
Robotic versus Laparoscopic Liver Resections for Colorectal Metastases: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
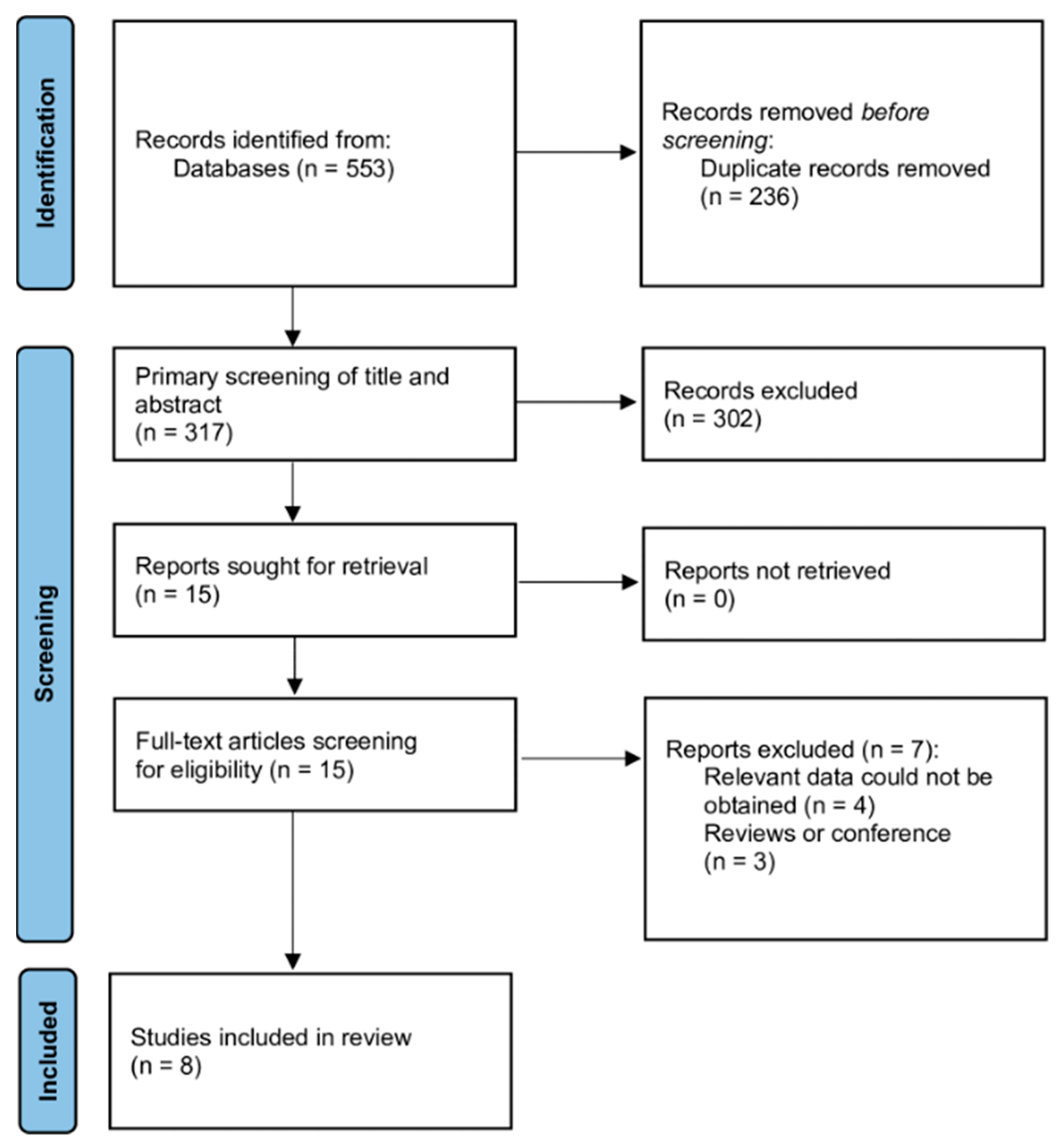
2.1. Literature Search and Selection
2.2. Data Extraction and Quality Assessment
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Eligible Studies and Study Characteristics
3.2. Patient Characteristics
3.3. Intraoperative Period Characteristics
3.4. Outcomes Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baidoun, F.; Elshiwy, K.; Elkeraie, Y.; Merjaneh, Z.; Khoudari, G.; Sarmini, M.T.; Gad, M.; Al-Husseini, M.; Saad, A. Colorectal Cancer Epidemiology: Recent Trends and Impact on Outcomes. Curr. Drug Targets 2021, 22, 998–1009. [Google Scholar] [PubMed]
- Aran, V.; Victorino, A.P.; Thuler, L.C.; Ferreira, C.G. Colorectal Cancer: Epidemiology, Disease Mechanisms and Interventions to Reduce Onset and Mortality. Clin. Colorectal Cancer 2016, 15, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.P.; Qiu, H.; Liao, S.J.; Ai, J.H.; Shi, J. Mini-invasive vs. open resection of colorectal cancer and liver metastases: A metaanalysis. World J. Gastroenterol. 2019, 25, 2819–2832. [Google Scholar] [CrossRef] [PubMed]
- Rahimli, M.; Perrakis, A.; Schellerer, V.; Gumbs, A.; Lorenz, E.; Franz, M.; Arend, J.; Negrini, V.R.; Croner, R.S. Robotic and laparoscopic liver surgery for colorectal liver metastases: An experience from a German Academic Center. World J. Surg. Oncol. 2020, 18, 333. [Google Scholar] [CrossRef] [PubMed]
- Aghayan, D.L.; Kazaryan, A.M.; Dagenborg, V.J.; Røsok, B.I.; Fagerland, M.W.; Waaler Bjørnelv, G.M.; Kristiansen, R.; Flatmark, K.; Fretland, Å.A.; Edwin, B.; et al. Long-Term Oncologic Outcomes After Laparoscopic Versus Open Resection for Colorectal Liver Metastases: A Randomized Trial. Ann. Intern. Med. 2021, 174, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.M.; Xiong, J.J.; Liu, X.T.; Chen, H.Y.; Iglesia-García, D.; Altaf, K.; Bharucha, S.; Huang, W.; Nunes, Q.M.; Szatmary, P.; et al. Laparoscopic Versus Open Liver Resection for Colorectal Liver Metastases: A Comprehensive Systematic Review and Metaanalysis. Sci. Rep. 2017, 7, 1012. [Google Scholar] [CrossRef] [PubMed]
- Schmelzle, M.; Feldbrügge, L.; Ortiz Galindo, S.A.; Moosburner, S.; Kästner, A.; Krenzien, F.; Benzing, C.; Biebl, M.; Öllinger, R.; Malinka, T.; et al. Robotic vs. laparoscopic liver surgery: A single-center analysis of 600 consecutive patients in 6 years. Surg. Endosc. 2022, 36, 5854–5862. [Google Scholar] [CrossRef] [PubMed]
