Seroprevalence of SARS-CoV-2 and Hepatitis B Virus Coinfections among Ethiopians with Acute Leukemia

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data and Sample Collection
2.3. SARS-CoV-2 Seroprevalence Testing
2.4. HBV Laboratory Testing
2.5. HIV Laboratory Testing
2.6. HCV Laboratory Testing
2.7. Quality Assurance
2.8. Data Analysis
2.9. Ethical Clearance
3. Results
3.1. Sociodemographic and Clinical Characteristics of Study Participants
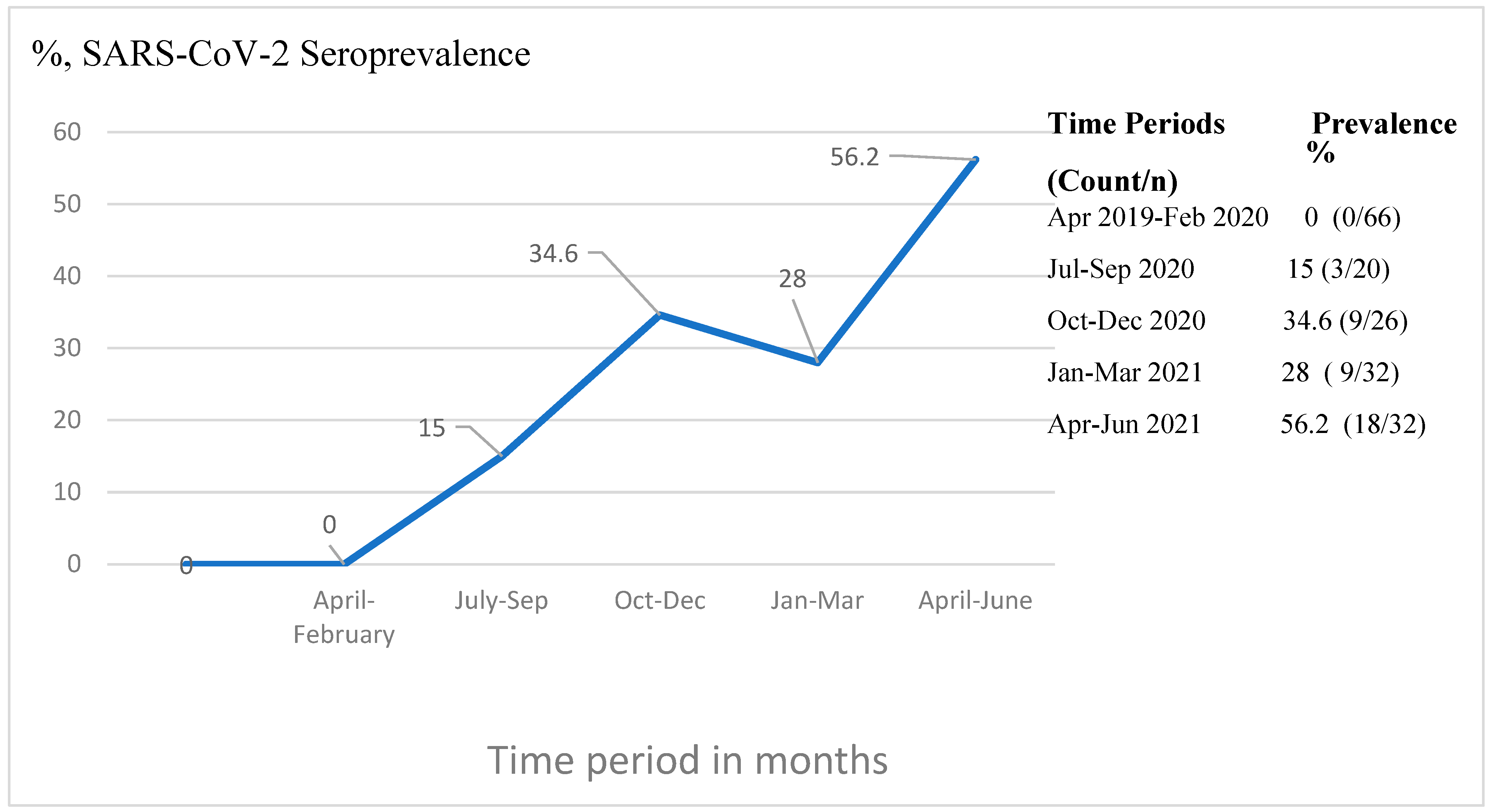
3.2. Seroprevalence of SARS-CoV-2 and Its Distribution
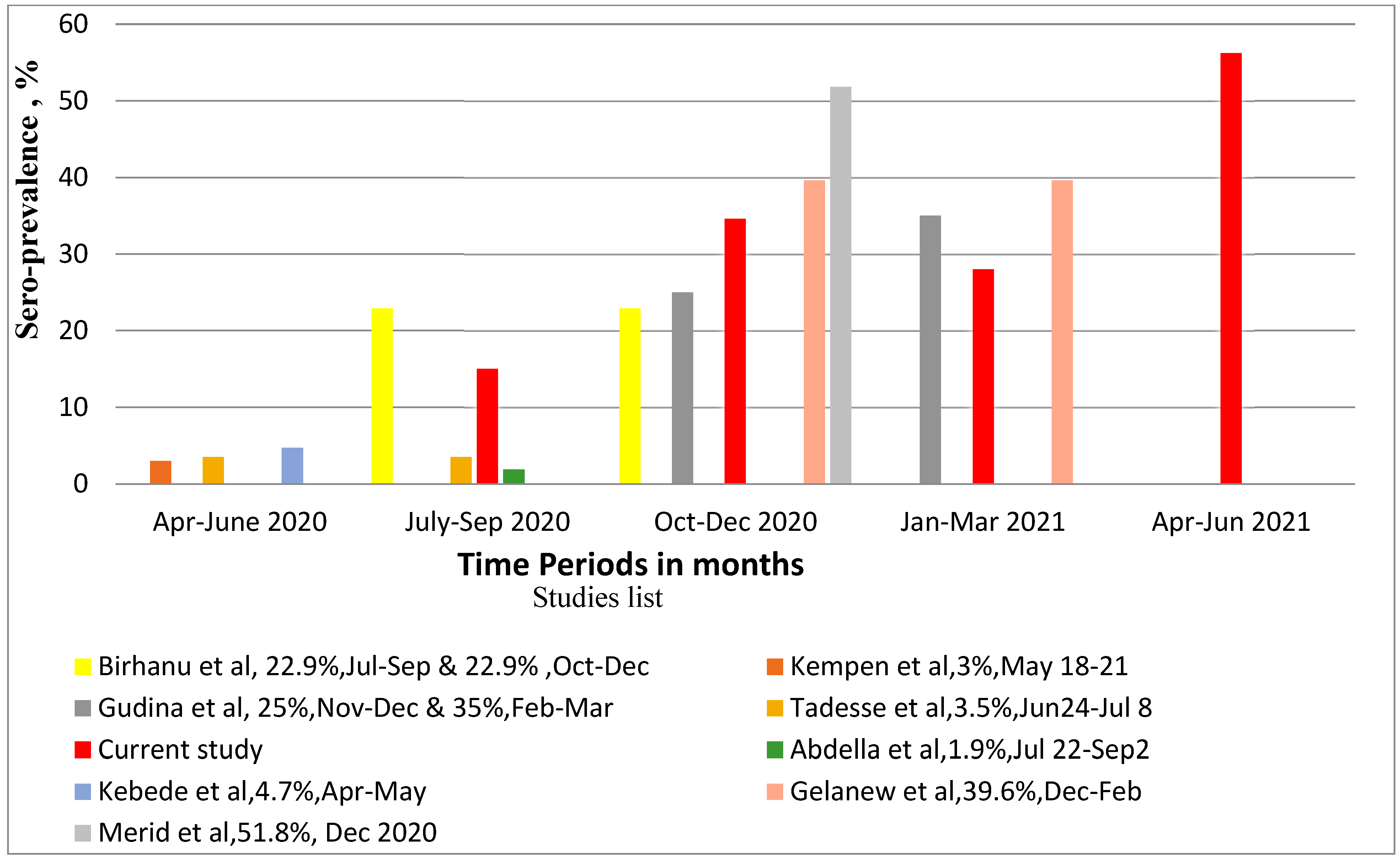
3.3. Seroprevalence of SARS-CoV-2 in Relation to Other Studies in Ethiopia
3.4. Blood-Borne Virus Distribution and Association with SARS-CoV-2 Seropositivity
4. Discussion
4.1. Strength
4.2. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J.A.; Tullius, B.P.; Lamb, M.G.; Sayegh, R.; Stanek, J.R.; Auletta, J.J. COVID-19 in immunocompromised patients: A systematic review of cancer, hematopoietic cell and solid organ transplant patients. J. Infect. 2021, 82, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Finelli, C.; Parisi, S. The clinical impact of COVID-19 epidemic in the hematologic setting. Adv. Biol. Regul. 2020, 77, 100742–100747. