
A Multicenter International Retrospective Investigation Assessing the Prognostic Role of Inflammation-Based Scores (Neutrophil-to-Lymphocyte, Lymphocyte-to-Monocyte, and Platelet-to-Lymphocyte Ratios) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations of the Liver

 , , , , , , , , ,
, , , , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Treatment
2.3. Outcomes and Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
- -
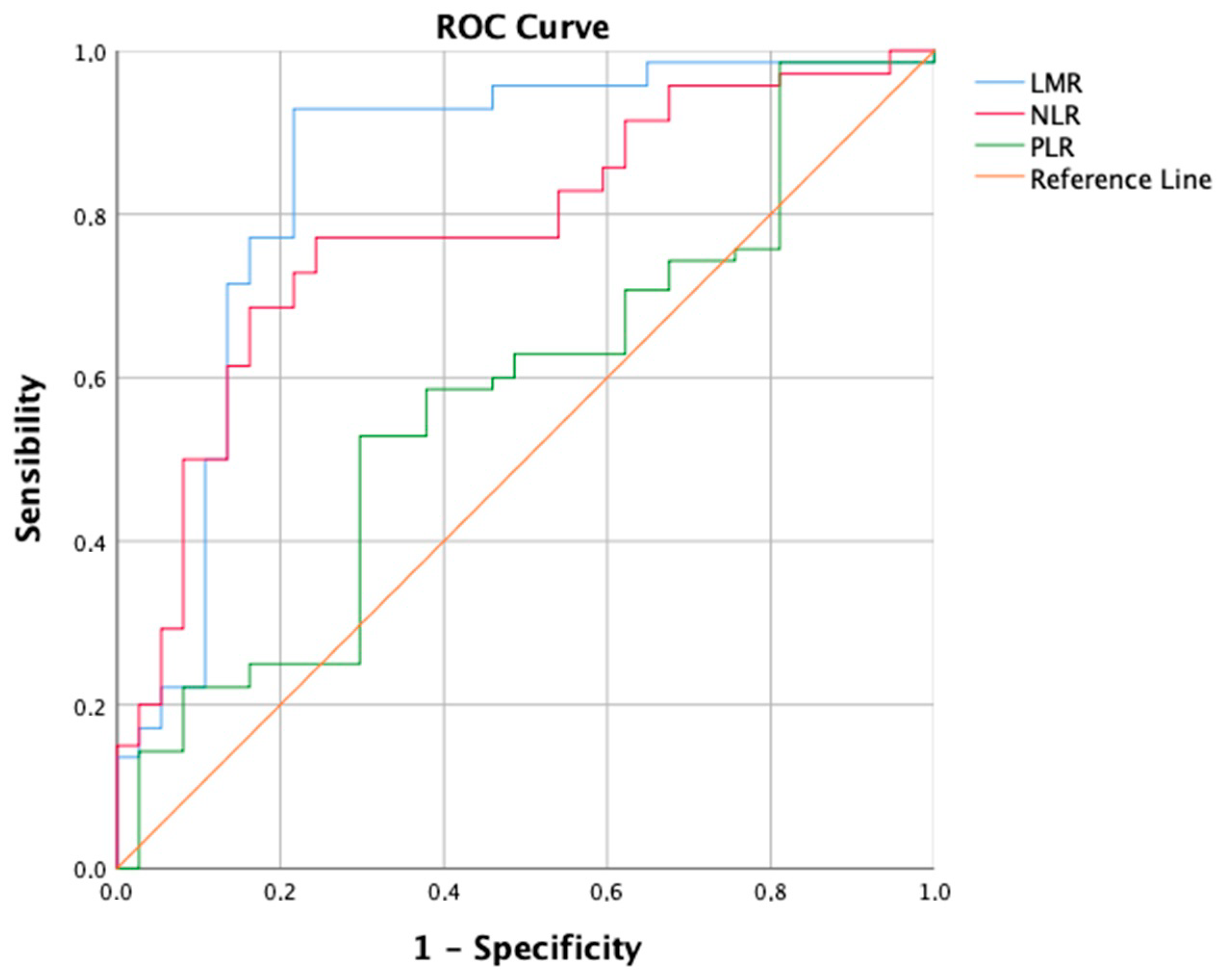
- In patients with intermediate-stage HCC undergoing TACE, LMR demonstrates a good predictive value for short-term outcomes like 6-month PFS, while NLR shows a moderate accuracy according to ROC analysis. Conversely, PLR’s predictive performance is only marginally better than random chance.
- -
- One hundred-and-forty-four patients have a high LMR (≥2.24), also exhibiting better objective response (42.4% vs. 14.3%, p < 0.001) and 6-month PFS (75% vs. 45.7%, p < 0.001) rates compared to patients with low LMR. One hundred-and-one patients have a low NLR (<4.72), also showing better objective response (45.5% vs. 22.1%, p < 0.001) and 6-month PFS (78.2% vs. 54%, p < 0.001) rates compared to patients with high NLR. Notably, high LMR alone is also linked to higher Complete Response (13.9% vs. 0%, p = 0.001) and 6-month successful downstaging (15.3% vs. 0%, p = 0.001) rates.
