Selection and Outcome of Portal Vein Resection in Pancreatic Cancer

Abstract
:
1. History of Portal Vein Resection
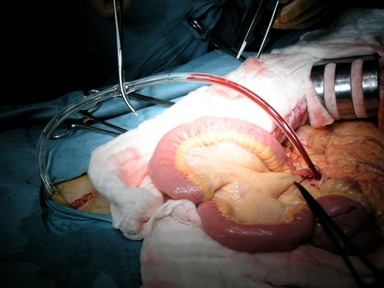
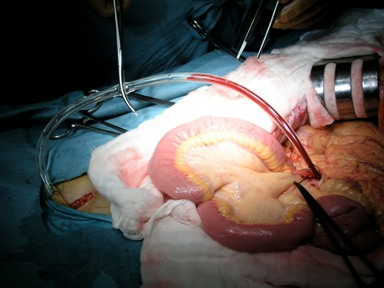
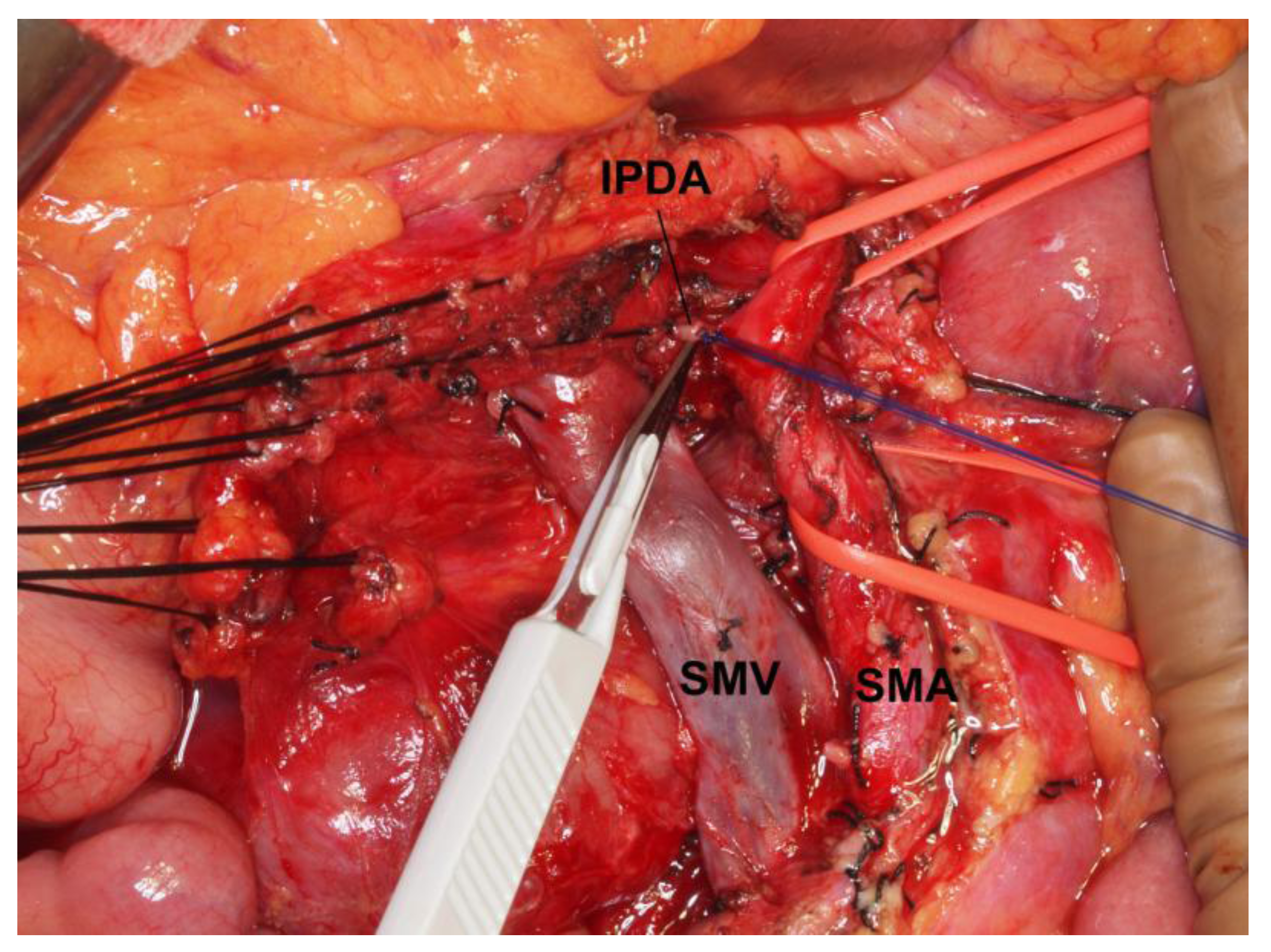
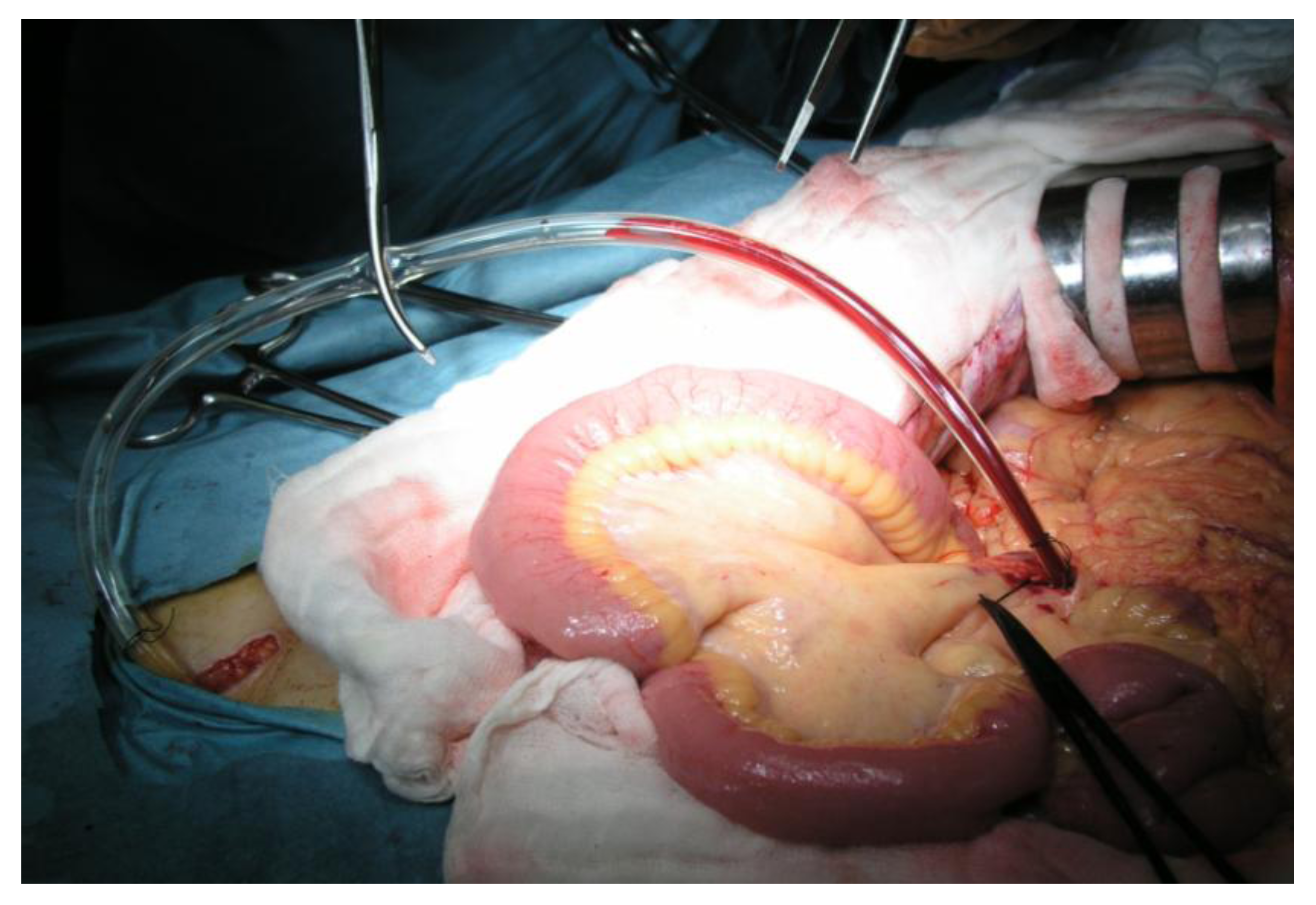
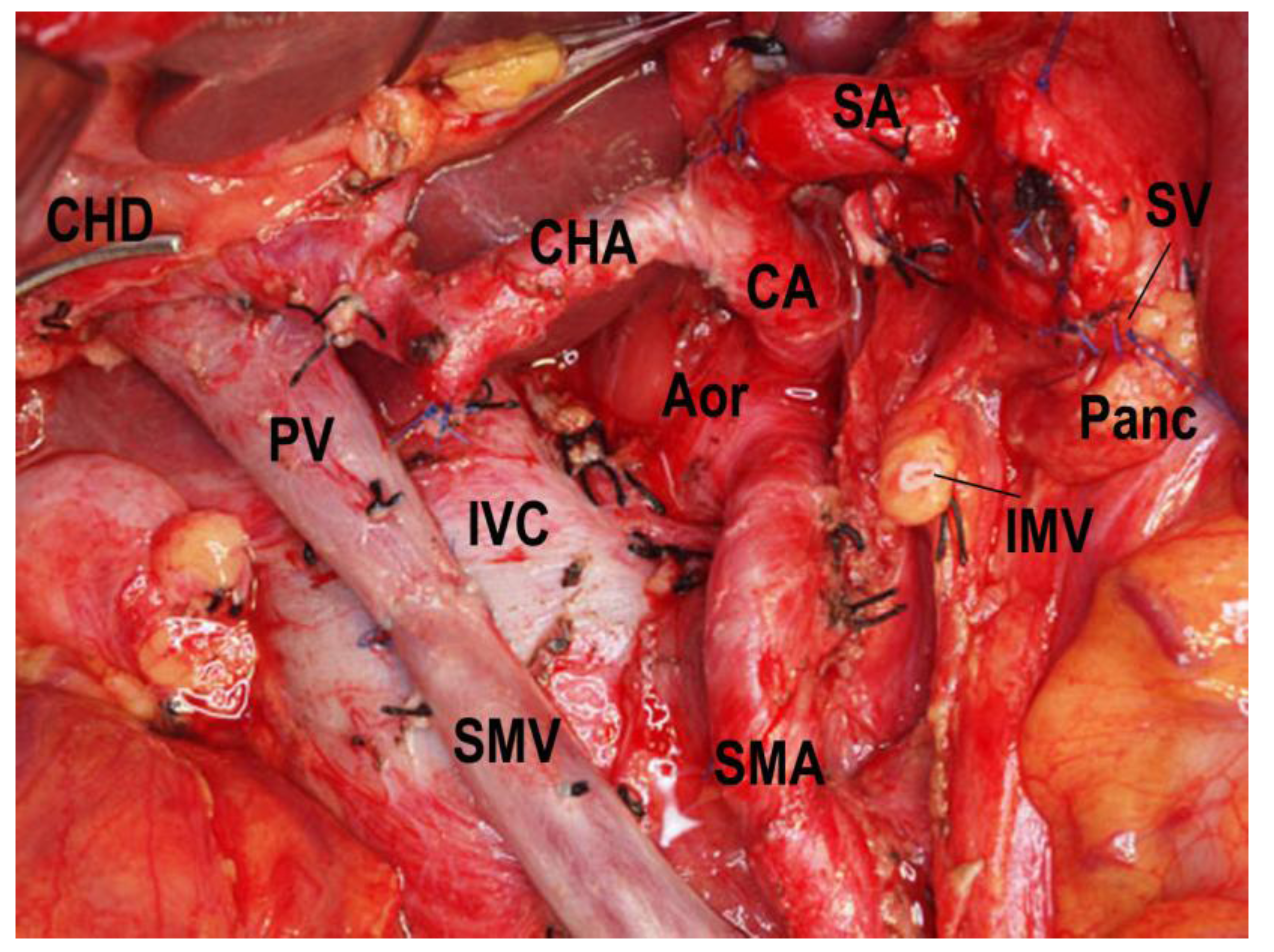
2. Catheter-Bypass Procedure and Isolated Pancreatectomy




3. Morbidity and Mortality
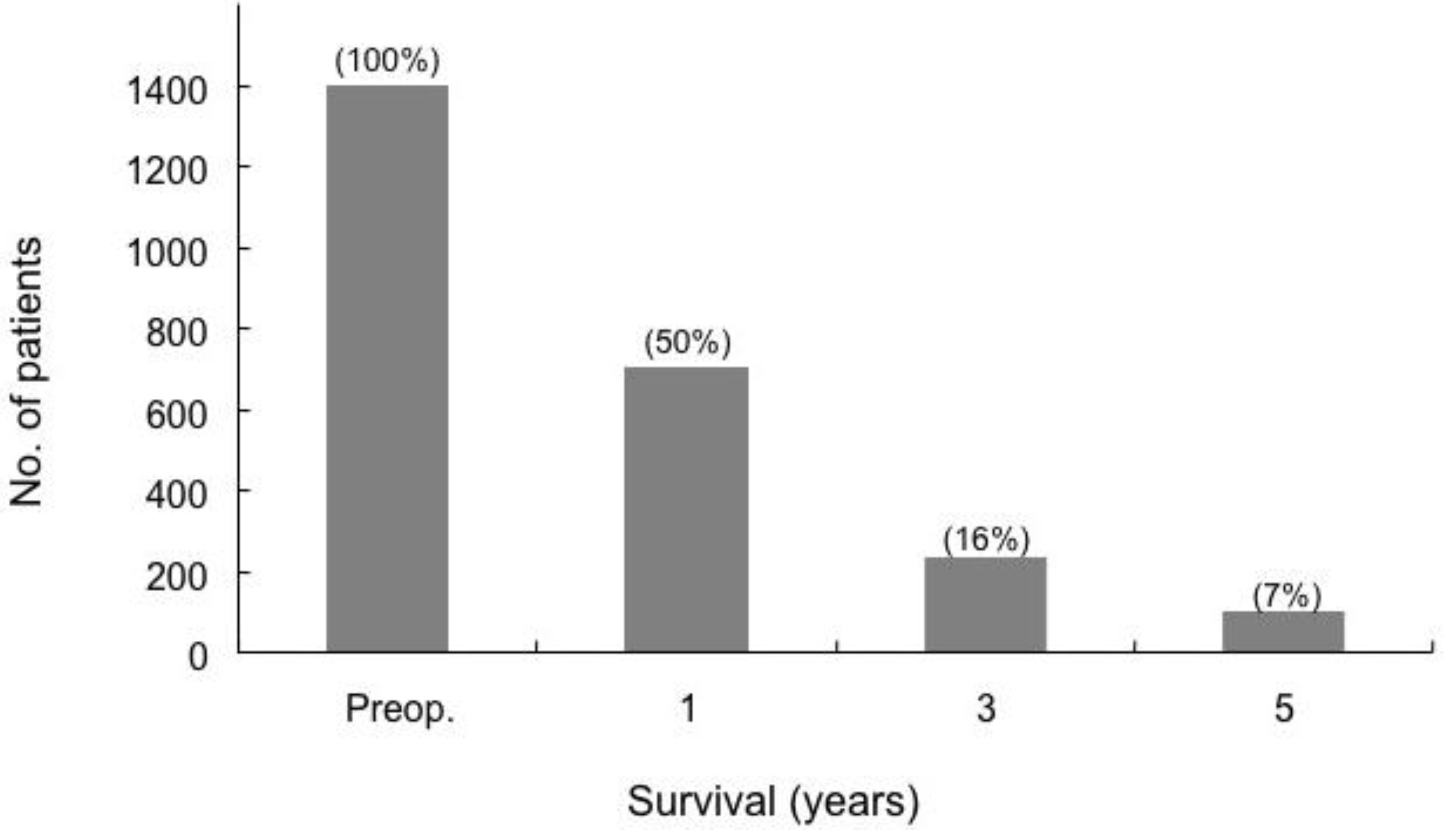
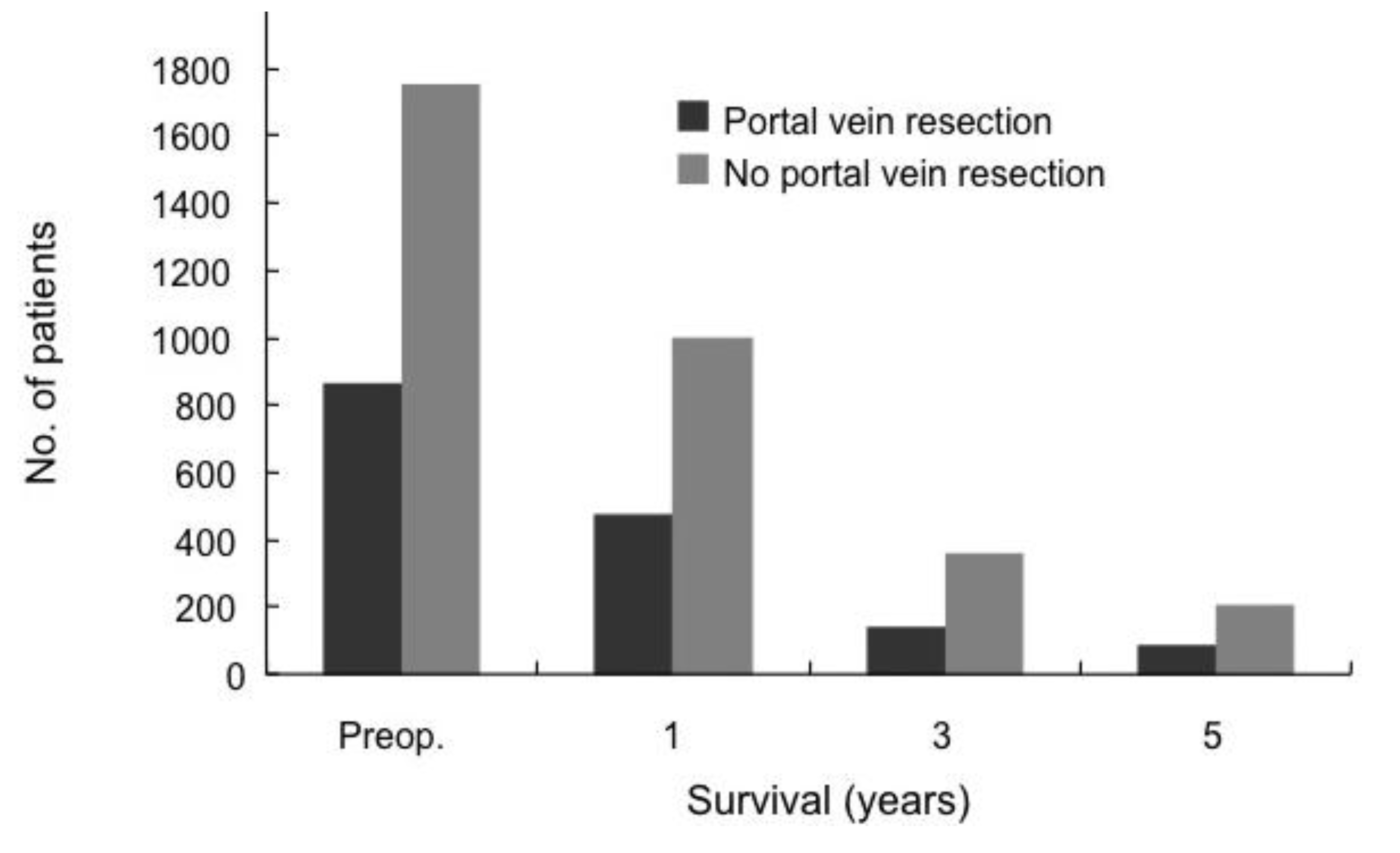
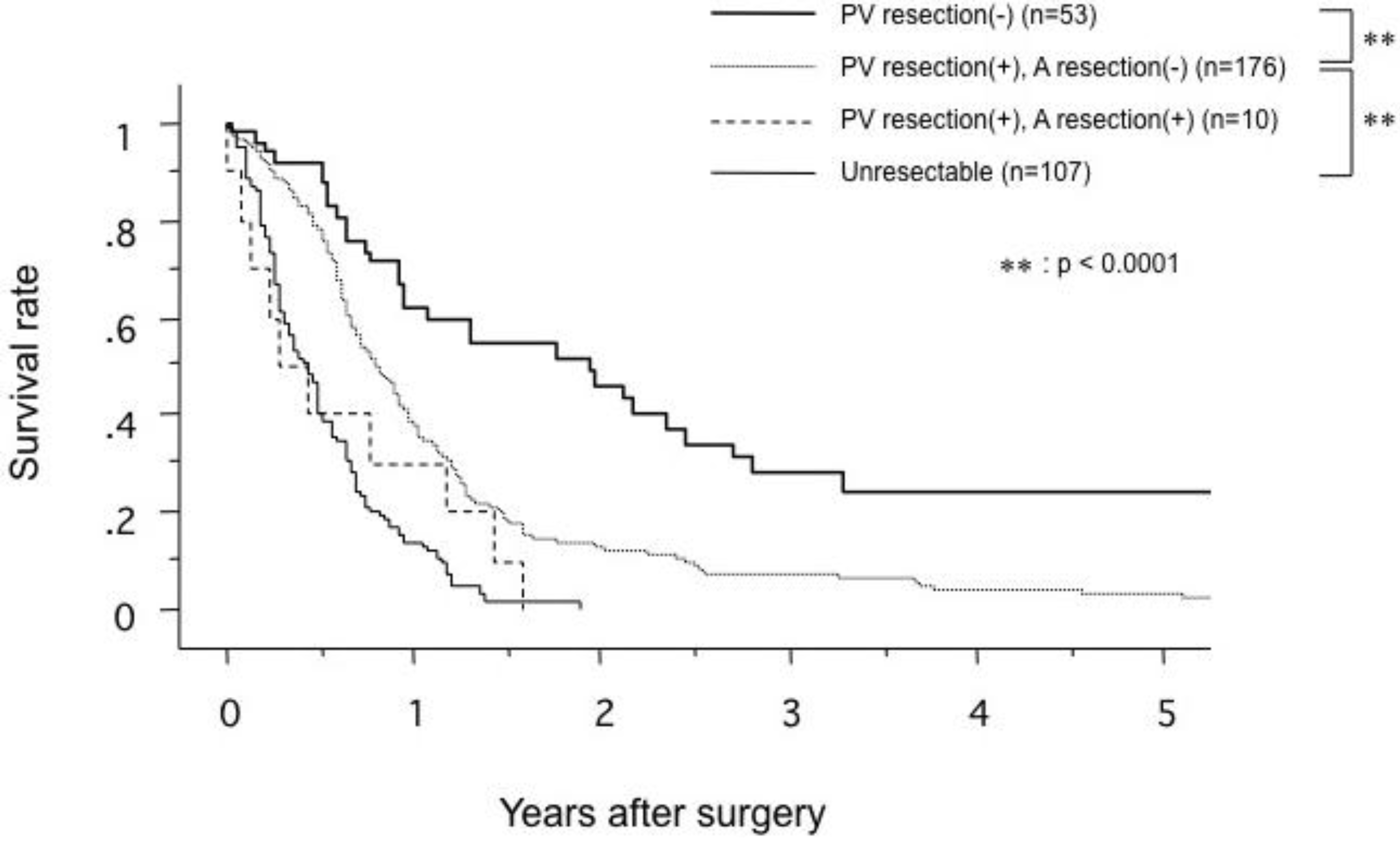
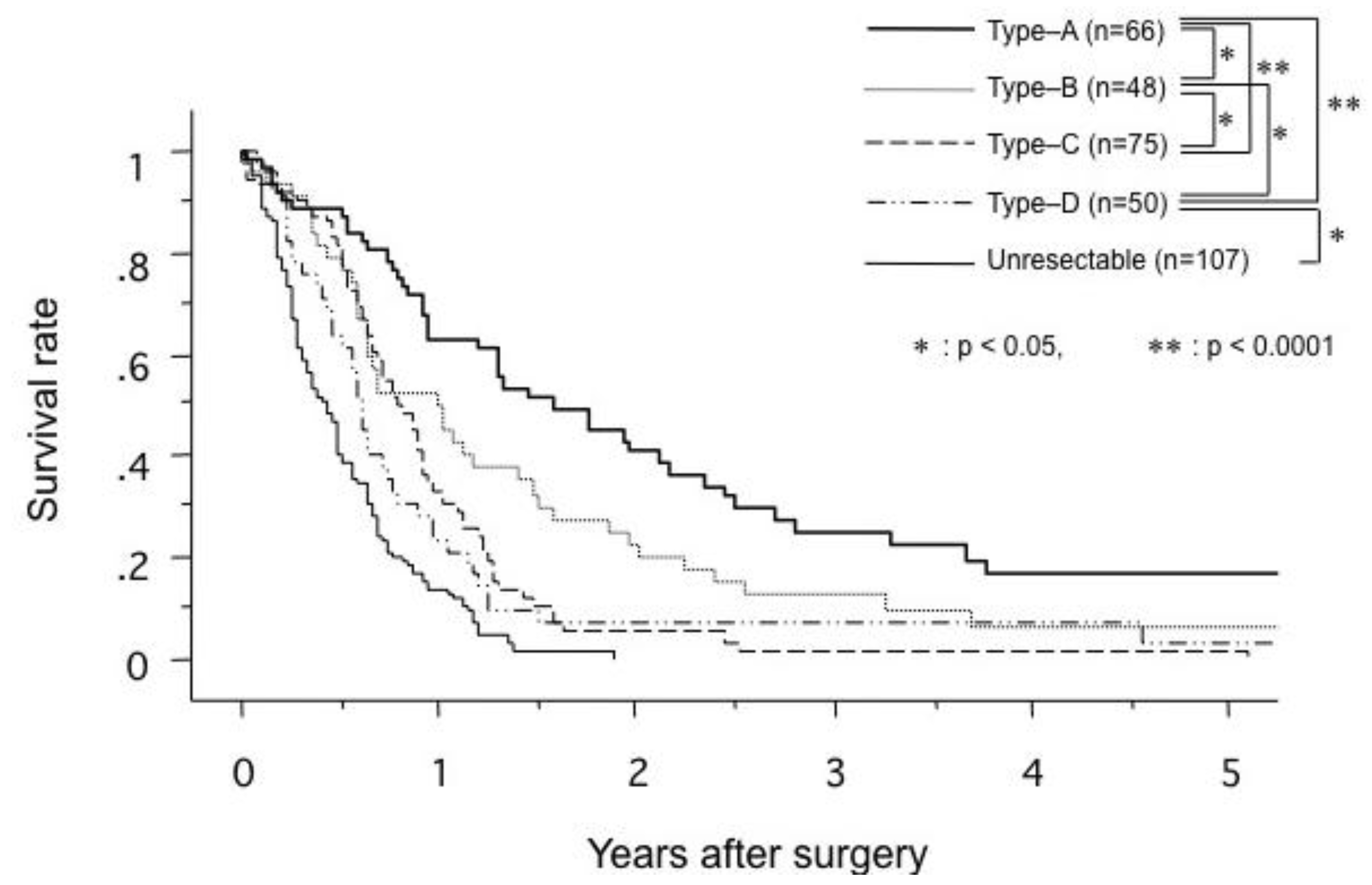
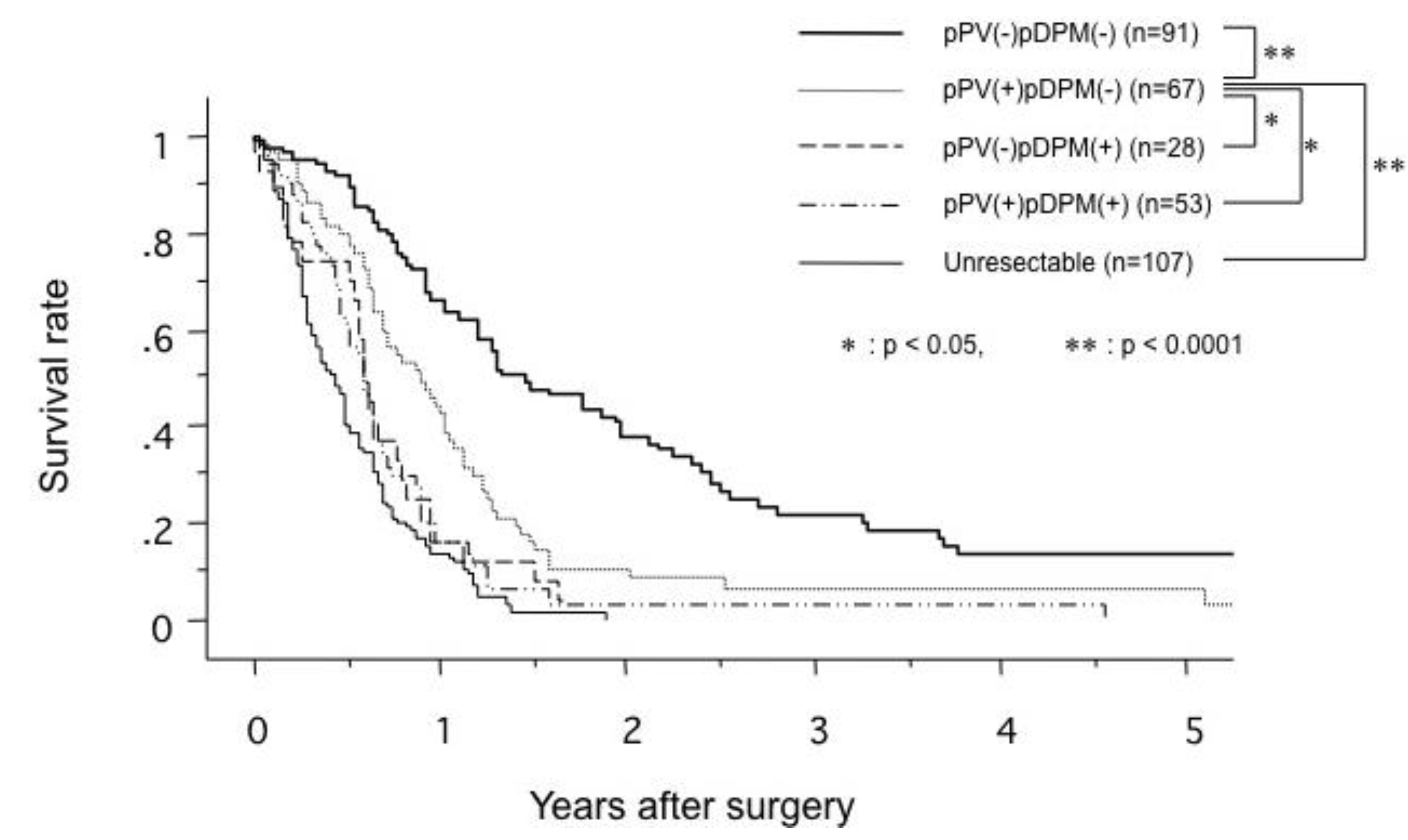
4. Survival





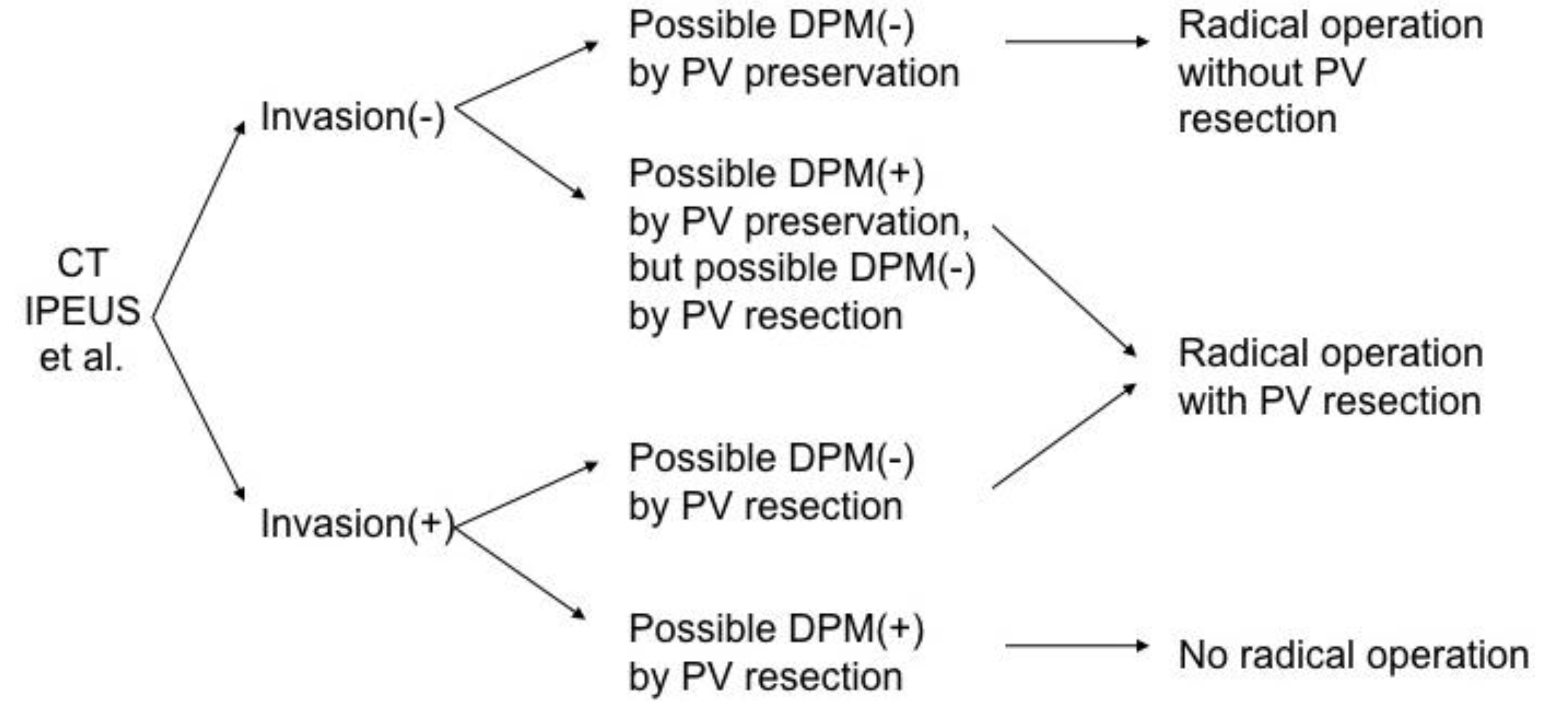
5. Indications for Portal Vein Resection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resectable |
| No distant metastases (liver, peritoneal, etc.) |
| No superior mesenteric, celiac or hepatic artery encasement |
| Normal portography |