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Willan, J.; King, A.J.; Hayes, S.; Collins, G.P.; Peniket, A. Care of haematology patients in a COVID-19 epidemic. Br. J. Haematol. 2020, 189, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Yan, Y.; Wang, L. Coronavirus disease 2019: Coronaviruses and blood safety. Transfus. Med. Rev. 2020, 34, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-C.; Huang, D.Q.; Nguyen, M.H. Global burden of hepatitis B virus: Current status, missed opportunities and a call for action. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 524–537. [Google Scholar] [CrossRef]
- Iannacone, M.; Guidotti, L.G. Immunobiology and pathogenesis of hepatitis B virus infection. Nat. Rev. Immunol. 2022, 22, 19–32. [Google Scholar] [CrossRef]
- Yang, S.; Wang, S.; Du, M.; Liu, M.; Liu, Y.; He, Y. Patients with COVID-19 and HBV Coinfection are at Risk of Poor Prognosis. Infect. Dis. Ther. 2022, 11, 1229–1242. [Google Scholar] [CrossRef]
- Shoraka, S.; Mohebbi, S.R.; Hosseini, S.M.; Ghaemi, A.; Zali, M.R. SARS-CoV-2 and chronic hepatitis B: Focusing on the possible consequences of co-infection. J. Clin. Virol. Plus 2023, 3, 100167–100170. [Google Scholar] [CrossRef]
