 2023, 52, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Xiao, M.; Zhang, J.; Chen, W.; Chen, W. M1-like tumor-associated macrophages activated by exosome-transferred THBS1 promote malignant migration in oral squamous cell carcinoma. J. Exp. Clin. Cancer Res. 2018, 37, 143. [Google Scholar] [CrossRef] [PubMed]
- Jin, N.; Jin, N.; Bu, W.; Li, X.; Liu, L.; Wang, Z.; Tong, J.; Li, D. Long non-coding RNA TIRY promotes tumor metastasis by enhancing epithelial-to-mesenchymal transition in oral cancer. Exp. Biol. Med. 2020, 245, 585–596. [Google Scholar] [CrossRef]
- Pang, X.; Wang, S.; Zhang, M.; Jiang, J.; Fan, H.; Wu, J.; Wang, H.; Liang, X.; Tang, Y. OSCC cell-secreted exosomal CMTM6 induced M2-like macrophages polarization via ERK1/2 signaling pathway. Cancer Immunol. Immunother. 2021, 70, 1015–1029. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qin, X.; Zhu, X.; Chen, W.; Zhang, J.; Chen, W. Oral cancer-derived exosomal NAP1 enhances cytotoxicity of natural killer cells via the IRF-3 pathway. Oral Oncol. 2018, 76, 34–41. [Google Scholar] [CrossRef]
- Zorrilla, S.R.; García, A.G.; Carrión, A.B.; Vila, P.G.; Martín, M.S.; Torreira, M.G.; Sayans, M.P. Exosomes in head and neck cancer. Updating and revisiting. J. Enzym. Inhib. Med. Chem. 2019, 34, 1641–1651. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zheng, Z.; Yuan, Y.; Pathak, J.L.; Yang, X.; Wang, L.; Ye, Z.; Cho, W.C.; Zeng, M.; Wu, L. The Emerging Role of Exosomes in Oral Squamous Cell Carcinoma. Front. Cell Dev. Biol. 2021, 9, 324. [Google Scholar] [CrossRef]
- Xu, Y.; Jiang, E.; Shao, Z.; Shang, Z. Long noncoding RNAs in the metastasis of oral squamous cell carcinoma. Front. Oncol. 2021, 10, 616717. [Google Scholar] [CrossRef]
- Li, C.; Zhou, Y.; Liu, J.; Su, X.; Qin, H.; Huang, S.; Huang, X.; Zhou, N. Potential markers from serum-purified exosomes for detecting oral squamous cell carcinoma metastasis. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1668–1681. [Google Scholar] [CrossRef]
- Yu, J.; Liu, Y.; Guo, C.; Zhang, S.; Gong, Z.; Tang, Y.; Yang, L.; He, Y.; Lian, Y.; Li, X. Upregulated long non-coding RNA LINC00152 expression is associated with progression and poor prognosis of tongue squamous cell carcinoma. J. Cancer 2017, 8, 523. [Google Scholar] [CrossRef]
- Campanella, C.; Rappa, F.; Sciumè, C.; Marino Gammazza, A.; Barone, R.; Bucchieri, F.; David, S.; Curcurù, G.; Caruso Bavisotto, C.; Pitruzzella, A. Heat shock protein 60 levels in tissue and circulating exosomes in human large bowel cancer before and after ablative surgery. Cancer 2015, 121, 3230–3239. [Google Scholar] [CrossRef] [PubMed]
- Bunduc, S.; Gede, N.; Váncsa, S.; Lillik, V.; Kiss, S.; Juhász, M.F.; Erőss, B.; Szakács, Z.; Gheorghe, C.; Mikó, A.; et al. Exosomes as prognostic biomarkers in pancreatic ductal adenocarcinoma–a systematic review and meta-analysis. Transl. Res. 2022, 244, 126–136. [Google Scholar] [CrossRef]