| Locally advanced resectable (Borderline resectable) |
| Abnormal portography, but possibility of reconstruction |
| Tumor abutment on celiac or superior mesenteric artery |
| Invasion of stomach, colon or mesocolon |
| Unresectable |
| Distant metastases (liver, peritoneal, etc.) |
| Superior mesenteric, celiac, or hepatic artery encasement |
| Lymph–node metastases outside the dissection field |
| Portal or superior mesenteric venous invasion with obstruction indicating impossibility of reconstruction |
| Severe concomitant disease |

6. Effect of Clinical Volume
7. Conclusions
References
- Whipple, A.O.; Parsons, W.B. Treatment of Carcinoma of the Ampulla of Vater. Ann. Surg. 1935, 102, 763–779. [Google Scholar] [CrossRef]
- Child, C.G. Pancreaticojejunostomy and Other Problems Associated with the Surgical Management of Carcinoma Involving the Head of the Pancreas: Report of Five Additional Cases of Radical Pancreaticoduodenectomy. Ann. Surg. 1944, 119, 845–855. [Google Scholar] [CrossRef]
- Cattell, R.B. A Technic for Pancreatoduodenal Resection. Surg. Clin. North Am. 1948, 28, 761–775. [Google Scholar]
- Child, C.G., 3rd.; Holswade, G.R.; McClure, R.D., Jr.; Gore, A.L.; O'Neill, E.A. Pancreaticoduodenectomy with Resection of the Portal Vein in the Macaca mulatta Monkey and in Man. Surg. Gynecol. Obstet. 1952, 94, 31–45. [Google Scholar]
- McDermott, W.V., Jr. A One-stage Pancreatoduodenectomy with Resection of the Portal Vein for Carcinoma of the Pancreas. Ann. Surg. 1952, 136, 1012–1018. [Google Scholar] [CrossRef]
- Kikuchi, S. A Clinical and Experimental Study on the Management of Portal Vein During Pancreaticoduodenectomy. III. Clinical Cases with Operation on the Portal Vein During Pancreaticoduodenectomy. Tohoku J. Exp. Med. 1956, 64, 143–149. [Google Scholar] [CrossRef]