- Lin, Y.; Yuan, J.; Long, Q.; Hu, J.; Deng, H.; Zhao, Z.; Chen, J.; Lu, M.; Huang, A. Patients with SARS-CoV-2 and HBV co-infection are at risk of greater liver injury. Genes Dis. 2021, 8, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, S.D.; Unger, J.M.; Baker, L.H.; Little, R.F.; Loomba, R.; Hwang, J.P.; Chugh, R.; Konerman, M.A.; Arnold, K.; Menter, A.R. Prevalence of hepatitis B virus, hepatitis C virus, and HIV infection among patients with newly diagnosed cancer from academic and community oncology practices. JAMA Oncol. 2019, 5, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Mallet, V.; van Bömmel, F.; Doerig, C.; Pischke, S.; Hermine, O.; Locasciulli, A.; Cordonnier, C.; Berg, T.; Moradpour, D.; Wedemeyer, H. Management of viral hepatitis in patients with haematological malignancy and in patients undergoing haemopoietic stem cell transplantation: Recommendations of the 5th European Conference on Infections in Leukaemia (ECIL-5). Lancet Infect. Dis. 2016, 16, 606–617. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO Africa). First Case of COVID-19 Confirmed in Ethiopia. Available online: https://www.afro.who.int/news/first-case-covid-19-confirmed-ethiopia#:~:text=March%2013%2C%202020%2C%20The%20Federal,in%20China%20in%20December%202019 (accessed on 24 June 2023).
- WHO. COVID-19 Update in Ethiopia. Available online: https://covid19.who.int/region/afro/country/et (accessed on 19 December 2023).