- Cappello, F.; Logozzi, M.; Campanella, C.; Bavisotto, C.C.; Marcilla, A.; Properzi, F.; Fais, S. Exosome levels in human body fluids: A tumor marker by themselves? Eur. J. Pharm. Sci. 2017, 96, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Lugini, L.; Valtieri, M.; Federici, C.; Cecchetti, S.; Meschini, S.; Condello, M.; Signore, M.; Fais, S. Exosomes from human colorectal cancer induce a tumor-like behavior in colonic mesenchymal stromal cells. Oncotarget 2016, 7, 50086–50098. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Yang, L.; Baddour, J.; Achreja, A.; Bernard, V.; Moss, T.; Marini, J.C.; Tudawe, T.; Seviour, E.G.; San Lucas, F.A.; et al. Tumor microenvironment derived exosomes pleiotropically modulate cancer cell metabolism. eLife 2016, 5, e10250. [Google Scholar] [CrossRef] [PubMed]
- Cossetti, C.; Lugini, L.; Astrologo, L.; Saggio, I.; Fais, S.; Spadafora, C. Soma-to-germline transmission of RNA in mice xenografted with human tumour cells: Possible transport by exosomes. PLoS ONE 2014, 9, e101629. [Google Scholar] [CrossRef]
- Logozzi, M.; Mizzoni, D.; Angelini, D.F.; Di Raimo, R.; Falchi, M.; Battistini, L.; Fais, S. Microenvironmental pH and exosome levels interplay in human cancer cell lines of different histotypes. Cancers 2018, 10, 370. [Google Scholar] [CrossRef]
- Logozzi, M.; Capasso, C.; Di Raimo, R.; Del Prete, S.; Mizzoni, D.; Falchi, M.; Supuran, C.T.; Fais, S. Prostate cancer cells and exosomes in acidic condition show increased carbonic anhydrase IX expression and activity. J. Enzym. Inhib. Med. Chem. 2019, 34, 272–278. [Google Scholar] [CrossRef]
- Logozzi, M.; Orefice, N.S.; Di Raimo, R.; Mizzoni, D.; Fais, S. The Importance of Detecting, Quantifying, and Characterizing Exosomes as a New Diagnostic/Prognostic Approach for Tumor Patients. Cancers 2023, 15, 2878. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | |
|---|---|---|
| Qualitative Analysis | ||
| Gender | Male | 14 (51.9) |
| Female | 13 (48.1) | |
| Tumor localization | Buccal mucosa | 3 (11.1) |
| Gum | 6 (22.2) | |
| Floor of the mouth | 3 (11.1) | |
| Retromolar trigone | 3 (11.1) | |
| Hard palate | 5 (18.5) | |
| Tongue | 5 (18.5) | |
| Maxilla | 2 (7.4) | |
| Tobacco consumption | No | 14 (51.9) |
| Yes | 11 (40.7) | |
| Ex consumer | 2 (7.4) | |
| Tumor stage | Stage 1 | 8 (29.6) |
| Stage 2 | 7 (25.9) | |
| Stage 3 | 2 (7.4) | |
| Stage 4 | 10 (37) | |
| TNM stage (T) | T1 | 7 (25.9) |
| T2 | 7 (25.9) | |
| T3 | 3 (11.1) | |
| T4 | 9 (33.3) | |
| TNM stage (N) | N1 | 3 (11.1) |
| N2 | 9 (33.3) | |
| N3 | 1 (3.7) | |
| TNM stage (M) | M0 | 24 (88.9) |
| M1 | 3 (11.1) | |
| Differentiation | Mild | 12 (44.4) |
| Moderate | 14 (51.9) | |
| Severe | 1 (3.7) | |
| Radiotherapy | No | 17 (63) |
| Yes | 10 (37) | |
| Chemotherapy | No | 22 (81.5) |
| Yes | 5 (18.5) | |