- -
- Among the leukocyte components comprising LMR and NLR, only lymphocyte count remains a robust predictor of Objective Response in both simple and multiple logistic regression analyses. Furthermore, in the multiple logistic regression model, both lymphocyte and monocyte counts significantly predict 6-month PFS.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; de Lope, C.R.; Bruix, J. Current Strategy for Staging and Treatment: The BCLC Update and Future Prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Yao, F.Y.; Mehta, N.; Flemming, J.; Dodge, J.; Hameed, B.; Fix, O.; Hirose, R.; Fidelman, N.; Kerlan, R.K., Jr.; Roberts, J.P. Downstaging of hepatocellular cancer before liver transplant: Long-term outcome compared to tumors within Milan criteria. Hepatology 2015, 61, 1968–1977. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of Patients with Intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a Subclassification to Facilitate Treatment Decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef]
- Kudo, M.; Arizumi, T.; Ueshima, K.; Sakurai, T.; Kitano, M.; Nishida, N. Subclassification of BCLC B Stage Hepatocellular Carcinoma and Treatment Strategies: Proposal of Modified Bolondi’s Subclassification (Kinki Criteria). Dig. Dis. 2015, 33, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Bugada, D.; Allegri, M.; Lavand’Homme, P.; De Kock, M.; Fanelli, G. Inflammation-Based Scores: A New Method for Patient-Targeted Strategies and Improved Perioperative Outcome in Cancer Patients. BioMed Res. Int. 2014, 2014, 142425. [Google Scholar] [CrossRef]
- Rossi, J.-F.; Lu, Z.Y.; Massart, C.; Levon, K. Dynamic Immune/Inflammation Precision Medicine: The Good and the Bad Inflammation in Infection and Cancer. Front. Immunol. 2021, 12, 595722. [Google Scholar] [CrossRef]
- Minici, R.; Siciliano, M.A.; Ammendola, M.; Santoro, R.C.; Barbieri, V.; Ranieri, G.; Laganà, D. Prognostic Role of Neutrophil-to-Lymphocyte Ratio (NLR), Lymphocyte-to-Monocyte Ratio (LMR), Platelet-to-Lymphocyte Ratio (PLR) and Lymphocyte-to-C Reactive Protein Ratio (LCR) in Patients with Hepatocellular Carcinoma (HCC) undergoing Chemoembolizations (TACE) of the Liver: The Unexplored Corner Linking Tumor Microenvironment, Biomarkers and Interventional Radiology. Cancers 2022, 15, 257. [Google Scholar] [CrossRef]
- Fan, W.; Liu, Y.; Shi, M.; Chen, S.; Wan, W.; Shen, L.; Shen, B.; Qi, H.; Cao, F.; Wu, Y.; et al. Intermediate stage hepatocellular carcinoma: Comparison of the value of inflammation-based scores in predicting progression-free survival of patients receiving transarterial chemoembolization. J. Cancer Res. Ther. 2021, 17, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Barzi, A.; Zhou, K.; Wang, S.; Dodge, J.L.; El-Khoueiry, A.; Setiawan, V.W. Etiology and Outcomes of Hepatocellular Carcinoma in an Ethnically Diverse Population: The Multiethnic Cohort. Cancers 2021, 13, 3476. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Gaba, R.C.; Lokken, R.P.; Hickey, R.M.; Lipnik, A.J.; Lewandowski, R.J.; Salem, R.; Brown, D.B.; Walker, T.G.; Silberzweig, J.E.; Baerlocher, M.O.; et al. Quality Improvement Guidelines for Transarterial Chemoembolization and Embolization of Hepatic Malignancy. J. Vasc. Interv. Radiol. 2017, 28, 1210–1223.e3. [Google Scholar] [CrossRef] [PubMed]
- Lucatelli, P.; Burrel, M.; Guiu, B.; de Rubeis, G.; van Delden, O.; Helmberger, T. CIRSE Standards of Practice on Hepatic Transarterial Chemoembolisation. Cardiovasc. Interv. Radiol. 2021, 44, 1851–1867. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; De Baere, T.; Burrel, M.; Caridi, J.G.; Lammer, J.; Malagari, K.; Martin, R.C.G.; O’Grady, E.; Real, M.I.; Vogl, T.J.; et al. Transcatheter Treatment of Hepatocellular Carcinoma with Doxorubicin-loaded DC Bead (DEBDOX): Technical Recommendations. Cardiovasc. Interv. Radiol. 2012, 35, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Lammer, J.; Malagari, K.; Vogl, T.; Pilleul, F.; Denys, A.; Watkinson, A.; Pitton, M.; Sergent, G.; Pfammatter, T.; Terraz, S.; et al. Prospective Randomized Study of Doxorubicin-Eluting-Bead Embolization in the Treatment of Hepatocellular Carcinoma: Results of the PRECISION V Study. Cardiovasc. Interv. Radiol. 2010, 33, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, M.; Chen, M.; Mei, J.; Xu, L.; Guo, R.; Lin, X.; Li, J.; Peng, Z. Association of Sustained Response Duration With Survival After Conventional Transarterial Chemoembolization in Patients With Hepatocellular Carcinoma. JAMA Netw. Open 2018, 1, e183213. [Google Scholar] [CrossRef]