- Cabezón-Gutiérrez, L.; Custodio-Cabello, S.; Palka-Kotlowska, M.; Oliveros-Acebes, E.; García-Navarro, M.J.; Khosravi-Shahi, P. Seroprevalence of SARS-CoV-2–specific antibodies in cancer outpatients in Madrid (Spain): A single center, prospective, cohort study and a review of available data. Cancer Treat. Rev. 2020, 90, 102102–102106. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Chen, L.; Chen, L.; Yuan, G.; Fang, Y.; Chen, W.; Wu, D.; Liang, B.; Lu, X.; Ma, Y. COVID-19 in persons with haematological cancers. Leukemia 2020, 34, 1637–1645. [Google Scholar] [CrossRef] [PubMed]
- Gavillet, M.; Klappert, J.C.; Spertini, O.; Blum, S. Acute leukemia in the time of COVID-19. Leuk. Res. 2020, 92, 106353–106356. [Google Scholar] [CrossRef]
- Gelanew, T.; Seyoum, B.; Mulu, A.; Mihret, A.; Abebe, M.; Wassie, L.; Gelaw, B.; Sorsa, A.; Merid, Y.; Muchie, Y. High seroprevalence of anti-SARS-CoV-2 antibodies among Ethiopian healthcare workers. BMC Infect. Dis. 2022, 22, 261. [Google Scholar] [CrossRef] [PubMed]
- Alemu, J.; Gumi, B.; Tsegaye, A.; Abubeker, A.; Tadesse, F.; Shewaye, A.; Rahimeto, Z.; Mihret, A.; Mulu, A.; Gebremedhin, A. Frequency of viral infections in adolescent and adult in-patient Ethiopians with acute leukemia at presentation to a tertiary care teaching hospital: A cross-sectional study. Infect. Agents Cancer 2023, 18, 44–50. [Google Scholar] [CrossRef]
- Kebede, F.; Kebede, T.; Kebede, B. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) IgG-antibody seroprevalence among quarantined population, during the first wave of COVID-19 pandemic, In North West Ethiopia (from 30 April to 30 May 2020). SAGE Open Med. 2022, 10, 20503121221076931. [Google Scholar] [CrossRef]
- Birhanu, A.; Ayana, G.M.; Bayu, M.; Mohammed, A.; Dessie, Y. Features associated with SARS-COV-2 positivity among people presenting with acute respiratory tract infections to public Hospitals in Harari region, Ethiopia. SAGE Open Med. 2021, 9, 20503121211062793. [Google Scholar] [CrossRef] [PubMed]
- Kempen, J.H.; Abashawl, A.; Suga, H.K.; Difabachew, M.N.; Kempen, C.J.; Debele, M.T.; Menkir, A.A.; Assefa, M.T.; Asfaw, E.H.; Habtegabriel, L.B. SARS-CoV-2 serosurvey in Addis Ababa, Ethiopia. Am. J. Trop. Med. Hyg. 2020, 103, 2022–2023. [Google Scholar] [CrossRef] [PubMed]
- Tadesse, E.B.; Endris, A.A.; Solomon, H.; Alayu, M.; Kebede, A.; Eshetu, K.; Teka, G.; Seid, B.E.; Ahmed, J.; Abayneh, S.A. Seroprevalence and risk factors for SARS-CoV-2 Infection in selected urban areas in Ethiopia: A cross-sectional evaluation during July 2020. Int. J. Infect. Dis. 2021, 111, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Gudina, E.K.; Ali, S.; Girma, E.; Gize, A.; Tegene, B.; Hundie, G.B.; Sime, W.T.; Ambachew, R.; Gebreyohanns, A.; Bekele, M. Seroepidemiology and model-based prediction of SARS-CoV-2 in Ethiopia: Longitudinal cohort study among front-line hospital workers and communities. Lancet Glob. Health 2021, 9, e1517–e1527. [Google Scholar] [CrossRef] [PubMed]
- Merid, Y.; Tekleselasie, W.; Tesfaye, E.; Gadisa, A.; Fentahun, D.; Abate, A.; Alemu, A.; Mihret, A.; Mulu, A.; Gelanew, T. SARS-CoV-2 Infection-and mRNA Vaccine-induced Humoral Immunity among Schoolchildren in Hawassa, Ethiopia. Front. Immunol. 2023, 14, 1163688. [Google Scholar] [CrossRef] [PubMed]