- Asada, S.; Itaya, H.; Nakamura, K.; Isohashi, T.; Masuoka, S. Radical Pancreatoduodenectomy and Portal Vein Resection. Report of Two Successful Cases with Transplantation of Portal Vein. Arch. Surg. 1963, 87, 609–613. [Google Scholar] [CrossRef]
- Sigel, B.; Bassett, J.G.; Cooper, D.R.; Dunn, M.R. Resection of the Superior Mesenteric Vein and Replacement with a Venous Autograft During Pancreaticoduodenectomy: Case Report. Ann. Surg. 1965, 162, 941–945. [Google Scholar] [CrossRef]
- Moore, G.E.; Sako, Y.; Thomas, L.B. Radical Pancreatoduodenectomy with Resection and Reanastomosis of the Superior Mesenteric Vein. Surgery 1951, 30, 550–553. [Google Scholar]
- Longmire, W.P. Jr. The Technique of Pancreaticoduodenal Resection. Surgery 1966, 59, 344–352. [Google Scholar]
- Cassebaum, W.H. Resection of Superior Mesenteric Vessels in Pancreatectomy. N. Y. State J. Med. 1971, 71, 366–368. [Google Scholar]
- Norton, L.; Eiseman, B. Replacement of Portal Vein During Pancreatectomy for Carcinoma. Surgery 1975, 77, 280–284. [Google Scholar]