- Gumbs, A.A.; Lorenz, E.; Tsai, T.J.; Starker, L.; Flanagan, J.; Benedetti Cacciaguerra, A.; Yu, N.J.; Bajul, M.; Chouillard, E.; Croner, R.; et al. Study: International Multicentric Minimally Invasive Liver Resection for Colorectal Liver Metastases (SIMMILR-CRLM). Cancers 2022, 14, 379. [Google Scholar] [CrossRef] [PubMed]
- Giulianotti, P.C.; Coratti, A.; Sbrana, F.; Addeo, P.; Bianco, F.M.; Buchs, N.C.; Annechiarico, M.; Benedetti, E. Robotic liver surgery: Results for 70 resections. Surgery 2011, 149, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.B.; Wang, H.G.; Zhao, Z.M.; Duan, W.D.; Lu, F.; Dong, J.H. Robotic-assisted laparoscopic anatomic hepatectomy in China: Initial experience. Ann. Surg. 2011, 253, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Aboudou, T.; Li, M.; Zhang, Z.; Wang, Z.; Li, Y.; Feng, L.; Chu, X.; Chen, N.; Zhou, W.; Yang, K. Laparoscopic versus Robotic Hepatectomy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5831. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wallace, B.; Small, K.; Brodley, C.; Lau, J.; Trikalinos, T. Deploying an interactive machine learning system in an evidence-based practice center: Abstrackr. In Proceedings of the ACM International Health Informatics Symposium (IHI), Miami, FL, USA, 28–30 January 2012; pp. 819–824. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing the risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Beard, R.E.; Khan, S.; Troisi, R.I.; Montalti, R.; Vanlander, A.; Fong, Y.; Kingham, T.P.; Boerner, T.; Berber, E.; Kahramangil, B.; et al. Long-Term and Oncologic Outcomes of Robotic Versus Laparoscopic Liver Resection for Metastatic Colorectal Cancer: A Multicenter, Propensity Score Matching Analysis. World J. Surg. 2020, 44, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Gumbs, A.A.; Croner, R.; Lorenz, E.; Cacciaguerra, A.B.; Tsai, T.J.; Starker, L.; Flanagan, J.; Yu, N.J.; Chouillard, E.; Abu Hilal, M. Survival Study: International Multicentric Minimally Invasive Liver Resection for Colorectal Liver Metastases (SIMMILR-2). Cancers 2022, 14, 4190. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Fu, L. Application Effect of Robot-Assisted Laparoscopy in Hepatectomy for Colorectal Cancer Patients with Liver Metastases. Comput. Math. Methods Med. 2022, 2022, 5492943. [Google Scholar] [CrossRef] [PubMed]
- Masetti, M.; Fallani, G.; Ratti, F.; Ferrero, A.; Giuliante, F.; Cillo, U.; Guglielmi, A.; Ettorre, G.M.; Torzilli, G.; Vincenti, L.; et al. Minimally invasive treatment of colorectal liver metastases: Does robotic surgery provide any technical advantages over laparoscopy? A multicenter analysis from the IGoMILS (Italian Group of Minimally Invasive Liver Surgery) registry. Updates Surg. 2022, 74, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Balzano, E.; Bernardi, L.; Roesel, R.; Vagelli, F.; Ghinolfi, D.; Tincani, G.; Catalano, G.; Melandro, F.; Petrusic, A.; Popeskou, S.G.; et al. Robotic versus laparoscopic liver resections: Propensity-matched comparison of two-center experience. Surg. Endosc. 2023, 37, 8123–8132. [Google Scholar] [CrossRef] [PubMed]