- Rossi, R.; Talarico, M.; Pascale, A.; Pascale, V.; Minici, R.; Boriani, G. Low Levels of Vitamin D and Silent Myocardial Ischemia in Type 2 Diabetes: Clinical Correlations and Prognostic Significance. Diagnostics 2022, 12, 2572. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; Ierardi, A.M.; Petullà, M.; Bracale, U.M.; Carrafiello, G.; Laganà, D. Thoracic endovascular repair for blunt traumatic thoracic aortic injury: Long-term results. Vascular 2022, 32, 5–18. [Google Scholar] [CrossRef]
- Bracale, U.M.; Peluso, A.; Panagrosso, M.; Cecere, F.; DEL Guercio, L.; Minici, R.; Giannotta, N.; Ielapi, N.; Licastro, N.; Serraino, G.F.; et al. Ankle-Brachial Index evaluation in totally percutaneous approach vs. femoral artery cutdown for endovascular aortic repair of abdominal aortic aneurysms. Chirurgia 2022, 35, 349–354. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; Giurdanella, M.; Talarico, M.; Siciliano, M.A.; Carrafiello, G.; Laganà, D. Efficacy and Safety of Distal Radial Access for Transcatheter Arterial Chemoembolization (TACE) of the Liver. J. Pers. Med. 2023, 13, 640. [Google Scholar] [CrossRef] [PubMed]
- Minici, R.; Venturini, M.; Fontana, F.; Guzzardi, G.; Pingitore, A.; Piacentino, F.; Serra, R.; Coppola, A.; Santoro, R.; Laganà, D. Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study. Medicina 2023, 59, 710. [Google Scholar] [CrossRef]
- Minici, R.; Fontana, F.; Venturini, M.; Guzzardi, G.; Siciliano, A.; Piacentino, F.; Serra, R.; Coppola, A.; Guerriero, P.; Apollonio, B.; et al. Transcatheter Arterial Embolization (TAE) in the Management of Bleeding in the COVID-19 Patient. Medicina 2023, 59, 1062. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.-F.; Zhuang, L.-P.; Zhang, C.-Y.; Ning, Z.-Y.; Wang, D.; Sheng, J.; Hua, Y.-Q.; Xie, J.; Xu, L.-T.; Meng, Z.-Q. Predictive role of the monocyte-to-lymphocyte ratio in advanced hepatocellular carcinoma patients receiving anti-PD-1 therapy. Transl. Cancer Res. 2022, 11, 160–170. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; De Rosi, N.; Ciranni, S.; Talarico, M.; Petullà, M.; Guzzardi, G.; Fontana, F.; Laganà, D. Endovascular treatment of femoro-popliteal occlusions with retrograde tibial access after failure of the antegrade approach. Catheter. Cardiovasc. Interv. 2023, 101, 1108–1119. [Google Scholar] [CrossRef]
- Cernigliaro, M.; Stanca, C.; Galbiati, A.; Spinetta, M.; Coda, C.; Negroni, D.; Laganà, D.; Minici, R.; Airoldi, C.; Carriero, A.; et al. Innovation in Acute Ischemic Stroke Patients over 80 y/o—A Retrospective Monocentric Study on Mechanical Thrombectomy of Consecutive Patients: Is Age an Adequate Selection Criterion? J. Clin. Med. 2023, 12, 3688. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Gerolami, R.; Caparello, C.; et al. Outcomes of sequential treatment with sorafenib followed by regorafenib for HCC: Additional analyses from the phase III RESORCE trial. J. Hepatol. 2018, 69, 353–358. [Google Scholar] [CrossRef]
- Su, T.-H.; Hsu, S.-J.; Kao, J.-H. Paradigm shift in the treatment options of hepatocellular carcinoma. Liver Int. 2022, 42, 2067–2079. [Google Scholar] [CrossRef]
- Sandow, T.A.; Arndt, S.E.; Albar, A.A.; DeVun, D.A.; Kirsch, D.S.; Gimenez, J.M.; Bohorquez, H.E.; Gilbert, P.J.; Thevenot, P.T.; Nunez, K.G.; et al. Assessment of Response to Transcatheter Arterial Chemoembolization with Doxorubicin-eluting Microspheres: Tumor Biology and Hepatocellular Carcinoma Recurrence in a 5-year Transplant Cohort. Radiology 2018, 286, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Hirose, R.; LaBerge, J.M.; Davern, T.J.; Bass, N.M.; Kerlan, R.K.; Merriman, R.; Feng, S.; Freise, C.E.; Ascher, N.L.; et al. A prospective study on downstaging of hepatocellular carcinoma prior to liver transplantation. Liver Transplant. 2005, 11, 1505–1514. [Google Scholar] [CrossRef] [PubMed]
- Mei, J.; Sun, X.-Q.; Lin, W.-P.; Li, S.-H.; Lu, L.-H.; Zou, J.-W.; Wei, W.; Guo, R.-P. Comparison of the Prognostic Value of Inflammation-Based Scores in Patients with Hepatocellular Carcinoma After Anti-PD-1 Therapy. J. Inflamm. Res. 2021, 14, 3879–3890. [Google Scholar] [CrossRef]
- Wang, C.; Wang, M.; Zhang, X.; Zhao, S.; Hu, J.; Han, G.; Liu, L. The neutrophil-to-lymphocyte ratio is a predictive factor for the survival of patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Ann. Transl. Med. 2020, 8, 541. [Google Scholar] [CrossRef] [PubMed]
- Xue, T.-C.; Jia, Q.-A.; Ge, N.-L.; Zhang, B.-H.; Wang, Y.-H.; Ren, Z.-G.; Ye, S.-L. The platelet-to-lymphocyte ratio predicts poor survival in patients with huge hepatocellular carcinoma that received transarterial chemoembolization. Tumor Biol. 2015, 36, 6045–6051. [Google Scholar] [CrossRef]