- Abdella, S.; Riou, S.; Tessema, M.; Assefa, A.; Seifu, A.; Blachman, A.; Abera, A.; Moreno, N.; Irarrazaval, F.; Tollera, G. Prevalence of SARS-CoV-2 in urban and rural Ethiopia: Randomized household serosurveys reveal level of spread during the first wave of the pandemic. eClinicalMedicine 2021, 35, 100880–100886. [Google Scholar] [CrossRef] [PubMed]
- Jazieh, A.-R.; Alenazi, T.H.; Alhejazi, A.; Al Safi, F.; Al Olayan, A. Outcome of oncology patients infected with coronavirus. JCO Glob. Oncol. 2020, 6, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Oh, W.K. COVID-19 infection in cancer patients: Early observations and unanswered questions. Ann. Oncol. 2020, 31, 838–839. [Google Scholar] [CrossRef] [PubMed]
- Langerbeins, P.; Hallek, M. COVID-19 in patients with hematologic malignancy. Blood 2022, 140, 236–252. [Google Scholar] [CrossRef]
- Paul, S.; Rausch, C.R.; Jain, N.; Kadia, T.; Ravandi, F.; DiNardo, C.D.; Welch, M.A.; Dabaja, B.S.; Daver, N.; Garcia-Manero, G. Treating leukemia in the time of COVID-19. Acta Haematol. 2021, 144, 132–145. [Google Scholar] [CrossRef]
- Bonifacio, M.; Tiribelli, M.; Miggiano, M.C.; Abruzzese, E.; Binotto, G.; Scaffidi, L.; Cordioli, M.; Damiani, D.; Di Bona, E.; Trawinska, M.M. The serological prevalence of SARS-CoV-2 infection in patients with chronic myeloid leukemia is similar to that in the general population. Cancer Med. 2021, 10, 6310–6316. [Google Scholar] [CrossRef] [PubMed]
- Claudiani, S.; Rosadas, C.; McClure, M.; Khan, M.; Tedder, R.S.; Innes, A.J.; Milojkovic, D.; Apperley, J. Prevalence of Sars-Cov-2 infection in patients with chronic myeloid leukemia. Blood 2020, 136, 20–22. [Google Scholar] [CrossRef]
- Kgatle, M.; Das, R.; Lawal, I.; Boshomane, T.; Mokoala, K.; Gaspar, C.; Mbokazi, L.; Nkambule, N.; Gow, V.; Ndlovu, H. The SARS-COV-2 Seroprevalence among Oncology Patients. J. Clin. Med. 2023, 12, 529. [Google Scholar] [CrossRef] [PubMed]
- Gedefie, A.; Tilahun, M.; Fiseha, M.; Alemayehu, E.; Shibabaw, A.; Bisetegn, H.; Debash, H.; Kassa, Y.; Ali, A.; Seid, A. Epidemiology of SARS-CoV-2 Infection in Ethiopia: A Systematic Review and Meta-Analysis. COVID 2023, 3, 703–714. [Google Scholar] [CrossRef]
- Sisay, A.; Tshiabuila, D.; van Wyk, S.; Tesfaye, A.; Mboowa, G.; Oyola, S.O.; Tesema, S.K.; Baxter, C.; Martin, D.; Lessells, R. Molecular epidemiology and diversity of SARS-CoV-2 in Ethiopia, 2020–2022. Genes 2023, 14, 705. [Google Scholar] [CrossRef] [PubMed]
- O’Nions, J.; Muir, L.; Zheng, J.; Rees-Spear, C.; Rosa, A.; Roustan, C.; Earl, C.; Cherepanov, P.; Gupta, R.; Khwaja, A. SARS-CoV-2 antibody responses in patients with acute leukaemia. Leukemia 2021, 35, 289–292. [Google Scholar] [CrossRef]
- Chen, X.; Jiang, Q.; Ma, Z.; Ling, J.; Hu, W.; Cao, Q.; Mo, P.; Yao, L.; Yang, R.; Gao, S. Clinical characteristics of hospitalized patients with SARS-CoV-2 and hepatitis B virus co-infection. Virol. Sin. 2020, 35, 842–845. [Google Scholar] [CrossRef]
- Fuentes-Prior, P. Priming of SARS-CoV-2 S protein by several membrane-bound serine proteinases could explain enhanced viral infectivity and systemic COVID-19 infection. J. Biol. Chem. 2021, 296, 100135–100152. [Google Scholar] [CrossRef]