- Cheung, T.T.; Liu, R.; Cipriani, F.; Wang, X.; Efanov, M.; Fuks, D.; Choi, G.H.; Syn, N.L.; Chong, C.C.N.; Di Benedetto, F.; et al. Robotic versus laparoscopic liver resection for huge (≥10 cm) liver tumors: An international multicenter propensity-score matched cohort study of 799 cases. Hepatobiliary Surg. Nutr. 2023, 12, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Radomski, S.N.; Chen, S.Y.; Stem, M.; Done, J.Z.; Atallah, C.; Safar, B.; Efron, J.E.; Gabre-Kidan, A. Procedure-specific risks of robotic simultaneous resection of colorectal cancer and synchronous liver metastases. J. Robot. Surg. 2023, 17, 2555–2558. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Country | Study Design | LLR Group | RLR Group | ||||
|---|---|---|---|---|---|---|---|---|
| No. of Patients | Age | Sex, Male | No. of Patients | Age | Sex, Male | |||
| Balzano et al., 2023 [23] | Italy | Prospective | 192 | 66 ± 12 | 110 (57.3%) | 77 | 66 ± 12.1 | 49 (63.6%) |
| Beard et al. 2020 [19] | Multi-country | Retrospective | 514 | 63 ± 12 | 314 (61.2%) | 115 | 61 ±11 | 39 (33.9%) |
| Cheung et al., 2023 [24] | Multi-country | Retrospective | 219 | 55 ± 4.3 | 105 | 73 | 53.5 ± 4.3 | 34 |
| Gumbs et al., 2022 [20] | Multi-country | Retrospective | 462 | 63.8 ± 11.7 | 259 (56.1%) | 36 | 61.8 ± 11.0 | 21 (58.3%) |
| Li et al., 2022 [21] | China | Randomized | 61 | 57.51 ± 6.27 | 38 (62.30%) | 61 | 57.13 ± 586 | 44 (72.13%) |
| Masetti et al., 2022 [22] | Italy | Retrospective | 953 | 65.6 ± 10.9 | 589 (62.7%) | 77 | 65.0 ± 10.6 | 50 (64.9%) |
| Radomski et al., 2023 [25] | USA | Retrospective | 266 | 52 | NS | 79 | 63 | NS |
| Rahimli et al., 2020 [4] | Germany | Retrospective | 13 | 62.1 ± 12.6 | 10 (76.9%) | 12 | 63.5 ± 11.3 | 6 (50.0%) |
| Outcome | No. of Studies | Event/Participants or Mean ± SD | Events | Heterogeneity between Trials | p-Value for Differences across Groups | |||
|---|---|---|---|---|---|---|---|---|
| LLR | RLR | OR or MD | 95%CI | p-Value | I2 Statistics | |||
| Sex, male | 7 | 1383/2330 (59.4%) | 270/443 (60.9%) | 0.92 | 0.74 to 1.15 | 0.22 | 28% | 0.49 |
| Age, years | 7 | 63.5 ± 11.3 | 60.9 ± 10.6 | 1.21 | 0.39 to 2.02 | 0.87 | 0% | 0.004 |
| BMI | 6 | 25.97 ± 4.37 | 26.11 ± 5.66 | −0.49 | −1.11 to 0.13 | 0.04 | 58% | 0.12 |