- Lin, Z.-X.; Ruan, D.-Y.; Li, Y.; Wu, D.-H.; Ma, X.-K.; Chen, J.; Chen, Z.-H.; Li, X.; Wang, T.-T.; Lin, Q.; et al. Lymphocyte-to-monocyte ratio predicts survival of patients with hepatocellular carcinoma after curative resection. World J. Gastroenterol. 2015, 21, 10898–10906. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Qiao, W.; Liu, B.; Li, J.; Yuan, C.; Long, J.; Hu, C.; Zang, C.; Zheng, J.; Zhang, Y. The monocyte to lymphocyte ratio not only at baseline but also at relapse predicts poor outcomes in patients with hepatocellular carcinoma receiving locoregional therapy. BMC Gastroenterol. 2022, 22, 98. [Google Scholar] [CrossRef]
- Shen, Y.; Wang, H.; Chen, X.; Li, W.; Chen, J. Prognostic significance of lymphocyte-to-monocyte ratio and platelet-to-lymphocyte ratio in patients with hepatocellular carcinoma undergoing transcatheter arterial chemoembolization and radiofrequency ablation. OncoTargets Ther. 2019, 12, 7129–7137. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, W.; Niu, R.; Li, Y.; Zhou, X.; Han, X. A combination of the preoperative neutrophil-to-lymphocyte and lymphocyte-to-monocyte ratios as a useful predictor of survival outcomes following the transarterial chemoembolization of huge hepatocellular carcinoma. Saudi Med. J. 2020, 41, 376–382. [Google Scholar] [CrossRef]
- Li, S.; Feng, X.; Cao, G.; Wang, Q.; Wang, L. Prognostic significance of inflammatory indices in hepatocellular carcinoma treated with transarterial chemoembolization: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0230879. [Google Scholar] [CrossRef]
- Cho, E.J.; Yu, S.J.; Bin Lee, Y.; Lee, J.-H.; Kim, Y.J.; Yoon, J.-H. Prognostic Values of Inflammation-Based Scores and Fibrosis Markers in Patients with Hepatocellular Carcinoma Treated with Transarterial Chemoembolization. Diagnostics 2022, 12, 1170. [Google Scholar] [CrossRef] [PubMed]
- Schobert, I.T.; Savic, L.J.; Chapiro, J.; Bousabarah, K.; Chen, E.; Laage-Gaupp, F.; Tefera, J.; Nezami, N.; Lin, M.; Pollak, J.; et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictors of tumor response in hepatocellular carcinoma after DEB-TACE. Eur. Radiol. 2020, 30, 5663–5673. [Google Scholar] [CrossRef] [PubMed]
- Itoh, S.; Yugawa, K.; Shimokawa, M.; Yoshiya, S.; Mano, Y.; Takeishi, K.; Toshima, T.; Maehara, Y.; Mori, M.; Yoshizumi, T. Prognostic significance of inflammatory biomarkers in hepatocellular carcinoma following hepatic resection. BJS Open 2019, 3, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Nahm, F.S. Receiver operating characteristic curve: Overview and practical use for clinicians. Korean J. Anesthesiol. 2022, 75, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.P.; Tomlinson, G.; Marrie, T.J.; Tang, P.; McGeer, A.; Low, D.E.; Detsky, A.S.; Gold, W.L. Can Routine Laboratory Tests Discriminate between Severe Acute Respiratory Syndrome and Other Causes of Community-Acquired Pneumonia? Clin. Infect. Dis. 2005, 40, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Aster, R.H. Pooling of platelets in the spleen: Role in the pathogenesis of “hypersplenic” thrombocytopenia. J. Clin. Investig. 1966, 45, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Takeshita, A.; Souda, K.; Kobayashi, Y.; Kikuyama, M.; Suzuki, F.; Kageyama, F.; Sasada, Y.; Shimizu, E.; Murohisa, G.; et al. Serum Thrombopoietin Levels in Patients With Chronic Hepatitis and Liver Cirrhosis. Am. J. Gastroenterol. 1999, 94, 1918–1922. [Google Scholar] [CrossRef] [PubMed]
- Peck-Radosavljevic, M.; Zacherl, J.; Meng, Y.; Pidlich, J.; Lipinski, E.; Längle, F.; Steininger, R.; Mühlbacher, F.; Gangl, A. Is inadequate thrombopoietin production a major cause of thrombocytopenia in cirrhosis of the liver? J. Hepatol. 1997, 27, 127–131. [Google Scholar] [CrossRef]
- Mitchell, O.; Feldman, D.M.; Diakow, M.; Sigal, S.H. The pathophysiology of thrombocytopenia in chronic liver disease. Hepat. Med. 2016, 8, 39–50. [Google Scholar] [CrossRef]
- Weksler, B.B. Review article: The pathophysiology of thrombocytopenia in hepatitis C virus infection and chronic liver disease. Aliment. Pharmacol. Ther. 2007, 26 (Suppl. S1), 13–19. [Google Scholar] [CrossRef]