- Sebastián-Martín, A.; Sánchez, B.G.; Mora-Rodríguez, J.M.; Bort, A.; Díaz-Laviada, I. Role of dipeptidyl peptidase-4 (DPP4) on COVID-19 physiopathology. Biomedicines 2022, 10, 2026. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Anti-SARS-CoV-2 RBD-IgG Detection | Total Count (%) | p Value * | |
|---|---|---|---|---|
| Positive, n (%) | Negative, n (%) | |||
| Sex | 0.901 | |||
| Male | 23 (36) | 41 (64) | 64 (58) | |
| Female | 16 (35) | 30 (65) | 46 (42) | |
| Age group (in years) | 0.452 | |||
| 13–17 | 5 (26) | 14 (74) | 19 (17.3) | |
| 18–39 | 27 (40) | 41 (60) | 68 (61.8) | |
| 40–59 | 6 (38) | 10 (62) | 16 (14.5) | |
| 60 and above | 1 (14) | 6 (86) | 7 (6.4) | |
| Residency | 0.833 | |||
| Addis Ababa | 5 (56) | 4 (44) | 9 (9) | |
| Other regions in Ethiopia | 30 (33) | 60 (67) | 90 (91) | |
| Leukemia Diagnosis | 0.407 | |||
| ALL | 16 (31) | 36 (69) | 52 (47.3) | |
| AML | 17 (39) | 27 (61) | 44 (40) | |
| CML with blast crisis | 0 (0) | 2 (100) | 2 (1.8) | |
| Acute leukemia, not specified | 6 (50) | 6 (50) | 12 (10.9) | |
| Blood-Borne Viral Infections | Viral Markers | Viral Marker Detection | Anti-SARS-CoV-2 RBD-IgG Detection | Total Count (%) | p Value * | |
|---|---|---|---|---|---|---|
| Positive, n (%) | Negative, n (%) | |||||
| HBV | HBsAg | Positive | 7 (50) | 7 (50) | 14 (12.7) | 0.223 |
| Negative | 32 (33) | 64 (67) | 96 (87.2) | |||
| HBV-DNA | Positive | 4 (36) | 7 (64) | 11 (10) | 0.947 | |
| Negative | 35 (35) | 64 (65) | 99 (90) | |||
| Total HBV | Positive | 11 (44) | 14 (56) | 25 (22.7) | 0.310 | |
| (HBsAg + HBV-DNA) | Negative | 28 (33) | 57 (67) | 85 (77.3) | ||
| HIV | Anti-HIV | Positive | 1 (33) | 2 (67) | 3 (2.7) | 0.938 |
| Negative | 38 (36) | 69 (64) | 107 (97.3) | |||
| HCV | Anti-HCV | Positive | 0 | 0 | 0 (0) | --- |
| Negative | 39 (35) | 71 (65) | 110 (100) | |||
| Leukemia Diagnosis | HBV Infection Status | Total | * p Value | |
|---|---|---|---|---|
| Positive | Negative | |||
| ALL | 4 | 14 | 11 | 0.2273 |
| AML | 7 | 10 | 28 | |
| Total | 11 | 24 | 35 | |
| Number of Cases with Indicated Serostatus | ALT Level | Total | * p Value | |
|---|---|---|---|---|
| 0–45 IU/mL | ≥46 IU/mL | |||
| SARS-CoV-2 Pos, HBV pos | 10 | 1 | 11 | 0.6624 |
| SARS-CoV-2 Neg, HBV pos | 24 | 4 | 28 | |
| Total | 34 | 5 | 39 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alemu, J.; Gumi, B.; Tsegaye, A.; Rahimeto, Z.; Fentahun, D.; Ibrahim, F.; Abubeker, A.; Gebremedhin, A.; Gelanew, T.; Howe, R. Seroprevalence of SARS-CoV-2 and Hepatitis B Virus Coinfections among Ethiopians with Acute Leukemia. Cancers 2024, 16, 1606. https://doi.org/10.3390/cancers16081606
Alemu J, Gumi B, Tsegaye A, Rahimeto Z, Fentahun D, Ibrahim F, Abubeker A, Gebremedhin A, Gelanew T, Howe R. Seroprevalence of SARS-CoV-2 and Hepatitis B Virus Coinfections among Ethiopians with Acute Leukemia. Cancers. 2024; 16(8):1606. https://doi.org/10.3390/cancers16081606
Chicago/Turabian StyleAlemu, Jemal, Balako Gumi, Aster Tsegaye, Ziyada Rahimeto, Dessalegn Fentahun, Fozia Ibrahim, Abdulaziz Abubeker, Amha Gebremedhin, Tesfaye Gelanew, and Rawleigh Howe. 2024. "Seroprevalence of SARS-CoV-2 and Hepatitis B Virus Coinfections among Ethiopians with Acute Leukemia" Cancers 16, no. 8: 1606. https://doi.org/10.3390/cancers16081606