| Prior abdominal surgery | 6 | 1602/2269 (70.6%) | 248/382 (64.9%) | 0.97 | 0.74 to 1.26 | 0.36 | 9% | 0.80 |
| Prior chemotherapy | 4 | 575/966 (59.5%) | 115/215 (53.5%) | 0.97 | 0.70 to 1.34 | 0.82 | 0% | 0.85 |
| Liver cirrhosis | 2 | 48/597 (8.0%) | 13/101 (12.9%) | 0.70 | 0.22 to 2.19 | 0.12 | 58% | 0.54 |
| Preoperative CEA | 2 | 260.2 ± 162.5 | 61.62 ± 206.2 | 73.51 | −290.02 to 437.004 | 0.002 | 90% | 0.69 |
| Outcome | No. of Studies | Event/Participants or Mean ± SD | Events | Heterogeneity between Trials | p-Value for Differences across Groups | |||
|---|---|---|---|---|---|---|---|---|
| LLR | RLR | OR or MD | 95%CI | p-Value | I2 Statistics | |||
| Major resection | 3 | 261/1344 (19.4%) | 19/117 (16.2%) | 1.15 | 0.29 to 4.47 | 0.008 | 79% | 0.84 |
| Minor resection | 3 | 1078/1344 (80.2%) | 98/117 (83.8%) | 0.86 | 0.21 to 3.47 | 0.006 | 80% | 0.83 |
| Pringle maneuver | 4 | 881/1735 (50.8%) | 78/255 (30.6%) | 3.33 | 1.53 to 7.22 | 0.002 | 79% | 0.002 |
| Tumor size | 4 | 3.94± 2.37 | 4.01 ± 1.82 | 0.03 | −0.56 to 0.63 | 0.005 | 76% | 0.91 |
| Intraoperative blood loss (mL) | 6 | 294.3 ± 312.0 | 190.8 ± 118.7 | 178.68 | 101.82 to 255.53 | <0.001 | 99% | <0.001 |
| Intraoperative transfusion | 5 | 568/1891 (30.0%) | 34/354 (9.6%) | 2.29 | 0.79 to 6.63 | <0.001 | 82% | 0.13 |
| Conversion to open | 6 | 312/2522 (12.4%) | 30/449 (6.7%) | 2.18 | 1.46 to 3.24 | 0.76 | 0% | <0.001 |
| R1 resection | 4 | 328/1457 (22.5%) | 39/225 (17.3%) | 1.32 | 0.70 to 2.46 | 0.16 | 42% | 0.39 |
| Operative time, min | 7 | 272.9 ± 97.4 | 247.9 ± 81.5 | 21.50 | −5.28 to 48.28 | <0.001 | 97% | 0.12 |
| Outcome | No. of Studies | Event/Participants or Mean ± SD | Events | Heterogeneity between Trials | p-Value for Differences across Groups | |||
|---|---|---|---|---|---|---|---|---|
| LLR | RLR | OR or MD | 95%CI | p-Value | I2 Statistics | |||
| Mortality | ||||||||
| Intraoperative | 1 | 0/953 (0.0%) | 0/77 (0.0%) | NE | NE | NA | NA | NA |
| 30-day | 2 | 13/1931 (0.7%) | 2/372 (0.5%) | 1.23 | 0.32 to 4.83 | 0.66 | 0% | 0.76 |
| 90-day | 5 | 10/789 (1.3%) | 0/178 (0.0%) | 1.78 | 0.23 to 14.03 | 0.35 | 0% | 0.58 |
| 1-year | 3 | 32/176 (18.2%) | 14/176 (8.0%) | 2.56 | 0.94 to 6.98 | 0.15 | 53% | 0.07 |
| 2-years | 2 | 60/176 (34.1%) | 47/176 (26.7%) | 1.42 | 0.90 to 2.24 | 0.69 | 0% | 0.13 |
| 3-years | 2 | 92/176 (52.3%) | 85/176 (48.3%) | 1.17 | 0.77 to 1.78 | 0.56 | 0% | 0.46 |
| Hospital length of stay, days | 7 | 5.6 ± 2.5 | 5.8 ± 2.1 | 0.34 | −0.59 to 1.28 | <0.001 | 99% | 0.47 |
| 30-days complications | ||||||||
| Total postoperative complications | 7 | 404/1806 (22.4%) | 106/482 (21.9%) | 1.04 | 0.81 to 1.32 | 0.25 | 26% | 0.78 |