- Fortner, J.G. Regional Resection of Cancer of the Pancreas: A New Surgical Approach. Surgery 1973, 73, 307–320. [Google Scholar]
- Nakao, A.; Nonami, T.; Harada, A.; Kasuga, T.; Takagi, H. Portal Vein Resection with a New Antithrombogenic Catheter. Surgery 1990, 108, 913–918. [Google Scholar]
- Nakao, A.; Takagi, H. Isolated Pancreatectomy for Pancreatic Head Carcinoma Using Catheter Bypass of the Portal Vein. Hepatogastroenterology 1993, 40, 426–429. [Google Scholar]
- Siriwardana, H.P.; Siriwardena, A.K. Systematic Review of Outcome of Synchronous Portal-superior Mesenteric Vein Resection During Pancreatectomy for Cancer. Br. J. Surg. 2006, 93, 662–673. [Google Scholar] [CrossRef]
- Nakao, A.; Harada, A.; Nonami, T.; Kaneko, T.; Inoue, S.; Takagi, H. Clinical Significance of Portal Invasion by Pancreatic Head Carcinoma. Surgery 1995, 117, 50–55. [Google Scholar] [CrossRef]
- Nakao, A.; Takeda, S.; Inoue, S.; Nomoto, S.; Kanazumi, N.; Sugimoto, H.; Fujii, T. Indications and Techniques of Extended Resection for Pancreatic Cancer. World J. Surg. 2006, 30, 976–982; discussion 983–984. [Google Scholar] [CrossRef]
- Nakao, A. The Pancreas: An Integrated Textbook of Basic Science, Medicine, and Surgery, 2nd Edition; Hans, G.B., Markus, B., Eds.; Wiley-Blackwell Publishing: Oxford, UK, 2008; pp. 689–695. [Google Scholar]
- Kaneko, T.; Nakao, A.; Inoue, S.; Harada, A.; Nonami, T.; Itoh, S.; Endo, T.; Takagi, H. Intraportal Endovascular Ultrasonography in the Diagnosis of Portal Vein Invasion by Pancreatobiliary Carcinoma. Ann. Surg. 1995, 222, 711–718. [Google Scholar] [CrossRef]
- Nakao, A.; Kaneko, T. Intravascular Ultrasonography for Assessment of Portal Vein Invasion by Pancreatic Carcinoma. World J. Surg. 1999, 23, 892–895. [Google Scholar] [CrossRef]