- Ruggeri, Z.M. Mechanisms of shear-induced platelet adhesion and aggregation. Thromb. Haemost. 1993, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.; Accatino, L.; Alfaro, J.; Brahm, J.; Hidalgo, P.; Mezzano, D. Platelet autoantibodies in patients with chronic liver disease. Am. J. Hematol. 1995, 50, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Caly, W.R.; Strauss, E. A prospective study of bacterial infections in patients with cirrhosis. J. Hepatol. 1993, 18, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Zhang, Y.; Wang, Y.; Yao, X.; Yang, J.; Li, J. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios as Predictors of Survival and Metastasis for Recurrent Hepatocellular Carcinoma after Transarterial Chemoembolization. PLoS ONE 2015, 10, e0119312. [Google Scholar] [CrossRef]
- Rebonato, A.; Graziosi, L.; Maiettini, D.; Marino, E.; De Angelis, V.; Brunese, L.; Mosca, S.; Metro, G.; Rossi, M.; Orgera, G.; et al. Inflammatory Markers as Prognostic Factors of Survival in Patients Affected by Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. Gastroenterol. Res. Pract. 2017, 2017, 4164130. [Google Scholar] [CrossRef] [PubMed]
- Ruopp, M.D.; Perkins, N.J.; Whitcomb, B.W.; Schisterman, E.F. Youden Index and Optimal Cut-Point Estimated from Observations Affected by a Lower Limit of Detection. Biom. J. 2008, 50, 419–430. [Google Scholar] [CrossRef]
- Wei, R.; Liu, S.; Zhang, S.; Min, L.; Zhu, S. Cellular and Extracellular Components in Tumor Microenvironment and Their Application in Early Diagnosis of Cancers. Anal. Cell. Pathol. 2020, 2020, 6283796. [Google Scholar] [CrossRef]
- Labani-Motlagh, A.; Ashja-Mahdavi, M.; Loskog, A. The Tumor Microenvironment: A Milieu Hindering and Obstructing Antitumor Immune Responses. Front. Immunol. 2020, 11, 940. [Google Scholar] [CrossRef] [PubMed]
- Väyrynen, J.P.; Tuomisto, A.; Klintrup, K.; Mäkelä, J.; Karttunen, T.J.; Mäkinen, M.J. Detailed analysis of inflammatory cell infiltration in colorectal cancer. Br. J. Cancer 2013, 109, 1839–1847. [Google Scholar] [CrossRef]
- Hoffmann, T.K.; Dworacki, G.; Tsukihiro, T.; Meidenbauer, N.; Gooding, W.; Johnson, J.T.; Whiteside, T.L. Spontaneous apoptosis of circulating T lymphocytes in patients with head and neck cancer and its clinical importance. Clin. Cancer Res. 2002, 8, 2553–2562. [Google Scholar]
- Motomura, T.; Shirabe, K.; Mano, Y.; Muto, J.; Toshima, T.; Umemoto, Y.; Fukuhara, T.; Uchiyama, H.; Ikegami, T.; Yoshizumi, T.; et al. Neutrophil–lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J. Hepatol. 2013, 58, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Gajewski, T.F.; Schreiber, H.; Fu, Y.-X. Innate and adaptive immune cells in the tumor microenvironment. Nat. Immunol. 2013, 14, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer Immunoediting: Integrating Immunity’s Roles in Cancer Suppression and Promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Unitt, E.; Marshall, A.; Gelson, W.; Rushbrook, S.M.; Davies, S.; Vowler, S.L.; Morris, L.S.; Coleman, N.; Alexander, G.J. Tumour lymphocytic infiltrate and recurrence of hepatocellular carcinoma following liver transplantation. J. Hepatol. 2006, 45, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Qiu, S.-J.; Fan, J.; Zhou, J.; Wang, X.-Y.; Xiao, Y.-S.; Xu, Y.; Li, Y.-W.; Tang, Z.-Y. Intratumoral Balance of Regulatory and Cytotoxic T Cells Is Associated With Prognosis of Hepatocellular Carcinoma After Resection. J. Clin. Oncol. 2007, 25, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-J.; Zhou, L.; Xie, H.-Y.; Ahmed, T.-E.; Feng, X.-W.; Zheng, S.-S. Intratumoral regulatory T cells alone or in combination with cytotoxic T cells predict prognosis of hepatocellular carcinoma after resection. Med. Oncol. 2012, 29, 1817–1826. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Dong, L.; Cheng, L. Neutrophils in cancer carcinogenesis and metastasis. J. Hematol. Oncol. 2021, 14, 173. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Ko, S.Y.; Mohamed, M.S.; Kenny, H.A.; Lengyel, E.; Naora, H. Neutrophils facilitate ovarian cancer premetastatic niche formation in the omentum. J. Exp. Med. 2019, 216, 176–194. [Google Scholar] [CrossRef] [PubMed]
- van der Windt, D.J.; Sud, V.; Zhang, H.; Varley, P.R.; Goswami, J.; Yazdani, H.O.; Tohme, S.; Loughran, P.; O’Doherty, R.M.; Minervini, M.I.; et al. Neutrophil extracellular traps promote inflammation and development of hepatocellular carcinoma in nonalcoholic steatohepatitis. J. Hepatol. 2018, 68, 1347–1360. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, H.; Wang, Y.; Brown, Z.J.; Xia, Y.; Huang, Z.; Shen, C.; Hu, Z.; Beane, J.; Ansa-Addo, E.A.; et al. Regulatory T-cell and neutrophil extracellular trap interaction contributes to carcinogenesis in non-alcoholic steatohepatitis. J. Hepatol. 2021, 75, 1271–1283. [Google Scholar] [CrossRef]