| Local metastasis | No | 24 (88.9) |
| Yes | 3 (11.1) | |
| Relapse | No | 18 (66.7) |
| Yes | 9 (33.3) | |
| Exitus | No | 17 (63) |
| Yes | 10 (37) | |
| Quantitative analysis | Mean ± SD | Min–max |
| Age | 70.35 (13.57) | 46.7–100.19 |
| Cigarettes per day | 11.89 (14.96) | 0–40 |
| Presurgical concentration (particles/mL) | 1.02 × 109 (5.89 × 108) | 1 × 108–2 × 109 |
| Postsurgical concentration (particles/mL) | 1.76 × 109 (1.98 × 109) | 3 × 108–9 × 109 |
| Presurgical (nm) | 133.57 (17.46) | 107.1–171.7 |
| Postsurgical (nm) | 135.52 (10.36) | 111.2–154 |
| Follow-up (months) | 38.56 (23.36) | 4.37–105.59 |
| Follow-up with relapse patients (months) | 26.46 (26.44) | 2.43–85.37 |
| Follow-up with exitus patients (months) | 18.22 (11.71) | 4.37–34.92 |
| Variable | Univariate (HR 95%CI) | p | Adjusted (HR 95%CI) | p-Value |
|---|---|---|---|---|
| Presurgical concentration | ||||
| High vs. low | 11.37 (1.65–78.37) | 0.014 | 18.35 (1.61–208.35) | 0.019 |
| Male vs. female | 1.56 (0.31–7.82) | 0.587 | 0.38 (0.04–4.22) | 0.433 |
| Postsurgical concentration | ||||
| Particles/mL | ||||
| High vs. low | 9.00 (0.717–113.016) | 0.89 | 9.00 (0.660–122.794) | 0.99 |
| Male vs. female | 1.56 (0.31–7.82) | 0.587 | 1.00 (0.124–8.090) | 1 |
| Presurgical dimension (nm) | ||||
| High vs. low | 2.25 (0.419–12.092) | 0.345 | 2.17 (0.398–11.897) | 0.370 |
| Male vs. female | 1.56 (0.31–7.82) | 0.587 | 1.261 (0.239–6.659) | 0.785 |
| Postsurgical dimension (nm) | ||||
| High vs. low | 1.200 (0.185–7.770) | 0.848 | 1.337 (0.194–9.202) | 0.768 |
| Male vs. female | 1.56 (0.31–7.82) | 0.587 | 1.653 (0.246–11.088) | 0.605 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Zorrilla, S.; Lorenzo-Pouso, A.I.; Fais, S.; Logozzi, M.A.; Mizzoni, D.; Di Raimo, R.; Giuliani, A.; García-García, A.; Pérez-Jardón, A.; Ortega, K.L.; et al. Increased Plasmatic Levels of Exosomes Are Significantly Related to Relapse Rate in Patients with Oral Squamous Cell Carcinoma: A Cohort Study. Cancers 2023, 15, 5693. https://doi.org/10.3390/cancers15235693
Rodríguez-Zorrilla S, Lorenzo-Pouso AI, Fais S, Logozzi MA, Mizzoni D, Di Raimo R, Giuliani A, García-García A, Pérez-Jardón A, Ortega KL, et al. Increased Plasmatic Levels of Exosomes Are Significantly Related to Relapse Rate in Patients with Oral Squamous Cell Carcinoma: A Cohort Study. Cancers. 2023; 15(23):5693. https://doi.org/10.3390/cancers15235693
Chicago/Turabian StyleRodríguez-Zorrilla, Samuel, Alejandro I. Lorenzo-Pouso, Stefano Fais, Maria A. Logozzi, Davide Mizzoni, Rossella Di Raimo, Alessandro Giuliani, Abel García-García, Alba Pérez-Jardón, Karem L. Ortega, and et al. 2023. "Increased Plasmatic Levels of Exosomes Are Significantly Related to Relapse Rate in Patients with Oral Squamous Cell Carcinoma: A Cohort Study" Cancers 15, no. 23: 5693. https://doi.org/10.3390/cancers15235693