- Edge, S.B.; Schmieg, R.E., Jr; Rosenlof, L.K.; Wilhelm, M.C. Pancreas Cancer Resection Outcome in American University Centers in 1989–1990. Cancer 1993, 71, 3502–3508. [Google Scholar] [CrossRef]
- Lieberman, M.D.; Kilburn, H.; Lindsey, M.; Brennan, M.F. Relation of Perioperative Deaths to Hospital Volume Among Patients Undergoing Pancreatic Resection for Malignancy. Ann. Surg. 1995, 222, 638–645. [Google Scholar] [CrossRef]
- Gordon, T.A.; Burleyson, G.P. The Effectiveness of Whipple Resection in Patients with Pancreatic Cancer at Veterans Affairs (VA) Hospitals. Ann. Surg. 1996, 223, 446. [Google Scholar]
- Imperato, P.J.; Nenner, R.P.; Starr, H.A.; Will, T.O.; Rosenberg, C.R.; Dearie, M.B. The Effects of Regionalization on Clinical Outcomes for a High Risk Surgical Procedure: A Study of the Whipple Procedure in New York State. Am. J. Med. Qual. 1996, 11, 193–197. [Google Scholar] [CrossRef]
- Gouma, D.J.; van Geenen, R.C.; van Gulik, T.M.; de Haan, R.J.; de Wit, L.T.; Busch, O.R.; Obertop, H. Rates of Complications and Death After Pancreaticoduodenectomy: Risk Factors and the Impact of Hospital Volume. Ann. Surg. 2000, 232, 786–795. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Finlayson, S.R.; Tosteson, A.N.; Sharp, S.M.; Warshaw, A.L.; Fisher, E.S. Effect of Hospital Volume on In-hospital Mortality with Pancreaticoduodenectomy. Surgery 1999, 125, 250–256. [Google Scholar] [CrossRef]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Nakao, A. Selection and Outcome of Portal Vein Resection in Pancreatic Cancer. Cancers 2010, 2, 1990-2000. https://doi.org/10.3390/cancers2041990
Nakao A. Selection and Outcome of Portal Vein Resection in Pancreatic Cancer. Cancers. 2010; 2(4):1990-2000. https://doi.org/10.3390/cancers2041990
Chicago/Turabian StyleNakao, Akimasa. 2010. "Selection and Outcome of Portal Vein Resection in Pancreatic Cancer" Cancers 2, no. 4: 1990-2000. https://doi.org/10.3390/cancers2041990