- Fridlender, Z.G.; Sun, J.; Kim, S.; Kapoor, V.; Cheng, G.; Ling, L.; Worthen, G.S.; Albelda, S.M. Polarization of tumor-associated neutrophil pheno-type by TGF-beta: “N1” versus “N2” TAN. Cancer Cell 2009, 16, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Chanmee, T.; Ontong, P.; Konno, K.; Itano, N. Tumor-Associated Macrophages as Major Players in the Tumor Microenvironment. Cancers 2014, 6, 1670–1690. [Google Scholar] [CrossRef] [PubMed]
- Stotz, M.; Pichler, M.; Absenger, G.; Szkandera, J.; Arminger, F.; Schaberl-Moser, R.; Samonigg, H.; Stojakovic, T.; Gerger, A. The preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Br. J. Cancer 2014, 110, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Gabrilovich, D.I.; Nagaraj, S. Myeloid-derived suppressor cells as regulators of the immune system. Nat. Rev. Immunol. 2009, 9, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, A.; Iwashita, Y.; Shibata, K.; Matsumoto, T.; Ohta, M.; Kitano, S. Prognostic value of preoperative peripheral blood monocyte count in patients with hepatocellular carcinoma. Surgery 2006, 139, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.-L.; Fu, S.-J.; Huang, X.-Q.; Chen, B.; Kuang, M.; Li, S.-Q.; Hua, Y.-P.; Liang, L.-J.; Peng, B.-G. Elevated preoperative peripheral blood monocyte count predicts poor prognosis for hepatocellular carcinoma after curative resection. BMC Cancer 2014, 14, 744. [Google Scholar] [CrossRef]
- Hu, P.; Shen, H.; Wang, G.; Zhang, P.; Liu, Q.; Du, J. Prognostic Significance of Systemic Inflammation-Based Lymphocyte- Monocyte Ratio in Patients with Lung Cancer: Based on a Large Cohort Study. PLoS ONE 2014, 9, e108062. [Google Scholar] [CrossRef]
- Banerjee, A.; Chitnis, U.B.; Jadhav, S.L.; Bhawalkar, J.S.; Chaudhury, S. Hypothesis testing, type I and type II errors. Ind. Psychiatry J. 2009, 18, 127–131. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 214) | |||
|---|---|---|---|---|
| Group 1 Low LMR (n = 70) | Group 2 High LMR (n = 144) | p Value | ||
| Age (years) | 57.2 (±13.7) | 54.4 (±14.1) | 58.6 (±13.4) | 0.025 |
| Sex (Female) | 75 (35%) | 30 (42.9%) | 45 (31.3%) | 0.095 |
| Body Mass Index | 26.6 (±5) | 26.2 (±5) | 26.8 (±5) | 0.411 |
| Smoking history | 146 (68.2%) | 47 (67.1%) | 99 (68.7%) | 0.813 |
| Hepatitis B virus | 28 (13.1%) | 8 (11.4%) | 20 (13.9%) | 0.617 |
| Hepatitis C virus | 91 (42.5%) | 14 (20%) | 77 (53.5%) | <0.001 |
| Non-alcoholic fatty liver disease | 27 (12.6%) | 11 (15.7%) | 16 (11.1%) | 0.341 |
| Alcoholic liver disease | 73 (34.1%) | 33 (47.1%) | 40 (27.8%) | 0.005 |
| α-Fetoprotein (ng/mL) | 237.8 (±226.2) | 311.9 (±284.6) | 201.7 (±182) | 0.026 |
| Carbohydrate antigen 19-9 (U/mL) | 11.5 (±13.6) | 12.3 (±13.6) | 11.2 (±13.6) | 0.836 |
| γ-Glutamyltransferase (U/L) | 89.1 (±56.7) | 91.8 (±70.9) | 87.8 (±48.4) | 0.860 |
| Alkaline phosphatase (U/L) | 52.6 (±21.9) | 54.3 (±20.8) | 51.8 (±22.4) | 0.161 |
| Aspartate transaminase (U/L) | 63.6 (±28.2) | 57.7 (±29.1) | 66.5 (±27.4) | 0.166 |
| Alanine transaminase (U/L) | 68.3 (±24.8) | 70.3 (±25.6) | 67.3 (±24.5) | 0.227 |
| Albumin (g/L) | 30.1 (±2.7) | 29.5 (±2.4) | 30.4 (±2.8) | 0.027 |
| Total bilirubin (mg/dL) | 1.12 (±0.4) | 1.05 (±0.4) | 1.15 (±0.4) | 0.048 |
| Direct bilirubin (mg/dL) | 0.35 (±0.4) | 0.34 (±0.4) | 0.36 (±0.4) | 0.742 |
| Indirect bilirubin (mg/dL) | 0.77 (±0.4) | 0.71 (±0.4) | 0.79 (±0.4) | 0.189 |
| Prothrombin time (seconds prolonged) | 6.3 (±1.2) | 6.1 (±1.2) | 6.4 (±1.3) | 0.136 |
| Ascites | 0 (0%) | 0 (0%) | 0 (0%) | NA |
| Child–Pugh score, A6/B7/B8/B9 | 10 (4.7%)/72 (33.6%)/128 (59.8%)/4 (1.9%) | 0 (0%)/26 (37.1%)/42 (60%)/2 (2.9%) | 10 (6.9%)/46 (31.9%)/86 (59.7%)/2 (1.4%) | 0.123 |
| ALBI grade, 1/2/3 | 20 (9.3%)/186 (86.9%)/8 (3.8%) | 6 (8.6%)/61 (87.1%)/3 (4.3%) | 14 (9.7%)/125 (86.8%)/5 (3.5%) | 0.927 |
| Cirrhosis | 213 (99.5%) | 69 (98.6%) | 114 (100%) | 0.151 |
| Total cholesterol (mg/dL) | 215.9 (±53.9) | 214.5 (±53.3) | 216.7 (±54.1) | 0.779 |
| Triglycerides (mg/dL) | 105.5 (±22) | 105.2 (±22) | 105.7 (±22) | 0.876 |
| Platelet count (No. ×103/μL) | 134.2 (±49.5) | 128.5 (±42.8) | 137 (±52.3) | 0.502 |
| Hemoglobin (g/dL) | 11.5 (±1.43) | 11.8 (±1.47) | 11.4 (±1.40) | 0.077 |
| White blood cell count (per μL) | 4649.4 (±823.5) | 4771 (±717.4) | 4590.3 (±866.5) | 0.043 |
| Neutrophil count (per μL) | 3342.4 (±774.6) | 3604.9 (±742.4) | 3214.7 (±760) | <0.001 |
| Lymphocyte count (per μL) | 896.9 (±321.6) | 710.8 (±285.5) | 987.3 (±299.2) | <0.001 |
| Monocyte count (per μL) | 247.2 (±81.2) | 277.1 (±78.6) | 231.7 (±78.7) | <0.001 |