| Major complications | 7 | 167/2123 (7.9%) | 28/449 (6.2%) | 1.37 | 0.91 to 2.08 | 0.31 | 17% | 0.13 |
| Ascites | 1 | 7/953 (0.7%) | 0/77 (0.0%) | 1.23 | 0.07 to 21.71 | NA | NA | 0.89 |
| Haemorrhage | 2 | 19/1014 (1.9%) | 0/138 (0.0%) | 3.06 | 0.37 to 25.50 | 1.00 | 0% | 0.30 |
| Coagulopathy | 1 | 4/953 (0.4%) | 0/77 (0.0%) | 0.73 | 0.04 to 13.77 | NA | NA | 0.84 |
| Biliary fistula | 2 | 25/1014 (2.5%) | 0/138 (0.0%) | 4.45 | 0.56 to 35.20 | 0.89 | 0% | 0.16 |
| Bowel complications | 1 | 34/953 (3.6%) | 0/77 (0.0%) | 5.82 | 0.35 to 95.77 | NA | NA | 0.22 |
| Surgical site infection | 1 | 17/953 (1.8%) | 1/77 (1.3%) | 1.38 | 0.18 to 10.51 | NA | NA | 0.76 |
| Intra-abdominal abscess | 2 | 32/1014 (3.2%) | 3/138 (2.2%) | 1.39 | 0.40 to 4.84 | 0.72 | 0% | 0.60 |
| Pneumonia | 1 | 19/953 (2.0%) | 2/77 (2.6%) | 0.76 | 0.17 to 3.34 | NA | NA | 0.72 |
| Pleural effusion | 2 | 28/1014 (2.8%) | 6/138 (4.3%) | 0.62 | 0.15 to 2.55 | 0.22 | 34% | 0.50 |
| Pneumothorax | 1 | 2/953 (0.2%) | 0/77 (0.0%) | 0.41 | 0.02 to 8.56 | NA | NA | 0.56 |
| Deep vein thrombosis | 1 | 2/953 (0.2%) | 0/77 (0.0%) | 0.41 | 0.02 to 8.56 | NA | NA | 0.56 |
| Pulmonary embolism | 1 | 1/953 (0.1%) | 0/77 (0.0%) | 0.24 | 0.01 to 6.04 | NA | NA | 0.39 |
| Posthepatectomy liver failure | 1 | 5/953 (0.5%) | 0/77 (0.0%) | 0.90 | 0.05 to 16.41 | NA | NA | 0.94 |
| 30-d readmission | 4 | 49/598 (8.2%) | 16/267 (6.0%) | 1.39 | 0.76 to 2.56 | 0.46 | 0% | 0.29 |
| 30-d reoperation | 4 | 18/600 (3.0%) | 4/267 (1.5%) | 1.72 | 0.61 to 4.87 | 0.57 | 0% | 0.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Safiejko, K.; Pedziwiatr, M.; Pruc, M.; Tarkowski, R.; Juchimiuk, M.; Domurat, M.; Smereka, J.; Anvarov, K.; Sielicki, P.; Kurek, K.; et al. Robotic versus Laparoscopic Liver Resections for Colorectal Metastases: A Systematic Review and Meta-Analysis. Cancers 2024, 16, 1596. https://doi.org/10.3390/cancers16081596
Safiejko K, Pedziwiatr M, Pruc M, Tarkowski R, Juchimiuk M, Domurat M, Smereka J, Anvarov K, Sielicki P, Kurek K, et al. Robotic versus Laparoscopic Liver Resections for Colorectal Metastases: A Systematic Review and Meta-Analysis. Cancers. 2024; 16(8):1596. https://doi.org/10.3390/cancers16081596
Chicago/Turabian StyleSafiejko, Kamil, Michal Pedziwiatr, Michal Pruc, Radoslaw Tarkowski, Marcin Juchimiuk, Marian Domurat, Jacek Smereka, Khikmat Anvarov, Przemyslaw Sielicki, Krzysztof Kurek, and et al. 2024. "Robotic versus Laparoscopic Liver Resections for Colorectal Metastases: A Systematic Review and Meta-Analysis" Cancers 16, no. 8: 1596. https://doi.org/10.3390/cancers16081596