| Lymphocyte-to-monocyte Ratio (LMR) | 4.20 (±2.27) | 2.82 (±1.57) | 4.87 (±2.26) | <0.001 |
| Neutrophil-to-lymphocyte Ratio (NLR) | 4.43 (±2.61) | 6.14 (±3.39) | 3.60 (±1.57) | <0.001 |
| Platelet-to-lymphocyte Ratio (PLR) | 169.46 (±88.01) | 210.73 (±106.11) | 149.4 (±69.75) | <0.001 |
| Maximum tumor size (cm) | 4.49 (±1.13) | 4.42 (±1.09) | 4.53 (±1.16) | 0.557 |
| Bilobar disease | 85 (39.7%) | 29 (41.4%) | 56 (38.9%) | 0.722 |
| Capsule | 112 (52.3%) | 40 (57.1%) | 72 (50%) | 0.326 |
| Variables | All Patients (n = 214) | |||
|---|---|---|---|---|
| Group 1 High NLR (n = 113) | Group 2 Low NLR (n = 101) | p Value | ||
| Age (years) | 57.2 (±13.7) | 57.5 (±15) | 56.8 (±12.2) | 0.455 |
| Sex (Female) | 75 (35%) | 35 (31%) | 40 (39.6%) | 0.186 |
| Body Mass Index | 26.6 (±5) | 26.6 (±5) | 26.7 (±5) | 0.884 |
| Smoking history | 146 (68.2%) | 74 (65.5%) | 72 (71.3%) | 0.363 |
| Hepatitis B virus | 28 (13.1%) | 10 (8.8%) | 18 (17.8%) | 0.052 |
| Hepatitis C virus | 91 (42.5%) | 32 (31.7%) | 59 (52.2%) | 0.002 |
| Non-alcoholic fatty liver disease | 27 (12.6%) | 11 (9.7%) | 16 (15.8%) | 0.179 |
| Alcoholic liver disease | 73 (34.1%) | 38 (33.6%) | 35 (34.7%) | 0.875 |
| α-Fetoprotein (ng/mL) | 237.8 (±226.2) | 258 (±248.7) | 215.1 (±196.8) | 0.118 |
| Carbohydrate antigen 19-9 (U/mL) | 11.5 (±13.6) | 12.9 (±14.2) | 10 (±12.8) | 0.550 |
| γ-Glutamyltransferase (U/L) | 89.1 (±56.7) | 91.3 (±52.9) | 86.6 (±60.7) | 0.379 |
| Alkaline phosphatase (U/L) | 52.6 (±21.9) | 52.5 (±20.7) | 52.6 (±23.3) | 0.495 |
| Aspartate transaminase (U/L) | 63.6 (±28.2) | 64 (±30.4) | 63.2 (±25.7) | 0.424 |
| Alanine transaminase (U/L) | 68.3 (±24.8) | 71.1 (±26.2) | 65.2 (±22.9) | 0.058 |
| Albumin (g/L) | 30.1 (±2.7) | 30.3 (±2.8) | 29.9 (±2.6) | 0.382 |
| Total bilirubin (mg/dL) | 1.12 (±0.4) | 1.15 (±0.4) | 1.08 (±0.4) | 0.174 |
| Direct bilirubin (mg/dL) | 0.35 (±0.4) | 0.35 (±0.4) | 0.35 (±0.4) | 0.956 |
| Indirect bilirubin (mg/dL) | 0.77 (±0.4) | 0.80 (±0.4) | 0.73 (±0.4) | 0.203 |
| Prothrombin time (seconds prolonged) | 6.3 (±1.2) | 6.3 (±1.4) | 6.3 (±1.1) | 0.669 |
| Ascites | 0 (0%) | 0 (0%) | 0 (0%) | NA |
| Child–Pugh score, A6/B7/B8/B9 | 10 (4.7%)/72 (33.6%)/128 (59.8%)/4 (1.9%) | 6 (5.3%)/36 (31.9%)/69 (61.1%)/2 (1.8%) | 4 (4%)/36 (35.6%)/59 (58.4%)/2 (2%) | 0.917 |
| ALBI grade, 1/2/3 | 20 (9.3%)/186 (86.9%)/8 (3.8%) | 10 (8.8%)/99 (87.6%)/4 (3.6%) | 10 (9.9%)/87 (86.1%)/4 (4%) | 0.950 |
| Cirrhosis | 213 (99.5%) | 113 (100%) | 100 (99%) | 0.289 |
| Total cholesterol (mg/dL) | 215.9 (±53.9) | 215.6 (±53.8) | 216.3 (±54) | 0.924 |
| Triglycerides (mg/dL) | 105.5 (±22) | 105.6 (±22) | 105.3 (±22) | 0.921 |
| Platelet count (No. ×103/μL) | 134.2 (±49.5) | 121.1 (±39.6) | 148.9 (±55.2) | <0.001 |
| Hemoglobin (g/dL) | 11.5 (±1.43) | 11.6 (±1.42) | 11.4 (±1.46) | 0.553 |
| White blood cell count (per μL) | 4649.4 (±823.5) | 4589 (±791.9) | 4717 (±856.3) | 0.247 |
| Neutrophil count (per μL) | 3342.4 (±774.6) | 3374.4 (±759.8) | 3306.6 (±793.1) | 0.531 |
| Lymphocyte count (per μL) | 896.9 (±321.6) | 784.5 (±300.6) | 1022.6 (±298) | <0.001 |
| Monocyte count (per μL) | 247.2 (±81.2) | 250.3 (±88) | 243.8 (±73.2) | 0.378 |
| Lymphocyte-to-monocyte Ratio (LMR) | 4.20 (±2.27) | 3.75 (±2.32) | 4.70 (±2.11) | <0.001 |
| Neutrophil-to-lymphocyte Ratio (NLR) | 4.43 (±2.61) | 5.12 (±2.88) | 3.66 (±2.02) | <0.001 |
| Platelet-to-lymphocyte Ratio (PLR) | 169.46 (±88.01) | 179.15 (±94.86) | 158.62 (±78.71) | 0.272 |
| Maximum tumor size (cm) | 4.49 (±1.13) | 4.60 (±1.18) | 4.38 (±1.08) | 0.371 |
| Bilobar disease | 85 (39.7%) | 40 (35.4%) | 45 (44.6%) | 0.172 |
| Capsule | 112 (52.3%) | 62 (54.9%) | 50 (49.5%) | 0.433 |
| Variables | All Patients (n = 214) | |||
|---|---|---|---|---|
| Group 1 Low LMR (n = 70) | Group 2 High LMR (n = 144) | p Value | ||
| Technical success | 214 (100%) | 70 (100%) | 144 (100%) | NA |
| Tumor Response CR PR SD PD | 20 (9.3%) 51 (23.8%) 97 (45.3%) 46 (21.5%) | 0 (0%) 10 (14.3%) 40 (57.1%) 20 (28.6%) | 20 (13.9%) 41 (28.5%) 57 (39.6%) 26 (18.1%) | <0.001 |
| Complete Response | 20 (9.3%) | 0 (0%) | 20 (13.9%) | 0.001 |
| Objective Response (CR + PR) | 71 (33.2%) | 10 (14.3%) | 61 (42.4%) | <0.001 |
| Sustained Response Duration ≥ 6 months | 111 (51.9%) | 38 (54.3%) | 73 (50.7%) | 0.662 |
| Overall Survival at 6 months | 214 (100%) | 70 (100%) | 144 (100%) | NA |
| Progression-free survival at 6 months | 140 (65.4%) | 32 (45.7%) | 108 (75%) | <0.001 |
| Successful Downstaging at 6 months | 22 (10.3%) | 0 (0%) | 22 (15.3%) | 0.001 |
| Adverse Events | 66 (30.8%) | 24 (34.3%) | 42 (29.2%) | 0.447 |
| Variables | All Patients (n = 214) | |||
|---|---|---|---|---|
| Group 1 High NLR (n = 113) | Group 2 Low NLR (n = 101) | p Value | ||
| Technical success | 214 (100%) | 113 (100%) | 101 (100%) | NA |
| Tumor Response CR PR SD PD | 20 (9.3%) 51 (23.8%) 97 (45.3%) 46 (21.5%) | 9 (8%) 16 (14.2%) 58 (51.3%) 30 (26.5%) | 11 (10.9%) 35 (34.7%) 39 (38.6%) 16 (15.8%) | 0.002 |
| Complete Response | 20 (9.3%) | 9 (8%) | 11 (10.9%) | 0.463 |
| Objective Response (CR + PR) | 71 (33.2%) | 25 (22.1%) | 46 (45.5%) | <0.001 |
| Sustained Response Duration ≥ 6 months | 111 (51.9%) | 55 (48.7%) | 56 (55.4%) | 0.322 |
| Overall Survival at 6 months | 214 (100%) | 113 (100%) | 101 (100%) | NA |
| Progression-free survival at 6 months | 140 (65.4%) | 61 (54%) | 79 (78.2%) | <0.001 |
| Successful Downstaging at 6 months | 22 (10.3%) | 13 (11.5%) | 9 (8.9%) | 0.533 |
| Adverse Events | 66 (30.8%) | 38 (33.6%) | 28 (27.7%) | 0.350 |
| Predictors | Coeff. | Std. Err. | Wald | p > |z| |
|---|---|---|---|---|
| Age (years) | 0.052–0.068 | 0.013–0.017 | 17.464–16.714 | <0.001–<0.001 |
| Sex (female) | −0.011 | 0.304 | 0.001 | 0.972 |
| Hepatitis C virus | −0.922–−1.858 | 0.312–0.422 | 8.714–19.382 | 0.003–<0.001 |
| α-Fetoprotein (ng/mL) | −0.004–−0.004 | 0.001–0.001 | 14.285–11.734 | <0.001–0.001 |
| Albumin (g/L) | 0.058 | 0.053 | 1.204 | 0.272 |
| White blood cell count (per μL) | <0.001 | <0.001 | 0.193 | 0.661 |
| Neutrophil count (per μL) | <0.001 | <0.001 | 0.898 | 0.343 |
| Lymphocyte count (per μL) | 0.003–0.004 | 0.001–0.001 | 26.029–33.849 | <0.001–<0.001 |
| Monocyte count (per μL) | −0.005–−0.004 | 0.002–0.002 | 6.091–3.398 | 0.014–0.065 |
| Neutrophil-to-lymphocyte ratio (NLR) | −0.503 | 0.108 | 21.585 | <0.001 |
| NLR Groups (<4.72) | 1.080 | 0.302 | 12.772 | <0.001 |
| Lymphocyte-to-monocyte ratio (LMR) | 0.322 | 0.069 | 21.615 | <0.001 |
| LMR Groups (≥2.24) | 1.484 | 0.381 | 15.172 | <0.001 |
| Bilobar disease | −0.562 | 0.307 | 3.350 | 0.067 |
| Predictors | Coeff. | Std. Err. | Wald | p > |z| |
|---|---|---|---|---|
| Age (years) | −0.013 | 0.011 | 1.477 | 0.224 |
| Sex (female) | −0.177 | 0.304 | 0.339 | 0.560 |
| Hepatitis C virus | −0.213 | 0.290 | 0.541 | 0.462 |
| α-Fetoprotein (ng/mL) | −0.002–−0.001 | 0.001–0.001 | 6.332–2.286 | 0.012–0.131 |
| Albumin (g/L) | −0.009 | 0.053 | 0.031 | 0.860 |
| White blood cell count (per μL) | <0.001 | <0.001 | 4.335 | 0.037 |
| Neutrophil count (per μL) | −0.001–<0.001 | <0.001–<0.001 | 8.588–2.286 | 0.003–0.131 |
| Lymphocyte count (per μL) | 0.003–0.003 | 0.001–0.001 | 29.031–21.985 | <0.001–<0.001 |
| Monocyte count (per μL) | −0.016–−0.014 | 0.003–0.003 | 39.167–26.015 | <0.001–<0.001 |
| Neutrophil-to-lymphocyte ratio (NLR) | −0.427 | 0.082 | 26.832 | <0.001 |
| NLR Groups (<4.72) | 1.119 | 0.306 | 13.353 | <0.001 |
| Lymphocyte-to-monocyte ratio (LMR) | 0.768 | 0.121 | 40.453 | <0.001 |
| LMR Groups (≥2.24) | 1.270 | 0.308 | 17.062 | <0.001 |
| Bilobar disease | 0.034 | 0.294 | 0.013 | 0.908 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minici, R.; Venturini, M.; Guzzardi, G.; Fontana, F.; Coppola, A.; Piacentino, F.; Torre, F.; Spinetta, M.; Maglio, P.; Guerriero, P.; et al. A Multicenter International Retrospective Investigation Assessing the Prognostic Role of Inflammation-Based Scores (Neutrophil-to-Lymphocyte, Lymphocyte-to-Monocyte, and Platelet-to-Lymphocyte Ratios) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations of the Liver. Cancers 2024, 16, 1618. https://doi.org/10.3390/cancers16091618
Minici R, Venturini M, Guzzardi G, Fontana F, Coppola A, Piacentino F, Torre F, Spinetta M, Maglio P, Guerriero P, et al. A Multicenter International Retrospective Investigation Assessing the Prognostic Role of Inflammation-Based Scores (Neutrophil-to-Lymphocyte, Lymphocyte-to-Monocyte, and Platelet-to-Lymphocyte Ratios) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations of the Liver. Cancers. 2024; 16(9):1618. https://doi.org/10.3390/cancers16091618
Chicago/Turabian StyleMinici, Roberto, Massimo Venturini, Giuseppe Guzzardi, Federico Fontana, Andrea Coppola, Filippo Piacentino, Federico Torre, Marco Spinetta, Pietro Maglio, Pasquale Guerriero, and et al. 2024. "A Multicenter International Retrospective Investigation Assessing the Prognostic Role of Inflammation-Based Scores (Neutrophil-to-Lymphocyte, Lymphocyte-to-Monocyte, and Platelet-to-Lymphocyte Ratios) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations of the Liver" Cancers 16, no. 9: 1618. https://doi.org/10.3390/cancers16091618